
Abstract
To compare the outcomes of three-port and four-port laparoscopic cholecystectomy. In compliance with PRISMA statement standards, electronic databases were searched to identify all comparative studies investigating outcomes of three-port vs four-port laparoscopic cholecystectomy. Two techniques were compared using direct comparison meta-analysis model. The risks of type 1 or type 2 error in the meta-analysis model were assessed using trial sequential analysis model. The certainty of evidence was assessed using GRADE system. Random effects modelling was applied to calculate pooled outcome data. Analysis of 2524 patients from 17 studies showed that both techniques were comparable in terms of operative time (MD:− 0.13, P = 0.88), conversion to open operation (OR:0.80, P = 0.43), gallbladder perforation (OR: 1.43, P = 0.13), bleeding from gallbladder bed (OR:0.81, P = 0.34), bile duct injury (RD: 0.00, P = 0.97), iatrogenic visceral injury (RD: − 0.00, P = 0.81), bile or stone spillage (OR:1.67, P = 0.08), port site infection (OR: 0.90, P = 0.76), port site hernia (RD: 0.00, P = 0.89), port site haematoma (RD: − 0.01, P = 0.23), port site seroma (RD: 0.00, P = 1.00), and need for reoperation (RD: − 0.00, P = 0.94). However, the three-port technique was associated with lower VAS pain score at 12 h (MD: − 0.66, P < 0.00001) and 24 h (MD: − 0.54, P < 0.00001) postoperatively, shorter length of hospital stay (MD:-0.09, P = 0.41), and shorter time to return to normal activities (MD: − 0.79, P = 0.02). Trial sequential analysis confirmed that the meta-analysis was conclusive with no significant risks of type 1 or type 2 error. Robust evidence (level 1 with high certainty) suggests that in an elective setting with uncomplicated cholelithiasis as indication for cholecystectomy, three-port laparoscopic cholecystectomy is comparable with the four-port technique in terms of procedural and morbidity outcomes and may be associated with less postoperative pain, shorter length of hospital stay and shorter time to return to normal activities.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Laparoscopic cholecystectomy is the gold standard procedure for symptomatic cholelithiasis and other benign diseases of gallbladder. It was first performed in 1987 [1], and very soon after that it replaced the open approach due to fewer incision-related complications, less postoperative pain, and shorter length of hospital stay [2, 3]. Laparoscopic cholecystectomy is conventionally performed using four laparoscopic ports. Despite the observed benefits of the standard four-port technique, there have been many efforts to make laparoscopic cholecystectomy even less invasive by reducing the size or number of ports to reduce the postoperative pain and analgesia requirement.
Single-incision laparoscopic cholecystectomy initially gained popularity in terms of cosmetic outcomes and pain reduction; however, it lost its popularity due to higher risks of complications in comparison with the standard technique [4]. Three-port laparoscopic cholecystectomy has been proposed as an alternative to standard four-port technique. In the three-port technique, the fourth or lateral port which is normally used to retract the fundus of gallbladder is omitted. The outcomes of three-port and four-port laparoscopic cholecystectomy have been compared by reasonable number of randomised and non-randomised studies supporting the rationale for conducting a comprehensive systematic review.
We aimed to conduct a comprehensive systematic review using meta-analytical and trial sequential analytical models to compare the outcomes of three-port and four-port laparoscopic cholecystectomy. We also aimed to perform trial sequential analysis to assess the conclusiveness of the meta-analysis.
PICOS (participants, interventions, comparisons, outcomes, and study design) research question
In patients undergoing laparoscopic cholecystectomy, is there any difference between three-port and four-port techniques in terms of perioperative outcomes reported in a comprehensive systematic review using meta-analytical and trial sequential analytical models?
Methods
This study was conducted following a predefined protocol in compliance with Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement standards [5].
Objectives
The objectives of the current study were:
-
To compare perioperative outcomes of three-port and four-port laparoscopic cholecystectomy using direct comparison meta-analysis model [6].
-
To assess the risk of type 1 or type 2 error in the meta-analysis model and to assess if the meta-analysis is conclusive to inform decision-making using trial sequential analysis model [7].
-
To assess the certainty of the available evidence using the Grading of Recommendation, Assessment, Development and Evaluation (GRADE) system [8].
Eligibility criteria
Study design
All randomised controlled trials (RCTs) and comparative cohort studies (retrospective or prospective) comparing the outcomes of three-port and four-port laparoscopic cholecystectomy were considered eligible for inclusion. Case control studies, case series, systematic reviews, review articles and case reports were excluded.
Population
All participants of any age or gender undergoing laparoscopic cholecystectomy were considered eligible for inclusion. The indications of interest for cholecystectomy included cholelithiasis, uncomplicated cholecystitis, and gallbladder polyp. Both elective and emergency cases were included. The participants who underwent cholecystectomy due to gallbladder perforation, gallbladder empyema, choledocholithiasis, and gallbladder malignancy were excluded.
Intervention and comparison
Laparoscopic cholecystectomy using three ports was considered as intervention of interest and laparoscopic cholecystectomy using four ports was considered as comparison of interest.
Outcomes
The outcomes of interest included operative time, conversion to open operation, gallbladder perforation, bleeding from gallbladder bed, bile duct injury, iatrogenic visceral injury, bile or stone spillage, port site infection, port site hernia, port site haematoma, port site seroma, need for reoperation, visual analog scale (VAS) pain score at 12 h and 24 h postoperatively, length of hospital stay, and time to return to normal activities.
Search methods
Two independent authors with experience in evidence synthesis used appropriate keywords, thesaurus headings, search limits and operators to develop a comprehensive search strategy (Appendix I). The following sources were searched:
Electronic databases
The Cochrane Central Register of Controlled Trials (CENTRAL), Medical Literature Analysis and Retrieval System Online (MEDLINE), Excerpta Medica database (EMBASE), Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Scopus.
Sources for unpublished or on-going studies
System for Information on Grey Literature, European Association for Grey Literature Exploitation, International Standard Randomised Controlled Trial Number Registry, World Health Organization International Clinical Trials Registry, and ClinicalTrials.gov.
Other sources
Reference lists of relevant reviews and articles.
The search was last applied on 25 October 2020 and the search strategy had no language restrictions.
Selection of studies
The titles and abstracts of the articles identified through application of the above search strategy were screened by two independent authors, the full-texts of relevant articles were retrieved and studies that met the eligibility criteria of the current review were selected. Disagreements in selection of eligible studies between the first two authors were resolved by involving a separate third author.
Data extraction and management
An online data collection sheet consistent with Cochrane’s data collection form was created using random pilot-testing technique by two independent authors. The disagreements were resolved by involving a separate third author. The following data were extracted from each study: First author’s name, year, country of origin, and journal of the published study, study design, sample size, description of included participants, age, gender, operative time, conversion to open operation, gallbladder perforation, bleeding from gallbladder bed, bile duct injury, iatrogenic visceral injury, bile or stone spillage, port site infection, port site hernia, port site haematoma, port site seroma, need for reoperation, VAS pain score at 12 h and 24 h postoperatively, length of hospital stay, and time to return to normal activities.
Assessment of risk of bias in included studies
Two independent authors evaluated the methodological quality of the included studies using the following tools:
Cochrane tool for assessing the risk of bias of randomised trials
This tool evaluates the methodological quality of randomised controlled trials in terms of selection, performance, detection, attrition, reporting and other sources of bias [9].
Risk of bias in non-randomized studies—of interventions (ROBINS-I) assessment tool
This tool evaluates the methodological quality of observational studies in terms of bias due to confounding, bias in selection of participants into the study, bias in classification of interventions, bias due to deviations from intended interventions, bias due to missing data, bias in measurement of outcomes, and bias in selection of the reported results [10].
A separate third author was involved in case of disagreements between the first two authors.
Statistical analyses
Review Manager 5.3 (RevMan, Version 5.3. Copenhagen, 2014) software was used for comparison meta-analysis model and trial sequential analysis (TSA) (TSA software 0.9.5.5 Beta, Copenhagen Trial Unit, Denmark) software was used for trial sequential analysis model.
Comparison meta-analysis model
Intention to treat information data from the included studies were used for data analysis. Random effects modelling with consideration of individual patients as unit of analysis was utilised to calculate pooled odds ratio (OR) and pooled mean difference (MD) as summary measures for dichotomous and continuous outcomes, respectively. When more than a third of the included studies reported zero event (no occurrence of the outcome event) in both 3-port and 4-port groups, the pooled risk difference (RD) was calculated. The statistical heterogeneity was measured as I2 using Cochran Q test (χ2) and it was classified as low heterogeneity when I2 was 0–25%, moderate heterogeneity when I2 was 25–75%, and high heterogeneity when I2 was 75–100%. We planned to generate funnel plots for the outcomes reported by at least 10 studies and we planned to assess the likelihood of publication bias by assessing the symmetry of the funnel plots.
Trial sequential analysis model
Trial sequential analysis (TSA) of data from randomised controlled trials was conducted when an outcome was reported by at least five randomised trials. To assess the likelihood of type 1 error, O’Brien-Fleming α-spending function was used to adjust the thresholds for the Z-values. Furthermore, the Z values were penalised using the iterated logarithm law. To assess the likelihood of type 2 error, the β-spending function and futility boundaries were used. Random effects models were used for TSA and constant continuity correction was used to deal with the no event RCTs. The required information size (IS) was computed according to 10% relative risk reduction between the 3-port and 4-port groups and achievement of 80% power.
All statistical analyses were modelled based on 95% confidence level to demonstrate statistical significance.
Additional analyses
The following additional analyses were planned:
Sensitivity analyses
Sensitivity analyses were modelled for outcomes reported by at least five studies. These included elimination of one study at a time followed by repeating the analyses, independent calculation of risk ratio (RR) and risk difference (RD) for dichotomous outcomes, and separate analyses for studies with low overall risk of bias.
Subgroup analyses
Subgroup analyses were planned based on randomised controlled trials, observational studies, and emergency procedures.
Summary of findings table
The quality and certainty of available evidence for each outcome was graded as very low, low, moderate, or high in terms across studies risk of bias, directness of evidence, heterogeneity, precision of effects estimates, and risk of publication bias using the GRADE system [8]. The results were presented in a 'Summary of findings’ table.
Results
Results of the search
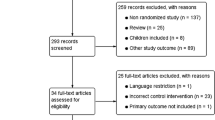
Running the search strategy described above resulted in 290 articles among which 278 studies were excluded directly, because they were not relevant to the topic of this study. After reviewing the full-text of remaining relevant articles, five more article were excluded, because one article was a review article and four articles had unclear study design and methodology. The remaining 17 articles [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27] met the eligibility criteria of this study. These included 12 randomised controlled trials [11,12,13,14,15,16,17,18, 20, 23, 24, 26] and five comparative observational studies [19, 21, 22, 25, 27] enrolling a total of 2524 patients. Figure 1 demonstrates the study flow chart and Table 1 highlights the baseline characteristics of the included studies.

PRISMA flow chart
Risk of bias in included studies
Figure 2 highlights the outcomes of methodological quality assessment of the included studies based on the Cochrane tool and ROBINS-I tool.

Risk of bias summary and graph showing authors’ judgements about each risk of bias item for: a randomised controlled trials b observational studies
Results of comparison meta-analysis model (Fig. 3).





Results of comparison meta-analysis model: a operative time; b conversion to open operation; c gallbladder perforation; d bleeding from gallbladder bed; e bile duct injury; f iatrogenic visceral injury; g bile or stone spillage; h port site infection; i port site hernia; j port site haematoma; k port site seroma; l need for reoperation; m VAS pain score at 12 h postoperatively; n VAS pain score at 24 h postoperatively; o length of hospital stay; p time to return to normal activities
Operative time
All studies
Analysis of 2111 patients from 13 studies showed no difference in operative time between the two groups (MD: − 0.13, 95% CI − 1.78 to 1.53, P = 0.88). The level of between-study heterogeneity was moderate (I2 = 57%, P = 0.005). The likelihood of publication bias was low based on funnel plot.
Randomised controlled trials
Analysis of 961 patients from nine RCTs showed no difference in operative time between the two groups (MD: − 0.03, 95% CI − 2.28 to 2.22, P = 0.98). The level of between-study heterogeneity was moderate (I2 = 55%, P = 0.02). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1a).
Observational studies
Analysis of 1150 patients from four observational studies showed no difference in operative time between the two groups (MD: − 0.23, 95% CI − 3.15 to 2.68, P = 0.88). The level of between-study heterogeneity was moderate (I2 = 69%, P = 0.02). The GRADE certainty of the evidence was judged to be moderate (Supplementary Table 1a).
Conversion to open operation
All studies
Analysis of 2150 patients from 12 studies showed no difference in the risk of conversion to open operation between the two groups (OR: 0.80, 95% CI 0.45–1.41, P = 0.43). The level of between-study heterogeneity was low (I2 = 0%, P = 0.72). The likelihood of publication bias was low based on funnel plot.
Randomised controlled trials
Analysis of 1000 patients from eight RCTs showed no difference in the risk of conversion to open operation between the two groups (OR: 0.76, 95% CI 0.36–1.62, P = 0.48). The level of between-study heterogeneity was low (I2 = 0%, P = 0.57). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1b).
Observational studies
Analysis of 1150 patients from four observational studies showed no difference in the risk of conversion to open operation between the two groups (OR: 0.84, 95% CI 0.35–2.02, P = 0.70). The level of between-study heterogeneity was low (I2 = 0%, P = 0.51). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1b).
Gallbladder perforation
All studies
Analysis of 870 patients from six studies showed no difference in the risk of gallbladder perforation between the two groups (OR: 1.43, 95% CI 0.90–2.29, P = 0.13). The level of between-study heterogeneity was low (I2 = 0%, P = 0.92).
Randomised controlled trials
Analysis of 470 patients from five RCTs showed no difference in the risk of gallbladder perforation between the two groups (OR: 1.33, 95% CI 0.78–2.26, P = 0.29). The level of between-study heterogeneity was low (I2 = 0%, P = 0.90). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1c).
Observational studies
Analysis of 400 patients from one observational study showed no difference in the risk of gallbladder perforation between the two groups (OR: 1.88, 95% CI 0.68–5.19, P = 0.22). The GRADE certainty of the evidence was judged to be low (Supplementary Table 1c).
Bleeding from gallbladder bed
All studies
Analysis of 1164 patients from eight studies showed no difference in the risk of bleeding form gallbladder bed between the two groups (OR: 0.81, 95% CI 0.53–1.24, P = 0.34). The level of between-study heterogeneity was low (I2 = 0%, P = 0.87).
Randomised controlled trials
Analysis of 764 patients from seven RCTs showed no difference in the risk of bleeding form gallbladder bed between the two groups (OR: 0.71, 95% CI 0.44–1.14, P = 0.15). The level of between-study heterogeneity was low (I2 = 0%, P = 0.96). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1d).
Observational studies
Analysis of 400 patients from one observational study showed no difference in the risk of bleeding form gallbladder bed between the two groups (OR: 1.40, 95% CI 0.55–3.55, P = 0.48). The GRADE certainty of the evidence was judged to be moderate (Supplementary Table 1d).
Bile duct injury
All studies
Analysis of 2310 patients from 14 studies showed no difference in the risk of bile duct injury between the two groups (RD: 0.00, 95% CI − 0.01 to 0.01, P = 0.97). The level of between-study heterogeneity was low (I2 = 0%, P = 1.00). The likelihood of publication bias was low based on funnel plot.
Randomised controlled trials
Analysis of 1160 patients from 10 RCTs showed no difference in the risk of bile duct injury between the two groups (RD: 0.00, 95% CI − 0.01 to 0.01, P = 0.89). The level of between-study heterogeneity was low (I2 = 0%, P = 1.00). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1e).
Observational studies
Analysis of 1150 patients from four observational studies showed no difference in the risk of bile duct injury between the two groups (RD: − 0.00, 95% CI − 0.01 to 0.01, P = 0.88). The level of between-study heterogeneity was low (I2 = 0%, P = 0.79). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1e).
Iatrogenic visceral injury
All studies
Analysis of 973 patients from seven studies showed no difference in the risk of iatrogenic visceral injury between the two groups (RD: − 0.00, 95% CI − 0.01 to 0.01, P = 0.83). The level of between-study heterogeneity was low (I2 = 0%, P = 0.95).
Randomised controlled trials
Analysis of 518 patients from five RCTs showed no difference in the risk of iatrogenic visceral injury between the two groups (RD: − 0.00, 95% CI − 0.02 to 0.01, P = 0.81). The level of between-study heterogeneity was low (I2 = 0%, P = 0.89). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1f).
Observational studies
Analysis of 455 patients from two observational studies showed no difference in the risk of iatrogenic visceral injury between the two groups (RD: − 0.00, 95% CI − 0.01 to 0.01, P = 0.94). The level of between-study heterogeneity was low (I2 = 0%, P = 0.52). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1f).
Bile or stone spillage
All studies
Analysis of 754 patients from four studies showed no difference in the risk of bile or stone spillage between the two groups (OR: 1.67, 95% CI 0.94–2.98, P = 0.08). The level of between-study heterogeneity was low (I2 = 0%, P = 0.71).
Randomised controlled trials
Analysis of 354 patients from three RCTs showed no difference in the risk of bile or stone spillage between the two groups (OR: 1.85, 95% CI 0.96–3.55, P = 0.07). The level of between-study heterogeneity was low (I2 = 0%, P = 0.57). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1g).
Observational studies
Analysis of 400 patients from one observational study showed no difference in the risk of bile or stone spillage between the two groups (OR: 1.21, 95% CI 0.36–4.02, P = 0.76). The GRADE certainty of the evidence was judged to be low (Supplementary Table 1g).
Port site infection
All studies
Analysis of 1290 patients from eight studies showed no difference in the risk of port site infection between the two groups (OR: 0.90, 95% CI 0.46–1.77, P = 0.76). The level of between-study heterogeneity was low (I2 = 0%, P = 0.91).
Randomised controlled trials
Analysis of 795 patients from seven RCTs showed no difference in the risk of port site infection between the two groups (OR: 0.95, 95% CI 0.44–2.06, P = 0.91). The level of between-study heterogeneity was low (I2 = 0%, P = 0.85). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1h).
Observational studies
Analysis of 495 patients from one observational study showed no difference in the risk of port site infection between the two groups (OR: 0.75, 95% CI 0.18–3.02, P = 0.68). The GRADE certainty of the evidence was judged to be moderate (Supplementary Table 1h).
Port site hernia
All studies
Analysis of 458 patients from four studies showed no difference in the risk of port site hernia between the two groups (RD: 0.00, 95% CI − 0.01 to 0.02, P = 0.89). The level of between-study heterogeneity was low (I2 = 0%, P = 0.87).
Randomised controlled trials
Analysis of 458 patients from four RCTs showed no difference in the risk of port site hernia between the two groups (RD: 0.00, 95% CI − 0.01 to 0.02, P = 0.89). The level of between-study heterogeneity was low (I2 = 0%, P = 0.87). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1i).
Observational studies
This outcome was not reported by observational studies.
Port site haematoma
All studies
Analysis of 893 patients from four studies showed no difference in the risk of port site haematoma between the two groups (RD: − 0.01, 95% CI − 0.02 to 0.00, P = 0.23). The level of between-study heterogeneity was low (I2 = 0%, P = 0.72).
Randomised controlled trials
Analysis of 398 patients from three RCTs showed no difference in the risk of port site haematoma between the two groups (RD: − 0.00, 95% CI − 0.02 to 0.02, P = 0.89). The level of between-study heterogeneity was low (I2 = 0%, P = 0.83). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1j).
Observational studies
Analysis of 495 patients from one observational study showed no difference in the risk of port site haematoma between the two groups (RD: − 0.01, 95% CI − 0.03 to 0.00, P = 0.12). The GRADE certainty of the evidence was judged to be moderate (Supplementary Table 1j).
Port site seroma
All studies
Analysis of 200 patients from one study showed no difference in the risk of port site seroma between the two groups (RD: 0.00, 95% CI − 0.04 to 0.04, P = 1.00).
Randomised controlled trials
Analysis of 200 patients from one RCT showed no difference in the risk of port site seroma between the two groups (RD: 0.00, 95% CI − 0.04 to 0.04, P = 1.00). The GRADE certainty of the evidence was judged to be moderate (Supplementary Table 1k).
Observational studies
This outcome was not reported by observational studies.
Need for reoperation
All studies
Analysis of 575 patients from four studies showed no difference in the need for reoperation between the two groups (RD: − 0.00, 95% CI − 0.01 to 0.01, P = 0.94). The level of between-study heterogeneity was low (I2 = 0%, P = 0.94).
Randomised controlled trials
Analysis of 120 patients from two RCTs showed no difference in the need for reoperation between the two groups (RD: 0.00, 95% CI − 0.04 to 0.04, P = 1.00). The level of between-study heterogeneity was low (I2 = 0%, P = 1.00). The GRADE certainty of the evidence was judged to be moderate (Supplementary Table 1l).
Observational studies
Analysis of 455 patients from two observational studies showed no difference in the need for reoperation between the two groups (RD: − 0.00, 95% CI − 0.01 to 0.01, P = 0.94). The level of between-study heterogeneity was low (I2 = 0%, P = 0.52). The GRADE certainty of the evidence was judged to be moderate (Supplementary Table 1l).
VAS pain score at 12 h postoperatively
All studies
Analysis of 523 patients from six studies showed lower VAS pain score at 12 h postoperatively in the 3-port group (MD: − 0.66, 95% CI − 0.87 to 0.45, P < 0.00001). The level of between-study heterogeneity was low (I2 = 0%, P = 0.91).
Randomised controlled trials
Analysis of 523 patients from six RCTs showed lower VAS pain score at 12 h postoperatively in the 3-port group (MD: − 0.66, 95% CI − 0.87 to 0.45, P < 0.00001). The level of between-study heterogeneity was low (I2 = 0%, P = 0.91). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1m).
Observational studies
This outcome was not reported by observational studies.
VAS pain score at 24 h postoperatively
All studies
Analysis of 439 patients from four studies showed lower VAS pain score at 24 h postoperatively in the 3-port group (MD: − 0.54, 95% CI − 0.68 to 0.41, P < 0.00001). The level of between-study heterogeneity was low (I2 = 0%, P = 0.47).
Randomised controlled trials
Analysis of 439 patients from four RCTs showed lower VAS pain score at 24 h postoperatively in the 3-port group (MD: − 0.54, 95% CI − 0.68 to 0.41, P < 0.00001). The level of between-study heterogeneity was low (I2 = 0%, P = 0.47). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1n).
Observational studies
This outcome was not reported by observational studies.
Length of hospital stay
All studies
Analysis of 921 patients from eight studies showed no difference in length of hospital stay between the two groups (MD: − 0.09, 95% CI − 0.29 to 0.12, P = 0.41). The level of between-study heterogeneity was high (I2 = 94%, P < 0.00001).
Randomised controlled trials
Analysis of 521 patients from seven RCTs showed shorter length of hospital stay in the 3-port group (MD: − 0.21, 95% CI − 0.29 to 0.13, P < 0.00001). The level of between-study heterogeneity was moderate (I2 = 56%, P = 0.03). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1o).
Observational studies
Analysis of 400 patients from one observational study showed longer length of hospital stay in the 3-port group (MD: 0.80, 95% CI 0.62–0.98, P < 0.00001). The GRADE certainty of the evidence was judged to be low (Supplementary Table 1o).
Time to return to normal activities
All studies
Analysis of 373 patients from four studies showed shorter time to return to normal activities in the 3-port group (MD: − 0.79, 95% CI − 1.47 to 0.10, P = 0.02). The level of between-study heterogeneity was high (I2 = 92%, P < 0.00001).
Randomised controlled trials
Analysis of 373 patients from four RCTs showed shorter time to return to normal activities in the 3-port group (MD: − 0.79, 95% CI − 1.47 to 0.10, P = 0.02). The level of between-study heterogeneity was high (I2 = 92%, P < 0.00001). The GRADE certainty of the evidence was judged to be high (Supplementary Table 1p).
Observational studies
This outcome was not reported by observational studies.
Additional analyses
Sensitivity analyses
Elimination of one study at a time from the analyses did not change the effect size and overall heterogeneity for any of the outcomes except length of hospital stay, where removal of a single observational study (Akay et al. [21]) changed the direction of the effect size in favour of 3-port group and reduced the heterogeneity significantly. Therefore, considering that Akay et al. [21] is an outlier in analysis of length of hospital stay, the results of the analysis without Akay et al. [21] is more robust. Independent calculation of RR and risk difference RD for dichotomous outcomes did not affect the results for any of the outcomes. Finally, separate analyses of studies with low overall risk of bias did not change the effect size and overall heterogeneity for any of the outcomes except length of hospital stay, where removal of a single observational study (Akay et al. [21]) changed the direction of the effect size in favour of 3-port group.
Subgroup analyses
The results of subgroup analyses based on randomised controlled trials and observational studies have been reported in the outcomes section. The available data from the included studies were not adequate for subgroup analysis based on emergency procedures.
Results of trial sequential analysis model (Fig. 4).





Results of trial sequential analysis model: a operative time; b conversion to open operation; c gallbladder perforation; d bleeding from gallbladder bed; e bile duct injury; f iatrogenic visceral injury; g port site infection; h VAS pain score at 12 h postoperatively; i length of hospital stay
Operative time
The information size for operative time was calculated at 796 patients. The conventional boundaries were not crossed by Z-curve after the information size was reached and the absolute number for penalised Z value remained smaller than 1.96 in both sides; therefore, the meta-analysis was conclusive and the risk of type 2 error was minimal.
Conversion to open operation
The information size for conversion to open operation was calculated at 872 patients. The conventional boundaries were not crossed by Z-curve after the information size was reached and the absolute number for penalised Z value remained smaller than 1.96 in both sides; therefore, the meta-analysis was conclusive and the risk of type 2 error was minimal.
Gallbladder perforation
The information size for gallbladder perforation was calculated at 872 patients. The information size was not reached for this outcome and the conventional boundaries, alpha-spending boundaries, and futility boundaries were not crossed by Z-curve; therefore, the meta-analysis was not conclusive and the risk of type 2 error cannot be excluded.
Bleeding from gallbladder bed
The information size for bleeding from gallbladder bed was calculated at 872 patients. The information size was not reached for this outcome. The conventional boundaries and alpha-spending boundaries were not crossed by Z-curve but the futility boundaries were crossed by Z-curve and the absolute number for penalised Z value remained smaller than 1.96 in both sides; therefore, the meta-analysis was conclusive and the risk of type 2 error was minimal.
Bile duct injury
The information size for bile duct injury was calculated at 872 patients. The conventional boundaries were not crossed by Z-curve after the information size was reached and the absolute number for penalised Z value remained smaller than 1.96 in both sides; therefore, the meta-analysis was conclusive and the risk of type 2 error was minimal.
Iatrogenic visceral injury
The information size for iatrogenic visceral injury was calculated at 933 patients. The information size was not reached for this outcome. The conventional boundaries and alpha-spending boundaries were not crossed by Z-curve but the futility boundaries were crossed by Z-curve and the absolute number for penalised Z value remained smaller than 1.96 in both sides; therefore, the meta-analysis was conclusive and the risk of type 2 error was minimal.
Port site infection
The information size for port site infection was calculated at 872 patients. The information size was not reached for this outcome. The conventional boundaries and alpha-spending boundaries were not crossed by Z-curve but the futility boundaries were crossed by Z-curve and the absolute number for penalised Z value remained smaller than 1.96 in both sides; therefore, the meta-analysis was conclusive and the risk of type 2 error was minimal.
VAS pain score at 12 h postoperatively
The information size for VAS pain score at 12 h postoperatively was calculated at 226 patients. The Z-curve crossed the conventional boundaries in favour of 3-port technique after the information size was reached and the penalised Z value remained greater than 1.96; therefore, the meta-analysis was conclusive and the risk of type 1 error was minimal.
Length of hospital stay
The information size for length of hospital stay was calculated at 318 patients. The Z-curve crossed the conventional boundaries in favour of 3-port technique after the information size was reached and the penalised Z value remained greater than 1.96; therefore, the meta-analysis was conclusive and the risk of type 1 error was minimal.
Discussion
In this study we compared outcomes of three-port and four-port laparoscopic cholecystectomy using meta-analytical and trial sequential analytical models. Analysis of 2524 patients from 17 comparative studies showed that three-port laparoscopic cholecystectomy is comparable with the four-port technique in terms of procedural and morbidity outcomes and may be associated with less postoperative pain, shorter length of hospital stay and shorter time to return to normal activities. The results remained consistent through sensitivity analyses and separate analyses of randomised and non-randomised studies. TSA confirmed that the meta-analysis was conclusive with no significant risks of type 1 or type 2 error. The overall quality of the available evidence was moderate to high and the GRADE certainty of the available evidence was judged to be high.
The results of current study suggest that omitting the lateral or forth port from the standard four-port laparoscopic cholecystectomy technique does not have negative impact on procedural outcomes. On the other hand, our results suggest that reducing the number of ports from four to three results in less postoperative pain for patients which subsequently explains the shorter length of hospital stay and shorter time to return to normal activities. Although less postoperative pain is an important finding, it is debatable whether shorter hospital stay is clinically important as nowadays most cases of elective laparoscopic cholecystectomy are done as day case procedure.
There is currently no comprehensive meta-analysis in the literature to compare our findings with. Sun et al.[28] conducted a meta-analysis in 2009 including five comparative studies which reported operative time, success rate, postoperative analgesia requirement, and length of hospital stay as outcome measures. [28] Consistent with our findings, Sun et al. reported comparable operative time and success rate between three-port and four-port techniques. Unlike the current study, Sun et al. found no difference between the two groups in terms of analgesia requirement and length of hospital stay [28]. However, as correctly highlighted by the authors at the time of study, the quality of the available evidence and the included studies were not high [28]. In fact, in the current study we had to exclude four out of five studies that had been included in the study by Sun et al. [28] due to inadequate information about their study designs. Owing to publication of adequate number of randomised and non-randomised comparative studies, the current study provides more robust comparative evidence on outcomes of three-port and four-port laparoscopic cholecystectomy.
The safety of three-port laparoscopic cholecystectomy in emergency setting and in cases with complicated gallstone disease remains unanswered in this study as the included population in current study underwent laparoscopic cholecystectomy predominantly for uncomplicated cholelithiasis or gallbladder polyp in elective or semi-elective settings. It can be argued that the fourth port potentially plays a significant role during laparoscopic cholecystectomy in complicated and emergency cases, where severely inflamed or scarred tissue can make tissue dissection more difficult and the fourth port can be used for further retraction of gallbladder.
The current study has strengths and limitations. The strengths of the current study include systematic and objective approach in evidence synthesis, providing evidence from 17 comparative studies of which 12 were randomised controlled trials, low between-study heterogeneity for most of the outcomes, consistency of results through additional analyses, low risks of type 1 and type 2 errors as per trial sequential analysis, and high certainty of evidence as per GRADE system. The limitations of the current study include inadequate data to perform subgroup analysis based on indications for cholecystectomy and based on emergency operations, inability to perform sensitivity analyses and TSA for the outcomes reported by less than five studies, and inability to assess publication bias for the outcomes reported by less than 10 studies.
Conclusion
Robust evidence (Level 1 with high certainty) suggests that in an elective setting with uncomplicated cholelithiasis as indication for cholecystectomy, three-port laparoscopic cholecystectomy is comparable with the four-port technique in terms of procedural and morbidity outcomes and may be associated with less postoperative pain, shorter length of hospital stay and shorter time to return to normal activities. The comparative evidence in emergency setting and in cases with complicated disease remains unanswered.
References
Litynski GS (1999) Profiles in laparoscopy: Mouret, Dubois, and Perissat: the laparoscopic breakthrough in Europe (1987–1988). JSLS 3(2):163–167
Antoniou SA, Antoniou GA, Koch OO, Pointner R, Granderath FA (2014) Meta-analysis of laparoscopic vs open cholecystectomy in elderly patients. World J Gastroenterol 20(46):17626–17634
Coccolini F, Catena F, Pisano M, Gheza F, Fagiuoli S, Di Saverio S et al (2015) Open versus laparoscopic cholecystectomy in acute cholecystitis. Systematic review and meta-analysis. Int J Surg 18:196–204
Arezzo A, Passera R, Forcignanò E, Rapetti L, Cirocchi R, Morino M (2018) Single-incision laparoscopic cholecystectomy is responsible for increased adverse events: results of a meta-analysis of randomized controlled trials. Surg Endosc 32(9):3739–3753
Liberati A, Altman DG, Tetzlaff J et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339:b2700
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (eds) (2019) Cochrane handbook for systematic reviews of interventions, 2nd edn. Wiley, Chichester (UK)
Thorlund K, Engstrøm J, Wetterslev JG, Brok J, Imberger Gluud C (2011) User manual for trial sequential analysis (TSA). Copenhagen Trial Unit, Centre for Clinical Intervention Research, Copenhagen, Denmark. 2011. . p. 1–115. Available at www.ctu.dk/tsa. Accessed 28 Nov 2020
Schünemann H, Brożek J, Guyatt G, Oxman A (2013) GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available at GRADE handbook (gradepro.org). Accessed 28 Nov 2020
Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC. Chapter 8: Assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.1 (updated September 2020). Cochrane, 2020. Available from www.training.cochrane.org/handbook. Accessed 28 Nov 2020
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M et al (2016) ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355:i4919
Koirala R, Gurung T, Rajbhandari A, Rai P (2019) Three-port versus four-port laparoscopic cholecystectomy: a randomized controlled trial. Nepal Med Coll J 21(1):40–43
Mirza AA, Asif M, Sukh N, Saeed A, Jamil K, Zaidi AH (2017) Outcome of three ports versus four ports laparoscopic cholecystectomy in terms of mean operative time, hospital stay and pain. Ann Pak Inst Med Sci 13(2):169–172
Shah SF, Waqar SH, Chaudry MA, Hameed S (2017) Three ports versus four ports laparoscopic cholecystectomy. RMJ 42(3):359–362
Sharma PK, Mehta KS (2017) Three port versus standard four port laparoscopic cholecystectomy—a prospective study. JK Sci 17(1):38–42
Khorgami Z, Shoar S, Anbara T, Soroush A, Nasiri S, Movafegh A et al (2014) A randomized clinical trial comparing 4-port, 3-port, and single-incision laparoscopic cholecystectomy. J Invest Surg 27(3):147–154
Harsha HS, Gunjiganvi M, Singh C, Moirangthem GS (2013) A study of three-port versus four-port laparoscopic cholecystectomy. J Med Soc 27:208–211
Mohamed AE, Zaazou MM (2020) Three-port versus conventional four-port laparoscopic cholecystectomy: a comparative study. Egypt J Surg 39:119–123
Kumar M, Agrawal CS, Gupta RK (2007) Three-port versus standard four-port laparoscopic cholecystectomy: a randomized controlled clinical trial in a community-based teaching hospital in eastern Nepal. JSLS 11(3):358–362
Hashimoto D, Hirota M, Yagi Y, Baba H (2011) Umbilicus saving three-port laparoscopic cholecystectomy. Webmed Cent Laparosc 2(4):WMC001882
Eroler E, Dilektasli E, Tihan D, Duman U, Bayam EM, Erol FM et al (2016) Reducing one port in laparoscopic cholecystectomy: does that really make a difference? Int J Clin Exp Med 9(6):11558–11565
Akay T, Örün S, Leblebici M (2019) Three-port versus standard four-port laparoscopic cholecystectomy: a clinical trial. Laparosc Endosc Surg Sci 26(4):175–180
Al-Azawi D, Houssein N, Rayis AB, McMahon D, Hehir DJ (2007) Three-port versus four-port laparoscopic cholecystectomy in acute and chronic cholecystitis. BMC Surg 13(7):8
Bari S, Islam F, Rather A, Malik A (2019) Three port versus four port laparoscopic cholecystectomy: a prospective comparative clinical study. Int J Res Med Sci 7(8):3054–3059
Kumar A, Kumar D, Gupta P, Shakya JPS (2018) Three port versus four port laparoscopic cholecystectomy: a comparative study. Indian J Appl Res 8(10):18–20
Mayir B, Dogan U, Koc U, Aslaner A, Bılecık T, Ensarı CO et al (2014) Safety and effectiveness of three-port laparoscopic cholecystectomy. Int J Clin Exp Med 7(8):2339–2342
Reshie AA, Rather ZM, Bhat MY, Salroo NA, Majid AN, Ahmed MM (2015) Three port versus four port laparoscopic cholecystectomy: a comparative study. Int J of Adv Res 3:1040–1044
Wilkinson TRV, Mehrotra P, Bansod P, Akhtar M (2017) Three port versus four port laparoscopic cholecystectomy—a prospective study. Int J Med Res Rev 5(03):235–241
Sun S, Yang K, Gao M, He X, Tian J, Ma B (2009) Three-port versus four-port laparoscopic cholecystectomy: meta-analysis of randomized clinical trials. World J Surg 33(9):1904–1908
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Conception and design: TS, SH. Data collection: DAF, SH. Analysis and interpretation: all authors. Writing the article: SH, DAF. Critical revision of the article: all authors. Final approval of the article: all authors. Statistical analysis: SH, AYYM, SH, DAF.
Corresponding author
Ethics declarations
Conflict of interest
All authors included in this work declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix I
Appendix I
Search No | Search strategya |
|---|---|
#1 | Three port: TI,AB,KW |
#2 | Three-port: TI,AB,KW |
#3 | 3-Port: TI,AB,KW |
#4 | 3 Port: TI,AB,KW |
#5 | #1 OR #2 OR #3 OR #4 |
#6 | Four port: TI,AB,KW |
#7 | Four-port: TI,AB,KW |
#8 | 4-Port: TI,AB,KW |
#9 | 4 Port: TI,AB,KW |
#10 | Standard: TI,AB,KW |
#11 | Conventional: TI,AB,KW |
#12 | #6 OR #7 OR #8 OR #9 OR #10 OR #11 |
#13 | MeSH descriptor: [laparoscopic cholecystectomy] explode all trees |
#14 | Laparosco* near2 cholecystectomy: TI,AB,KW |
#15 | Cholecystectomy: TI,AB,KW |
#16 | #13 OR #14 OR #15 |
#17 | #5 AND #11 AND #16 |
Rights and permissions
About this article

Cite this article
Hajibandeh, S., Finch, D.A., Mohamedahmed, A.Y.Y. et al. Meta-analysis and trial sequential analysis of three-port vs four-port laparoscopic cholecystectomy (level 1 evidence). Updates Surg 73, 451–471 (2021). https://doi.org/10.1007/s13304-021-00982-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13304-021-00982-z