
Abstract
The prognostic value of matrix metalloproteinase-7 (MMP-7) for survival of patients with non-small cell lung cancer (NSCLC) remains controversial. We performed a meta-analysis of the literatures to clarify its impact. Trials were selected for meta-analysis if they provided an independent assessment of MMP-7 in NSCLC and reported the analysis of survival data based on MMP-7 status. Pooled hazard ratio (HR) with 95 % confidence interval (95 % CI) was used to evaluate the associations between MMP-7 expression and survival of NSCLC patients. Heterogeneity and publication bias were also assessed. Seven studies involving 1,446 patients were identified. The combined HR for all studies was 1.28 (95 % CI 0.86–1.91; P = 0.22). Subgroup analysis revealed that MMP-7 overexpression had a favorable impact on survival in Caucasians (HR = 0.74; 95 % CI 0.55–0.99; P = 0.043) but showed a poor survival prognosis in Asians (HR = 1.74; 95 % CI 1.05–2.88, P = 0.031). Its effect also appeared significant when the analysis was restricted to Asian patients with squamous cell cancer (HR = 3.42; 95 % CI 1.92–6.11, P = 0.000) and adenocarcinoma (HR = 2.1; 95 % CI 1.34–3.29, P = 0.001). Our meta-analysis suggests that there are ethnic differences in the clinical significance of MMP-7 expression for patients with NSCLC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lung cancer (LC) is the most frequent and lethal human malignancy. Non-small cell lung cancer (NSCLC) accounts for approximately 85 % of all cases of lung cancer [1]. Despite diagnostic and therapeutic improvements, approximately 40–50 % of NSCLC presented as metastatic disease when they were diagnosed and a large percentage of the patients will die from relapse of their lung cancer, presumably most often because of undetected residual disease or metastasis. As the overall five-year survival rate for lung cancer patients is approximately 15 % [2], effective prognostic biomarkers are required for treatment selection of lung cancer patients classified with the same TNM stage.
Matrix metalloproteinases (MMPs) are a family of highly conserved enzymes that are capable of degrading the extracellular matrix (ECM). The degradation of the ECM is required in tumor angiogenesis, as well as tumor invasion and metastasis. Up to now, over 25 well-characterized members of this proteinase family have been identified. Matrix metalloproteinase-7 (MMP-7), the smallest (28 kDa) member of the MMP family, is produced by tumor cells [3, 4] and has broad substrate specificity against ECM components, including elastin, type IV collagen, fibronectin, vitronectin, aggrecan, and proteoglycans [5–7]. Previous clinical studies have shown an overexpression of MMP-7 to correlate with poor prognosis in many malignant tumors, including colorectal cancer [8–11], gastric cancer [12–14], esophageal cancer [4, 15], pancreatic cancer [16, 17], prostate cancer [18], and bladder cancer[19–21], indicating that MMP-7 could be useful as a tumor-associated biological marker. However, the prognostic value of MMP-7 for survival of patients with NSCLC remains controversial. Therefore, we conducted a meta-analysis of the published literatures to assess the prognostic value of its overexpression for the survival of patients with NSCLC.
Materials and methods
Search strategy
Published trials were sought by using electronic databases (PubMed, Embase, Web of Science, and CNKI). Search terms were “non-small cell lung cancer” or “carcinoma, non-small cell lung” or “NSCLC,” “MMP-7” or “matrix metalloproteinase-7” or “matrilysin” and “prognosis.” The published languages and years were not limited. The references reported in all the identified studies were used for the completion of the studies’ search, and the last search was updated on June 10, 2013.
Inclusion and exclusion criteria
This meta-analysis includes publications from studies meeting the following criteria: (1) The histologic type of the tumors was NSCLC; (2) It assessed the relationship between MMP-7 and survival and had been published as a full paper; (3) Hazard ratio (HR) and its 95 % confidence interval (95 % CI) are described or statistically extractable from data in the article. The major reasons for exclusion of studies were the following: (1) family studies, (2) case reports, (3) review papers, and (4) containing overlapping data. Only the most recent or informative study was included into this meta-analysis, when the same authors reported two or more publications on possibly the same patient populations.
Data extraction
All the data were extracted independently by two reviewers using a standard protocol. Potential disagreements were resolved by consensus. The following characteristics were extracted: name of the first author, year of publication, sample size, test method, cut-off value, tumor stage, histologic type, patient source, and percentage of MMP-7 high expression.
Statistical analysis
The analysis was done by comparisons of survival between the MMP-7 positive arm and the respective MMP-7 negative arm of the identified studies. The HRs and their 95 % CIs were used to combine as the effective value. If the HRs and their 95 % CIs were given explicitly in the articles, we used crude ones. Since intermixed factors are included in the multivariate analysis, HR obtained from multivariate analysis is more accurate than HR obtained from univariate analysis. Therefore, useful data for calculation from the latter was chosen when both univariate analysis and multivariate analysis were available for the studies. When these statistical variables were not provided, they were calculated from available numerical data or Kaplan–Meier survival curve. In these cases, after dividing the time axis into non-overlapping intervals, logHR and its variance for each interval were calculated. These estimated values were combined in a stratified manner to obtain the overall HR and 95 % CI [22]. All the statistical analyses were performed using Stata version 11 (Stata Corp, College Station, TX, USA). A statistical test with a P value less than 0.05 was considered significant. By convention, an observed HR > 1 implied a worse survival for the group with positive MMP-7 expression. In addition, the statistical heterogeneity within studies was tested with the chi-squared based Q-test (meaningful differences between studies indicated by P < 0.10). A random-effect model was employed when there was evidence of significant statistical heterogeneity. The potential publication bias was assessed using Begg’s [23] and Egger’s [24] tests.
Results
Study selection and characteristics
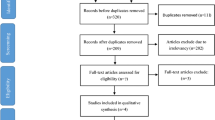
Figure 1 showed the flow chart of study selection in this meta-analysis. We identified 126 abstracts, of which 31 were further assessed for eligibility by full text. After excluding irrelevant studies, overlapping studies, and those without information to calculate the HR, a total of seven studies [25–31] that met the inclusion criteria were identified. There were two studies from Caucasians and five from Asians. The media follow-up was ranged from 20.8 to 97 months. The total number of included patients was 1,446 ranging from 66 to 452 patients per study (median, 206). The positive rate for MMP-7 overexpression in the individual studies ranged from 29.7 to 77.9 % by immunohistochemistry (IHC). The main characteristics of the seven eligible publications are reported in Table 1.

The flow diagram of search strategy
Surgery was performed for all patients in studies except one [28]. These publications concerned different cohorts of patients, five studies [25, 27, 28, 30, 31] (902 patients, 62.4 %) originated from East Asian, and the remaining two studies [26, 29] (544 patients, 37.6 %) originated from Europe. Three of the seven studies [25, 26, 30] concluded that MMP-7 was not a prognostic factor for survival; three [27, 28, 31] identified MMP-7 overexpression as a pejorative prognostic factor for survival; one [29] reporting a better prognosis for MMP-7 positivity was included. Subgroup analysis based on pathological subtype was performed in two studies [27, 28]. The included seven published studies investigated multiple factors of prognosis in NSCLC, such as age, gender, tumor status, nodal status, tumor type, tumor stage, cell differentiation, lymphovascular invasion, and performance status. Overall, according to the positive threshold for MMP-7 expression defined by the authors, MMP-7 was highly expressed in 53.8 % (778/1,446) of the evaluable NSCLC patients.
Meta-analysis
In three of the seven studies [27–29], the useful data for calculation were obtained directly from the original articles. In other four studies [25, 26, 30, 31], HRs had to be extrapolated from Kaplan–Meier survival curve.
The main results of the meta-analysis are summarized in Figs. 2 and 3. Overall, the combined HR for all seven studies was 1.28 (95 % CI 0.86–1.91, P = 0.22), suggesting that overall survival was slightly, but not significantly, worse in patients with positive MMP-7 expression than in those with negative MMP-7 expression. There was significant heterogeneity (Q = 27.60, P = 0.000), so the pooled HR for overall survival was performed using random-effort model and it was possible to go further in categorizing the trials. When we limited the source of patients involved in the studies to Asian, the combined HR was 1.74 (95 % CI 1.05–2.88, P = 0.031), showing a worse survival when MMP-7 expression is increased. Interestingly, a totally converse result was observed when the trials conducted in Caucasians were analyzed. The combined HR was 0.74 (95 % CI 0.55–0.99, P = 0.043), and the test for heterogeneity was non-significant (Q = 1.29, P = 0.26), suggesting that a positive MMP-7 status has a favorable impact on survival for Caucasian patients. We also focused on the predominant histologic type in each study. When the analysis was limited to studies focused on squamous cell cancer, the pooled HR was 3.42 (95 % CI 1.92–6.11, P = 0.000) without heterogeneity (Q = 0.27, P = 0.602). When the analysis was limited to studies focused on adenocarcinoma, the pooled HR was 2.1 (95 % CI 1.34–3.29, P = 0.001) without heterogeneity (Q = 1.03, P = 0.311).

Forest plot of meta-analysis of the effect of MMP-7 expression on survival in NSCLC patients

The two evaluable studies assessing MMP-7 in squamous cell cancer (a) and adenocarcinoma (b)
Publication bias
Both Begg’s funnel plot and Egger’s test were performed to assess the publication bias. Begg’s funnel plot did not reveal any evidence of obvious asymmetry in the overall meta-analysis (Fig. 4). There was no indication of publication bias from either Egger’s (P = 0.11) or Begg’s (P = 0.23) tests.

Begg’s funnel plot of the seven eligible studies assessing MMP-7 in NSCLC
Sensitivity analysis
A sensitivity analysis, in which one study was removed at a time, was performed to evaluate result stability. The corresponding pooled HRs were not significantly altered, suggesting stability of our results (Table 1).
Discussion
In recent years, substantial efforts have been made to identify prognostic factors to individualize treatment and improve survival. As far as we know, MMP-2 [32] and MMP-9 [33] have been implicated in prognosis of NSCLC; so we hypothesized that MMP-7 status in NSCLC may also have a correlation with prognosis. After searching for studies according to our methodology, we indeed found some experiments reporting that MMP-7 overexpression was a poor prognostic factor for survival in NSCLC. However, converse outcome was reported, too. The present study summarized all of the available data on the impact of MMP-7 expression on the prognosis of NSCLC in 1,446 cases. Our results using the pooled HR of OS did not indicate that high MMP-7 expression was associated with poor prognosis in mixed populations. As there was extreme heterogeneity (P = 0.000) among the seven studies, we went further to perform subgroup analysis. Interestingly, high MMP-7 had totally different clinical significance to the Asians and Caucasians, respectively. We observed a significant role of MMP-7 in the subgroup of Asian studies (HR = 1.74; 95 % CI 1.05–2.88), while the outcomes of European studies produced an HR of 0.74 (95 % CI 0.55–0.99).
To our knowledge, MMP-7 allows tumor cells to become resistant to apoptotic signals by cleavage of the pro-apoptotic FAS ligand (FASL) [34, 35]. MMP-7 also inhibits apoptosis by cleaving pro-heparin-binding epidermal growth factor (pro-HB-EGF) to generate mature HB-EGF, which promotes cell survival by stimulating the ERBB4 receptor tyrosine kinase [36]. In addition, MMP-7 can cleave E-cadherin, which promotes tumor-cell invasion in vitro [37]. In animal experiments, tissue-specific overexpression of MMP-7 leads to hyperproliferative disease and increased cancer susceptibility [38]; while downregulation of MMP-7 by antisense oligonucleotide results in reduced tumor burden or metastasis [39]. All these functions imply that MMP-7 may associate with poor prognosis in NSCLC. In this study, MMP-7 positive expression showed shorter overall survival in Asian populations, which matched with the functions of MMP-7; while it suggested a favorable prognosis in Caucasians. Although the outcome about white populations did not agree with the opinions of the existing functions of MMP-7, it was supported by similar results from other studies. Luukkaa et al. showed that high expression of MMP-7 in acinic cell carcinomas and mucoepidermoid carcinomas of the salivary glands was associated with a better overall survival [40]. Sillanpaa et al. demonstrated that high MMP-7 level was a marker of better differentiation and relatively favorable prognosis in epithelial ovarian cancer [41]. This phenomenon also appears in other prognosis factors. Dahabreh et al. reported that increased EGFR gene copy number was associated with an improvement in overall survival among studies enrolling predominantly white individuals but did not appear to have an effect in studies enrolling individuals of East Asian descent [42]. Therefore, we assume that the differences in the constitutional genetic background between populations may partly account for the divergent results.
We also analyzed the data according to histology subtypes. Survival probability was found to be influenced by the histological type of NSCLC at diagnosis. Subgroup analysis based on lung cancer subtypes showed that high MMP-7 expression might be associated with poor prognosis in squamous cell cancer and adenocarcinoma. Interestingly, the populations used to make the subgroup analysis were all Asian patients. That is to say, MMP-7 overexpression also had a significant correlation with poor survival in Asian patients who were diagnosed as squamous cell cancer and adenocarcinoma.
As MMP-7 overexpression was closely associated with the prognosis in NSCLC according to the present study, the factors regulating MMP-7 expression should also be attached great importance to. To our knowledge, MMP-7 is one of target genes of β-catenin, which is a pivotal component of the canonical Wnt signaling pathway [43]. Thereby, any factor taking part in the regulation of β-catenin expression or Wnt signaling pathway may have effect on the MMP-7 expression. Zhang et al. reported that NKD1 knockdown could markedly up-regulate dishevelled-1 and β-catenin protein levels and enhance the transcription of MMP-7 in NSCLC cells [44]. Su et al. showed that TC-1 expression positively regulated β-catenin transcription and MMP-7 expression at the mRNA and protein level [45]. Besides the Wnt/β-catenin pathway, MMP-7 expression can be regulated by other pathway or factors in NSCLC. Fibulin-5, a recently identified fibulin family member, functions as an inhibitor of ERK signaling via its RGD motif to inhibit MMP-7 expression; silencing of fibulin-5 can up-regulate MMP-7 in NSCLC [46]. Suppression of fibulin-3, which is homologous to fibulin-5, can significantly elevate cellular levels of MMP-7 [47]. Furthermore, MMP-7 expression can be enhanced by silencing Kaiso [48]; δ-catenin overexpression could significantly decrease the binding between Kaiso and MMP-7, which results in increased expression of MMP-7 [49]. In addition to the vitro findings, previous study demonstrated the intratumoral Wnt1 overexpression was associated with the high MMP-7 expression in NSCLC [43]; up-regulation of MMP-7 was related to β-catenin nuclear accumulation in lung neuroendocrine tumors [50]. Although the role of MMP-7 overexpression has been evaluated in our study, the association between MMP-7 and its upstream regulation factors in NSCLC tissues is not very clear yet. Further study is needed to investigate the role of these factors in prognosis and their expression in relation to MMP-7 in NSCLC patients with different genetic background. On the other hand, MMP-7 can also be regulated by extracellular agents. Recent studies showed that artesunate, andrographolide, and α-tomatine considerably suppressed invasion and metastasis in NSCLC cells by reducing the expression of MMP-7 [51–53], which supported the necessity of future preclinical and clinical studies investigating the suitability and efficacy of these agents as additional therapeutics or anti-cancer agents in the treatment of NSCLC, especially for Asians with MMP-7 overexpression.
Though the method used for the assessment of MMP-7 expression in NSCLC patients in the seven studies was the same, IHC results depend on the primary antibody used. A range of antibodies purchased from different manufacturers and the antibody concentration are important factors having an influence on the staining result, and the cut-off of defining the specimens as MMP-7 positivity varied substantially. Therefore, the divergent findings between species may also partly be explained by the differences of the antibodies, concentration, and cut-off value used in IHC. However, due to the small groups of studies evaluating the same antibody, subgroup analysis could not be performed to explore this technical problem. Well-designed clinical trials with large patient size are urgently needed.
In conclusion, our meta-analysis suggests that ethnic differences in clinical significance of MMP-7 expression for patients with NSCLC exist. High expression of MMP-7 predicts favorable prognosis in white populations; however, for Asian patients, MMP-7 overexpression had a significant correlation with poor survival, especially for patients who diagnosed as squamous cell cancer and adenocarcinoma. Since racial and ethnic differences in MMP expression are poorly understood, our data help to get a precise estimate of the prognostic role of MMP-7 expression and provided information that the potential underlying mechanism of MMP-7 in tumor metastasis vary between different ethnicities. Several racial/ethnic determinants and/or lifestyle linked to race are likely to affect expression of the MMP-7, which merits further investigation.
References
Molina JR, Yang P, Cassivi SD, Schild SE, Adjei AA. Non-small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clin Proc. 2008;83:584–94.
Alberg AJ, Ford JG, Samet JM. Epidemiology of lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007;132:29S–55.
Polette M, Nawrocki-Raby B, Gilles C, Clavel C, Birembaut P. Tumour invasion and matrix metalloproteinases. Crit Rev Oncol Hematol. 2004;49:179–86.
Tanioka Y, Yoshida T, Yagawa T, Saiki Y, Takeo S, Harada T, et al. Matrix metalloproteinase-7 and matrix metalloproteinase-9 are associated with unfavourable prognosis in superficial oesophageal cancer. Br J Cancer. 2003;89:2116–21.
Woessner Jr JF, Taplin CJ. Purification and properties of a small latent matrix metalloproteinase of the rat uterus. J Biol Chem. 1988;263:16918–25.
Miyazaki K, Hattori Y, Umenishi F, Yasumitsu H, Umeda M. Purification and characterization of extracellular matrix-degrading metalloproteinase, matrin (pump-1), secreted from human rectal carcinoma cell line. Cancer Res. 1990;50:7758–64.
Wilson CL, Matrisian LM. Matrilysin: an epithelial matrix metalloproteinase with potentially novel functions. Int J Biochem Cell Biol. 1996;28:123–36.
Wang WS, Chen PM, Wang HS, Liang WY, Su Y. Matrix metalloproteinase-7 increases resistance to Fas-mediated apoptosis and is a poor prognostic factor of patients with colorectal carcinoma. Carcinogenesis. 2006;27:1113–20.
Martinez-Fernandez A, Garcia-Albeniz X, Pineda E, Visa L, Gallego R, Codony-Servat J, et al. Serum matrilysin levels predict outcome in curatively resected colorectal cancer patients. Ann Surg Oncol. 2009;16:1412–20.
Koskensalo S, Louhimo J, Nordling S, Hagstrom J, Haglund C. Mmp-7 as a prognostic marker in colorectal cancer. Tumour Biol. 2011;32:259–64.
Yang B, Su K, Gao J, Rao Z. Expression and prognostic value of matrix metalloproteinase-7 in colorectal cancer. Asian Pac J Cancer Prev. 2012;13:1049–52.
Lee KH, Shin SJ, Kim KO, Kim MK, Hyun MS, Kim TN, et al. Relationship between e-cadherin, matrix metalloproteinase-7 gene expression and clinicopathological features in gastric carcinoma. Oncol Rep. 2006;16:823–30.
Koskensalo S, Mrena J, Wiksten JP, Nordling S, Kokkola A, Hagstrom J, et al. Mmp-7 overexpression is an independent prognostic marker in gastric cancer. Tumour Biol. 2010;31:149–55.
Yeh YC, Sheu BS, Cheng HC, Wang YL, Yang HB, Wu JJ. Elevated serum matrix metalloproteinase-3 and -7 in H. pylori-related gastric cancer can be biomarkers correlating with a poor survival. Dig Dis Sci. 2010;55:1649–57.
Yamashita K, Mori M, Shiraishi T, Shibuta K, Sugimachi K. Clinical significance of matrix metalloproteinase-7 expression in esophageal carcinoma. Clin Cancer Res. 2000;6:1169–74.
Yamamoto H, Itoh F, Iku S, Adachi Y, Fukushima H, Sasaki S, et al. Expression of matrix metalloproteinases and tissue inhibitors of metalloproteinases in human pancreatic adenocarcinomas: clinicopathologic and prognostic significance of matrilysin expression. J Clin Oncol. 2001;19:1118–27.
Jones LE, Humphreys MJ, Campbell F, Neoptolemos JP, Boyd MT. Comprehensive analysis of matrix metalloproteinase and tissue inhibitor expression in pancreatic cancer: increased expression of matrix metalloproteinase-7 predicts poor survival. Clin Cancer Res. 2004;10:2832–45.
Szarvas T, Becker M, Vom Dorp F, Meschede J, Scherag A, Bankfalvi A, et al. Elevated serum matrix metalloproteinase 7 levels predict poor prognosis after radical prostatectomy. Int J Cancer. 2011;128:1486–92.
Szarvas T, Laszlo V, Vom Dorp F, Reis H, Szendroi A, Romics I, et al. Serum endostatin levels correlate with enhanced extracellular matrix degradation and poor patients' prognosis in bladder cancer. Int J Cancer. 2012;130:2922–9.
Svatek RS, Shah JB, Xing J, Chang D, Lin J, McConkey DJ, et al. A multiplexed, particle-based flow cytometric assay identified plasma matrix metalloproteinase-7 to be associated with cancer-related death among patients with bladder cancer. Cancer. 2010;116:4513–9.
Szarvas T, Jager T, Becker M, Tschirdewahn S, Niedworok C, Kovalszky I, et al. Validation of circulating MMP-7 level as an independent prognostic marker of poor survival in urinary bladder cancer. Pathol Oncol Res. 2011;17:325–32.
Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med. 1998;17:2815–34.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–101.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Lin TS, Chiou SH, Wang LS, Huang HH, Chiang SF, Shih AY, et al. Expression spectra of matrix metalloproteinases in metastatic non-small cell lung cancer. Oncol Rep. 2004;12:717–23.
Leinonen T, Pirinen R, Bohm J, Johansson R, Ropponen K, Kosma VM. Expression of matrix metalloproteinases 7 and 9 in non-small cell lung cancer. Relation to clinicopathological factors, beta-catenin and prognosis. Lung Cancer. 2006;51:313–21.
Liu D, Nakano J, Ishikawa S, Yokomise H, Ueno M, Kadota K, et al. Overexpression of matrix metalloproteinase-7 (MMP-7) correlates with tumor proliferation, and a poor prognosis in non-small cell lung cancer. Lung Cancer. 2007;58:384–91.
Liu H, Zhang T, Li X, Huang J, Wu B, Huang X, et al. Predictive value of MMP-7 expression for response to chemotherapy and survival in patients with non-small cell lung cancer. Cancer Sci. 2008;99:2185–92.
Stenvold H, Donnem T, Andersen S, Al-Saad S, Al-Shibli K, Busund LT, et al. Overexpression of matrix metalloproteinase-7 and -9 in NSCLC tumor and stromal cells: correlation with a favorable clinical outcome. Lung Cancer. 2012;75:235–41.
Yamamoto T, Oshima T, Yoshihara K, Nishi T, Arai H, Inui K, et al. Clinical significance of immunohistochemical expression of insulin-like growth factor-1 receptor and matrix metalloproteinase-7 in resected non-small cell lung cancer. Exp Ther Med. 2012;3:797–802.
Song BH, Yang QB, Zhang JT, Yu JB. Expression of matrix metalloproteinase-7 and urokinase plasminogen activator receptor in non-small cell lung cancer. Chin Clin Oncol. 2009;14:1069–72.
Qian Q, Wang Q, Zhan P, Peng L, Wei SZ, Shi Y, et al. The role of matrix metalloproteinase 2 on the survival of patients with non-small cell lung cancer: a systematic review with meta-analysis. Cancer Invest. 2010;28:661–9.
Peng WJ, Zhang JQ, Wang BX, Pan HF, Lu MM, Wang J. Prognostic value of matrix metalloproteinase 9 expression in patients with non-small cell lung cancer. Clin Chim Acta. 2012;413:1121–6.
Fingleton B, Vargo-Gogola T, Crawford HC, Matrisian LM. Matrilysin [MMP-7] expression selects for cells with reduced sensitivity to apoptosis. Neoplasia. 2001;3:459–68.
Mitsiades N, Yu WH, Poulaki V, Tsokos M, Stamenkovic I. Matrix metalloproteinase-7-mediated cleavage of Fas ligand protects tumor cells from chemotherapeutic drug cytotoxicity. Cancer Res. 2001;61:577–81.
Yu WH, Woessner Jr JF, McNeish JD, Stamenkovic I. CD44 anchors the assembly of matrilysin/MMP-7 with heparin-binding epidermal growth factor precursor and erbb4 and regulates female reproductive organ remodeling. Genes Dev. 2002;16:307–23.
Noe V, Fingleton B, Jacobs K, Crawford HC, Vermeulen S, Steelant W, et al. Release of an invasion promoter e-cadherin fragment by matrilysin and stromelysin-1. J Cell Sci. 2001;114:111–8.
Sternlicht MD, Werb Z. How matrix metalloproteinases regulate cell behavior. Annu Rev Cell Dev Biol. 2001;17:463–516.
Yonemura Y, Endo Y, Fujita H, Kimura K, Sugiyama K, Momiyama N, et al. Inhibition of peritoneal dissemination in human gastric cancer by MMP-7-specific antisense oligonucleotide. J Exp Clin Cancer Res. 2001;20:205–12.
Luukkaa H, Klemi P, Hirsimaki P, Vahlberg T, Kivisaari A, Kahari VM, et al. Matrix metalloproteinase (MMP)-7 in salivary gland cancer. Acta Oncol. 2010;49:85–90.
Sillanpaa SM, Anttila MA, Voutilainen KA, Ropponen KM, Sironen RK, Saarikoski SV, et al. Prognostic significance of matrix metalloproteinase-7 in epithelial ovarian cancer and its relation to beta-catenin expression. Int J Cancer. 2006;119:1792–9.
Dahabreh IJ, Linardou H, Kosmidis P, Bafaloukos D, Murray S. EGFR gene copy number as a predictive biomarker for patients receiving tyrosine kinase inhibitor treatment: a systematic review and meta-analysis in non-small-cell lung cancer. Ann Oncol. 2011;22:545–52.
Huang CL, Liu D, Ishikawa S, Nakashima T, Nakashima N, Yokomise H, et al. Wnt1 overexpression promotes tumour progression in non-small cell lung cancer. Eur J Cancer. 2008;44:2680–8.
Zhang S, Wang Y, Dai SD, Wang EH. Down-regulation of NKD1 increases the invasive potential of non-small-cell lung cancer and correlates with a poor prognosis. BMC Cancer. 2011;11:186.
Su K, Huang L, Li W, Yan X, Li X, Zhang Z, et al. TC-1 (c8orf4) enhances aggressive biologic behavior in lung cancer through the Wnt/beta-catenin pathway. J Surg Res. 2013;185:255–63.
Yue W, Sun Q, Landreneau R, Wu C, Siegfried JM, Yu J, et al. Fibulin-5 suppresses lung cancer invasion by inhibiting matrix metalloproteinase-7 expression. Cancer Res. 2009;69:6339–46.
Kim EJ, Lee SY, Woo MK, Choi SI, Kim TR, Kim MJ, et al. Fibulin-3 promoter methylation alters the invasive behavior of non-small cell lung cancer cell lines via MMP-7 and MMP-2 regulation. Int J Oncol. 2012;40:402–8.
Dai SD, Wang Y, Miao Y, Zhao Y, Zhang Y, Jiang GY, et al. Cytoplasmic Kaiso is associated with poor prognosis in non-small cell lung cancer. BMC Cancer. 2009;9:178.
Dai SD, Wang Y, Zhang JY, Zhang D, Zhang PX, Jiang GY, et al. Upregulation of delta-catenin is associated with poor prognosis and enhances transcriptional activity through Kaiso in non-small-cell lung cancer. Cancer Sci. 2011;102:95–103.
Pelosi G, Scarpa A, Veronesi G, Spaggiari L, Del Curto B, Moore PS, et al. A subset of high-grade pulmonary neuroendocrine carcinomas shows up-regulation of matrix metalloproteinase-7 associated with nuclear beta-catenin immunoreactivity, independent of EGFR and HER-2 gene amplification or expression. Virchows Arch. 2005;447:969–77.
Rasheed SA, Efferth T, Asangani IA, Allgayer H. First evidence that the antimalarial drug artesunate inhibits invasion and in vivo metastasis in lung cancer by targeting essential extracellular proteases. Int J Cancer. 2010;127:1475–85.
Lee YC, Lin HH, Hsu CH, Wang CJ, Chiang TA, Chen JH. Inhibitory effects of andrographolide on migration and invasion in human non-small cell lung cancer A549 cells via down-regulation of PI3K/Akt signaling pathway. Eur J Pharmacol. 2010;632:23–32.
Shieh JM, Cheng TH, Shi MD, Wu PF, Chen Y, Ko SC, et al. Alpha-tomatine suppresses invasion and migration of human non-small cell lung cancer NCI-H460 cells through inactivating FAK/PI3K/Akt signaling pathway and reducing binding activity of NF-kappaB. Cell Biochem Biophys. 2011;60:297–310.
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Additional information
Yonggang Liang and Shanxian Guo contributed equally to this work.
Rights and permissions
About this article
Cite this article
Liang, Y., Guo, S. & Zhou, Q. Prognostic value of matrix metalloproteinase-7 expression in patients with non-small cell lung cancer. Tumor Biol. 35, 3717–3724 (2014). https://doi.org/10.1007/s13277-013-1491-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-013-1491-7