
Abstract
Introduction
2,4-Dinitrophenol (DNP) is a known uncoupler of oxidative phosphorylation that clinically leads to hyperthermia, tachycardia, tachypnea, and metabolic acidosis. Intentional overdoses of DNP are often fatal. We present an analytically confirmed fatal case of DNP overdose with a falsely positive elevated salicylate concentration. We further explored this cross reactivity of DNP with two salicylate assays.
Methods
Clinically relevant serial dilutions of DNP were prepared in drug-free serum and analyzed using two different colorimetric NADH/NAD-based analytical methodologies.
Results
The enzymatic salicylate assay demonstrated a reproducible false elevation of salicylate starting at a DNP level of 100 mg/L while the EMIT-based methodology was without any such interference at the maximum concentration tested (150 mg/L).
Conclusions
DNP cross reacts with some salicylate assays. This knowledge is important for providers, as there are significant variations in the management of DNP versus salicylate toxicity.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The chemical 2,4-Dinitrophenol (DNP) was first used in World War I for munitions manufacturing [1]. It is now used in manufacturing wood preservative, dyes, explosives, and pesticides [1,2,3]. DNP ingestion was noted to cause significant weight loss and its use as a weight loss agent started in the 1930s; however, it was banned in the USA in 1938 due to its toxicity, which included deaths [4]. In the last decade, DNP exposures have increased secondary to online availability and targeted advertisement toward body builders [1]. There have been 12 published deaths associated with DNP between 2000 and 2010 [1].
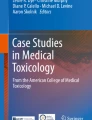
DNP acts by uncoupling oxidative phosphorylation and inhibiting ATP formation, resulting in an increased metabolic rate and hyperthermia. These effects can lead to alterations in cellular functioning, cellular necrosis, multi-organ dysfunction, and death [1,2,3,4,5]. Clinically, acute DNP toxicity presents with tachycardia, tachypnea, hyperthermia, and metabolic acidosis. Deaths are related to an increased hypermetabolic state resulting in hyperthermia and cardiac arrest. A characteristic yellow coloring sometimes stains the skin, sclera, and body fluids and is suggestive of DNP exposure [1, 2, 4, 6,7,8]. Other drugs that have a similar mechanism of action include pentachlorophenol, salicylates, [8, 9] valinomycin, and oligomycin [10]. The structures of DNP and salicylate are shown in Fig. 1. Note the structural similarity of the electron withdrawing side groups (nitro, carboxylic acid) on the aromatic ring. For comparative purposes, DNP is depicted with its phenolic proton, although at physiologic pH it is predominantly present as a resonance stabilized phenolate ion.

Structure of Dinitrophenol (left) and salicylate (right)
We present a fatality from an intentional DNP overdose, presenting with an elevated salicylate concentration. As salicylates are also uncouplers of oxidative phosphorylation, this finding was initially unexpected and clinically confusing. False positive interference of DNP on the salicylate assay has not previously been described in the literature.
Case Presentation
As we were unable to obtain consent from the patient’s next of kin, the following case has been anonymized according to JMT guidelines and approved by the editorial board since the manuscript primarily focuses on the laboratory issues involved in this clinical event.
A college student presented to the Emergency Department (ED) via EMS with an intentional self-harm ingestion of 12 tablets of dinitrophenol 250 mg (3000 mg total) 4 hours prior to arrival. Data presented by the EMS crew was consistent with a suicide attempt. En route, the patient was hyperthermic to 39.3 °C and ice packs were placed by EMS. In the ED, the patient was tachycardic to the 160 bpm, tachypneic at 40 breaths per minute, diaphoretic and had depressed consciousness. Cooling measures with ice packs and cold IV fluids were continued in the ED. Chest X-ray showed no acute abnormalities, and the EKG demonstrated sinus tachycardia at 150 bpm, QRS of 88 ms, and QTc of 404 ms, without ST segment abnormalities. The patient was intubated for airway protection, using etomidate and rocuronium, and the heart rate dropped to 90 bpm. Soon after intubation, the patient’s QRS interval widened on the monitor and pulses were lost. ACLS was initiated and continued for approximately 45 min. During the cardiac arrest resuscitation, the patient received 5 mg of epinephrine, 150 mEq of sodium bicarbonate, and 13.6 mEq of calcium chloride. The patient’s skin developed a yellow hue and increased muscular tone was noted. Despite resuscitative efforts, the patient died just over an hour after arrival. Review of laboratory testing showed a leukocytosis of 16.6 × 109/L, creatinine of 1.5 mg/dL (132 μmol/L), lactate of 3 mmol/L, glucose of 194 mg/dL (10.7 mmol/L), and potassium of 5.2 mmol/L. Urine drug screen, ethanol, and acetaminophen concentrations were negative. An elevated salicylate concentration of 224 mg/L (1.62 mmol/L) was reported.
Autopsy conducted 10 hours after the time of death demonstrated firm rigor mortis and large amounts of pulmonary edema. There was no noted abnormal yellowing of the viscera or any bodily fluids. The medical examiner determined the cause of death to be due to DNP; other substances including benzodiazepines, cocaine, ethanol, opiates/opioids and organic acids/bases/neutrals were not detected. A postmortem iliac vein blood DNP concentration determined by GC/MS was 98 mg/L; blood obtained about 1 hour prior to death demonstrated a blood DNP concentration of 120 mg/L.
A fatality associated with DNP ingestion was not surprising. However, the elevated salicylate concentration was unexpected. The question arose as to whether DNP could cause a falsely elevated salicylate concentration. To further explore this question, we performed an in vitro analysis of two commonly used clinical salicylate quantitative methods.
Methods
2,4-Dinitrophenol (DNP, 99.9% Sigma-Aldrich) was dissolved in 100 ml of pH 7.0 0.1 M phosphate buffer to a final concentration of 990 mg/L. Four dilutions of 0, 50, 100, and 150 mg/L DNP were prepared using salicylate-free serum and buffer. Samples were analyzed with two methodologies. The first was a Beckman DXC/LX 20 system using a Synchron® systems salicylate reagent with a sensitivity limit of < 40 mg/L. This relies on salicylate hydroxylase to catalyze the conversion of salicylate and NADH to catechol and NAD. It measures the change in absorbance at 340 nm, which is proportional to the amount of salicylate present; this was the methodology used in the above case report. The second method used an NAD based EMIT method where the competing antigen is labeled with G6PD with a sensitivity of < 25 mg/L. As binding occurs, enzymatic activity converting NAD to NADH is decreased and salicylate competes with the labeled antigen.
Each sample (n = 4) was analyzed twice and if there was any detectable salicylate, they were analyzed twice again. The final value of salicylate at a given concentration was the average of the four results or expressed as the sensitivity limit for the assay (i.e., none was detected).
Results
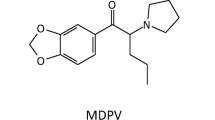
The EMIT-based methodology did not result in any detectable salicylate at any DNP concentrations. The enzymatic salicylate assay demonstrated a false elevation of salicylate starting at a DNP level of 100 mg/L. The coefficient of variance was < 2% for 100 and 150 mg/L concentrations, suggesting a stable and reproducible interference effect (Fig. 2).

Graph of the measured salicylate concentrations vs. DNP concentrations. The error bar at 50 mg/L reflects the assay detection limit of 40 mg/L of salicylate. The error bars at 100 and 150 mg/L depict a 5% coefficient of variance based on assay limits. The dotted lines suggest an estimate of the inference between 50 and 100 mg/L
Discussion
Our laboratory testing demonstrated that elevated DNP concentrations cross-react with the salicylate enzymatic assay and give a false positive result at high concentrations. This interference may be linear in fashion, but the shape of the full curve is uncertain. This is because 100 mg/L DNP resulted in a false positive salicylate concentration that was not quite twice the detection limit of the assay. If the effect was linear, half that concentration of DNP would result in a signal that would be ignored as it would not reach the detection limit, which is what was observed. The exact cause of this interference is not known; simple colorimetric interference seems unlikely, as both assays use the change in absorbance at 340 nm. The cause was probably related to cross-reactivity of the salicylate hydroxylase enzyme with DNP. Although it would be ideal to repeat the experiment to further explore where the interference began with this assay, due to administration, personnel and laboratory equipment changes, this is unfortunately not possible.
DNP is a rare ingestion, but often fatal. The lowest published lethal human oral dose reported was 4.3 mg/kg; this reference provides a comprehensive overview of the majority of deaths reported in the last 100 years [1]. Serum concentrations associated with fatalities range considerably but are usually above 25 mg/L [11]. Being aware of the cross-reactivity with the salicylate assay is important for providers to avoid mismanagement of the patient due to the potential clinical similarities.
Management choices in DNP toxicity are limited, as there is no antidote. Activated charcoal can be considered for awake patients who present within 1 hour of ingestion [1]. The mainstay of treatment focuses on aggressive IVF resuscitation and cooling of the patient with various methods such as ice packs, cooling blankets, cold IVF, or fans. Airway management with endotracheal intubation, monitoring of electrolytes, glucose, and renal function are often necessary. Benzodiazepines are the drug of choice for agitation or seizure activity [1,2,3, 5, 7]. Salicylates and anticholinergic agents should not be used, as they can worsen the hyperthermia [1, 5,6,7,8].
DNP toxicity is secondary to uncoupling of oxidative phosphorylation and inhibition of ATP formation, resulting in an increased metabolic rate and hyperthermia. These effects can lead to alterations in cellular functioning, cellular necrosis, multi-organ dysfunction, and death [1,2,3,4,5]. DNP is also reported to cause a release of calcium from intracellular stores [12]. This excessive intracellular calcium may lead to increased muscle contractions and further heat production. Dantrolene is traditionally used in malignant hyperthermia to limit the Ca2+ release from the sarcoplasmic reticulum, decrease muscular contractions, and limit further heat production [1,2,3]. This suggested mechanism of increased calcium release and muscular contractions is dantrolene has been proposed to be of benefit in DNP toxicity [1,2,3, 12].
Hemodialysis is standard of care for severe salicylate toxicity [9]. However, DNP has a pKa of 4.09, is lipophilic, and highly protein bound, making it a poor candidate for removal by hemodialysis [2, 5, 13, 14]. Nevertheless, hemodialysis may be considered for correction of acid-base dysfunctions in these cases.
Conclusion
DNP toxicity has a high fatality rate with limited available resuscitative therapies. DNP can cross-react with some laboratory salicylate assays and cause a falsely elevated salicylate concentration. This interaction is important for clinicians to be aware of beyond the diagnostic conundrum, as there are significant differences in the treatment modalities between salicylate and DNP toxicity.
References
Grundlingh J, Dargan PI, El-Zanfaly M, Wood DM. 2-4-Dinitrophenol (DNP): a weight loss agent with significant acute toxicity and risk of death. J. Med Toxicol. 2011;7:205–12.
Holborow A, Purnell RM, Wong JF. Beware the yellow slimming pill: fatal 2,4-dinitrophenol overdose. BMJ Case Rep. 2016:1–3.
McFee RB, Caraccio TP, McGuigan, Reynolds SA, Bellanger P. Dying to be thin: a Dinitrophenol related fatality. Vet Human Toxicology. Oct;46(5):251–4.
Kamour A, George N, Gwynnette D, Cooper G, Lupton D, Eddleston M, et al. Increasing frequency of severe clinical toxicity after use of 2,4-Dinitrophenol in the UK: a report from the National Poisons Information Service. Emerg Med J. 2015;32:383–6.
Hsiao AL, Santucci KA, Seo-Mayer P, Mariappan MR, Hodsdon ME, Banasiak KJ, et al. Pediatric fatality following ingestion of Dinitrophenol: postmortem identification of a “Dietary Supplement”. Clin Toxicol. 2005;43:281–5.
Leftwich RB, Floro JF, Neal RA, Wood AJJM. Dinitrophenol poisoning: a diagnosis to consider in undiagnosed fever. South Med J. 1982;75(2):182–4.
Roberts, JR, Reigart, JR. “Pentachlorophenol and Dinitrophenolic pesticides.” Recognition and Management of Pesticide Poisonings. 6th Ed. United States Environmental Protection Agency: Office of Pesticide Programs. 2013. Chapter 11:103–109.
Macnab AJ, Fielden SJ. Successful treatment of dinitrophenol poisoning in a child. Pediatr Emerg Care. 1998;14(2):136–8.
O’Malley GF. Emergency department management of the salicylate-poisoned patient. Emerg Med Clin N Am. 2007;25:333–46.
Watabe M, Nakaki T. ATP depletion does not account for apoptosis induced by inhibition of mitochondrial electron transport chain in human dopaminergic cells. Neuropharmacology. 2007;52(2):536–41.
Miranda EJ, McIntyre IM, Parker DR, Gary RK, Logan BK. Two deaths attributed to the use of 2,4-Dinitrophenol. J Anal Toxicol. 2006;30(3):219–22.
Tewari A, Ali A, O’Donnel AS, Butt M. Weight loss and 2,4-Dinitrophenol poisoning. Br J Anaesth. 2009;102(4):566–7.
2,4-Dinitrophenol. National Center for Biotechnology Information PubChem Compound Database; CID=1493, https://pubchem.ncbi.nlm.nih.gov/compound/1493 (accessed Apr. 11, 2018).
Agency for Toxic Substances and Disease Registry (ATSDR). 1995. Toxicological profile for Dinitrophenols. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service. https://www.atsdr.cdc.gov/toxprofiles/TP.asp?id=729&tid=132, https://www.atsdr.cdc.gov/toxprofiles/tp64-c2.pdf
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Consent was not available, but this case was anonymized according to JMT guidelines and publication was approved after review by members of the editorial board because the manuscript primarily focuses on the laboratory issues identified by this clinical event.
Conflicts of Interest
None.
Rights and permissions
About this article

Cite this article
Kopec, K.T., Freiermuth, C., Maynard, S. et al. Dinitrophenol (DNP) Fatality Associated with a Falsely Elevated Salicylate Level: a Case Report with Verification of Laboratory Cross Reactivity. J. Med. Toxicol. 14, 323–326 (2018). https://doi.org/10.1007/s13181-018-0677-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13181-018-0677-1