
Abstract
There is a possible association between myeloperoxidase (MPO) 463G>A polymorphism and risk of lung cancer, but previous studies report conflicting results. We performed a meta-analysis of available molecular epidemiologic studies to comprehensively assess the association between MPO 463G>A polymorphism and risk of lung cancer. A systemic literature search was performed in Pubmed, Embase, and Wanfang databases for molecular epidemiologic studies on the association MPO 463G>A polymorphism and risk of lung cancer on March 16, 2013. The pooled odds ratios (ORs) with their 95 % confidence interval (95 % CI) were calculated to assess the strength of the association. Twenty-six individual case–control studies with a total of 18,433 subjects (7,752 cases and 10,681 controls) were finally included into the meta-analysis. Overall, MPO 463G>A polymorphism was significantly associated with decreased risk of lung cancer under two main genetic comparison models (for A versus G, OR = 0.91, 95 % CI 0.83–0.99, P = 0.035; for AG/AA versus GG, OR = 0.90, 95 % CI 0.81–0.99, P = 0.029). Meta-analysis of studies with high quality also showed that MPO 463G>A polymorphism was significantly associated with decreased risk of lung cancer under two main genetic comparison models (for A versus G, OR = 0.91, 95 % CI 0.83–0.99, P = 0.035; for AG/AA versus GG, OR = 0.90, 95 % CI 0.80–0.99, P = 0.048). Subgroup analysis by ethnicity further showed that there was a significant association between MPO 463G>A polymorphism and decreased risk of lung cancer in Caucasians but not in Asians. The meta-analysis suggests that MPO 463G>A polymorphism is associated with decreased risk of lung cancer, especially in Caucasians.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lung cancer is the second most common malignancy and has the highest cancer mortality rate worldwide [1, 2]. Currently, lung cancer accounts for about 15 % of all new cancer cases and nearly 30 % of all cancer-related deaths in the USA [3]. Previous studies have suggested that risk of developing lung cancer can be modified by the interactions between genetic and environmental factors such as smoking [4, 5]. Besides, tobacco smoking is accepted as the dominant causal factor of lung cancer, but fewer than 20 % of cigarette smokers develop lung cancer, suggesting that the genetic factors also play important roles in the development of lung cancer [5]. Myeloperoxidase (MPO) is an oxidative lysosomal enzyme, and it is linked to both inflammation and oxidative stress by its role in catalyzing the formation of oxidizing agents [6, 7]. The MPO gene is located on chromosome 17q23.1 and consists of 11 introns and 12 exons [8]. MPO 463G>A polymorphism (rs2333227) is a common single nucleotide polymorphism within the 5′ untranslated region of the MPO gene [8–10]. Previous studies suggested that the -463A allele could result in a decreased MPO expression, and individuals with the -463A allele may be afforded protection due to the decreased transcriptional activity of MPO and subsequent decreased metabolic activation of procarcinogens [8–10]. Therefore, there was a possible association between MPO 463G>A polymorphism and risk of lung cancer, and many studies were case–control studies performed to assess the association [11–25]. However, results from previous studies reported conflicting findings [11–25]. These inconclusive results may be due to the low sample size of single study or the different characteristics among studies, such as ethnicity and sources of controls [11–25]. We performed a meta-analysis of available molecular epidemiologic studies to comprehensively assess the association between MPO 463G>A polymorphism and risk of lung cancer.
Methods
Search strategy
An electronic search in the Pubmed, Embase, Web of Science, and Wanfang databases was performed to identify the eligible studies assessing the association between MPO 463G>A polymorphism and risk of lung cancer. There were no language restrictions, and the last search time was March 16, 2013. We used the keywords and subject terms: (“lung carcinoma” or “lung cancer”), (“polymorphism” or “variant” or “genotype” or “mutation”) and (“Myeloperoxidase” or “MPO” or “rs2333227”). All eligible studies were retrieved, and their bibliographies were checked for other relevant publications.
Inclusion criteria and exclusion criteria
To be eligible for the inclusion criteria in the meta-analysis, the following criteria were used: (1) case–control studies comparing lung cancer cases with healthy or non-cancer controls; (2) studies evaluating the association between MPO 463G > A polymorphism and risk of lung cancer; (3) sufficient genotype data of MPO 463G > A polymorphism were reported; and (4) studies was excluded if they were the following: (a) case-only studies; (b) case reports, letters, or reviews; (c) incomplete data or no usable data were reported; (d) studies containing overlapping data; and (e) family-based design or related cases and controls were contained.
Data extraction and quality assessment
The data extraction was performed independently by two reviewers, and the conflicting data extracted were settled by discussion. A standardized form was used in the data extraction from the published studies, and the following data were extracted: first author, year of publication, country, ethnicity, study design, diagnostic criteria, source of cases and controls, number of cases and controls, genotyping methods, frequencies of MPO 463G > A genotypes, and the confirmation of Hardy–Weinberg equilibrium (HWE) in controls. The quality of included studies was assessed by the confirmation of HWE in controls, and studies without the confirmation of HWE in controls were defined as low-quality studies, while studies with the confirmation of HWE in controls were defined as high-quality studies.
Statistical analysis
We firstly tested whether the genotype frequencies of MPO 463G > A genotypes in the controls were confirmed with HWE using the χ 2 test. The strength of the associations between the MPO 463G>A polymorphism and risk of lung cancer was estimated using odds ratios (ORs) and their 95 % confidence interval (95 % CI). The following contrasts for the associations between the MPO 463G>A polymorphism and lung cancer were evaluated: comparison of the variant allele with ancestral allele (A versus G), comparison of the variant homozygote with the ancestral homozygote (AA versus GG), comparison of the variant homozygote combined with the heterozygote versus ancestral homozygote (AA/GA versus GG), and comparison of the variant homozygote versus ancestral homozygote combined with the heterozygote (AA versus GA/GG). The I 2 statistic to quantify the proportion of the total variation due to heterogeneity were calculated, and an I 2 value of more than 50 % was interpreted as significant heterogeneity among studies [26]. When the effects were assumed to be homogenous, the fixed-effects model was used (Mantel–Haenszel method) [27]. If obvious heterogeneity was present, the random-effects model was used (DerSimonian–Laird method) [28]. Subgroup analysis based on ethnicity was used to explore the possible race-specific effect in the association. Potential publication bias was assessed by visual inspection of the funnel plots, in which the standard error of logOR of each study was plotted against its logOR, and an asymmetric plot suggested possible publication bias. In addition, we also performed the Egger linear regression test at the P < 0.05 level of significance to assess the funnel plot asymmetry [29]. All analyses were conducted using STATA (Version 11, StataCorp, College Station, TX, USA). All P values in the meta-analysis were two-sided, and statistical significance was considered when the P value was less than 0.05.
Results
Study selection and description of included studies
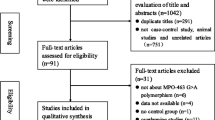
A total of 123 potentially individual abstracts were found from the Pubmed, Embase, Web of Science, and Wanfang databases. After checking the abstracts and reviewing the full texts of possible studies, 26 individual case–control studies from 25 publications were finally included into the meta-analysis [9, 11–25, 30–38]. There were a total of 18,433 subjects (7,752 cases and 10,681 controls) from those 26 studies. There were 17 studies from Caucasians [9, 11, 13, 15–18, 20, 22, 25, 30–34, 37, 38], and 7 studies from Asians [14, 19, 21, 23, 24, 35, 36]. In addition, 19 studies from those 26 studies had the confirmation of HWE in controls and were defined as high-quality studies [13–16, 18, 19, 21–23, 25, 30, 32–38]. There were seven studies without the confirmation of HWE in controls and were defined as low-quality studies [9, 11, 12, 17, 20, 24, 31].
Meta-analysis
Overall, MPO 463G > A polymorphism was significantly associated with decreased risk of lung cancer under two main genetic comparison models (for A versus G, OR = 0.91, 95 % CI 0.83 − 0.99, P = 0.035; for AG/AA versus GG, OR = 0.90, 95 % CI 0.81 − 0.99, P = 0.029) (Table 1, Fig. 1).

Forest plot describing the association between MPO 463G>A polymorphism and lung cancer (each study is shown by the point estimate of the OR and 95 % CI, and the size of the square is proportional to the weight of each study). a A versus G. b AA/GA versus GG
Meta-analysis of studies with high quality also showed that MPO 463G > A polymorphism was significantly associated with decreased risk of lung cancer under two main genetic comparison models (for A versus G, OR = 0.91, 95 % CI 0.83 − 0.99, P = 0.035; for AG/AA versus GG, OR = 0.90, 95 % CI 0.80 − 0.99, P = 0.048) (Table 1). Subgroup analysis by ethnicity further showed that there was a significant association between MPO 463G > A polymorphism and decreased risk of lung cancer in Caucasians but not in Asians (Table 1).
Publication bias
Publication bias was investigated by funnel plot, and funnel plot asymmetry was further assessed by Egger's test. There was a low possibility of asymmetry in the comparison model (AA/GA versus GG) of this meta-analysis (Fig. 2). The Egger's test also suggested that there was no evidence for the funnel plot asymmetry (P = 0.204). Therefore, there was no obvious risk of publication bias in this meta-analysis.

Funnel plot for the detection of the publication bias in this meta-analysis
Discussion
There is a possible association between MPO 463G > A polymorphism and risk of lung cancer, but previous studies report conflicting results. We performed a meta-analysis of available molecular epidemiologic studies to comprehensively assess the association between MPO 463G > A polymorphism and risk of lung cancer. However, results from previous studies reported conflicting findings [11–25]. These inconclusive results may due to the low sample size of single study or the different characteristics among studies, such as ethnicity and sources of controls [11–25]. We performed a meta-analysis of available molecular epidemiologic studies to comprehensively assess the association between MPO 463G > A polymorphism and risk of lung cancer. Therefore, we performed a systemic literature search in Pubmed, Embase, and Wanfang databases and carried out a meta-analysis of 26 individual case–control studies with a total of 18,433 subjects (7,752 cases and 10,681 controls). Overall, MPO 463G>A polymorphism was significantly associated with decreased risk of lung cancer under two main genetic comparison models (Table 1, Fig. 1). Meta-analysis of studies with high quality also showed that MPO 463G>A polymorphism was significantly associated with decreased risk of lung cancer under two main genetic comparison models (Table 1). Subgroup analysis by ethnicity further showed that there was a significant association between MPO 463G>A polymorphism and decreased risk of lung cancer in Caucasians but not in Asians. Therefore, the meta-analysis suggests that MPO 463G>A polymorphism is associated with decreased risk of lung cancer, especially in Caucasians.
Previous studies have suggested that risk of developing lung cancer can be modified by the interactions between genetic and environmental factors such as smoking, and the genetic factors also play important roles in the development of lung cancer [4, 5]. MPO is an oxidative lysosomal enzyme, and it is linked to both inflammation and oxidative stress by its role in catalyzing the formation of oxidizing agents [6, 7]. MPO 463G>A polymorphism is a common single nucleotide polymorphism within the 5′ untranslated region of the MPO gene, and the -463A allele could result in decreased MPO expression [8–10]. Individuals with the -463A allele may be afforded protection due to the decreased transcriptional activity of MPO and subsequent decreased metabolic activation of procarcinogens [8–10]. Previous studies have shown that individuals with lower transcriptional activity AA genotype of MPO 463G>A polymorphism may have significantly reduced risk of cancer, such as breast cancer [39]. Therefore, there is biochemical evidence for the association between MPO 463G>A polymorphism and risk of lung cancer.
The previous study by Taioli et al. included 10 studies (3,688 cases and 3,874 controls) [40], while this present meta-analysis included 26 individual case–control studies with a total of 18,433 subjects (7,752 cases and 10,681 controls), which had obviously larger size and could provide a more precise assessment of the association between MPO 463G>A polymorphism and lung cancer. Besides, subgroup analysis by ethnicity further showed that there was a significant association between MPO 463G>A polymorphism and decreased risk of lung cancer in Caucasians but not in Asians (Table 1). These results may indicate that there is a race-specific effect in the association between MPO 463G>A polymorphism and lung cancer.
There were some limitations in our meta-analysis. Firstly, there was a limited number of eligible studies in the subgroup analysis of the association between MPO 463G>A polymorphism and lung cancer in Asians. The limited sample size in the subgroup analysis of Asians may fail to provide enough statistical power to detect a possible or weak effect of MPO 463G>A polymorphism on lung cancer in Asians. Therefore, more studies with large sample are needed to give a more precise estimation of the association between MPO 463G>A polymorphism and lung cancer in Asians. Secondly, this meta-analysis was based on unadjusted data, as the ORs adjusted for the main confounding variables were not available from those studies. To provide a more reliable estimation of the association, more studies with well-designed and large sample size are needed to further identify the association. Finally, gene–gene interactions were not fully addressed in the meta-analysis for the lack of relevant data. Future studies may further assess the possible gene–gene interactions in the association between MPO 463G>A polymorphism and lung cancer risk.
In summary, the meta-analysis suggests that MPO 463G>A polymorphism is associated with decreased risk of lung cancer, especially in Caucasians. Besides, more studies with large sample are needed to give a more precise estimation of the association between MPO 463G>A polymorphism and lung cancer in Asians.
References
Goldstraw P, Ball D, Jett JR, Le Chevalier T, Lim E, Nicholson AG, et al. Non-small-cell lung cancer. Lancet. 2011;378:1727–40.
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90.
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29.
Herbst RS, Heymach JV, Lippman SM. Lung cancer. N Engl J Med. 2008;359:1367–80.
Brennan P, Hainaut P, Boffetta P. Genetics of lung-cancer susceptibility. Lancet Oncol. 2011;12:399–408.
Schindhelm RK, van der Zwan LP, Teerlink T, Scheffer PG. Myeloperoxidase: a useful biomarker for cardiovascular disease risk stratification? Clin Chem. 2009;55:1462–70.
Shao B, Oda MN, Oram JF, Heinecke JW. Myeloperoxidase: an oxidative pathway for generating dysfunctional high-density lipoprotein. Chem Res Toxicol. 2010;23:447–54.
Yuzhalin AE, Kutikhin AG. Common genetic variants in the myeloperoxidase and paraoxonase genes and the related cancer risk: a review. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev. 2012;30:287–322.
Cascorbi I, Henning S, Brockmoller J, Gephart J, Meisel C, Muller JM, et al. Substantially reduced risk of cancer of the aerodigestive tract in subjects with variant–463a of the myeloperoxidase gene. Cancer Res. 2000;60:644–9.
Ahn J, Gammon MD, Santella RM, Gaudet MM, Britton JA, Teitelbaum SL, et al. Myeloperoxidase genotype, fruit and vegetable consumption, and breast cancer risk. Cancer Res. 2004;64:7634–9.
London SJ, Lehman TA, Taylor JA. Myeloperoxidase genetic polymorphism and lung cancer risk. Cancer Res. 1997;57:5001–3.
Le Marchand L, Seifried A, Lum A, Wilkens LR. Association of the myeloperoxidase -463g– > a polymorphism with lung cancer risk. Cancer Epidemiol Biomarkers Prev. 2000;9:181–4.
Feyler A, Voho A, Bouchardy C, Kuokkanen K, Dayer P, Hirvonen A, et al. Point: Myeloperoxidase -463g –> a polymorphism and lung cancer risk. Cancer Epidemiol Biomarkers Prev. 2002;11:1550–4.
Lu W, Xing D, Qi J, Tan W, Miao X, Lin D. Genetic polymorphism in myeloperoxidase but not gstm1 is associated with risk of lung squamous cell carcinoma in a chinese population. Int J Cancer. 2002;102:275–9.
Schabath MB, Spitz MR, Delclos GL, Gunn GB, Whitehead LW, Wu X. Association between asbestos exposure, cigarette smoking, myeloperoxidase (mpo) genotypes, and lung cancer risk. Am J Ind Med. 2002;42:29–37.
Xu LL, Liu G, Miller DP, Zhou W, Lynch TJ, Wain JC, et al. Counterpoint: The myeloperoxidase -463g–> a polymorphism does not decrease lung cancer susceptibility in caucasians. Cancer Epidemiol Biomarkers Prev. 2002;11:1555–9.
Cajas-Salazar N, Sierra-Torres CH, Salama SA, Zwischenberger JB, Au WW. Combined effect of mpo, gstm1 and gstt1 polymorphisms on chromosome aberrations and lung cancer risk. Int J Hyg Environ Health. 2003;206:473–83.
Chevrier I, Stucker I, Houllier AM, Cenee S, Beaune P, Laurent-Puig P, et al. Myeloperoxidase: new polymorphisms and relation with lung cancer risk. Pharmacogenetics. 2003;13:729–39.
Wu XM, Zhou YK, Ren S, Hao QL. Gene polymorphism of myeloperoxidase and genetic susceptibility to lung cancer. Ai Zheng. 2003;22:912–5.
Harms C, Salama SA, Sierra-Torres CH, Cajas-Salazar N, Au WW. Polymorphisms in DNA repair genes, chromosome aberrations, and lung cancer. Environ Mol Mutagen. 2004;44:74–82.
Chan EC, Lam SY, Fu KH, Kwong YL. Polymorphisms of the gstm1, gstp1, mpo, xrcc1, and nqo1 genes in chinese patients with non-small cell lung cancers: relationship with aberrant promoter methylation of the cdkn2a and rarb genes. Cancer Genet Cytogenet. 2005;162:10–20.
Larsen JE, Colosimo ML, Yang IA, Bowman R, Zimmerman PV, Fong KM. Cyp1a1 ile462val and mpo g-463a interact to increase risk of adenocarcinoma but not squamous cell carcinoma of the lung. Carcinogenesis. 2006;27:525–32.
Park JH, Park JM, Kim EJ, Cha SI, Lee EB, Kim CH, et al. Myeloperoxidase -463g > a polymorphism and risk of primary lung cancer in a korean population. Cancer Detect Prev. 2006;30:257–61.
Zhang T, Hong X, Wu Y. Myeloperoxidase polymorphism in lung cancer patients of henan han population. J Zhengzhou Univ (Med Sci). 2006;42:448–50.
Arslan S, Pinarbasi H, Silig Y. Myeloperoxidase g-463a polymorphism and risk of lung and prostate cancer in a turkish population. Mol Med Rep. 2011;4:87–92.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959;22:719–48.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Schabath MB, Spitz MR, Zhang X, Delclos GL, Wu X. Genetic variants of myeloperoxidase and lung cancer risk. Carcinogenesis. 2000;21:1163–6.
Misra RR, Tangrea JA, Virtamo J, Ratnasinghe D, Andersen MR, Barrett M, et al. Variation in the promoter region of the myeloperoxidase gene is not directly related to lung cancer risk among male smokers in finland. Cancer Lett. 2001;164:161–7.
Dally H, Gassner K, Jager B, Schmezer P, Spiegelhalder B, Edler L, et al. Myeloperoxidase (mpo) genotype and lung cancer histologic types: the mpo −463 a allele is associated with reduced risk for small cell lung cancer in smokers. Int J Cancer. 2002;102:530–5.
Kantarci OH, Lesnick TG, Yang P, Meyer RL, Hebrink DD, McMurray CT, et al. Myeloperoxidase −463 (g– > a) polymorphism associated with lower risk of lung cancer. Mayo Clin Proc. 2002;77:17–22.
Liu G, Zhou W, Wang LI, Park S, Miller DP, Xu LL, et al. Mpo and sod2 polymorphisms, gender, and the risk of non-small cell lung carcinoma. Cancer Lett. 2004;214:69–79.
Yang M, Choi Y, Hwangbo B, Lee JS. Combined effects of genetic polymorphisms in six selected genes on lung cancer susceptibility. Lung Cancer. 2007;57:135–42.
Yoon KA, Kim JH, Gil HJ, Hwang H, Hwangbo B, Lee JS. Cyp1b1, cyp1a1, mpo, and gstp1 polymorphisms and lung cancer risk in never-smoking korean women. Lung Cancer. 2008;60:40–6.
Zienolddiny S, Campa D, Lind H, Ryberg D, Skaug V, Stangeland LB, et al. A comprehensive analysis of phase I and phase II metabolism gene polymorphisms and risk of non-small cell lung cancer in smokers. Carcinogenesis. 2008;29:1164–9.
Rotunno M, Yu K, Lubin JH, Consonni D, Pesatori AC, Goldstein AM, et al. Phase I metabolic genes and risk of lung cancer: multiple polymorphisms and mrna expression. PLoS One. 2009;4:e5652.
Pabalan N, Jarjanazi H, Sung L, Li H, Ozcelik H. Menopausal status modifies breast cancer risk associated with the myeloperoxidase (mpo) g463a polymorphism in caucasian women: a meta-analysis. PLoS One. 2012;7:e32389.
Taioli E, Benhamou S, Bouchardy C, Cascorbi I, Cajas-Salazar N, Dally H, et al. Myeloperoxidase g-463a polymorphism and lung cancer: a huge genetic susceptibility to environmental carcinogens pooled analysis. Genet Med. 2007;9:67–73.
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Additional information
Chengzhi Zhou and Qun Lou contributed equally to this work.
Rights and permissions
About this article
Cite this article
Zhou, C., Luo, Q., Qing, Y. et al. Association between MPO 463G>A polymorphism and risk of lung cancer: a meta-analysis. Tumor Biol. 34, 3449–3455 (2013). https://doi.org/10.1007/s13277-013-0921-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-013-0921-x