
Abstract
The incidence of colorectal cancer (CRC) is increasing rapidly in Asian countries during the past few decades, but no comprehensive analysis has been done to find out the exact cause of this disease. In this study, we investigated the frequencies of mutations and expression pattern of K-ras, APC (adenomatosis polyposis coli) and p53 in tumor, adjoining and distant normal mucosa and to correlate these alterations with patients clinicopathological parameters as well as with the survival. Polymerase chain reaction (PCR)-restriction digestion was used to detect mutations in K-ras and PCR-SSCP (Single Strand Conformation Polymorphism) followed by DNA sequencing was used to detect mutations in APC and p53 genes. Immunohistochemistry was used to detect the expression pattern of K-ras, APC and p53 proteins. The frequencies of mutations of K-ras, APC and p53 in 30 tumor tissues samples were 26.7 %, 46.7 % and 20 %, respectively. Only 3.3 % of tumors contained mutations in all the three genes. The most common combination of mutation was APC and p53 whereas mutation in both p53 and K-ras were extremely rare. There was no association between the mutations and expression pattern of K-ras, APC and p53 (p > 0.05). In Indians, the frequency of alterations of K-ras and APC is similar as in Westerns, whereas the frequency of p53 mutation is slightly lower. The lack of multiple mutations in tumor specimens suggests that these genetic alterations might have independent influences on CRC development and there could be multiple alternative genetic pathways to CRC in our present study cohort.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) is one of the leading causes of cancer-related deaths worldwide and the second most common cause of cancer deaths in the United States. It is second only to lung cancer [1]. The traditional pathogenic pathway, the adenoma–carcinoma sequence, plays an important role in the majority of colorectal carcinogenesis. Majority of CRC arises sporadically and only a small proportion 5–10 % arises due to familial inheritance. The incidence rates of CRC vary widely in different geographical areas, with relatively low incidence in Asian and African countries and a relatively high incidence in Western countries [2]. Many Asian countries have experienced an increase of two to four times in the incidence of CRC during the past few decades. Although adopting a globalized Western-style diet high in fat and animal protein and low in fiber, vegetables and fruit and a more sedentary lifestyle are believed to be the underlying reasons for the increase, but the interaction between these factors and genetic characteristics of the Asian populations might also have a pivotal role [3].
CRC has been associated with the progressive accumulation of a variety of genomic alterations in neoplastic cells. It is one of the best studied systems of human carcinogenesis, which can arise from a combination of mutations in oncogenes or tumor suppressor genes or from epigenetic changes in DNA such as methylation. Development of CRC is a process with multiple steps in which a healthy colonic epithelia go through small adenoma, large adenoma and finally become adenocarcinoma [4]. This process involves the activation of oncogenes and inactivation of tumor suppressor genes. Certain of the genes identified in the adenoma to carcinoma pathway are APC, K-ras, DCC, p53 and DNA mismatch repair (MMR) genes whereas APC and MMR genes are found to be mutated in familial CRC [5, 6]. It has been suggested that adenoma to carcinoma progression requires several genetic changes and it is the accumulation rather than the order of the mutations which is most critical [7]. Inactivation of the tumor suppressor genes APC and p53 and activation of the oncogene K-ras are the most important determinants that are required for tumor initiation and progression in CRC [5].
Mutation of APC gene is the initiating alteration in most CRCs [8]. This gene was first localized to chromosome 5q21 by disease linkage in patients with familial adenomatous polyposis (FAP) [9]. APC is a relatively large gene, encoding a protein of 312 kDa. A mutation cluster region (MCR) located between codons 1286 and 1513 of exon 15 has been identified in patients with FAP and sporadic CRC [10]. Although this MCR comprises only 10 % of the total APC coding sequence, but it contains more than 90 % of APC mutations reported in both familial and sporadic CRC [7]. APC has been proposed to function as a “gatekeeper” gene, regulating the entry of epithelial cells into the adenoma–carcinoma progression [7].
Mutations of the K-ras gene are known to be early genetic event in CRC. K-ras is a proto-oncogene, located on the short arm of chromosome 12, encodes a small (21-kDa) protein (p21ras) which is involved in G protein mediated signal transduction. This protein has intrinsic GTPase activity, which is lost when the gene is mutated, most commonly at codons 12, 13, and 61 leading to increased and unregulated cellular proliferation and malignant transformation [11].
Mutations in p53 which is a tumor suppressor gene are proposed to be relatively late events in the development of CRC. p53 gene, localized on the short arm of chromosome 17 and is found to be mutated in up to 70 % of CRCs [12]. p53 functions as a transcription factor, causing cell cycle arrest in response to DNA damage or other cellular stress [13]. Based on the hypothesis that mutation of specific target genes may be important molecular mechanisms that influence the pathogenesis of CRC, we examined the mutation spectra in three key genes, APC, K-ras, and p53 in 30 patients with sporadic CRC and compared the findings with western population to determine whether our populations has same pattern of genetic alterations as in west. We have also completed a follow up of these patients and analyzed the association of mutations of these genes with patients' survival.
The exact mechanism of CRC genesis is still controversial. Some authors support the adenoma–carcinoma sequence while others suggested the presence of de novo development of CRC. In a recent study from Europe, Smith et al. [14] suggested the presence of multiple alternative genetic pathways to CRC. It is known that the incidence of CRC in Asians is low and that the presence of synchronous adenomas is rare. In a study conducted in India by one of the investigators in the present study indicates that only 7.7 % of CRC patients have synchronous adenomas [15]. These findings raise a question that in Asians, CRC may have a different genesis to that of the Westernized population. The aim of the study was to assess if the low incidence of colorectal synchronous adenomatous polyps and cancer in Asians is reflected in a different pattern of genetic alterations.
Materials and methods
Patients and specimens
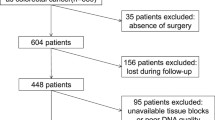
A total of 30 patients undergoing surgery for colorectal adenocarcinoma at a post-graduate institute of medical education and research, India, between July 2004 and July 2006 were enrolled in this study, which was designed to examine the clinicopathological features, mutation and expression pattern of K-ras, APC and p53 in tumor, adjoining and normal colonic mucosa. Inclusion criteria included the freshly resected primary adenocarcinoma. Patients who had history of prior chemotherapy or radiotherapy, with inoperable tumors, family history of colorectal adenocarcinoma, mucinous/signet cell carcinoma were excluded from the present study. Follow-up end point was September 2007. A written informed consent was obtained from each patient for inclusion in this study. This study was approved by the Institute Ethics Committee. Apart from the description of the gross features of the tumor at the time of surgery, the rest of the colon was examined for any synchronous polyp or tumor. Fresh samples from tumor, adjoining (2–5 cm from the tumor tissue) and distant normal mucosa (5–10 cm from the main tumor mass) were taken from the freshly resected colorectal specimen.
DNA extraction and mutation detection
Genomic DNA from each tumor tissue, adjoining and normal mucosa was isolated using proteinase-K digestion and a phenol/chloroform extraction procedure according to the method proposed by Sambrook and Russell [16]. Specifically, the MCR (codons 1286–1513) of APC, codon 12 of K-ras and the exons 5–8 of p53 were examined.
Mutation detection in case of codon 12 of K-ras was carried out by using polymerase chain reaction (PCR)-Msp1 restriction digestion according to the method of Ando et al. [17]. A band of 99 bp was obtained after PCR amplification. In the case of APC gene, MCR was amplified as four overlapping fragments using a nested PCR strategy [18]. Outside PCR was carried out to generate two fragments, A (356 bp) and B (511 bp). Fragment A was then used as starting material for the amplification of nested fragments S1 (219 bp) and S2 (204 bp) and fragment B was used for nested fragments S3 (205 bp) and S4 (267 bp). In the case of p53, exons 5–8 were studied. The primer sequences of K-ras, APC and p53 were taken from previously published sequences [17–19].
Restriction digestion
Restriction enzyme digestion was performed by incubating K-ras PCR products with 1 U of Msp1 restriction enzyme (Bangalore Genei, Bangalore, India), at 37 °C for 4 h to ensure complete digestion. For all the samples, a negative control of a similar reaction mixture but lacking the restriction enzyme was also included. Digested PCR products were analyzed on 3–4 % agarose gel. Appropriate molecular weight marker and undigested PCR product were also run along with the samples. To avoid partial digestion, PCR products from normal colonic mucosa were also digested in the same manner as a normal control. A sample was considered as possibly harboring a mutation if 99 bp band could be demonstrated after digestion and considered normal if 78- and 21-bp bands were demonstrated after digestion.
SSCP analysis
Because of the number and complexity of mutations in p53 and APC, the PCR-SSCP (Single Strand Conformation Polymorphism) analysis [20] was used as a “prescreen” to identify samples containing mutations in these genes. For SSCP analysis, the PCR amplified products (7 μl) were diluted with the same amount in a denaturing buffer heated at 95 °C for 5 min, followed by immediate cooling on ice. This mixture was loaded on a 10 % polyacrylamide non-denaturing gel. Gels were run at 50–80 V at 4 °C for 24–30 h, and were then stained by silver staining.
DNA sequencing
DNA samples with suspected APC and p53 mutations were amplified using Phusion™ high-fidelity DNA polymerase enzyme (New England Biolabs, Finland) and products obtained were purified and sent for DNA sequencing. All obtained sequences were aligned with previously published sequences in NCBI for each of the target genes.
Immunohistochemistry
The streptavidin–biotin peroxidase complex method was used for IHC staining. The antibody used were K-ras-2B (C-19) sc-521 to detect K-ras protein, APC (c-20) sc-896 to detect APC protein (Santa Cruz Biotechnology Inc., Santa Cruz, CA, USA) and p53 Ab-5 (DO-7) to detect p53 protein (Neomarkers, California, USA). A score of 0-3 for staining intensity was assigned. An intensity score of 0 = no staining, 1 = weak positivity, 2 = moderate positivity and 3 = strong positivity was given. The total IHC score was calculated as: \( \mathrm{IHC}\,\,\mathrm{score}=\%\ \mathrm{age}\ \mathrm{of}\ \mathrm{positivity}\times \mathrm{intensity}\ \mathrm{score} \).
Statistical analysis
Pearson’s χ 2 test was performed to analyze the relationship between mutation pattern and their respective protein expression and with each of the clinicopathological parameters. Mann–Whitney U-test was performed to determine the relationship between the expression of K-ras, APC and p53 with each of the clinicopathological parameters. Comparisons of the different groups were performed using the ANOVA followed by post-hoc test. The overall survival (OS) and disease-free survival (DFS) were estimated by the Kaplan–Meier method and the log-rank test was used to evaluate the difference between survival of the patients with and without mutation and expression of K-ras, APC and p53.
Results
All the clinical information of 30 patients with sporadic colorectal adenocarcinoma is presented in the Table 1.
Mutation analysis of K-ras, APC and p53
K-ras gene was found to be mutated in eight (26.7 %) tumor tissues whereas no mutations were detected in normal and adjoining mucosa (Fig. 1).

Analysis of K-ras mutations in CRC. a PCR amplified products of codon 12; b restriction digested product of codon 12; 99-bp band after digestion represents the point mutation at codon 12 of K-ras. MW molecular weight marker, –ve negative control, N normal mucosa, A adjoining mucosa, T tumor, U undigested, D digested
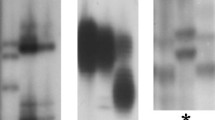
In the case of APC gene, PCR-SSCP revealed a shift in the band mobility in 14 (46.7 %) of tumor tissues and three (10 %) in adjoining mucosa. Two tumors had mutations in fragment S1, four had mutations in fragment S2, five had mutations in S3 fragment and five had mutations in S4 fragment. One sample revealed mutations in S2, S3 and S4 fragments. In case of adjoining mucosa, out of three cases; one had mutations in S1 fragment and two had mutations in S2 fragment. No mutation was observed in normal mucosa. A significant difference was observed in the frequencies of APC mutations between the adjoining mucosa and the tumor tissues (p = 0.002). The mutation of p53 was found to be in six (20 %) tumor tissues, of which one had mobility shift in exon 6, four in exon 7 and one in exon 8. In the case of adjoining and normal mucosa, no band mobility shift was found in any exon of the p53 (Fig. 2).

Mutation analysis of APC and p53 by PCR-SSCP. PCR-SSCP pattern of APC fragment: a S1, b S2, c S3, d S4, and e exon 6, f exon 7, g exon 8 of p53. N normal mucosa, A adjoining mucosa, T tumor tissue. Arrowheads indicate bands showing mobility shift
DNA sequencing analysis
DNA sequence analysis revealed the presence of point mutations in 14 tumor samples in case of APC. Out of these, nine were frameshift, seven silent and two missense mutations. All frameshift mutations showed the deletion of one nucleotide. In case of adjoining mucosa, there were one missense mutation and two frameshift mutations. The details of these mutations are given in Tables 2 and 3.
In the case of p53, there were five frameshift and three missense mutations in tumor tissues. Majority of mutations were found at exon 7 (Table 3).
Combination of APC, K-ras and p53 gene mutations
Only one (3.3 %) tumor tissue contained alterations in all the three genes, i.e., APC, K-ras and p53. Common combination of mutations was between p53 and APC (16.6 %), whereas mutations in both p53 and K-ras were extremely rare (3.3 %). A significant correlation was found in the occurrence of APC and p53 genes mutations (p = 0.044).
Protein expression of K-ras, APC and p53
Twenty-six (86.6 %) of the tumor tissues were immunoreactive for K-ras. A complete loss of expression was observed in four (13.3 %) tumors. In the case of adjoining mucosa, eight (26.6 %) were immunoreactive for K-ras, whereas no immunoreactivity was observed in normal colorectal mucosa Fig. 3(I).

Immunohistochemical staining showing expression of K-ras, APC and p53. (I) In the case of K-ras, a tumor showing strong nuclear and cytoplasmic positivity; b tumor showing moderate nuclear positivity; c adjoining mucosa showing moderate nuclear and cytoplasmic positivity; d normal mucosa showing no positivity. (II) In the case of APC, a tumor showing moderate nuclear and cytoplasmic positivity; b tumor showing loss of expression; c adjoining mucosa showing moderate cytoplasmic positivity; d Normal mucosa showing strong cytoplasmic positivity. (III) In the case of p53, a tumor showing strong nuclear positivity; b tumor showing moderate nuclear positivity; c adjoining mucosa showing moderate nuclear and cytoplasmic positivity; d normal mucosa showing no positivity for p53 (SABP immunostaining; ×450)
APC protein was expressed in 19(63.3 %) of the tumors and complete loss of protein expression was observed in 11 (36.6 %) of the tumors. In adjoining mucosa, 25(83.3 %) samples were immunoreactive for APC and loss of protein expression was observed in five (16.6 %) cases. In normal mucosa, intact APC protein expression was present in almost all cases Fig. 3(II). In the case of p53, 23 (76.6 %) of the colorectal tumors showed immunoreactivity with 7(23.3 %) tumors being negative for p53 expression. In adjoining mucosa, p53 immunostaining was observed in seven (23.3 %) samples. Surface positivity was seen in majority of the samples, whereas a few samples showed basal positivity also. In normal mucosa, the expression of p53 protein was almost absent in Fig. 3(III).
Correlation of mutations and protein expression with clinicopathological factors
A significant correlation of K-ras gene mutations was observed with the age and histological grade of the tumor (p = 0.04, p = 0.036), whereas the nuclear positivity of p53 protein had a significant correlation with the distal site of the tumor (p = 0.029).
Effect of gene mutations on protein expression
In 26 adenocarcinoma cases positive for K-ras expression, eight had mutations in the K-ras gene. However four tumors negative for K-ras expression did not reveal any genetic alterations. Similarly, Out of the 19 colorectal adenocarcinoma positive for APC protein expression, nine had mutations in the MCR of APC gene while 11 tumors negative for APC expression, five had mutations. In the case of p53, 23 colorectal adenocarcinoma cases positive for p53 protein expression, six had mutations in the p53 gene. However, seven tumors negative for p53 expression did not reveal any genetic alterations. Mutations of K-ras, APC and p53 genes did not have a significant effect on their respective protein expression.
Survival analysis
The association of mutations as well as expression of APC, K-ras and p53 with DFS and OS was analyzed. The median follow-up period was 27 months with a range of 8–39 months (mean = 25.5 ± 8.14). The nuclear positivity of p53 had a significant correlation with the OS (p = 0.026) of the patients as shown in Fig. 4.

Survival curve of patients with colorectal adenocarcinoma showing overall survival according to the presence and absence of nuclear positivity of p53. (+) Patients with tumors positive for p53; (−) patients with tumors negative for p53 expression. p53 is significantly associated with poor prognosis in the cohort of patients (p = 0.026)
Discussion
A genetic model proposed by Fearon and Vogelstein for colorectal tumorigenesis, the so-called adenoma→carcinoma sequence that represents the paradigm and the basis of our understanding of the molecular and genetic basis of this disease [5, 7]. Recently, this model has been revised and presented in greater detail to include the interdependence of the different pathways and involvement of many more gene mutations than described before [21].
In contrast to the predictions of sequential mutation accumulation of genes, a recent study from Europe presented quite a different view, in which the gene mutation spectrum in a large cohort of CRC patients was correlated to only 6.6 % [15]. Similar observations were reported by another study from South Korea by Jeon et al. [22]. The heterogenous pattern of tumor mutations found in these studies suggests the presence of multiple alternatives genetic pathways to CRC and it was also speculated that the widely accepted genetic model of cancer development is not a representative of the majority of CRCs.
The present study analyzed a number of key genes (APC, K-ras and p53) involved in CRC genesis. In Indian population, the frequency of K-ras mutations in this group of patients was 27 % in tumor tissues whereas no mutations were observed in adjoining and normal mucosa. The incidence of K-ras mutations was 25–38 % in European [23–26], 33–39 % in US [27, 28] and 29–62.9 % in Asian populations [22, 29, 30]. Thus, the mutation frequency of K-ras in the present study fell within the range reported in the literature. Mutations of K-ras gene had a significant positive correlation with the age of the patient. The frequency of K-ras mutations was much less in patients at younger ages (<50 years, p = 0.040). In contrast older patients had increased frequency of K-ras mutations and are more in males than females. The observed low frequency of K-ras mutations may suggest that a different ras-independent pathway to neoplasia is dominating in the colon of younger patients. K-ras mutations also had a significant association with the well differentiated state of tumor (p = 0.036). Frequent occurrence of K-ras mutations in low grade tumors suggesting that mutation of K-ras gene is an early genetic event in colorectal carcinogenesis.
K-ras protein was overexpressed in 86.6 % tumor tissues and 40 % in adjoining mucosa, whereas in normal mucosa, immunohistochemistry did not reveal the presence of K-ras protein. There was a significant difference in the expression of K-ras in the adjoining and tumor tissue (p < 0.05). This suggests that there is an increase in K-ras expression during the gradual transition of adjoining mucosa to carcinoma. In a previous study, Servomaa et al. [31] observed that majority of the rectal tumors expressed K-ras (95 %) and mutations in K-ras were associated with strong staining of the protein. In the present study, the expression of K-ras protein was observed in both mutation positive and negative cases and no significant correlation was observed between mutation and expression of K-ras. This may be due to the variability in the analyzed gene region, i.e., only codon 12 was analyzed in this study. If mutations in codons 13 and 61 of the K-ras gene as well as in the N-ras gene are analyzed, a higher frequency of mutations would be expected. Secondly, there is a difference in the scoring methods used in different studies. In some studies, the intensity of immunostaining was taken into account whereas in the present study, the immunohistochemical score (%age positivity x intensity) was taken into account.
The incidence of APC gene mutations has been reported to be 37–56 % in European population [15, 26, 32]; 26–42 % in Asian population [22, 33, 34] and 60 % in US population [35]. In the present study, 46.7 % tumors and 10 % of adjoining mucosa presented a mutated form of APC and the mutation frequency fell within the reported range. DNA sequence analysis revealed frameshift mutations in nine cases, missense in two cases and silent mutations in seven cases. All the frameshift mutations were present in codons 1304, 1353 and 1408, silent mutations in codons 1365, 1493 and 1495 and missense mutations in codons 1366 and 1385. Mutations at these codons have been previously reported in colorectal carcinomas. Frameshift mutations have been reported to cluster in the region at codons 1309, 1350–1356, 1411–1419, 1465 and 1485–1495. The large number of missense mutations was distributed throughout the MCR of APC, but did not show any hot spots [32]. Fujimori et al. [36] reported the nonsense mutation in codon 1408 in CRC. Insertion in codon 1385 has been reported by Frattini et al. [37]. However, mutations in codons 1304, 1365 and 1366 have not been reported in the literature so far. The current data suggests that the majority of APC mutations are as reported in the literature, but a few new mutations were also observed. This may be due to the difference in the population studied. Moreover, in the present study, APC gene mutations were also observed in the adjoining mucosa, which suggests that mutations in the APC gene might be an early event in the development of CRC.
In the case of APC, 63 % tumor tissues expressed APC, whereas loss of expression was observed in 36.6 % cases and majority of tumors which expressed APC are low expressers. In adjoining mucosa, 80 % tumor tissues expressed APC protein and loss of expression was observed in 20 % cases and in case of normal mucosa intact APC protein was observed in almost all cases. A significant difference in the expression of APC was observed between normal, adjoining and tumor tissues (p < 0.05) which suggest that the expression of APC significantly reduced during transition from normal epithelium to carcinoma. Similar to the present data, Ozaki et al. [38] have reported reduced expression of APC in 34.7 % of the tumors. However, Iwamoto et al. [39] have reported loss of APC expression in 83 % of colon cancers. Correlation of APC mutation pattern with the protein expression was also analyzed but could not find any correlation between two because the reduced expression or loss of expression of APC was observed in both mutation positive and mutation negative cases and a few mutation negative cases retained APC integrity. This can be attributed to the fact that the reduction or loss of expression of APC protein is not only due to mutations but the methylation in the promoter region of APC gene may also play an important role as reported by Esteller et al. [40], who suggested that methylation in the promoter region of the APC gene constitutes an alternative mechanism for gene inactivation in colon and other tumors of the gastrointestinal tract. In addition, it might be possible that all tumors did not contain mutations within the exon 15 MCR, and mutations at other regions led to reduced expression of APC. Smith et al. [14] also found that a significant number of tumors had not lost APC tumor suppressor gene function, or at least did not contain mutations within the APC exon 15 MCR, suggesting that APC-driven alterations in colonic crypt architecture are not an absolute requirement for the initiation of dysplasia. Tumors retaining APC integrity must have an alternative mechanism of tumor initiation. It may also be possible that the beta-catenin mutation in exon-3 could also play an important role by enhancing the transcription of target genes through wnt signaling in the nucleus leading to hyperproliferation even without mutation in the APC gene in the initiation of tumor in the adenoma to carcinoma pathway suggesting an alternate pathway of tumorigenesis in CRC.
Mutations in p53 have been reported to occur with a frequency of 35–60 % in European subjects [15, 19, 24, 26, 41], 34–53 % in Asian subjects [22, 30] and 45.4 % in US population [42]. But in the present study, the mutation rate of p53 was quite low, i.e., 20 % in tumors, whereas no mutations was observed in case of adjoining and normal mucosa. The low frequency of p53 mutations may be due to the different dietary pattern, environmental conditions, population difference or some of the p53 mutations may occur outside exons 5–8. DNA sequencing analysis revealed the presence of point mutations in codons 198, 223, 237, 245 and 273. Mutations in codons 198 and 223 involved the deletion of one base resulting in the frameshift whereas transition was observed in codons 237 (A→G), 245 (G→A) and 273 (C→T) resulting in missense mutations. Mutations in five hotspot codons (175, 245, 248, 273, and 282) have been reported to account for approximately 43 % of all p53 mutations in CRC [43–45]. In the present study, mutations were observed in two hotspots, i.e., codons 245 and 273. Rodrigues et al. [46] reported the presence of missense mutations in codon 273 in addition to codons 241 and 248. Tullo et al. [47], Pfeifer et al. [48] and Liu and Bodmer [49] analyzed a large number of p53 codons in CRC and observed the presence of frameshift, missense and nonsense mutations in the codons 135, 148, 158, 176, 198, 204, 237, 242, 245, 249, 273, 275 and 337. Thus, pattern of mutations in the present study are similar to the previous reports.
In the present study, the expression of p53 was found in 76 % of colorectal tumors and 23 % of adjoining mucosa, whereas no p53 expression was observed in case of normal colorectal mucosa. A significant difference in the expression of p53 was observed between normal, adjoining and tumor tissues (p < 0.05), which suggested that the expression of p53 significantly increases during transition from normal epithelium to carcinoma. p53 expression in CRCs has been reported to be high. Approximately 50–75 % of tumors are positive for the p53 protein [50]. In the present study, there was no correlation between p53 mutations and p53 protein accumulation. This is not a surprising finding, because concordance between p53 nuclear overexpression and gene mutation was 68 % for CRCs in a study by Soong et al. [51]. Another study performed by Dix et al. [52] showed a 69 % concordance between the gene mutation and protein expression of p53. Further, studies comparing immunohistochemical detection of p53 (stabilization of p53) and mutation analysis, also showed that a substantial proportion of carcinomas with stabilized p53 protein do not contain mutations in exons 5–8, whereas some mutations are not associated with protein stabilization [53, 54]. In the present study, frequency of p53 gene mutations was low but the expression of p53 protein was high indicating that dysfunction of p53 gene might be caused by mechanisms other than mutations or due to the mutations occurring outside exons 5–8. The expression of p53 protein was found both in the proximal and distal colorectal adenocarcinomas. But the nuclear immunoreactivity of p53 was significantly higher in distal tumors as compared to proximal tumors (p = 0.029). This observation is consistent with the report of Campo et al. [55], who suggest that the expression of p53 protein in colorectal adenocarcinoma occurs more often in the rectum or distal colonic tumors.
In the present study, a comprehensive analysis of mutations in studied genes in colorectal tumors, adjoining and normal mucosa was performed, where only 3.3 % of tumors contained mutations in all three genes: APC, K-ras and p53. As the combination of these three gene mutations was rarely found together, this suggested that these mutations may lie on alternative pathways of tumor development in CRC. The most common combination of mutations in this study was that of APC and p53. More than one third of tumors contained mutations in only one of the three genes, demonstrating that the progressive accumulation of multiple mutations in these genes is not a prerequisite for tumor development. The mutational frequencies for the individual genes were entirely consistent with previous literature reports in CRC except p53 [12, 35, 56, 57].
Moreover, p53 and K-ras mutations were rarely found together in the same tumor, suggesting different genetic pathways leading to tumor formation. These observations are supported by mutation analysis in patients with ulcerative colitis, an inflammatory bowel disease that confers a significantly increased risk of CRC. APC mutations are relatively rare (10 %) in patients with ulcerative colitis, whereas p53 mutations are common, suggesting that loss of cell cycle and apoptotic control mechanisms through mutations in p53 may be one of the mechanisms to explain the observed increase in CRC risk [58]. Thus, in this study, a significant correlation was observed between the nuclear positivity of p53 and the OS of the patient which suggest that the patients with increased nuclear expression of p53 protein or a stable p53 protein due to mutations had a poor survival. So the nuclear expression of p53 can be used as a prognostic marker, but it should be validated on large patient cohort. Similar findings were observed by Belluco et al. [59] and Lim et al. [60].
All reported studies have conserved the adenoma→carcinoma sequence and reported the presence of mutations in adenomas, a precursor lesion that finally develops to carcinoma. However, only a very small number of the Asian patient population have adenomas; therefore, the present study included adjoining mucosa so as to determine the initial changes in CRC. But in the case of adjoining mucosa, mutations were observed in only APC gene, which suggested that there are no changes near the tumor region, and the process of tumorigenesis is restricted to a limited area.
Conclusion
Taken together, these results suggest that CRC is not the result of one event but many genetic alterations have a cumulative effect. The current study provides a number of insights into the mechanisms of colorectal tumor development. In the present study, mutations in K-ras, APC and p53 genes occurred uncommonly in the same tumor and p53 and K-ras mutations rarely co-existed in the same tumor suggesting that mutations in these genes lie on separate pathway in colorectal tumorigenesis. This data suggests that it is not the order of alterations but the cumulative effect of all the alterations that leads to CRC genesis. The frequency of alterations of all these genes in this cohort is similar to others except p53 which suggests that despite the rare occurrence of synchronous adenomas in the population studied, the pattern and frequency of alterations in these genes is almost same as compared to West which suggest that the process of tumorigenesis is similar but there is a difference at the initiation stage.
As these alterations are rarely found together in the same specimen, this suggests that these may independently initiate the carcinogenesis process and there might be an existence of more than one alternative genetic pathways leading to tumorigenesis in this population cohort. Further studies are needed to refine the causes and clinical implications of these genetic alterations and to explore the multiple alternative genetic pathways leading to the development of colorectal carcinogenesis in different ethnic and geographical cohorts with adequate number in each study population. In addition, screening of more number of genetic markers is required to elucidate their role in CRC genesis.
References
Boyle P, Lagman J. ABC of colorectal cancer—epidemiology. Br Med J. 2000;321:805–8.
Parkin DM, Muir CS, Whelan SL, Gao JT, Ferlay J, Powell J. Cancer Incidence in five continents, comparability and quality of data. Intl Agency Res Cancer Lyon France. 1992;120:45–173.
Sung JJ, Lau JY, Goh KL, Leung WK. Asia Pacific Working Group on Colorectal Cancer. Increasing incidence of colorectal cancer in Asia: implications for screening. Lancet Oncol. 2005;6(11):871–6.
Vogelstein B, Fearon ER, Hamilton SR, Kern SE, Preisinger AC, Leppert M, et al. Genetic alterations during colorectal tumor development. N Engl J Med. 1988;319:525–32.
Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell. 1990;61:759–67.
Groden J, Thliveris A, Samowitz W, Carlson M, Gelbert L, Albertsen H, et al. Identification and characterization of the familial adenomatous polyposis coli gene. Cell. 1991;66:589–600.
Kinzler KW, Vogelstein B. Lessons from hereditary colorectal cancer. Cell. 1996;87:159–70.
Fodde R, Smits R, Clevers H. APC, signal transduction and genetic instability in colorectal cancer. Nat Rev Cancer. 2001;1:55–67.
Bodmer WF, Bailey CJ, Bodmer J, Bussey H, Ellis A, Gorman P, et al. Localization of the gene for familial adenomatous polyposis on chromosome 5. Nature. 1987;328:614–6.
Nakamura Y. The role of the adenomatous polyposis coli (APC) gene in human cancers. Adv Cancer Res. 1993;62:65–87.
Bos JL. Ras oncogenes in human cancer: a review. Cancer Res. 1989;49:4682–6.
Baker SJ, Preisinger AC, Jessup JM, Paraskeva C, Markowitz S, Willson JK, et al. p53 gene mutations occur in combination with 17p allelic deletions as late events in colorectal tumorigenesis. Cancer Res. 1990;50:7717–22.
Levine AJ. p53, the cellular gatekeeper for growth and division. Cell. 1997;88:323–31.
Smith G, Carey FA, Beattie J, Wilkie MJ, Lightfoot TJ, Coxhead J, et al. Mutations in APC, Kirsten-ras, and p53—alternative genetic pathways to colorectal cancer. Proc Natl Acad Sci U S A. 2009;99(14):9433–8.
Sriram PVJ, Kochhar R, Bhasin DK, Vaiphei K, Goenka MK, Singh K. Colonoscopic surveillance for synchronous lesions in colorectal carcinoma in north India. Eur J Cancer Supp. 1998;2(34):S16.
Sambrook J, Russell DW. Molecular cloning: a laboratory manual. 3rd ed. Cold Spring Harbor: Cold Spring Harbor Laboratory Press; 2001. p. 6.4–6.12.
Ando M, Maruyama M, Oto M, Takemura K, Endo M, Yuasa Y. Higher frequency of point mutations in the c-k-ras2 gene in human colorectal adenomas with severe atypia than in carcinomas. Jpn J Cancer Res. 1991;82:245–9.
Poncin J, Mulkens J, Arends JW, De Goeij A. Optimizing the APC gene mutation analysis in archival colorectal tumor tissue. Diagn Mol Pathol. 1998;8:11–9.
Sturm I, Kohne CH, Wolff G, Petrowsky H, Hillebrand T, Hauptmann S, et al. Analysis of the p53/BAX pathway in colorectal cancer: low BAX is a negative prognostic factor in patients with resected liver metastases. J Clin Oncol. 1999;17:1364–74.
Hayashi K. PCR-SSCP: a simple and sensitive method for detection of mutations in the genomic DNA. PCR Methods Appl. 1991;1(1):34–8.
Ilyas M, Straub J, Tomlinson IP, Bodmer WF. Genetic pathways in colorectal and other cancers. Eur J Cancer. 1999;35:1986–2002.
Jeon CH, Lee HI, Shin IH, Park JW. Genetic alterations of APC, K-ras, p53, MSI, and MAGE in Korean colorectal cancer patients. Int J Color Dis. 2007;23(1):29–35.
Konig EA, Koves I, Rasinariu A, Popp AR, Kusser WC, Soyonki K, et al. Alterations of K-ras and p53 mutations in colorectal cancer patients in Central Europe. J Toxicol Environ Health A. 2001;62(5):333–47.
Esteller M, Gonzalez S, Risques RA, Marcuello E, Mangues R, Germa JR, et al. K-ras and p16 aberrations confer poor prognosis in human colorectal cancer. J Clin Oncol. 2001;19(2):299–304.
Brink M, Weijenberg MP, De Goeij AF, Schouten LJ, Koedijk FD, Roemen GM, et al. Fat and K-ras mutations in sporadic colorectal cancer in The Netherlands Cohort Study. Carcinogenesis. 2004;25(9):1619–28.
Conlin A, Smith G, Carey FA, Wolf CR, Steele RJ. The prognostic significance of K-ras, p53, and APC mutations in colorectal carcinoma. Gut. 2005;54(9):1283–6.
Samowitz WS, Holden JA, Curtin K, Edwards SL, Walker AR, Lin HA, et al. Inverse relationship between microsatellite instability and K-ras and p53 gene alterations in colon cancer. Am J Pathol. 2001;158(4):1517–24.
Van Engeland M, Roemen GM, Brink M, Pachen MM, Weijenberg MP, de Bruine AP, et al. K-ras mutations and RASSF1A promoter methylation in colorectal cancer. Oncogene. 2002;21(23):3792–5.
Onda M, Abe R, Tsuchiya A, Fukushima T, Ando Y, Yoshida T. K-ras and p53 gene mutations in colorectal cancer in 57 Japanese patients. Fukushima J Med Sci. 1997;43(1):29–39.
Pan ZZ, Wan DS, Chen G, Li LR, Lu ZH, Huang BJ. Co-mutation of p53, K-ras genes and accumulation of p53 protein and its correlation to clinicopathological features in rectal cancer. World J Gastroenterol. 2004;10(24):3688–90.
Servomaa K, Kiuru A, Kosma VM, Hirvikoski P, Rytomaa T. p53 and K-ras gene mutations in carcinoma of the rectum among Finnish women. Mol Pathol. 2000;53(1):24–30.
Luchtenborg M, Weijenberg MP, Roemen GM, de Bruine AP, van den Brandt PA, Lentjes MH, et al. APC mutations in sporadic colorectal carcinomas from The Netherlands Cohort Study. Carcinogenesis. 2004;25(7):1219–26.
Kim JC, Koo KH, Lee DH, Roh SA, Kim HC, Yu CS, et al. Mutations at the APC exon 15 in the colorectal neoplastic tissues of serial array. Int J Color Dis. 2001;16(2):102–7.
Yuan P, Sun MH, Zhang JS, Zhu XZ, Shi DR. APC and K-ras gene mutation in aberrant crypt foci of human colon. World J Gastroenterol. 2001;7(3):352–6.
Powell SM, Zilz N, Beazer-Barclay Y, Bryan TM, Hamilton SR, Thibodeau SN, et al. APC mutations occur early during colorectal tumorigenesis. Nature. 1992;359(6392):235–7.
Fujimori M, Ikeda S, Shimizu Y, Okajima M, Asahara T. Accumulation of beta-catenin protein and mutations in exon 3 of beta-catenin gene in gastrointestinal carcinoid tumor. Cancer Res. 2001;61(18):6656–9.
Frattini M, Balestra D, Suardi S, Oggionni M, Alberici P, Radice P, et al. Different genetic features associated with colon and rectal carcinogenesis. Clin Cancer Res. 2004;10(12):4015–21.
Ozaki S, Ikeda S, Ishizaki Y, Kurihara T, Tokumoto N, Iseki M, et al. Alterations and correlations of the components in the Wntsignaling pathway and its target genes in breast cancer. Oncol Rep. 2005;14(6):1437–43.
Iwamoto M, Ahnen DJ, Franklin WA, Maltzman TH. Expression of beta-catenin and full-length APC protein in normal and neoplastic colonic tissues. Carcinogenesis. 2000;21(11):1935–40.
Esteller M, Sparks A, Toyota M, Sanchez-Cespedes M, Capella G, Peinado MA, et al. Analysis of adenomatous polyposis coli promoter hypermethylation in human cancer. Cancer Res. 2000;60(16):4366–71.
Calistri D, Rengucci C, Seymour I, Lattuneddu A, Polifemo AM, Monti F, et al. Mutation analysis of p53, K-ras, and BRAF genes in colorectal cancer progression. J Cell Physiol. 2005;204(2):484–8.
Samowitz WS, Curtin K, Ma KN, Edwards S, Schaffer D, Leppert MF, et al. Prognostic significance of p53 mutations in colon cancer at the population level. Int J Cancer. 2002;99(4):597–602.
Soong R, Powell B, Elsaleh H, Gnanasampanthan G, Smith DR, Goh HS, et al. Prognostic significance of TP53 gene mutation in 995 cases of colorectal carcinoma. Influence of tumour site, stage, adjuvant chemotherapy and type of mutation. Eur J Cancer. 2000;36(16):2053–60.
Soussi T, Dehouche K, Beroud C. p53 website and analysis of p53 gene mutations in human cancer: forging a link between epidemiology and carcinogenesis. Hum Mutat. 2000;15(1):105–13.
Soussi T, Beroud C. Significance of TP53 mutations in human cancer: a critical analysis of mutations at CpG dinucleotides. Hum Mutat. 2003;21(3):192–200.
Rodrigues NR, Rowan A, Smith ME, Kerr IB, Bodmer WF, Gannon JV, et al. p53 mutations in colorectal cancer. Proc Natl Acad Sci U S A. 1990;87(19):7555–9.
Tullo A, D'Erchia AM, Honda K, Mitry RR, Kelly MD, Habib NA, et al. Characterization of p53 mutations in colorectal liver metastases and correlation with clinical parameters. Clin Cancer Res. 1999;5(11):3523–8.
Pfeifer GP, Denissenko MF, Olivier M, Tretyakova N, Hecht SS, Hainaut P. Tobacco smoke carcinogens, DNA damage and p53 mutations in smoking-associated cancers. Oncogene. 2002;21(48):7435–51.
Liu Y, Bodmer WF. Analysis of P53 mutations and their expression in 56 colorectal cancer cell lines. Proc Natl Acad Sci U S A. 2006;103(4):976–81.
Munro AJ, Lain S, Lane DP. P53 abnormalities and outcomes in colorectal cancer: a systematic review. Br J Cancer. 2005;92(3):434–44.
Soong R, Robbins PD, Dix BR, Grieu F, Lim B, Knowles S, et al. Concordance between p53 protein overexpression and gene mutation in a large series of common human carcinomas. Hum Pathol. 1996;27(10):1050–5.
Dix B, Robbins P, Carrello S, House A, Iacopetta B. Comparison of p53 gene mutation and protein overexpression in colorectal carcinomas. Br J Cancer. 1994;70(4):585–90.
Cripps KJ, Purdie CA, Carder PJ, White S, Komine K, Bird CC, et al. A study of stabilisation of p53 protein versus point mutation in colorectal carcinoma. Oncogene. 1994;9(9):2739–43.
Visscher DW, Sarkar FH, Shimoyama RK, Crissman JD. Correlation between p53 immunostaining patterns and gene sequence mutations in breast carcinoma. Diagn Mol Pathol. 1996;5(3):187–93.
Campo E, de la Calle-Martin O, Miquel R, Palacin A, Romero M, Fabregat V, et al. Loss of heterozygosity of p53 gene and p53 protein expression in human colorectal carcinomas. Cancer Res. 1991;51(16):4436–42.
Miyoshi Y, Nagase H, Ando H, Horii A, Ichii S, Nakatsuru S, et al. Somatic mutations of the APC gene in colorectal tumors: mutation cluster region in the APC gene. Hum Mol Genet. 1992;1(4):229–33.
Andreyev HJ, Tilsed JV, Cunningham D, Sampson SA, Norman AR, Schneider HJ, et al. K-ras mutations in patients with early colorectal cancers. Gut. 1997;41(3):323–9.
Brentnall TA, Crispin DA, Rabinovitch PS, Haggitt RC, Rubin CE, Stevens AC, et al. Mutations in the p53 gene: an early marker of neoplastic progression in ulcerative colitis. Gastroenterology. 1994;107(2):369–78.
Belluco C, Guillem JG, Kemeny N, Huang Y, Klimstra D, Berger MF, et al. p53 nuclear protein overexpression in colorectal cancer: a dominant predictor of survival in patients with advanced hepatic metastases. J Clin Oncol. 1996;14(10):2696–701.
Lim SC, Lee TB, Choi CH, Ryu SY, Min YD, Kim KJ. Prognostic significance of cyclooxygenase-2 expression and nuclear p53 accumulation in patients with colorectal cancer. J Surg Oncol. 2008;97:51–6.
Acknowledgements
We acknowledge the staff of OT, and Exp. Med and Biotech for their support and help in collecting the samples. Financial assistance from Indian Council of Medical research (ICMR), New Delhi is highly acknowledged.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Author contributions
Pooja Malhotra performed the research, analyzed and interpreted the data and drafted the manuscript. Rakesh Kochhar, Safrun Mahmood, Neha Nanda and Mumtaz Anwar participated in its design, analysis of data and helped to draft the manuscript. Kim Vaiphei analyzed the immunohistochemical part of the study and Jai Dev Wig provided the tissue specimens and all the clinical information regarding the patient. All authors have read and approved the final manuscript.
Rights and permissions
About this article
Cite this article
Malhotra, P., Anwar, M., Nanda, N. et al. Alterations in K-ras, APC and p53-multiple genetic pathway in colorectal cancer among Indians. Tumor Biol. 34, 1901–1911 (2013). https://doi.org/10.1007/s13277-013-0734-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-013-0734-y