
Abstract
There is a growing recognition that people with disabilities have the same sexual needs and rights as people without disabilities. However, less attention is paid to the sexuality of people diagnosed with intellectual disabilities. This narrative review summarises what is currently known about the level of sexual health knowledge of people with intellectual disabilities. A literature review was conducted of the published literature using Google Scholar, PubMed, PsychInfo, EBSCOhost and Science Direct. Forty-eight articles were identified that addressed the question about the level of sexual health knowledge of people with intellectual disabilities. Overall, studies demonstrate that people with intellectual disabilities are highly variable in levels of sexual knowledge, but on average have a range of deficits in knowledge compared to non-disabled individuals. More tailored education and support in accessing formal and informal sources of information are needed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
There is a growing recognition that people with intellectual disabilities have the same sexual needs and rights as people without disabilities. The United Nations Convention on the Rights of Persons with Disabilities (UN 2006) states that people with disabilities have equal sexual and reproductive health rights and access to sexual and reproductive health care. However, as the First World Report on Disability published by the World Health Organization and World Bank (2011) highlights, there are significant unmet needs when it comes to the sexual and reproductive health of people with disabilities. The WHO (2006) views sexual health as part of human development and human rights, and that if sexual health is to be attained, “the sexual rights of all persons must be respected, protected and fulfilled” (p. 5). However, there is a relative paucity of research on the sexuality and sexual health of people diagnosed with intellectual disabilities.
We have used the term intellectual disabilities in this paper (in the UK, this is referred to as learning disabilities), as used in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association 2013) definition where intellectual disability is a term describing individuals who have general cognitive impairments that have an impact on adaptive functioning. There are four levels of intellectual disability: mild (IQ 50–70), moderate (IQ 35–49), severe (IQ 20–34) and profound (IQ below 20; APA 2013).
Available research shows that adults with intellectual disabilities, on average, not only present lower levels of knowledge than people without disabilities (e.g. Szollos and McCabe 1995) but might also hold negative views towards sex (Bernert and Ogletree 2012). At the same time, many people with intellectual disabilities have sexual needs and hope to be in a relationship (Froese et al. 1999; Kelly et al. 2009). Research shows that many individuals with intellectual disabilities, especially with mild impairments, are sexually active (McCabe 1999; McGillivray 1999). However, sex education is not always available (Milligan and Neufeldt 2001; Rohleder and Swartz 2012), which may have many negative consequences, such as increased risk of sexually transmitted diseases (STD; Aderemi et al. 2013). What is more is that people with disabilities, especially children, are more vulnerable to abuse than their non-disabled peers (McKenzie and Swartz 2011). Incidents of sexual abuse may go unreported due to a lack of sexual health education as well as other factors such as the attitudes of workers in protection, support and legal services towards the sexuality of people with intellectual disabilities (Meer and Combrinck 2015). Finally, some authors suggest that deficits in sexual knowledge may lead to challenging behaviour, such as masturbating in public or invading other people’s personal space (Grieve et al. 2007; Timms and Goreczny 2002).
Despite the fact that more and more carers and professionals believe that sex education is needed (Lafferty et al. 2012), many of them experience anxiety and ambivalence about discussing the topic of sexuality and relationships, often due to concerns about causing harm or beliefs that providing sex education will lead to inappropriate sexual behaviour (Rohleder 2010). In a study conducted by de Reus et al. (2015), educators working with disabled people recognised a number of challenges in their work, including barriers in communication and language, cultural values and expectations, learners’ knowledge and behaviour, handling of sexual abuse cases and the teachers’ own life experiences. In addition, many educators and teachers report being inadequately trained (Christian et al. 2001). Some parents of adolescents with intellectual disabilities have been found to be resistant to discussing sex with their offspring (Pownall et al. 2012).
As a precursor to identifying gaps in education, and responding to specified concerns by the UN (2006) and WHO (2006, 2011), information is needed on people with intellectual disabilities’ knowledge about sex. The nature and extent of support required can best be determined through a careful assessment of the general level of knowledge. Details of knowledge held are also important for the purpose of counselling or therapy, as well as when investigating potential cases of sexual abuse (Bell and Cameron 2003). Swango-Wilson (2009) writes that education is a key to empower individuals to identify, report and prevent sexual assault and abuse.
The only other published review that looks at the level of sexual health knowledge amongst people with intellectual disabilities, as well as their needs, attitudes and feelings, was written by McCabe and Schreck (1992). Thus, this review summarises what is currently known about the level of sexual knowledge amongst people with intellectual disabilities.
Method
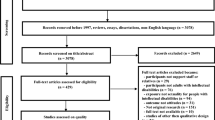
This is a narrative review, and as such, it summarises and critiques a body of literature. It has a broad research question, draws conclusions about the topic, identifies gaps and does not use systematic criteria for appraisal. The search was conducted using the following electronic databases: Google Scholar, PubMed, EBSCOhost, PsychInfo and Science Direct. Key words included: sexual knowledge, learning disability, intellectual disability, mental retardation, mental handicap, cognitive disability, mental deficiency, mental disability, retarded, mentally retarded, mentally handicapped, autism, autism spectrum disorder, ASD, Down syndrome, Down’s syndrome, Prader-Willi syndrome, Williams syndrome, Rett syndrome, Angelman syndrome, Angelman’s syndrome, fragile X syndrome, Klinefelter’s syndrome, congenital hydrocephalus, Smith-Magenis syndrome, fetal alcohol syndrome, foetal alcohol syndrome, 22q11 deletion syndrome. Articles were also identified from papers cited in the articles selected for inclusion in the review. The search was conducted between June 2013 and January 2014. The search was completed using many databases and a variety of key words; hence, it is not possible to calculate the exact number of retrieved articles. As an example, search combination that brought the most findings (889 papers) in the Google Scholar was ‘mental retardation & sexual knowledge’, whilst the same phrases in EBSCO Host were linked to 125 articles. In total, 48 articles were included. The inclusion criteria applied were: published papers, written in English and presenting original research specifically about intellectual disabilities and not disabilities in general. Included articles had to present data on the level of knowledge about sexuality and relationships in general or specific aspects of it, e.g. sexual abuse or sexually transmitted diseases. There were no criteria regarding the dates and only peer-reviewed papers were included.
O’Brien and Pearson (2004), in their review of the relationship between autism and intellectual disability, comment that, even though there is no agreement on the exact prevalence rates of disabilities amongst people with autism, as many as 75 % of individuals with autism may have an intellectual disability. Hence, research regarding individuals with autism is included in this review, with the exception of studies regarding individuals with high functioning autism (IQ ≥ 70).
Results
Forty-eight articles were identified that present original data and directly or indirectly assessed the level of sexual knowledge amongst people with intellectual disabilities and autism spectrum disorder. Two papers were case studies (Bell and Cameron 2003; Shapiro and Sheridan 1985). Therefore, it was decided that they would be excluded from the review as generalisation of findings would not be possible, leaving a total of 46 articles (see Table 1).
In these articles, level of sexual knowledge was either the main objective of the study (e.g. Kijak 2013; Leutar and Mihokovic 2007), was measured as a part of the construction of a new tool (e.g. Galea et al. 2004; McCabe 1999) or was measured as part of the evaluation of an intervention (e.g. McDermott et al. 1999). In the majority of the studies, quantitative methods or mixed methods were used to collect data, with the exception of Eastgate et al. (2011), Healy et al. (2009) and Kelly et al. (2009) who used qualitative methods.
Twenty-nine studies were conducted after 2000, which corresponds in time with an increasing emphasis in public policy on the civil rights, choice, independence and inclusion of people with intellectual disabilities (e.g. US Department of Health and Human Services 2000; UK Department of Health 2001). With regard to locality, 18 articles reported research carried out in Europe (nine in the UK, four in Ireland and one each in Croatia, Turkey, the Netherlands and Poland), 13 in the USA, 9 in Australia, 3 in Canada and 1 each in Nigeria, South Africa, Hong Kong and New Zealand.
Sample sizes vary from 4 (Dukes and McGuire 2006) to 300 participants (Aderemi et al. 2013), with the majority consisting of around 60 individuals. Samples were mainly drawn from special schools/educational settings (Aderemi et al. 2013; Bambury et al. 1999; Brantlinger 1985; Dawood et al. 2006; Fischer and Krajicek 1974; Gillies and McEwen 1981; Hall et al. 1973; Isler et al. 2009; Tang and Lee 1999; Watson and Rogers 1980) or institutions (such as residential settings and hospitals; Edmonson et al. 1979; Caspar and Glidden 2001; Forchuk et al. 1984; Hall and Morris 1976; Long et al. 2013; Niederbuhl and Morris 1993; Penny and Chataway 1982; Siebelink et al. 2006) or from offender populations (Lockhart et al. 2010; Lunsky et al. 2007; Michie et al. 2006; Murphy et al. 2007; Talbot and Langdon 2006). Only five studies recruited people living in the community (Garwood and McCabe 2000; McCabe 1999; McCabe and Cummins 1996; Szollos and McCabe 1995; Timmers et al. 1981). Thirty-one articles report research using mixed or unspecified samples, 11 with mild, 3 moderate and 1 severe intellectual disabilities.
Almost all studies examined the level of knowledge regarding sex and sexual health of people with intellectual disabilities. Three studies concerned people with autism, two of which compared people with autism and intellectual disabilities. No studies were found that reported research concerning people with genetic conditions such as Down’s syndrome, Prader–Willi syndrome or Williams syndrome.
Summary of Levels of Sexual Knowledge
In general, studies found that sexual knowledge amongst people with intellectual disabilities is often lacking in certain areas, is inaccurate or contains misconceptions. However, there are considerable individual differences and variability in the level of knowledge (Brantlinger 1985; Eastgate et al. 2011; Galea et al. 2004; Siebelink et al. 2006). In Edmonson and Wish’s (1975) study, the level of knowledge varied from 10 to 65 % correct responses to a questionnaire, and in the research of Aderemi et al. (2013) about HIV awareness, level of knowledge about HIV transmission varied from 0 to 100 % correct answers. Overall, the topic of body parts and physical characteristics appears to be the best understood, with birth control methods and STDs being the least understood. No further generalisations can be made.
Articles were grouped according to the level of disability of participants (mild, moderate and mixed or unspecified intellectual disabilities), as well as clustered into studies with participants with mean IQ at the level of 40, 50 and 60 scores. Comparisons were made between them to see whether there was a link between the level of functioning and the level of knowledge, but no generalisable conclusions can be made. This somehow surprising result might be due to factors such as lack of uniform terminology, use of poor quality assessment tools, scantiness or inadequacy of description of the samples used and/or results, and differences in samples and methods. A key finding is that no obvious differences were observed between studies across the four decades in terms of overall knowledge, which appears to be consistently low. There has also been little change in terms of methods or samples used. This is surprising given that, with deinstitutionalisation and supposedly improved sex education in schools, one would have expected a notable improvement in knowledge to be shown.
We had a look at the levels of knowledge in specific areas.
Body Parts and Physical Characteristics
Some studies report that participants present a sound knowledge of body parts and physical characteristics (Galea et al. 2004; Kijak 2013; Lindsay et al. 1992; Lockhart et al. 2010; Szollos and McCabe 1995; Timmers et al. 1981), whilst others found low levels of knowledge in these areas (Bender et al. 1983; Healy et al. 2009; Isler et al. 2009).
The difference in the above findings might be explained by several reasons. In the research conducted by Healy et al. (2009), only those under the age of 18 years had rudimentary knowledge about anatomy; older participants were well informed, which may suggest that young people with intellectual disabilities have gaps in knowledge about body parts, but the knowledge increases with age. In the Isler et al. (2009) study, participants were asked about internal organs such as tubes, ovary and uterus, as well as external ones (for example penis and vagina), which could lead to lower scores as the internal body parts might be less known to individuals with intellectual disabilities.
Sexual Intercourse
Edmonson et al. (1979), Gillies and McEwen (1981), Hall and Morris (1976) and Timmers et al. (1981) found that their participants had good comprehension of sexual intercourse, whilst Bender et al. (1983), Isler et al. (2009), Jahoda and Pownall (2014) Kelly et al. (2009), McCabe (1999) and Szollos and McCabe (1995) obtained contrary results. There are no differences in the methods and samples used in the studies that could explain these dissimilar results. It is also not clear from the papers whether the topic of ‘sexual intercourse’ refers to general sexual activity between two people or whether it is specific to heterosexual penetrative sex.
Pregnancy
There is no agreement about the level of knowledge about pregnancy, with some research showing that individuals with intellectual disabilities present good knowledge about it (Edmonson et al. 1979; Galea et al. 2004; Hall and Morris 1976; Leutar and Mihokovic 2007; Timmers et al. 1981) and others that the level is low (Bender et al. 1983; Fischer and Krajicek 1974; Kijak 2013; Lindsay et al. 1992; McCabe 1999). No differences in the methods or samples used were noticed that could account for these contrary results.
Masturbation
Contradictory results were also achieved for the level of knowledge about masturbation. Edmonson and Wish (1975), Galea et al. (2004), Hall and Morris (1976), Leutar and Mihokovic (2007) and Timmers et al. (1981) found that the knowledge about masturbation was good, whilst Bender et al. (1983), Fischer and Krajicek (1974), Garwood and McCabe (2000), Healy et al. (2009), Isler et al. (2009) and Szollos and McCabe (1995) found that it was low. When looking at the studies, nothing obvious was noticed that could explain these inconsistent outcomes.
Menstruation
Inconsistent results were also achieved in regard to knowledge about menstruation. Some authors found that the level of information was low (Galea et al. 2004; Garwood and McCabe 2000, men only; Isler et al. 2009; Lockhart et al. 2010, men only; McCabe 1999), whereas Hall and Morris (1976) and Leutar and Mihokovic (2007) found that it was good. Again, there were no observable differences between the studies that could clarify the various results.
Legal Aspects and Social Norms
Knowledge about the law on sexuality appears to be low. O’Callaghan and Murphy (2007) showed that adults with intellectual disabilities presented very limited understanding of the law, lower than the control group consisting of younger participants, but with no intellectual disabilities. Galea et al. (2004) found that knowledge of illegal behaviour was good, but insufficient for the rights of people with disabilities. In three studies (Galea et al. 2004; Healy et al. 2009, only for individuals over 18 years old; Leutar and Mihokovic 2007), participants showed good recognition of public/private spaces; in two, sound knowledge of socially appropriate/inappropriate behaviour (Leutar and Mihokovic 2007; Lockhart et al. 2010). However, Lockhart et al. (2010) concluded that participants appeared not to understand reasons why some behaviour was inappropriate.
Contraception and Sexually Transmitted Diseases
Knowledge regarding contraception and STDs appears to be the most lacking (Bender et al. 1983; Edmonson et al. 1979; Galea et al. 2004; Gillies and McEwen 1981; Hall and Morris 1976; Kijak 2013; Leutar and Mihokovic 2007; Lindsay et al. 1992; Lockhart et al. 2010), with the exception of the study conducted by Timmers et al. (1981), which found that most of the individuals had good knowledge about venereal diseases and all participants knew about contraception. However, the results achieved by Timmers et al. (1981) might be due to the scoring method used by the authors. Participants were assessed to have good knowledge if they could name one method of contraception. Hence, all 25 participants were described as knowledgeable on how to prevent pregnancy. In other studies, such as Kijak’s (2013), participants needed to name at least three methods of contraception in order to be classified as being well informed in this area. Also, in the study of Timmers et al. (1981), if participants were aware that venereal diseases were contracted through sexual contact, they were assessed as having good knowledge. In other studies, for example one by Leutar and Mihokovic (2007), participants were asked a number of questions about STDs, such as ways of transmission, prevention, their names, etc., in order to fully assess information they had about it.
The four studies investigating the level of knowledge of people with intellectual disabilities regarding HIV/AIDS (Aderemi et al. 2013; Dawood et al. 2006; Delaine 2012; McGillivray 1999) showed deficits in knowledge, especially about transmission and cure of HIV/AIDS. However, Delaine (2012) demonstrated that knowledge could be improved by training.
Factors Related to Sexual Knowledge
Differences in the level of knowledge might be due to many factors. The main reason is that people with intellectual disabilities are a very heterogeneous group and live in environments with varying levels of social restrictions. Additionally, there is diversity across different areas of the world about how intellectual disabilities should be labelled, and this review used a variety of search terms. In Europe and much of Australasia, the term ‘intellectual disabilities’ is often used differently in educational and other contexts, and which can include specific learning disabilities, intellectual disabilities and pervasive developmental disorders, whilst in the USA, the phrase ‘developmental disabilities’ is a broad umbrella term to refer to intellectual disabilities and pervasive developmental disorders (Davey 2008). Some studies, therefore, might report on a mixed group of people, some of whom may not fall into the current category definitions of having ‘intellectual disabilities’.
Individual studies show that general intelligence is positively related to levels of knowledge (Edmonson and Wish 1975; Hall et al. 1973; Konstantareas et al. 1997; Leutar and Mihokovic 2007; Michie et al. 2006; O’Callaghan and Murphy 2007; Ousley and Mesibov 1991). However, it is not clear how much the better performance of people with milder impairments is due to better communication and reading skills and how much to greater knowledge levels (Talbot and Langdon 2006). The better performance of people with higher levels of functioning might also be due to better access to sex education, especially if they attend mainstream schools, where they have access to more extensive and intensive sex education.
Hall and Morris (1976) suggest that years of institutionalisation have an impact on the level of knowledge, with those who have been institutionalised for some years having less sexual knowledge than those who have not. Similarly, Robinson (1984) found that community-based participants were more knowledgeable than those living in an institution. However, in a study conducted by Edmonson and Wish (1975), there was no correlation between years of institutional residence and correct responses.
Many authors (e.g. Lindsay et al. 1992; Penny and Chataway 1982) showed in their research that there was a significant and substantial increase in sexual knowledge after receiving sex education. Some researchers suggest that the effects of receiving sex education may be short term, not only due to cognitive abilities but also because of the lack of ability to transfer knowledge obtained during the training into real-life situations (O’Callaghan and Murphy 2007). However, research conducted by Delaine (2012), Dukes and McGuire (2006), McDermott et al. (1999), Murphy et al. (2007) and Robinson (1984) show that increases in knowledge were observed after taking part in training and on follow-up (posttests completed between 3 weeks to a year after the intervention or baseline assessment). In the study conducted by Penny and Chataway (1982), the level of knowledge continued to increase between posttest completed shortly after completion of sex education and posttest done 2 months later, despite no intervention during that period. The authors suggest that it may be due to informal learning occurring by sharing of information amongst participants who formed friendships during the sex education course.
Neither age nor gender seems to have an impact on the level of knowledge (Galea et al. 2004; Konstantareas et al. 1997; Leutar and Mihokovic 2007; McGillivray 1999; Ousley and Mesibov 1991; Siebelink et al. 2006). Only four articles showed sex differences. In three studies, men with intellectual disabilities were found to be more knowledgeable than women (Aderemi et al. 2013; Jahoda and Pownall 2014; Penny and Chataway 1982), and in one paper, women had higher levels of knowledge than men (Szollos and McCabe 1995).
It is not clear whether sexual experience is associated with sexual knowledge. Michie et al. (2006) found that sexual offenders with intellectual disabilities had higher levels of knowledge than non-offenders. According to the authors, it can be assumed that sex offenders had some experience of sexual activity, which cannot be presumed with the control participants. Other offender studies did not show a difference. Additionally, Ousley and Mesibov (1991) found no correlation between experience and level of knowledge amongst people with ‘developmental delay’ and autism.
In regard to a link between the nature of the diagnosis and level of knowledge, conclusions cannot be drawn as only three studies recruited individuals with autism, two of which compared the level of knowledge about sexuality between autistic participants and those with intellectual disabilities and found no difference (Ousley and Mesibov 1991; Konstantareas et al. 1997). No studies were found regarding other diagnoses.
Factors related to limited knowledge might be problems with communication and limited reading ability (Tang and Lee 1999). However, much of this may be down to social exclusion. Some knowledge regarding relationships comes not from formal sources, such as school, but rather informal sources such as friends and social networks. People with intellectual disabilities generally have much smaller social networks. For example, in Pownall and Jahoda’s (2014) research, disabled young people reported less formal and informal sources of sexual information and described smaller social networks than their non-disabled peers. What is more is that individuals with intellectual disabilities have much more restricted access to the types of leisure activities where people would exchange information pertaining to sexuality. Nowadays, digital exclusion of some people with intellectual disabilities may also play a role in their limited knowledge.
Consequences of Limited Knowledge
There are many possible consequences of low levels of sexual knowledge amongst people with intellectual disabilities. It is suggested that inadequate and incomplete knowledge might be contributing to the fact that people with intellectual disabilities are at greater risk of abuse (Hall and Morris 1976; Tang and Lee 1999; Turk and Brown 1993) and may increase risk of having STDs (Aderemi et al. 2013; McGillivray 1999) and unplanned pregnancies (Cheng and Udry 2005). Shapiro and Sheridan (1985) imply that limited knowledge of reproductive health care may lead to higher occurrence of undetected cancer amongst women with intellectual disabilities. However, no empirical evidence is presented for any of the above suggestions.
Some authors suggested that limited sexual knowledge might possibly account for the sexual offences of some people with intellectual disabilities (Barron et al. 2002). However, Talbot and Langdon (2006), Lunsky et al. (2007), Lockhart et al. (2010) and Michie et al. (2006) demonstrated in their research that offenders present the same or even higher levels of knowledge than people with no known history of sex offending. Timms and Goreczny (2002) suggested that lack of knowledge, especially regarding social norms, may lead to challenging behaviour, such as masturbation in public or invasion of other people’s personal space. To date, no clear evidence is available on this possibility.
Finally, Dukes and McGuire (2006) and Niederbuhl and Morris (1993) showed in their research that the higher the level of knowledge, the greater the capacity to make sexuality-related decisions. Hence, people with limited knowledge might not be able to make informed choices whether to consent to sexual behaviour or not.
Evaluation of Methods and Tools Used
The only observable change in methods over the four decades of the review is an increase in the use of qualitative methods after 2000. Samples in all studies were drawn by different means. For example, in some of the studies, participants were chosen by service managers (McGillivray 1999; Penny and Chataway 1982) or by a psychologist (Lockhart et al. 2010), which could result in the selective assessment of those with better communication skills and a preexisting interest in sexual issues. Furthermore, none of the studies report findings on representative groups of people as most used convenience sampling within a specific institutional or organisational setting. It is also worth noting that 11 studies had 25 or fewer participants with intellectual disabilities (Bambury et al. 1999; Brantlinger 1985; Caspar and Glidden 2001; Delaine 2012; Dukes and McGuire 2006; Eastgate et al. 2011; Garwood and McCabe 2000; Kelly et al. 2009; Leutar and Mihokovic 2007; Murphy et al. 2007; Szollos and McCabe 1995), which makes generalisation difficult.
Most of the researchers administered their questionnaires in a form of interview. However, it is unclear in some of the articles how the knowledge was assessed (e.g. Bender et al. 1983), which may mean that some of the information was obtained using a ‘pen and paper’ method, which could lead to non-generalisable results as only those who were able to write and were better functioning were included.
In the majority of studies, researchers used questionnaires developed for the particular study, with no or little attention paid to psychometric properties (Bender et al. 1983; Brantlinger 1985; Caspar and Glidden 2001; Hall et al. 1973; Isler et al. 2009; Penny and Chataway 1982; Timmers et al. 1981). Other measurements that had the reliability and validity assessed, and sometimes were used in more than one project, are listed and evaluated in Table 2. The authors of this review relied on information regarding the reliability/validity of the tools provided by the studies. All the tools presented were specifically developed or adapted (e.g. Sex-Ken) and evaluated in populations with intellectual disability.
General Methodological Issues
Apart from a tendency to not provide evidence of the reliability and validity of measures (described above), there are many general difficulties in assessing sexual knowledge in this population. Certain questions may be too difficult for people with intellectual disabilities to understand, especially if they use medical or formal terms. For example, Bender et al. (1983) found in their study that some of the participants did not know the word ‘masturbation’, but when the question was rephrased and they were asked about ‘playing with yourself’, they knew the answer. Additionally, some of the comprehensive measures are lengthy. For example, the Sex-Ken scale (McCabe et al. 1999; McCabe 1999, 2010) contains 248 questions, taking an hour to complete as a questionnaire and up to 3 h if completed as an interview. Siebelink et al. (2006) suggest that the assessment should take no longer than 30 min. Some people with intellectual difficulties may experience problems with memory and recalling information. Furthermore, all of the available tools are suitable only for people who communicate using speech.
Every self-report measure has limitations in terms of reliance on the respondents’ honesty, accuracy and their readiness to disclose information that may be seen as socially undesirable (Catania et al. 1990; Heiman et al. 1998). Galea et al. (2004) suggest that, since research on sexuality contains sensitive material, it can be difficult to recruit participants. Some authors (Hellemans et al. 2007; Ruble and Dalrymple 1993) chose to base their research on the estimation of proxies (e.g. parents) instead of actual individuals with intellectual disabilities or high functioning autism. One main concern is that people with difficulties and/or their parents might be reluctant to consent to take part in sexuality-related studies because it may upset them or trigger disruptive behaviour (Ousley and Mesibov 1991). However, Thomas and Kroese (2005) demonstrated in their research that there were no negative consequences of taking part in sexuality research and no increase in sexual behaviour or talk.
In the situation where participants are below 16 or 18 years old (depending on the law on age of consent in particular countries) or if they are found to be incapable of making decisions themselves, consultation with the parents/guardians is required. This might result in people who would be willing to participate being excluded. On the other hand, those who come from families where sexuality is not a taboo topic, and who might therefore achieve higher scores on sexuality knowledge measures, might be overrepresented.
Recommendations for Research and Policy
Studies have clearly established the fact that the level of knowledge is generally low. However, we need to know more about how this translates into practice. We also need more information, for example about prevalence of unsafe/safe sex practice and various factors that may affect level of knowledge.
The majority of studies have concentrated on people with mild to moderate intellectual disabilities. Far less is known about the sexuality of people with profound/ multiple disability or those who are not able to communicate verbally. More research is needed regarding specific genetic conditions, such as Prader–Willi syndrome, Williams syndrome or Angelman syndrome. We also need to know more about the interaction between disability and demographics, such as gender, sexual orientation and religion, as well as the effects of stigma and social isolation.
Several areas are worth further investigation. Research is particularly needed exploring sexual health issues across the life span, including children, adolescents, adults and older adults. More research is needed in places such as Africa, Asia and South America, as currently most of the available research has been done in Europe, North America and Australasia. Given the risk of HIV amongst people with disabilities in some of these less resourced areas of the world (see Groce et al. 2013), this is of great importance. More attention should be paid to the topic of pregnancy and reproduction as they seem to be under-researched. Finally, we need more evidence on the psychometric properties of the tools to measure levels of knowledge, with development of tools that can be used with people communicating in different ways other than speech.
This review suggests several policy recommendations. Better training and support for teachers is needed to reduce their anxiety about delivering sex education. Sexual health education has to be included (where it is not) in all school curricula, it should be tailored to the needs of learners, and education and support must be available after leaving school. It is clear from research that teaching people with intellectual disabilities is most effective when information is repeated several times, and this points to a collaborative approach between various stakeholders to ensure education takes place in school and at home.
Summary
Given the diverse range of studies, sample populations, constructs and measures used, we did not conduct a meta-analysis or systematic review, but rather a critical narrative review. We acknowledge that, to a certain extent, this can be subjective in the determination of which studies to include, the way the studies are analysed and the conclusions drawn. We also acknowledge that further critique could have been made between the study characteristics and study results, but we chose to concentrate primarily in reviewing the level of knowledge and the instruments used.
Studies demonstrate that people with intellectual disabilities are highly variable in levels of sexual knowledge, but on average have a range of deficits compared to non-disabled individuals. Comprehensive sex education, tailored to the needs of participants, is therefore needed (McCabe 1999). Overall, body parts and physical characteristics appear to be best understood, and birth control and STDs the least.
The assessment of knowledge is important so that the most appropriate and relevant materials can be included in sex education programmes. However, as McGillivray (1999) points out, although knowledge is an important factor in health-enhancing behaviour (such as safer sex practices), beliefs, attitudes and confidence need to be taken into consideration when planning interventions.
References
Aderemi, T. J., Pillay, B. J., & Esterhuizen, T. M. (2013). Differences in HIV knowledge and sexual practices of learners with intellectual disabilities and non-disabled learners in Nigeria. Journal of the International AIDS Society, 16, 1–9.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5). http://www.dsm5.org/Pages/Default.aspx. Retrieved 22 February 2014.
Bambury, J., Wilton, K., & Boyd, A. (1999). Effects of two experimental educational programs on the socio-sexual knowledge and attitudes of adults with mild intellectual disability. Education and Training in Mental Retardation and Developmental Disabilities, 34(2), 207–211.
Barron, P., Hassiotis, A., & Banes, J. (2002). Offenders with intellectual disability: the size of the problem and therapeutic outcomes. Journal of Intellectual Disability Research, 46(6), 454–463. doi:10.1046/j.1365-2788.2002.00432.x.
Bell, D. M., & Cameron, L. (2003). The assessment of the sexual knowledge of a person with severe learning disability and a severe communication disorder. British Journal of Learning Disabilities, 31, 123–129.
Bender, M. P., Aitman, J. B., Biggs, S. J., & Haug, U. (1983). Initial findings concerning a sexual knowledge questionnaire. Journal of the British Institute of Mental Handicap, 11(4), 168–169.
Bernert, D. J., & Ogletree, R. J. (2012). Women with intellectual disabilities talk about their perceptions of sex. Journal of Intellectual Disability Research, 57, 240–249.
Brantlinger, E. A. (1985). Mildly mentally retarded secondary students’ information about and attitudes toward sexuality and sexuality education. Education and Training of the Mentally Retarded, 20, 99–108.
Caspar, L. A., & Glidden, L. M. (2001). Sexuality education for adults with developmental disabilities. Education and Training in Mental Retardation and Developmental Disabilities, 172–177.
Catania, J. A., Gibson, D. R., Chitwood, D. D., & Coates, T. J. (1990). Methodological problems in AIDS behavioral research: influences on measurement error and participation bias in studies of sexual behavior. Psychological Bulletin, 108(3), 339–362. doi:10.1037/0033-2909.108.3.339.
Cheng, M. M., & Udry, J. R. (2005). Sexual experiences of adolescents with low cognitive abilities in the US. Journal of Developmental and Physical Disabilities, 17(2), 155–172.
Christian, L., Stinson, J., & Dotson, L. (2001). Staff values regarding the sexual expression of women with developmental disabilities. Sexuality and Disability, 19(4), 283–291.
Davey, G. (2008). Psychopathology: research, assessment and treatment in clinical psychology. Oxford: BPS Blackwell.
Dawood, N., Bhagwanjee, A., Govender, K., & Chohan, E. (2006). Knowledge, attitudes and sexual practices of adolescents with mild retardation, in relation to HIV/AIDS. African Journal of AIDS Research, 5(1), 1–10.
de Reus, L., Hanass-Hancock, J., Henken, S., & van Brakel, W. (2015). Challenges in providing HIV and sexuality education to learners with disabilities in South Africa: the voice of educators. Sex Education, 15(4), 333–347.
Delaine, K. (2012). A computer-based interactive multimedia program to reduce HIV transmission for women with intellectual disability. Journal of Intellectual and Disability Research, 56(4), 371–381.
Dukes, E., & McGuire, B. E. (2006). Enhancing capacity to make sexuality-related decisions in people with an intellectual disability. Journal of Intellectual Disability Research, 53, 727–734.
Eastgate, G., Van Driel, M. L., Lennox, N., & Sheermeyer, E. (2011). Women with intellectual disabilities. A study of sexuality, sexual abuse and protection skills. Australian Family Physician, 40(4), 226–230.
Edmonson, B., & Wish, J. (1975). Sex knowledge and attitudes of moderately retarded males. American Journal of Mental Deficiency, 80(2), 172–179.
Edmonson, B., McCombs, K., & Wish, J. (1979). What retarded adults believe about sex. American Journal of Mental Deficiency, 84(1), 11–18.
Fischer, H. L., & Krajicek, M. J. (1974). Sexual development of the moderately retarded child: level of information and parental attitudes. Mental Retardation, 12(3), 28–30.
Forchuk, C., Pitkeathly, F., Cook, D., Allen, J., & McDonald, D. S. (1984). Sex education and the mentally retarded. The Canadian Nurse, 80(4), 36–39.
Forchuk, C., Martin, M., & Griffiths, M. (1995). Sexual knowledge interview schedule: reliability. Journal of Intellectual Disability Research, 39(1), 35–39.
Froese, P., Richardson, M., Romer, L. T., & Swank, M. (1999). Comparing opinions of people with developmental disabilities and significant persons in their lives using the individual supports identification system (ISIS). Disability and Society, 14(6), 831–843.
Galea, J., Butler, J., Iacono, T., & Leighton, D. (2004). The assessment of sexual knowledge in people with intellectual disability. Journal of Intellectual and Developmental Disability, 29(4), 350–365.
Garwood, M., & McCabe, M. P. (2000). Impact of sex education programs on sexual knowledge and feelings of men with a mild intellectual disability. Education and training in mental retardation and developmental disabilities, 269–283.
Gillies, P., & McEwen, J. (1981). The sexual knowledge of the ‘normal’ and mildly subnormal adolescent. Health Education Journal, 40(4), 120–124.
Grieve, A., McLaren, S., & Lindsay, W. R. (2007). An evaluation of research and training resources for the sex education of people with moderate to severe learning disabilities. British Journal of Learning Disabilities, 35(1), 30–37.
Groce, N. E., Rohleder, P., Eide, A. H., MacLachlan, M., Mall, S., & Swartz, L. (2013). HIV issues and people with disabilities: a review and agenda for research. Social Science & Medicine, 77, 31–40.
Hall, J. E., & Morris, H. L. (1976). Sexual knowledge and attitudes of institutionalized and non-institutionalized retarded adolescents. American Journal of Mental Deficiency, 80(4), 382–387.
Hall, J., Morris, H. L., & Barker, H. R. (1973). Sexual knowledge and attitudes of mentally retarded adolescents. American Journal of Mental Deficiency, 77(6), 706–709.
Healy, E., McGuire, B. E., Evans, D. S., & Carley, S. N. (2009). Sexuality and personal relationships for people with an intellectual disability, part I: service-user perspectives. Journal of Intellectual Disability Research, 53, 905–912.
Heiman, J. R., Meston, C. M., Paulhus, D. L., & Trapnell, P. D. (1998). Socially desirable responding and sexuality self-reports. The Journal of Sex Research, 35(2), 148+.
Hellemans, H., Colson, K., Verbraeken, C., Vermeiren, R., & Deboutte, D. (2007). Sexual behavior in high-functioning male adolescents and young adults with autism spectrum disorder. Journal of Autism and Developmental Disorders, 37(2), 260–269.
Isler, A., Tas, F., Beytut, D., & Conk, Z. (2009). Sexuality in adolescents with intellectual disabilities. Sexuality and Disability, 27(1), 27–34.
Jahoda, A., & Pownall, J. (2014). Sexual understanding, sources of information and social networks; the reports of young people with intellectual disabilities and their non-disabled peers. Journal of Intellectual Disability Research, 58(5), 430–441.
Kelly, G., Crowley, H., & Hamilton, C. (2009). Rights, sexuality and relationships in Ireland: ‘it’d be nice to be kind of trusted’. British Journal of Learning Disabilities, 37(4), 308–315. doi:10.1111/j.1468-3156.2009.00587.x.
Kijak, R. (2013). The sexuality of adults with intellectual disability in Poland. Sexuality and Disability, 31(2), 109–123.
Konstantareas, M., Lunsky, M., Lunsky, Y., & Lunsky, J. (1997). Sociosexual knowledge, experience, attitudes, and interests of individuals with autistic disorder and developmental delay. Journal of Autism and Developmental Disorders, 27(4), 397–413.
Lafferty, A., McConkey, R., & Simpson, A. (2012). Reducing the barriers to relationships and sexuality education for persons with intellectual disabilities. Journal of Intellectual Disabilities, 16(1), 29–43.
Lambrick, F., & Glaser, W. (2004). Sex offenders with an intellectual disability. Sexual Abuse: A Journal of Research and Treatment, 16(4), 381–392.
Leutar, Z., & Mihokovic, M. (2007). Level of knowledge about sexuality of people with mental disabilities. Sexuality and Disability, 25(3), 93–109.
Lindsay, W. R., Bellshaw, E., Culross, G., Staines, C., & Michie, A. (1992). Increases in knowledge following a course of sex education for people with intellectual disabilities. Journal of Intellectual Disability Research, 36(6), 531–539.
Lockhart, K., Guerin, S., Shanahan, S., & Coyle, K. (2010). Expanding the test of counterfeit deviance: are sexual knowledge, experience and needs a factor in the sexualised challenging behaviour of adults with intellectual disability? Research in Developmental Disabilities, 31(1), 117–130. doi:10.1016/j.ridd.2009.08.003.
Long, C. G., Krawczyk, K. M., & Kenworthy, N. E. (2013). Assessing the sexual knowledge of women in secure settings: the development of a new screening measure. British Journal of Learning Disabilities, 41(1), 51–65. doi:10.1111/j.1468-3156.2011.00722.x.
Lunsky, Y., Frijters, J., Griffiths, D. M., Watson, S. L., & Williston, S. (2007). Sexual knowledge and attitudes of men with intellectual disability who sexually offend. Journal of Intellectual and Developmental Disability, 32(2), 74–81.
McCabe, M. P. (1999). Sexual knowledge, experience and feelings among people with disability. Sexuality and Disability, 17(2), 157–170.
McCabe, M. P. (2010). Sexual knowledge, experience, feelings and needs scale. In T. D. Fisher, C. M. Davis, W. L. Yarber, & S. L. Davis (Eds.), Handbook of sexuality-related measures (pp. 462–463). New York: Routledge.
McCabe, M. P., & Cummins, R. A. (1996). The sexual knowledge, experience, feelings and needs of people with mild intellectual disability. Education and Training in Mental Retardation and Developmental Disabilities, 31(1), 13–21.
McCabe, M. P., & Schreck, A. (1992). Before sex education: an evaluation of the sexual knowledge, experience, feelings and needs of people with mild intellectual disabilities. Journal of Intellectual and Developmental Disability, 18(2), 75–82.
McCabe, M. P., Cummins, A., & Deeks, A. A. (1999). Construction and psychometric properties of sexuality scales: sex knowledge, experience, and needs scales for people with intellectual disabilities (SexKen-ID), people with physical disabilities (SexKen-PD), and the general population (SexKen-GP). Research in Developmental Disabilities, 20(4), 241–254.
McDermott, S., Martin, M., Weinrich, M., & Kelly, M. (1999). Program evaluation of a sex education curriculum for women with mental retardation. Research in Developmental Disabilities, 20(2), 93–106. doi:10.1016/S0891-4222(98)00035-3.
McGillivray, J. A. (1999). Level of knowledge and risk of contracting HIV/AIDS amongst young adults with mild/moderate intellectual disability. Journal of Applied Research in Intellectual Disabilities, 12(2), 113–126. doi:10.1111/j.1468-3148.1999.tb00070.x.
Mckenzie, J., & Swartz, L. (2011). The shaping of sexuality in children with disabilities: AQ methodological study. Sexuality and Disability, 29(4), 363–376.
Meer, T., & Combrinck, H. (2015). Invisible intersections: understanding the complex stigmatisation of women with intellectual disabilities in their vulnerability to gender-based violence. Agenda, 29(2), 14–23.
Michie, A. M., Lindsay, W. R., Martin, V., & Grieveo, A. (2006). A test of counterfeit deviance: a comparison of sexual knowledge in groups of sex offenders with intellectual disability and controls. Sexual Abuse, 18(3), 271–278.
Milligan, M. S., & Neufeldt, A. H. (2001). The myth of asexuality: a survey of social and empirical evidence. Sexuality and Disability, 19(2), 91–109.
Murphy, G., Powell, S., Guzman, A., & Hays, S. (2007). Cognitive-behavioural treatment for men with intellectual disabilities and sexually abusive behaviour: a pilot study. Journal of Intellectual Disability Research, 51, 902–912.
Niederbuhl, J. M., & Morris, C. D. (1993). Sexual knowledge and the capability of persons with dual diagnoses to consent to sexual contact. Sexuality and Disability, 11(4), 295–307.
O’Brien, G., & Pearson, J. (2004). Autism and learning disability. Autism, 8(2), 125–140. doi:10.1177/1362361304042718.
O’Callaghan, A. C., & Murphy, G. H. (2007). Sexual relationships in adults with intellectual disabilities: understanding the law. Journal of Intellectual Disability Research, 51(3), 197–206.
Ousley, O. Y., & Mesibov, G. B. (1991). Sexual attitudes and knowledge of high-functioning adolescents and adults with autism. Journal of autism and developmental disorders, 21(4), 471–481.
Penny, R., & Chataway, J. (1982). Sex education for mentally retarded persons. Australia and New Zealand Journal of Developmental Disabilities, 8(4), 204–212.
Pownall, J. D., Jahoda, A., & Hastings, R. P. (2012). Sexuality and sex education of adolescents with intellectual disability: mothers’ attitudes, experiences, and support needs. Intellectual and Developmental Disabilities, 50(2), 140–154.
Robinson, S. (1984). Effects of a sex education program on intellectually handicapped adults. Australia and New Zealand Journal of Developmental Disabilities, 10(1), 21–26.
Rohleder, P. (2010). Educators’ ambivalence and managing anxiety in providing sex education for people with learning disabilities. Psychodynamic Practice, 16(2), 165–182.
Rohleder, P., & Swartz, L. (2012). Disability, sexuality and sexual health. In P. Aggleton, P. Boyce, H. L. Moore, & R. Parker (Eds.), Understanding global sexualities (pp. 138–152). Abingdon: Routledge.
Ruble, L. A., & Dalrymple, N. J. (1993). Social/sexual awareness of persons with autism: a parental perspective. Archives of sexual behavior, 22(3), 229–240.
Shapiro, E. S., & Sheridan, C. A. (1985). Systematic assessment and training of sex education for a mentally retarded woman. Applied Research in Mental Retardation, 6(3), 307–317.
Siebelink, E. M., de Jong, M. D. T., Taal, E., & Roelvink, L. (2006). Sexuality and people with intellectual disabilities: assessment of knowledge, attitudes, experiences, and needs. Mental Retardation, 44(4), 283–294. doi:10.1352/0047-6765(2006)44[283:SAPWID]2.0.CO;2.
Swango-Wilson, A. (2009). Perception of sex education for individuals with developmental and cognitive disability: a four cohort study. Sexuality and Disability, 27(4), 223–228.
Szollos, A. A., & McCabe, M. P. (1995). The sexuality of people with mild intellectual disability: perceptions of clients and caregivers. Australia and New Zealand Journal of Developmental Disabilities, 20(3), 205–222.
Talbot, T. J., & Langdon. (2006). A revised sexual knowledge assessment tool for people with intellectual disabilities: is sexual knowledge related to sexual offending behaviour? Journal of Intellectual Disability Research, 50(7), 523–531. doi:10.1111/j.1365-2788.2006.00801.x.
Tang, C. S., & Lee, Y. K. (1999). Knowledge on sexual abuse and self-protection skills: a study on female Chinese adolescents with mild mental retardation. Child Abuse & Neglect, 23(3), 269–279. doi:10.1016/S0145-2134(98)00124-0.
Thomas, G., & Kroese, B. S. (2005). An investigation of students’ with mild learning disabilities reactions to participating in sexuality research. British Journal of Learning Disabilities, 33(3), 113–119.
Timmers, R. L., DuCharme, P., & Jacob, G. (1981). Sexual knowledge, attitudes and behaviors of developmentally disabled adults living in a normalized apartment setting. Sexuality and Disability, 4(1), 27–39.
Timms, S., & Goreczny, A. J. (2002). Adolescent sex offenders with mental retardation: literature review and assessment considerations. Aggression and Violent Behavior, 7(1), 1–19. doi:10.1016/S1359-1789(00)00031-8.
UK Department of Health (2001).Valuing People: A New Strategy for Learning Disability for the 21st Century. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/250877/5086.pdf. Retrieved 24 February 2014
United Nations. (2006). Convention on the rights of persons with disabilities. Geneva: United Nations.
U.S. Department of Health and Human Services (2000). The Developmental Disabilities Assistance and Bill of Rights Act of 2000. https://www.gpo.gov/fdsys/pkg/PLAW-106publ402/html/PLAW-106publ402.htm. Retrieved 24 October 2016
Turk, V., & Brown, H. (1993). The sexual abuse of adults with learning disabilities: results of a two-year incidence survey. Mental Handicap Research, 6(3), 193–216.
Watson, S. (2002). Sex education for individuals who have a developmental disability: the need for assessment. Unpublished Master dissertation. Brock University, Ontario, Canada.
Watson, G., & Rogers, R. S. (1980). Sexual instruction for the mildly retarded and normal adolescent. Health Education Journal, 39(3), 88–95.
World Health Organization. (2006). Defining sexual health. Report of a technical consultation on sexual health, 28–31 January 2002, Geneva. http://www.who.int/reproductivehealth/publications/sexual_health/defining_sexual_health.pdf. Retrieved 24 February 2014.
World Health Organization and World Bank. (2011). World report on disability 2011. http://www.who.int/disabilities/world_report/2011/report.pdf. Retrieved 11 April 2014.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study had no funding.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Conflict of Interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Borawska-Charko, M., Rohleder, P. & Finlay, W.M.L. The Sexual Health Knowledge of People with Intellectual Disabilities: a Review. Sex Res Soc Policy 14, 393–409 (2017). https://doi.org/10.1007/s13178-016-0267-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13178-016-0267-4