
Abstract
Previous studies on the associations of the NFKB1 -94 insertion/deletion polymorphism with cancer risk have produced conflicting results. The purpose of this meta-analysis is to define the effect of the NFKB1 -94 insertion/deletion polymorphism on cancer risk. A search of the literature by PubMed was performed to identify studies based on the predetermined inclusion criteria. Twenty-three studies consisting of 6,494 cases and 9,884 controls were identified and analyzed. Overall, significant association was observed between the polymorphism and cancer risk under all genetic models. Subgroup analysis according to ethnicity and cancer type also detected significant association. The NFKB1 -94 insertion/deletion polymorphism was associated with cancer risk in Asian population (dominant model: OR = 1.52, 95 % CI = 1.17–1.98; recessive model: OR = 1.50, 95 % CI = 1.26–1.79; II vs. DD: OR = 1.90, 95 % CI = 1.37–2.65; ID vs. DD: OR = 1.32, 95 % CI = 1.05–1.66; I vs. D: OR = 1.37, 95 % CI = 1.17–1.60), but not in Caucasian population. In addition, significant associations in OC, HCC, and OSCC were observed, but significant associations were not found in BC and LC. The current meta-analysis suggested that NFKB1 -94 insertion/deletion polymorphism may influence cancer risk in Asian population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cancer is a complicated disease associated with individual genetic backgrounds and external factors such as lifestyle and inflammation [1, 2]. It has been reported that inflammation-associated molecules are associated with a majority of cancer types, and these molecules are activated by various elements related to environment and lifestyle [3].
Nuclear factor kappa B (NFKB) is an important transcription factor and is one of the key regulators of inflammatory mechanisms. NFKB comprises a number of related proteins that bind to a common sequence motif known as the kB site. Various homodimers and heterodimers of p65 and c-Rel or p50 protein subunits form the NFKB that acts on the canonical activation pathway dependent on inhibitor of kB kinase activation. The pathway is triggered by inflammatory cytokines via lipopolysaccharide receptors and the toll-like receptor signals induced by microbial, viral, and chemical exposure [4–7].
NFKB1 gene located on chromosome 4q23–24 and encoded p50 subunit. In the promoter region of NFKB1, there is a special -94 insertion/deletion (I/D) polymorphism (rs28362491) influencing the expression of NFKB1. A previous study found that the activity of I allele was twice as high as that of D allele [8]. In addition, several studies have demonstrated the -94 I/D polymorphism to be associated with increased cancer risk such as prostate cancer, hepatocellular carcinoma, colorectal cancer, gastric cancer, and others [9–13]. The probable mechanism behind the observed association may be related to the expression and activity of NFKB1. However, in other studies, the -94 I/D polymorphism was not observed to be associated with cancer risk [14, 15]. Therefore, we carried out a meta-analysis to clarify the association between this polymorphism and cancer risk.
Materials and methods
Literature search
To identify all articles that examined the association of NFKB1 -94 I/D polymorphism with cancer risk, PubMed database searches were performed using the following keywords: ‘NFKB1,’ ‘polymorphism,’ and ‘cancer’ (up to November 29, 2013). Reference lists in retrieved articles were also screened. Eligible studies should meet the following criteria: (a) case–control studies, (b) detailed genotype data for estimating odds ratio (OR) and 95 % confidence interval (CI), (c) P value on Hardy-Weinberg equilibrium (HWE) of controls must be more than 0.05, and (d) studies published in English. If multiple studies had overlapping or duplicate data, only those with complete data were included.
Data extraction
Two investigators (Xu and Cai) independently evaluated and extracted data. Any controversy on the baseline information was resolved by discussion. For each study, the following information was extracted: first author, year of publication, ethnicity, cancer type, genotyping method, HWE, the numbers of genotyped cases and controls, and genotype distributions of cases and controls, respectively.
Statistical analysis
HWE was tested by the chi-square test, and P < 0.05 was considered as departure from HWE. Heterogeneity among studies was tested using the Q statistics. Based on the heterogeneity test, the overall OR was calculated using fixed or random effects model with 95 % CI to measure the strength of the genetic association. The pooled OR were performed for dominant model (II + ID vs. DD), recessive model (II vs. ID + DD), and other genetic models (II vs. DD, ID vs. DD, and I vs. D), respectively. Subgroup analyses were also performed to test the effects of ethnicity and cancer type. Sensitivity analysis was conducted by removing each study and analyzing the others to ensure no single study was totally responsible for overall results. Begg’s funnel plot and the Egger’s linear regression test were performed to evaluate publication bias of literatures and P < 0.05 was considered significant. All analyses were done with STATA 12.0 software (Stata Corporation, College Station, TX).
Results
Study characteristics
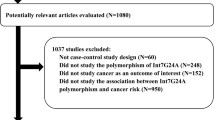
Figure 1 showed the detailed process of identifying eligible studies. A total of 20 articles, including 23 studies, met the inclusion criteria and were included in this meta-analysis. The main characteristics of the studies are listed in Table 1. Among these studies, including 6,494 cancer cases and 9,884 non-cancer controls, there were 14 studies of Asian population and 9 of Caucasian population. There were 3 bladder cancer (BC) studies, 2 prostate cancer (PC) studies, 2 ovarian cancer (OC) studies, 2 lung cancer (LC) studies, 2 hepatocellular carcinoma (HCC) studies, 2 oral squamous cell carcinoma (OSCC) studies, 2 colorectal cancer (CRC) studies, and 8 others.

The detailed process of identifying eligible studies
Quantitative synthesis
The meta-analysis was assessed by a random effects model because the heterogeneity among studies was significant under all genetic models (P < 0.01). The evaluations of the association of NFKB1 -94 I/D polymorphism with cancer risk are shown in Table 2.
When all the eligible studies were pooled into the meta-analysis, results showed that the polymorphism was significantly associated with cancer risk under all genetic models (Fig. 2; dominant model: OR = 1.32, 95 % CI = 1.09–1.58; recessive model: OR = 1.23, 95 % CI = 1.05–1.43; II vs. DD: OR = 1.47, 95 % CI = 1.15–1.87; ID vs. DD: OR = 1.22, 95 % CI = 1.04–1.43; I vs. D: OR = 1.19, 95 % CI = 1.06–1.34). In the stratified analysis by cancer type, significant associations were not found in BC and LC, but significant associations in OC, HCC, and OSCC were observed. Subgroup analysis based on ethnicity was performed; the NFKB1-94 I/D polymorphism was found to contribute to cancer risk in Asian population (dominant model: OR = 1.52, 95 % CI = 1.17–1.98; recessive model: OR = 1.50, 95 % CI = 1.26–1.79; II vs. DD: OR = 1.90, 95 % CI = 1.37–2.65; ID vs. DD: OR = 1.32, 95 % CI = 1.05–1.66; I vs. D: OR = 1.37, 95 % CI = 1.17–1.60), but not in Caucasian population (Table 2).

Forest plot representing the pooled result of ORs for the association between NFKB1 -94 insertion/deletion polymorphism and cancer risk under recessive model
Sensitivity analysis
The sensitivity analysis was performed to assess the influence of an individual study on the overall OR. Results showed that no individual study affected the pooled OR markedly, since omission of any single study made no substantial difference. The results verified the stability of this meta-analysis.
Publication bias
The Begg’s funnel plot and Egger’s test were performed to assess the publication bias of literatures. No evidence of publication bias was observed under the recessive model (Fig. 3; P = 0.054). However, there was publication bias under other genetic models (ID vs. DD: P = 0.004; II vs. DD: P = 0.016; I vs. D: P = 0.026).

Begg’s Funnel plot in the meta-analysis of the association between NFKB1 -94 insertion/deletion polymorphism and cancer risk under recessive model
Discussion
The NFKB1 -94 I/D polymorphism was found to be not associated with cancer risk in previous meta-analysis including 2,743 cases and 2,195 controls [30]. However, when stratified by ethnicity, the significant association of NFKB1 -94 I/D polymorphism with cancer risk was observed in Asian and Caucasian populations.
In the present study, we collected more studies and a larger number of subjects to assess the association between the NFKB1 -94 I/D polymorphism and cancer risk. There are obvious discrepancies between the previous meta-analysis and ours. We detected a statistically significant association between the polymorphism and cancer risk. Moreover, in the stratified analysis based on ethnicity, significantly increased risks were observed in Asian population, but not in Caucasian population. However, the abovementioned results were not found in previous meta-analysis. These diverse results may be due to the differences in the studies included in the meta-analysis. Three case–control studies departure from HWE were included in previous meta-analysis based on 11 publications, but they were excluded in ours [31, 32]. In addition, recently published 12 studies were included in our analysis [16–23, 25, 27]. Therefore, our meta-analysis has stronger evidence to clarify the association between the NFKB1 -94 I/D polymorphism and cancer risk. We also conducted subgroup analysis of cancer type, which was not performed in the previous analysis. The result revealed that NFKB1 polymorphism was associated with the risk of OC, HCC, and OSCC.
Heterogeneity for the NFKB1 -94 I/D polymorphism was observed in these studies. In order to explain the main reasons for the heterogeneity across studies, we performed the stratified analysis by ethnicity and cancer type. The results showed that heterogeneity for the total population may come from different ethnicities and different cancer types. In addition, the heterogeneity was also found in Asian population, which may result from differences in the number of cases and controls, study design, or genotyping method. Publication bias was not observed under recessive model. However, we found a potential publication bias under other genetic models. This reason may arise from a lack of publication of trials with opposite results.
Several limitations of this analysis should be considered. First, our results were based on unadjusted estimates, while a more precise analysis could be conducted if individual data were available. Second, the studies searched on PubMed were full text in English. This may result in a language bias that is partially responsible for the observed publication bias. Third, the number of studies for subgroup analysis was small and restrains further our analysis for risk factors.
In conclusion, we found significant associations between the NFKB1 -94 I/D polymorphism and cancer risk in Asian population. However, further studies are needed to warrant and validate the association between NFKB1 -94 I/D polymorphism and the risk of cancer.
Conflicts of interest
None
References
Yaghoobi M, Rakhshani N, Sadr F, Bijarchi R, Joshaghani Y, et al. Hereditary risk factors for the development of gastric cancer in younger patients. BMC Gastroenterol. 2004;4:28.
Berlau J, Glei M, Pool-Zobel BL. Colon cancer risk factors from nutrition. Anal Bioanal Chem. 2004;378:737–43.
Sethi G, Shanmugam MK, Ramachandran L, Kumar AP, Tergaonkar V. Multifaceted link between cancer and inflammation. Biosci Rep. 2012;32:1–15.
Song L, Li J, Zhang D, Liu ZG, Ye J, Zhan Q, et al. IKKβ programs to turn on the GADD45α-MKK4-JNK apoptotic cascade specifically via p50 NFkB1 in arsenite response. J Cell Biol. 2006;175:607–17.
Ghosh S, Karin M. Missing pieces in the NF-kappaB puzzle. Cell. 2002;109:81–96.
Solan NJ, Miyoshi H, Carmona EM, Bren GD, Paya CV. RelB cellular regulation and transcriptional activity are regulated by p100. J Biol Chem. 2002;277:1405–18.
Giefing M, Wierzbicka M, Rydzanicz M, Cegla R, Kujawski M, et al. Chromosomal gains and losses indicate oncogene and tumor suppressor gene candidates in salivary gland tumors. Neoplasma. 2008;55:55–60.
Karban AS, Okazaki T, Panhuysen CI, Gallegos T, Potter JJ, et al. Functional annotation of a novel NFKB1 promoter polymorphism that increases risk for ulcerative colitis. Hum Mol Genet. 2004;13:35–45.
Zhang P, Wei Q, Li X, Wang K, Zeng H, Bu H, et al. A functional insertion/deletion polymorphism in the promoter region of the NFKB1 gene increases susceptibility for prostate cancer. Cancer Genet Cytogenet. 2009;191:73–7.
Cheng CW, Su JL, Lin CW, Su CW, Shih CH, Yang SF, et al. Effects of NFKB1 and NFKBIA gene polymorphisms on hepatocellular carcinoma susceptibility and clinicopathological features. PLoS One. 2013;8:e56130.
Mohd Suzairi MS, Tan SC, Ahmad Aizat AA, Mohd Aminudin M, Siti Nurfatimah MS, Andee ZD, et al. The functional −94 insertion/deletion ATTG polymorphism in the promoter region of NFKB1 gene increases the risk of sporadic colorectal cancer. Cancer Epidemiol. 2013;37:634–8.
Lo SS, Chen JH, Wu CW, Lui WY. Functional polymorphism of NFKB1 promoter may correlate to the susceptibility of gastric cancer in aged patients. Surgery. 2009;145:280–5.
Lin SC, Liu CJ, Yeh WI, Lui MT, Chang KW, Chang CS. Functional polymorphism in NFKB1 promoter is related to the risks of oral squamous cell carcinoma occurring on older male areca (betel) chewers. Cancer Lett. 2006;243:47–54.
Riemann K, Becker L, Struwe H, Nückel H, Dührsen U, Alakus H, et al. No association of the NFKB1 insertion/deletion promoter polymorphism with survival in colorectal and renal cell carcinoma as well as disease progression in B cell chronic lymphocytic leukemia. Pharmacogenet Genomics. 2006;16:783–8.
Lehnerdt GF, Bankfalvi A, Grehl S, Adamzik M, Lang S, Schmid KW, et al. No association of the NF-kappaB1 -94ins/delATTG promoter polymorphism with relapse-free and overall survival in patients with squamous cell carcinomas of the head and neck region. Int J Immunopathol Pharmacol. 2008;21:827–32.
Li P, Gu J, Yang X, Cai H, Tao J, Yang X, et al. Functional promoter −94 ins/del ATTG polymorphism in NFKB1 gene is associated with bladder cancer risk in a Chinese population. PLoS One. 2013;8:e71604.
Kopp TI, Friis S, Christensen J, Tjønneland A, Vogel U. Polymorphisms in genes related to inflammation, NSAID use, and the risk of prostate cancer among Danish men. Cancer Genet. 2013.pii: S2210-7762(13)00084-7
Huo ZH, Zhong HJ, Zhu YS, Xing B, Tang H. Roles of functional NFKB1 and β-TrCP insertion/deletion polymorphisms in mRNA expression and epithelial ovarian cancer susceptibility. Genet Mol Res. 2013;12:3435–43.
Huang D, Yang L, Liu Y, Zhou Y, Guo Y, Pan M, et al. Functional polymorphisms in NFκB1/IκBα predict risks of chronic obstructive pulmonary disease and lung cancer in Chinese. Hum Genet. 2013;132:451–60.
Vangsted AJ, Nielsen KR, Klausen TW, Haukaas E, Tjønneland A, Vogel U. A functional polymorphism in the promoter region of the IL1B gene is associated with risk of multiple myeloma. Br J Haematol. 2012;158:515–8.
Lin CW, Hsieh YS, Hsin CH, Su CW, Lin CH, Wei LH, et al. Effects of NFKB1 and NFKBIA gene polymorphisms on susceptibility to environmental factors and the clinicopathologic development of oral cancer. PLoS One. 2012;7:e35078.
Fan Y, Yu W, Ye P, Wang H, Wang Z, Meng Q, et al. NFKB1 insertion/deletion promoter polymorphism increases the risk of advanced ovarian cancer in a Chinese population. DNA Cell Biol. 2011;30:241–5.
Zhou B, Qie M, Wang Y, Yan L, Zhang Z, Liang A, et al. Relationship between NFKB1–94 insertion/deletion ATTG polymorphism and susceptibility of cervical squamous cell carcinoma risk. Ann Oncol. 2010;21:506–11.
Tang T, Cui S, Deng X, Gong Z, Jiang G, Wang P, et al. Insertion/deletion polymorphism in the promoter region of NFKB1 gene increases susceptibility for superficial bladder cancer in Chinese. DNA Cell Biol. 2010;29:9–12.
Andersen V, Christensen J, Overvad K, Tjønneland A, Vogel U. Polymorphisms in NFkB, PXR. LXR and risk of colorectal cancer in a prospective study of Danes. BMC Cancer. 2010;10:484.
Zhou B, Rao L, Li Y, Gao L, Wang Y, Chen Y, et al. A functional insertion/deletion polymorphism in the promoter region of NFKB1 gene increases susceptibility for nasopharyngeal carcinoma. Cancer Lett. 2009;275:72–6.
He Y, Zhang H, Yin J, Xie J, Tan X, Liu S, et al. IkappaBalpha gene promoter polymorphisms are associated with hepatocarcinogenesis in patients infected with hepatitis B virus genotype C. Carcinogenesis. 2009;30:1916–22.
Burnik FS, Yalçin S. NFKB1–94 insertion/deletion ATTG polymorphism in gastroenteropancreatic neuroendocrine tumors. Chemotherapy. 2009;55:381–5.
Riemann K, Becker L, Struwe H, Rübben H, Eisenhardt A, Siffert W. Insertion/deletion polymorphism in the promoter of NFKB1 as a potential molecular marker for the risk of recurrence in superficial bladder cancer. Int J Clin Pharmacol Ther. 2007;45:423–30.
Zou YF, Yuan FL, Feng XL, Tao JH, Ding N, Pan FM, et al. Association between NFKB1 -94ins/delATTG promoter polymorphism and cancer risk: a meta-analysis. Cancer Invest. 2011;29:78–85.
Lewander A, Butchi AK, Gao J, He LJ, Lindblom A, Arbman G, et al. Polymorphism in the promoter region of the NFKB1 gene increases the risk of sporadic colorectal cancer in Swedish but not in Chinese populations. Scand J Gastroenterol. 2007;42:1332–8.
Bu H, Rosdahl I, Sun XF, Zhang H. Importance of polymorphisms in NF-kappaB1 and NF-kappaBIalpha genes for melanoma risk, clinicopathological features, and tumor progression in Swedish melanoma patients. J Cancer Res Clin Oncol. 2007;133:859–66.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Xu, L., Huang, S., Chen, W. et al. NFKB1 -94 insertion/deletion polymorphism and cancer risk: a meta-analysis. Tumor Biol. 35, 5181–5187 (2014). https://doi.org/10.1007/s13277-014-1672-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-014-1672-z