
Summary
Neurofeedback (NF) is a training to enhance self-regulatory capacity over brain activity patterns and consequently over brain mental states. Recent findings suggest that NF is a promising alternative for the treatment of attention-deficit/hyperactivity disorder (ADHD). We comprehensively reviewed literature searching for studies on the effectiveness and specificity of NF for the treatment of ADHD. In addition, clinically informative evidence-based data are discussed. We found 3 systematic review on the use of NF for ADHD and 6 randomized controlled trials that have not been included in these reviews. Most nonrandomized controlled trials found positive results with medium-to-large effect sizes, but the evidence for effectiveness are less robust when only randomized controlled studies are considered. The direct comparison of NF and sham-NF in 3 published studies have found no group differences, nevertheless methodological caveats, such as the quality of the training protocol used, sample size, and sample selection may have contributed to the negative results. Further data on specificity comes from electrophysiological studies reporting that NF effectively changes brain activity patterns. No safety issues have emerged from clinical trials and NF seems to be well tolerated and accepted. Follow-up studies support long-term effects of NF. Currently there is no available data to guide clinicians on the predictors of response to NF and on optimal treatment protocol. In conclusion, NF is a valid option for the treatment for ADHD, but further evidence is required to guide its use.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common [1], chronic [2], and debilitating disorder [3–6]. Although pharmacological treatments for ADHD can be easily implemented and are usually effective, their long-term therapeutic effects are still uncertain [7, 8] and adverse events are common, especially sleep problems, decreased appetite, and growth deceleration. Furthermore, psychosocial treatments, such eas parental training and behavioral therapy seem to be effective only during its delivery, and their effects are rarely sustained long-term [7–9]. Considering the significant limitations of current available interventions, it has become a consensus among clinicians that new treatment options for ADHD are needed. In recent years, neurofeedback (NF) has been suggested as a promising possibility.
Neurofeedback, also known as electroencephalogram (EEG) biofeedback, or brainwave biofeedback, is a training to improve self-control over brain activity patterns and consequently over brain mental states. Although feedback can also be based on magnetic (magnetoencephalogram) or on near real-time hemodynamic measures of brain activity (near infrared spectroscopy, real-time functional magnetic resonance imaging) apart from 1 study using tomographic neurofeedback (tNF) [10], only the low cost EEG-based neurofeedback has been used for ADHD treatment. Through operant conditioning, individuals can be trained to control brain electric activity and a growing body of evidence shows that this can be helpful for the treatment of mental/neurological conditions, such as epilepsy [11], brain injury [12], chronic pain [13], ADHD [14], insomnia [15], and others.
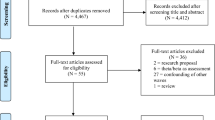
To date, 1 meta-analysis and 1 systematic review were already published reporting findings of at least 14 randomized control trials on the effectiveness of NF for the treatment of ADHD [14, 16]. In addition, several other nonrandomized and noncontrolled studies can be found in the literature. Arns et al’s [16] meta-analysis reports the effect of NF for ADHD, including different types of studies (controlled and noncontrolled, randomized and nonrandomized) published prior to 2009. Lofthouse et al. [14] systematically reviewed the literature, searching exclusively for randomized controlled studies. Although this last review was published online in November 2011, it only covers literature prior to September 2010. As scientific production on NF is growing every year, a considerable amount of data was not included in these 2 reviews. Only during the end of 2010, 2011, and 2012, there were 6 other randomized controlled studies that were published [10, 17–21], with 3 of them using sham-NF as a control group [17, 19, 20]. Another review covers more recent literature, but it is only available in German [22].
This article aims to review the existing evidence and inform clinicians on the use of NF as an alternative treatment for ADHD. In addition, clinically informative evidence-based data are discussed.
Background
Neurofeedback was introduced with the development of biofeedback during the 1960s. During the 1950s and 1960s, inspired by behaviorists ideas, Neal Miller, a researcher at Yale, proposed that it was possible to teach animals and humans to gain control of their autonomic functions [23]. The first experiments investigating classical conditioning of brain electrical activity dates back to the 1930s [24], but therapeutic applications were introduced several years later. Joe Kamiya is considered by many as the “father” of modern NF. During the 1960s, Kamiya developed a series of experiments showing that certain individuals could be trained to intentionally control its brain electrical activity and enter the “alpha state,” a mental state associated with feelings of relaxation [25]. In 1965, Sterman was studying sleep [26] when he accidentally discovered that cats could be conditioned to produce a fast EEG rhythm of approximately 12 to 15 Hz over the sensorimotor cortex (the sensorimotor rhythm [SMR]) [27]. Sterman used the same cats in another experiment in which the animals would be exposed to a toxic substance known to provoke seizures. He was surprised by the observation that the animals that had been taught to produce SMR were resistant to the convulsive effect of such substance [27]. Sterman then replicated his discovery in monkeys [28], in human open trials [29], and finally in a blind, repeated measurements controlled study [28], showing that NF could be used to control seizures. Sterman’s report encouraged other researchers to try NF for epilepsy and some of them eventually reported that children with both epilepsy and hyperkinetic symptoms showed surprising improvement of hyperkinesia after NF sessions. In 1976, Lubar and Shouse [30] were the first to report the benefit of NF for children with hyperkinetic disorders without epilepsy [30, 31].
Brain Electric Activity and Its Relation to Brain Function
Brain EEG signals can be filtered into frequency bands specified in terms of frequency in Hertz (Hz), the number of waves per second. The observation that certain EEG frequency patterns are related to certain brain activities dates back to the discovery of the EEG itself. When the German psychiatrist Hans Berger recorded the first human brain EEG, he also reported that slow-frequency waves were associated with resting states, whereas faster waves would appear in response to brain challenge (e.g., when performing a math test) [32]. Low frequencies lower than 4 Hz (Delta waves) are associated with sleep state; 4 to 7 Hz frequencies (Theta) are associated with sleep and decreased vigilance; Alpha waves (8-12 Hz) appears in relaxed/wakeful states, and fast 13 to 30 Hz waves (Beta) are related to concentration and neuronal excitability (for an overview see Table 1 in Banaschewski’s review [33]). SMR is a specific type of low Beta frequency ranging from 12 to 15 Hz observed over the sensorimotor cortex that is correlated with immobility [27]. Considering that some authors found a positive association between ADHD and higher Theta/Beta ratio [34] most NF protocols for ADHD treatment aim at increasing faster Beta frequencies, especially SMR, and decrease Theta waves. In practical terms, this training is simple and only requires an EEG amplifier plus some software or apparatus to generate continuous feedback and conditional reinforcement based on power in the critical EEG bands. In clinical practice, a computer interface (a computer game) translates for the patient how close he is to generating the target brain wave pattern. Electrodes are placed along the scalp and individuals are required to remain seated in front of a computer screen trying to find mental strategies to gain points. The computer reads the EEG signal and visual or auditory feedback is instantly generated. Changes in EEG activity made in a desired direction are rewarded. Although some differences exist in regard to frequency and number of sessions, in general NF is an intense treatment in which the patients have appointments 2 to 3 times per week (sometimes even more) having to remain seated and quiet, trying to focus on a monotonous task for 30 to 60 minutes each session.
In recent years, slow cortical potential (SCP) NF has emerged as a novel NF protocol for the treatment of ADHD. SCPs are a type of event-related potentials (ERPs). ERPs are EEG signals that appear in anticipation, or in response to the presentation of a stimulus or event. SCPs reflect the excitability level of underlying cortical regions; deflection in the negative direction appears to reflect higher excitability and positive shifts that are associated with reduced excitability or inhibition [35]. In SCP training, subjects are taught to intentionally alternate from negative to positive deflections; that means, subjects are trained to be able to produce both positive and negative shifts and consequently to intentionally and instantaneously shift brain mental state from relaxed to attentive and vice versa. This training aims to regulate the cortical excitation threshold that is possibly impaired in children with ADHD [10, 36, 37].
Is NF an Effective Treatment for ADHD and Is Its Efficacy in ADHD Based on a Specific Compounds?
To date, a considerable amount of studies already examined the effect of NF for the treatment of ADHD (see Table 1). Almost unequivocally, uncontrolled within subjects’ pre- to post-treatment analyses indicate positive results with medium-to-large effect sizes (ES) [16, 18, 21, 35, 38–47]. Arns et al. [16] computed data from 12 studies. They found a pooled within subjects ES of 1.02 for inattention; 0.71 for hyperactivity; and 0.94 for impulsivity. These results, however, may be influenced by the placebo effect, because the ES for controlled studies is considerably lower, although still impressive. In the same meta-analysis, NF was superior to passive or semi-active control groups with a pooled estimated ES of 0.81 for inattention; 0.4 for hyperactivity, and 0.69 for impulsivity. Nevertheless, only 4 of 10 studies used a randomized design and parent’s attitude in regard to treatment (preference for NF) may have lead to overestimation of its effect. Furthermore, in none of the studies, investigators were blind to the participant’s group assignment and parents were not aware of it in only 2 studies. In addition, only 1 study [18] used a truly equivalent control group that received electromyogram (EMG) biofeedback as a kind of sham-NF. Other control conditions may be problematic because the “high-tech” environment associated with NF or biofeedback can enhance parents and children expectation about positive treatment results. More recently, Lofthouse et al. [14] conducted a systematic review and reported the findings of 14 randomized controlled trials. These authors were able to identify 8 unpublished studies not included in Arns’ review [14]. Lofthouse et al. [14] were fairly more restrictive than the previous meta-analysis in regard to the minimal acceptable methodological quality of studies but found comparable ES of 0.69 (95 % CI 0.34-1.66) for overall ADHD symptoms, 0.79 (95 % CI 0.41-1.62) for inattention, and 0.71 (95 % CI 0.35-1.55) for hyperactivity/impulsivity. Since the publication of this review, however, 6 additional, well-conducted studies were published on the effectiveness of NF for treatment of children with ADHD [10, 19–21, 48], 1 for adult ADHD [49], and 1 for attentional problems in healthy adult subjects [17]. Three of these studies used a sham-controlled design [17, 19, 48], which is crucial to demonstrate that the effects seen in clinical trials are specifically related to the EEG training itself and not to nonspecific aspects of the treatment. It is possible that part of the effect of NF comes from nonspecific aspects of the attention training. It should be noted that many authors have argued that the use of sham-NF as a control group is unnecessary (although individuals are not told in which treatment group they are, it is easy for them to guess if they are in the effective treatment group or in the placebo group), unethical (ADHD is a debilitating disorder with known efficacious treatments) and even not feasible [50]. Although the ethical aspect is a debatable issue, it can often be resolved by offering real treatment after study completion and proof of superiority. The idea of feasibility is debatable, and the integrity of blinding procedures was verified in the 4 published sham-controlled studies [17, 19, 20, 48], and in all of them, blinding procedures showed to be achievable. Nevertheless, this result in favor of effective blinding may partly reflect the negative results of all 4 studies. One the other hand, the negative findings might have been determined by the use of suboptimal NF, because all of these studies used very experimental protocols and in none of them, the principals of learning theory were applied to ensure that subjects were really under conditioning procedures (see Sherlin et al. work for a review on the topic [24]). A summary of the findings from all sham- or EMG-biofeedback-controlled studies assessing efficacy of NF for ADHD can be found in Table 1. Four of these studies found no significant group differences [17–20], and 1 lacks between groups comparison [48]. Lofthouse et al.’s [14] review reports the findings of studies favoring NF in comparison to sham-NF [14], but unfortunately these studies were not published in peer-reviewed journals. One of them was described in detail in a book chapter [51], and authors’ findings are consistent with the hypothesis that it is essential to assure that patients are engaged with the training task to check its efficacy. In this study, only patients who showed good learning curves on NF training responded to treatment. It should also be highlighted that with the exception of 2 studies that included 37 and 39 participants, all other studies with negative results included very small samples and a type II error is possible. Furthermore, 1 of the 5 studies used adult healthy subjects and selected a population (university students) with attentional problems, but not ADHD [17]. It is possible that the lack of improvement found in both groups (NF and sham-NF) is a consequence of the insufficient room for improvement for such subjects. A major problem is also that the type of neurofeedback used in several sham- controlled studies did not follow standard training and transfer procedures. Additional indirect information on the specificity of NF comes from comparisons with active treatments (see Table 2 for an overview of randomized studies comparing NF to other control conditions, and see Table 3 for nonrandomized studies). There are 3 studies [43, 46, 52] reporting findings of the direct comparison of NF and stimulants, but all of them are nonrandomized (Table 3). None of these studies found NF to be inferior to medication, but comparison was restricted to neuropsychological measurements in 2 of them. Drechsler et al. [45] compared NF to cognitive behavioral therapy and found NF to be superior to psychotherapy according to parents and teachers ratings for inattention and metacognition, but not according to objective neuropsychological measurements. The 3 studies comparing NF to computerized attention skills training (CAST) yielded conflicting results. The largest study so far (including 94 individuals) found NF to be superior to CAST [39]. One study found no significant difference between groups, although only the NF group improved in relation to baseline, and the lack of difference may be due to the low power provided by the small sample sizes [53].
Another way of examining the specificity of NF is through electrophysiological study. We can obtain additional evidence for the specificity of NF if it changes the EEG pattern during and after the training toward the target state(s), and if these changes are correlated with clinical improvement. Several trials also evaluated the effect of NF on the EEG, and on learning EEG control during training. Frequency training NF compared to sham-NF has been found to effectively reduce Theta/Beta ratio during NF training and in a resting state baseline [18], and both SCP and frequency training can increase intentional control over brain electrical activity [38], although this may only hold for a subgroup of the ADHD children training with NF [45]. In a large randomized trial, the authors found SCP (when compared to CAST) to significantly decrease theta activity after training, and increase both participants capacity to modulate SCP, and Contingent Negative Variation (CNV) [54–56]. In addition, increase of the central midline alpha activity and decrease of the posterior midline theta activity was associated with improvement in ADHD symptoms [55, 56]. Controlled studies also found frequency training to be associated with a normalization of the frontal No-Go N2, [53] which is correlated with response inhibition, and with a decrease of cortical slowing [44]. Cannon et al. [57] used an innovative design to study the effect of tNF based on the estimated EEG source activity in the anterior cingulate gyrus (ACC), a structure known to be important for attention and control. The authors treated 8 healthy subjects with 30 tNF sessions and analyzed changes in ACC source activity across the sessions. They observed a significant increase of current density within the cognitive division of the ACC and in the anterior regions that receive its projections, providing strong evidence that NF categorically changes brain activity. In a follow-up study, the group reported similar, correlated increases after tomographic ACC and dorsolateral prefrontal cortex training [58]. Some authors, however, could not find NF to produce significant changes over EEG patterns [17, 19].
Alternatively, the effect of NF in the brain can be studied with high spatial resolution through hemodynamic neuroimaging. Beauregard and Lévesque [59] conducted a functional magnetic resonance imaging study and found NF to normalize the brain systems mediating selective attention and inhibitory control. This is comparable with electrophysiological data, strengthening the evidence for a specific effect of NF for ADHD. However, a recent study [10] using tNF, which also allows spatially specific feedback, showed that although it is possible to target specific brain regions with tNF training, part of the clinical improvement occurring with tNF may be due to unspecific effects.
In summary, the available studies point to a possible efficacy and specificity of NF for the treatment of ADHD, but still additional large, randomized controlled studies using blind assessment procedures are needed to clarify this issue. Sham or placebo control is an important standard approach to isolate specific effects, and another sham-controlled study has been recently completed [20]. However, future sham controlled studies should take greater care to ensure that NF remains optimized for learning of self regulation, that it includes transfer, and that it does not compromise the quality of NF just to facilitate blinding. Currently, a large multicenter randomized EMG biofeedback controlled study is being conducted in Germany (http://controlled-trials.com/ISRCTN76187185/neurofeedback), and important data can be expected in the next few years.
Which ADHD Subtypes Benefit from NF?
Very few studies computed response ratio to NF and because sample sizes are small for the majority of studies, most do not investigate possible predictors of response. Gevensleben et al. [60] defined response ratio as a reduction of at least 25 % in symptoms, and found 50 % of participants to respond to NF, suggesting that some individuals may benefit from NF, whereas others may not. Wangler et al. [61] found baseline EEG patterns, specifically, an increase of the CNV in an attention task, to be a predictor of good response to SCP training. Age and IQ have also been found to influence changes in Beta activity reached with NF: older and more intelligent children enhance Beta frequencies more strongly with treatment, but no analysis was performed in regard to clinical response [56]. Electrophysiological studies also provide additional evidence that some people are not able to gain control over brain electric activity through NF. Doehnert et al. [62] used quantitative resting EEG to examine if SCP NF versus group therapy would change CNV. No significant group by time interaction was found, but good NF performers had less pronounced CNV reduction [62]. A significant increase of positive ERPs components over frontal–central areas within the 180-420 ms latency range, possibly reflecting an activation of frontal cortical areas associated with 20 sessions of beta NF training, was found in another study using a Go/No-Go task for good, but not for bad performers [63]. Parents’ attitudes in regard to children have also been found to predict treatment response to NF. Participants whose parents use consistently reinforcing strategies have significant larger reductions of symptoms after NF [44], suggesting that at least in part, the effect of NF depends on factors not directly related to the training itself. It should be also noted that the vast majority of studies included male, school age children with ADHD combined subtype (see Tables 1, 2 and 3 for details). Thus, it is uncertain if NF works for adults, pre-schoolers, females, or other ADHD subtypes. The only study that included a majority of female subjects was the one with healthy adult academics [17], and authors failed to find positive results favoring NF in comparison with sham-NF, but no conclusive data exist to evaluate if women are less prone than man to respond to NF. Recently, a pre-post NF trial with adults with ADHD was published with encouraging preliminary results. After 15 sessions of NF, patients showed significant improvement of ADHD self-reported symptoms and a tendency for increased CNV amplitude [49]. It would be interesting to test the effects of NF for pre-schoolers because young children are less susceptible to benefit from stimulants [64] and the remission rate with behavioral therapy (as a first-line treatment) is also low [65]. However, pilot work needs to establish whether young children can regularly and for long enough attend and control artifacts to learn self-regulation.
Safety and Tolerability of NF for ADHD
Although it is regularly assumed that NF treatment does not cause side effects, only three studies systematically addressed this question. In these studies, no safety issues emerged [14, 19, 20] concerning sleep problems, tics, skin picking, headache, stomach ache, irritability, appetite loss, seizures, nausea, or feelings of agitation. In general, dropout rates from NF studies are very low and no discontinuation due to side effects are reported in clinical trials.
Is Long-Term NF Effective?
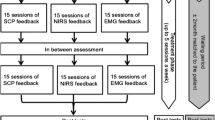
Very few studies examined the long-term effect of NF, but the few studies that did it found promising results. Gani et al. [66] conducted a 2-year follow-up of 23 of 47 children that have participated in a controlled trial in which subjects were randomized to SCP or frequency training. Two years after the end of the study, the behavioral and attentional improvements were maintained and some additional benefits could be seen, suggesting that patients were still improving even after the end of treatment. Gevensleben et al. [60] found similar results in the 6-month follow-up of their randomized controlled trial comparing NF to CAST. Sixty-five percent of participants were followed, and improvements in the NF group were superior to the control group and comparable to that of the end of the active treatment phase. At first glance, it can sound unreasonable that patients can continue to improve after treatment interruption; nevertheless, it is consistent with NF rationale. The aim of NF training is not only to promote the specific modification on the EEG pattern that is programmed to be rewarded (e.g., to enhance Beta activity), but it is to teach individuals that it is possible to gain control over mental states and to develop strategies to perceive and modify it in accordance with self control. An important part of the EEG treatment is “transfer training.” In other words, the training to transfer the skills acquired in the NF protocol to daily life. The two German trials that reported the 2 years and 6-month follow-up data previously described used transfer training to reach generalization of regulatory skills to everyday life [38, 39]. In those 2 studies, transfer training was applied as follows: in 23 % of trials patients did not receive immediate feedback, but had to guess if they were performing right or wrong for 8 seconds before they received feedback. In addition, from the 8th session onward, patients had to practice their strategy to remain “activated” for at least 10 minutes a day on some daily life task that require them to be attentive like doing the homework or playing a game. Children were instructed to identify situations in which these strategies would be important and to increase their attention control strategies [39]. In conclusion, available data suggest that NF is effective long-term, but it is possible that the long-term effects of NF depend on the generalization of regulatory skills to daily life.
What Treatment Protocol is the Best?
Frequency training and SCP are the most commonly used treatment protocols for ADHD. Some authors have hypothesized that frequency training would be better for improving tonic aspects of cortical arousal, whereas SCP would be preferable for enhancing phasic regulation of attentive behavior [39]. SCP protocols tend to be more homogeneous, but several different treatment protocols have been proposed for frequency training. Tables 1, 2, and 3 describe characteristics of the different protocols used in controlled trials in regard to the target frequency band, the electrode placement, the number, duration, and frequency of sessions. However, there is no controlled scientific data on the direct comparison of different frequency protocols. Arns et al. [16] found no difference for the effect size of studies using different protocols (SMR/Theta, SRM/Beta/Theta, and SCP). SCP has been compared to Theta/Beta training in 2 randomized controlled trials and both protocols showed to be equally effective for behavioral and cognitive improvements [38, 39]. One important difference between treatment protocols is whether they are individualized or standardized. The majority of clinical trials use standardized protocols. As standardization of all procedures is the regular practice in research, we do not have enough empirical data to assure the efficacy of personalized methods planned in accordance with each individual EEG pattern. Nevertheless, recently a small, open-label pilot study showed a significant clinical improvement and electrophysiological normalization after neurofeedback sessions [67]. This is compatible with empirical data showing that different behavioral profiles of children with ADHD present different patterns of EEG activity [34]. In summary, no conclusive data exist supporting the superiority of any of the available protocols.
In addition, there are scarce data on the minimum number of sessions needed for optimal results. Arns et al.’s [16] meta-analysis found a significant correlation between ES and treatment duration (i.e., the average number of sessions) only for improvement of inattention, but not for impulsivity and hyperactivity. However, a naturalistic quasi-experiment that included a large set of 1089 patients undergoing NF treatment found a statistically significant superiority of 40 sessions in comparison with 20 sessions for impulse control and response consistency in a continuous performance test [68]. Nevertheless, performance on neuropsychological tests may benefit from training, and this result can reflect not necessarily improvement but learning. In addition, a controlled study monitored symptoms improvement along 40 sessions of NF and could not find any additional improvement after session 24 [20].
Is There Evidence for the Use of NF as a Monotherapy for ADHD?
NF has been proven to be efficacious in the vast majority of trials conducted so far, but there is not enough data to support the use of NF as a monotherapy for ADHD. The great majority of studies tested NF as an adjunctive treatment, and for ethical reasons other treatments are usually not discontinued. Although only a minority of patients included in the studies are receiving medication (12 % of the 973 patients included in Arns’ meta-analysis [16]), psychoeducation and other psychosocial treatment are regularly allowed. Monastra et al. [44] compared NF combined with a multimodal treatment (comprising methylphenidate, parents counseling, and academic support) to the multimodal treatment itself. After the treatment phase, children were assessed with and without the ongoing stimulant therapy and results showed that both groups improved comparably, but only children in the NF group sustained the gains after medication washout. This may suggest that the association of NF to other treatments has the potential to consolidate achieved gains allowing medication to be withdrawn after awhile. Studies investigating not only the effectiveness of NF, but also the best scenario for its use are needed.
Conclusions and Future Directions
In conclusion, although the first positive trials for the use of NF for ADHD were published in the 1970s, well-designed, randomized controlled studies have been conducted only in recent years. Although some data suggest possible efficacy and specificity of NF for the treatment of ADHD, considerable work is still needed to determine the contribution of specific in comparison to nonspecific components, when and how to use NF in routinely clinical practice, and how to implement NF standards covering the fidelity of the EEG and artifact control methodology, as well the behavioral therapy aspects. Nevertheless, in specific settings, depending on parents and children preferences and on the acceptance for other treatment, NF provides a valuable alternative.
References
Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry 2007;164:942-948
Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med 2006;36:159-165.
Klassen AF, Miller A, Fine S. Health-related quality of life in children and adolescents who have a diagnosis of attention-deficit/hyperactivity disorder. Pediatrics 2004;114:e541-e547.
Lahey BB, Pelham WE, Loney J, et al. Three-year predictive validity of DSM-IV attention deficit hyperactivity disorder in children diagnosed at 4-6 years of age. Am J Psychiatry 2004;161:2014-2020.
Barkley RA, Murphy KR, Kwasnik D. Motor vehicle driving competencies and risks in teens and young adults with attention deficit hyperactivity disorder. Pediatrics 1996;98:1089-1095.
Mannuzza S, Klein RG, Bessler A, Malloy P, LaPadula M. Adult outcome of hyperactive boys. Educational achievement, occupational rank, and psychiatric status. Arch Gen Psychiatry 1993;50:565-576.
Hazell PL. 8-year follow-up of the MTA sample. J Am Acad Child Adolesc Psychiatry 2009;48:461-462.
Molina BS, Hinshaw SP, Swanson JM, et al. The MTA at 8 years: prospective follow-up of children treated for combined-type ADHD in a multisite study. J Am Acad Child Adolesc Psychiatry 2009;48:484-500.
Biederman J, Spencer T, Wilens T. Evidence-based pharmacotherapy for attention-deficit hyperactivity disorder. Int J Neuropsychopharmacol 2004;7:77-97.
Liechti MD, Maurizio S, Heinrich H, et al. First clinical trial of tomographic neurofeedback in attention-deficit/hyperactivity disorder: Evaluation of voluntary cortical control. Clin Neurophysiol 2012; doi:10.1016/j.clinph.2012.03.016.
Tan G, Thornby J, Hammond DC, et al. Meta-analysis of EEG biofeedback in treating epilepsy. Clin EEG Neurosci 2009;40:173-179.
Thornton KE, Carmody DP. Efficacy of traumatic brain injury rehabilitation: interventions of QEEG-guided biofeedback, computers, strategies, and medications. Appl Psychophysiol Biofeedback 2008;33:101-124.
Kayiran S, Dursun E, Dursun N, Ermutlu N, Karamursel S. Neurofeedback intervention in fibromyalgia syndrome; a randomized, controlled, rater blind clinical trial. Appl Psychophysiol Biofeedback 2010;35:293-302.
Lofthouse N, Arnold LE, Hersch S, Hurt E, Debeus R. A review of neurofeedback treatment for pediatric ADHD. J Atten Disord 2012;16:351-372.
Cortoos A, De Valck E, Arns M, Breteler MH, Cluydts R. An exploratory study on the effects of tele-neurofeedback and tele-biofeedback on objective and subjective sleep in patients with primary insomnia. Appl Psychophysiol Biofeedback 2010;35:125-134.
Arns M, de Ridder S, Strehl U, Breteler M, Coenen A. Efficacy of neurofeedback treatment in ADHD: the effects on inattention, impulsivity and hyperactivity: a meta-analysis. Clin EEG Neurosci 2009;40:180-189.
Logemann HN, Lansbergen MM, Van Os TW, Bocker KB, Kenemans JL. The effectiveness of EEG-feedback on attention, impulsivity and EEG: a sham feedback controlled study. Neurosci Lett 2010;479:49-53.
Bakhshayesh AR, Hansch S, Wyschkon A, Rezai MJ, Esser G. Neurofeedback in ADHD: a single-blind randomized controlled trial. Eur Child Adolesc Psychiatry 2011;20:481-491.
Lansbergen MM, van Dongen-Boomsma M, Buitelaar JK, Slaats-Willemse D. ADHD and EEG-neurofeedback: a double-blind randomized placebo-controlled feasibility study. J Neural Transm 2011;118:275-284.
Arnold LE, Lofthouse N, Hersch S, et al. EEG Neurofeedback for ADHD: Double-Blind Sham-Controlled Randomized Pilot Feasibility Trial. J Atten Disord 2012; doi:10.1177/1087054712446173.
Steiner NJ, Sheldrick RC, Gotthelf D, Perrin EC. Computer-based attention training in the schools for children with attention deficit/hyperactivity disorder: a preliminary trial. Clin Pediatr (Phila) 2011;50:615-622.
Drechsler R. Ist Neurofeedbacktraining eine wirksame Therapiemethode zur Behandlung von ADHS? Ein Überblick über aktuelle Befunde Zeitschrift für Neuropsychologie 2011;22:131-146.
Miller NE. Learning of visceral and glandular responses. Science 1969;163:434-445.
Sherlin LH, Arns M, Lubar J, et al. Neurofeedback and basic learning theory: Implications for research and practice. J Neurother 2011;15:292-304.
Kamiya J. Concious control of brain wave. Psychology Today 1968;1:56-60.
Sterman MB, Egner T. Foundation and practice of neurofeedback for the treatment of epilepsy. Appl Psychophysiol Biofeedback 2006;31:21-35.
Sterman MB, Wyrwicka W, Howe R. Behavioral and neurophysiological studies of the sensorimotor rhythm in the cat. Electroencephalogr Clin Neurophysiol 1969;27:678-679.
Sterman MB, Goodman SJ, Kovalesky RA. Effects of sensorimotor EEG feedback training on seizure susceptibility in the rhesus monkey. Exp Neurol 1978;62:735-747.
Sterman MB, Macdonald LR, Stone RK. Biofeedback training of the sensorimotor electroencephalogram rhythm in man: effects on epilepsy. Epilepsia 1974;15:395-416.
Lubar JF, Shouse MN. EEG and behavioral changes in a hyperkinetic child concurrent with training of the sensorimotor rhythm (SMR): a preliminary report. Biofeedback Self Regul 1976;1:293-306.
Shouse MN, Lubar JF. Operant conditioning of EEG rhythms and ritalin in the treatment of hyperkinesis. Biofeedback Self Regul 1979;4:299-312.
Berger H. Über das Elektrenkephalogramm des Menschen. Archiv für Psychiatrie und Nervenkrankheiten 1929;87:527-570.
Banaschewski T, Brandeis D. Annotation: what electrical brain activity tells us about brain function that other techniques cannot tell us — a child psychiatric perspective. J Child Psychol Psychiatry 2007;48:415-435.
Clarke AR, Barry RJ, Dupuy FE, et al. Behavioural differences between EEG-defined subgroups of children with Attention-Deficit/Hyperactivity Disorder. Clin Neurophysiol 2011;122:1333-1341.
Heinrich H, Gevensleben H, Freisleder FJ, Moll GH, Rothenberger A. Training of slow cortical potentials in attention-deficit/hyperactivity disorder: evidence for positive behavioral and neurophysiological effects. Biol Psychiatry 2004;55:772-775.
Banaschewski T, Brandeis D, Heinrich H, Albrecht B, Brunner E, Rothenberger A. Questioning inhibitory control as the specific deficit of ADHD-evidence from brain electrical activity. J Neural Transm 2004;111:841-864.
Banaschewski T, Brandeis D, Heinrich H, Albrecht B, Brunner E, Rothenberger A. Association of ADHD and conduct disorder — brain electrical evidence for the existence of a distinct subtype. J Child Psychol Psychiatry 2003;44:356-376.
Leins U, Goth G, Hinterberger T, Klinger C, Rumpf N, Strehl U. Neurofeedback for children with ADHD: a comparison of SCP and Theta/Beta protocols. Appl Psychophysiol Biofeedback 2007;32:73-88.
Gevensleben H, Holl B, Albrecht B, et al. Is neurofeedback an efficacious treatment for ADHD? A randomised controlled clinical trial. J Child Psychol Psychiatry 2009;50:780-789.
Levesque J, Beauregard M, Mensour B. Effect of neurofeedback training on the neural substrates of selective attention in children with attention-deficit/hyperactivity disorder: a functional magnetic resonance imaging study. Neurosci Lett 2006;394:216-221.
Linden M, Habib T, Radojevic V. A controlled study of the effects of EEG biofeedback on cognition and behavior of children with attention deficit disorder and learning disabilities. Biofeedback Self Regul 1996;21:35-49.
Strehl U, Leins U, Goth G, Klinger C, Hinterberger T, Birbaumer N. Self-regulation of slow cortical potentials: a new treatment for children with attention-deficit/hyperactivity disorder. Pediatrics 2006;118:e1530-e1540.
Fuchs T, Birbaumer N, Lutzenberger W, Gruzelier JH, Kaiser J. Neurofeedback treatment for attention-deficit/hyperactivity disorder in children: a comparison with methylphenidate. Appl Psychophysiol Biofeedback 2003;28:1-12.
Monastra VJ, Monastra DM, George S. The effects of stimulant therapy, EEG biofeedback, and parenting style on the primary symptoms of attention-deficit/hyperactivity disorder. Appl Psychophysiol Biofeedback 2002;27:231-249.
Drechsler R, Straub M, Doehnert M, Heinrich H, Steinhausen HC, Brandeis D. Controlled evaluation of a neurofeedback training of slow cortical potentials in children with Attention Deficit/Hyperactivity Disorder (ADHD). Behav Brain Funct 2007;3:35.
Rossiter T. The effectiveness of neurofeedback and stimulant drugs in treating AD/HD: part II. Replication. Appl Psychophysiol Biofeedback 2004;29:233-243.
Thompson L, Thompson M. Neurofeedback combined with training in metacognitive strategies: effectiveness in students with ADD. Appl Psychophysiol Biofeedback 1998;23:243-263.
Perreau-Linck E, Lessard N, Lévesque J, Beauregard M. Effects of neurofeedback training on inhibitory capacities in ADHD children: a single-blind, randomized, placebo-controlled study. J Neurother 2010;14:229-242.
Mayer K, Wyckoff SR, Schulz U, Strehl U. Neurofeedback for adult attention-deficit/hyperactivity disorder: investigation of slow cortical potential neurofeedback — preliminary results. J Neurother 2012;16:37-45.
Rossiter T. The effectiveness of neurofeedback and stimulant drugs in treating AD/HD: Part I. Review of methodological issues. Appl Psychophysiol Biofeedback 2004;29:95-112.
Debeus R, Kaiser DA. Neurofeedback with children with attention deificit: a randomized double-blind placebo-controlled study. In: Coben R, Evans JR, eds. Neurofeedback and neuromodulation techniques and applications. London: Academic Press, 2011:128-148.
Rossiter TR, LaVaque TJ. A comparison of EEG biofeedback and psychostimulants in theating attention deficit/hyperactivity disorder. J Neurother 1995;1:48-59.
Holtmann M, Grasmann D, Cionek-Szpak E, et al. Spezifische Wirksamkeit von Neurofeedback auf die Impulsivität bei ADHS. Kindheit und Entwicklung 2009;18:95-104.
Brandeis D. Neurofeedback training in ADHD: more news on specificity. Clin Neurophysiol 2011;122:856-857.
Wangler S, Gevensleben H, Albrecht B, et al. Neurofeedback in children with ADHD: specific event-related potential findings of a randomized controlled trial. Clin Neurophysiol 2011;122:942-950.
Gevensleben H, Holl B, Albrecht B, et al. Distinct EEG effects related to neurofeedback training in children with ADHD: a randomized controlled trial. Int J Psychophysiol 2009;74:149-157.
Cannon R, Lubar J, Congedo M, Thornton K, Towler K, Hutchens T. The effects of neurofeedback training in the cognitive division of the anterior cingulate gyrus. Int J Neurosci 2007;117:337-357.
Cannon R, Congedo M, Lubar J, Hutchens T. Differentiating a network of executive attention: LORETA neurofeedback in anterior cingulate and dorsolateral prefrontal cortices. Int J Neurosci 2009;119:404-441.
Beauregard M, Levesque J. Functional magnetic resonance imaging investigation of the effects of neurofeedback training on the neural bases of selective attention and response inhibition in children with attention-deficit/hyperactivity disorder. Appl Psychophysiol Biofeedback 2006;31:3-20.
Gevensleben H, Holl B, Albrecht B, et al. Neurofeedback training in children with ADHD: 6-month follow-up of a randomised controlled trial. Eur Child Adolesc Psychiatry 2010;19:715-724.
Wangler C, Schafer M, Schirrmacher R, Bartenstein P, Wangler B. DOTA derivatives for site-specific biomolecule-modification via click chemistry: synthesis and comparison of reaction characteristics. Bioorg Med Chem 2011;19:3864-3874.
Doehnert M, Brandeis D, Straub M, Steinhausen HC, Drechsler R. Slow cortical potential neurofeedback in attention deficit hyperactivity disorder: is there neurophysiological evidence for specific effects? J Neural Transm 2008;115:1445-1456.
Kropotov JD, Grin-Yatsenko VA, Ponomarev VA, Chutko LS, Yakovenko EA, Nikishena IS. ERPs correlates of EEG relative beta training in ADHD children. Int J Psychophysiol 2005;55:23-34.
McGough J, McCracken J, Swanson J, et al. Pharmacogenetics of methylphenidate response in preschoolers with ADHD. J Am Acad Child Adolesc Psychiatry 2006;45:1314-1322.
Vitiello B, Abikoff HB, Chuang SZ, et al. Effectiveness of methylphenidate in the 10-month continuation phase of the Preschoolers with Attention-Deficit/Hyperactivity Disorder Treatment Study (PATS). J Child Adolesc Psychopharmacol 2007;17:593-604.
Gani C, Birbaumer N, Strehl U. Long term effects after feedback of slow cortical potentials and of theta-beta-amplitudes in children with attention-deficit/hyperactivity disorder (ADHD). IJBEM 2008;10:209-232.
Arns M, Drinkenburg W, Leon Kenemans J. The Effects of QEEG-Informed Neurofeedback in ADHD: An Open-Label Pilot Study. Appl Psychophysiol Biofeedback 2012;xx:xx-xx.
Kaiser DA, Othmer S. Effect of neurofeedback on variables of attention in a large multi-center trial. J Neurother 2000;4:5-15.
Acknowledgments
This review is part of the formative phase for a research project financed by the Brazilian National Counsel of Technological and Scientific Development (process no. 483934/2010-0). Dr. Tais S. Moriyama receives financial support from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil. Authors declare no real or perceived conflict of interest, full conflict of interest disclosure is available in the electronic supplementary material for this article.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.
Author information
Authors and Affiliations
Corresponding author
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
ESM 1
(PDF 339 kb)
Rights and permissions
About this article
Cite this article
Moriyama, T.S., Polanczyk, G., Caye, A. et al. Evidence-Based Information on the Clinical Use of Neurofeedback for ADHD. Neurotherapeutics 9, 588–598 (2012). https://doi.org/10.1007/s13311-012-0136-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13311-012-0136-7