
Abstract
Background
Currently considered an occupational disease, the burnout syndrome affects 13–27% of the active population in multiple occupational sectors of the modern world.
Objectives
Considering the burnout syndrome from the new perspective of the predictive, preventive, personalized medicine concept as a pathological entity with a predictable appearance and evolution which allows a preventive approach and a personalized therapy, the main objective of the study is to highlight the possibility of psychotherapeutic interventions for producing measurable psychological changes in order to decrease the burnout level of hospital nurses.
Method
The research design is experimental, the independent variable being the participation or non-participation of nurses in psychotherapeutic sessions where specific classical psychodrama techniques are originally used. Nurses previously identified with medium or high levels of burnout participated in the clinical study, split into two groups: the experimental one, with 150-min weekly sessions, and the control one, without any intervention. Pre- and post-intervention questionnaires were administered to the members of both groups.
Results
The statistical analysis of the differences between pre- and post-intervention revealed (a) the decrease of the levels of personal burnout and of burnout generated by the working conditions and (b) the decrease of the depression and of anxiety on four dimensions (self-awareness, ergic tension, veiled and general anxiety).
Conclusions
The classical psychodrama method can be an effective solution in the prophylaxis and treatment of the burnout syndrome. The multidisciplinary approach according to the PPPM concept including changes of the environmental factors within the professional framework associated with stress control programmes can be promising solutions for the management of this syndrome.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Increasingly in recent years, the scientific community has been concerned with the debate and analysis of the influence of burnout on individuals and the society as a whole, transformed from a simple phenomenon, into a syndrome characteristic of the modern world. Freudenberger, after scientific observations, was the first to use the term of professional burnout in 1974 [1]. Subsequently, burnout was defined differently by Pines and Aronson, as a mental state that negatively affects especially those individuals who have other people as object of their work. Shaefeli stated that burnout differs from stress by several factors and it is characterized by difficulties of adaptation, as a result of prolonged stress and by a multidimensional symptomatology with specific attitudes [2].
The best known and the most widely used definition of burnout was given by Christina Maslach as being a “syndrome characterized by emotional exhaustion (depletion of emotional resources and decrease of individual energy), depersonalization (negative attitudes and feelings, insensitivity, and lack of compassion for the customers), and lack of personal accomplishment starting from a negative self-evaluation of one’s own professional activity and ending with feelings of diminished competence” [3, 4]. In the present, after this fuzzy definition was cleared, although the burnout syndrome has a specific place in ICD-10, being listed in the Z 73.0 category, it has not been yet mentioned in the Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-V) [4, 5]. However, the World Health Organization (WHO) recently updated its definition, including it in the International Classification of Diseases 11th Revision (ICD-11) as an occupational phenomenon and not as a medical condition. Burnout is defined in ICD-11 as follows: “a syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed. It is characterized by three dimensions: a) feelings of energy depletion or exhaustion; b) increased mental distance from one’s job, or feelings of negativism or cynicism related to one’s job; c) reduced professional efficacy. Burnout refers specifically to phenomena in the occupational context and should not be applied to describe experiences in other areas of life” [6].
Burnout can affect employees in many occupational sectors, occurring in 13–27% of the working population. For this reason, it was studied over time in various fields, teachers [7,8,9] and medical staff being most often affected by this syndrome [10].
Unlike employees in other sectors of public services, those in the medical sector are more frequently exposed to the burnout syndrome. The cause of its high frequency is related both to the occurrence of numerous, successive and far too frequent systemic changes in the health sector and, in particular, to the specificity of the profession [11,12,13]. As for the Romanian public health system, one of the main causes of burnout is the difficult and prolonged transition from the centralized system to the modern one, whose characteristics, constantly changing, determine the occurrence of stress effects, both individual and organizational [14].
Other factors which could cause burnout are the long work period in 12-h shifts [15], the existence of a second job [16], the multiple, repetitive interactions with specific categories of patients (uncooperative, aggressive or/and in terminal stages) [17,18,19], the permanent increase of responsibility and the precarious working conditions [20] and the lack of an organizational system to recognize and reward the proven performance of the nurses at the workplace [12, 13, 21, 22].
Despite the fact that the negative impact of burnout on the medical staff, on the patient and on the organization was demonstrated in numerous published studies [23,24,25,26,27], the attention paid by hospital managers to understand its generating causes (sources), to take measures for the prophylaxis or intervention in case of burnout and, in particular, to elaborate concrete strategies in this regard proved to be relatively small up to date, at least compared to other areas of activity.
In order to prevent, manage or treat the burnout syndrome, first of all, it is necessary that the medical personnel have a clear perception of what it represents, what causes it and which conditions favour it. Thus, an adequate level of understanding both from the medical staff and from the decision makers would allow measures to be taken to support its prophylaxis and to decrease the effects of the burnout syndrome. Intervention programmes could be carried out with the purpose of either treating the medical personnel identified with burnout or preventing the occurrence of this syndrome.
The clinical picture of the burnout syndrome comprises an association of symptoms of social dysfunction and psychosomatic and somatic disorders [28]. These symptoms are associated with a general emotional, physical and psychological distress [1]. The psychological symptoms are the feelings generated by frustration, anger, dissatisfaction and anxiety. The appearance of these feelings or emotions is normal in any workplace, but people, “trapped” in the cycle of exhaustion, experience these negative emotions in an almost continuous way. Most people who experience this syndrome of emotional exhaustion no longer see themselves in the workplace that they once considered interesting, showing indifference to the medical act or to the patients.
Regarding the presence of physical signs and symptoms, they are usually interpreted as pathological, but in the case of burnout, they are often psychosomatic in nature [29]. The physical problems associated with emotional exhaustion include headaches, digestive disorders, high blood pressure, palpitations and insomnia [30]. Even a moderate amount of stress can cause the medical staff to materialize the risk of high blood pressure, cardiovascular disease and even diabetes. The burnout syndrome is often manifested through behavioural reactions, such as slowness, absenteeism, poor work performance, lack of interest and commitment. Health professionals are often less empathetic, have a lower tolerance for somewhat difficult patients, consume alcohol or caffeine excessively or adopt unhealthy eating habits [29].
The effect of the occupational exhaustion syndrome on health is proven paraclinically, too. Studies show that in patients with burnout there are changes in the hypothalamo-hypophyseal axis (HPA) and in the sympatho-adreno-medullary axis (SAM) [31]. Also, the low concentration of brain-derived neurotrophic factor (BDNF) appears to be associated with the burnout symptoms, including changes in cognitive functioning [32].
S100B (glial marker S100 B) can also be used as a screening marker to detect people at high risk of developing depressive or exhaustion syndromes, meaning that increased levels of S100B can be correlated with high scores of depression and emotional exhaustion in the burnout syndrome [33].The diversity of the nonspecific symptoms of the burnout syndrome requires its multidisciplinary approach [28].
Of all the new concepts of multidisciplinary approaches in modern medicine, preventive and personalized medicine (PPPM) proved to be the most comprehensive. Since 2011 the promoters of this new concept set as main objective the creation of future strategies in order to consolidate the innovative field of preventive, predictive and personalized medicine, allowing innovation in science and healthcare. From the strategic developments designed and discussed, the implementation of personalized medicine from the practitioner and patient perspectives remains one of the most rewarding for researchers [34].
Nowadays, it is well known that PPPM is the new integrative concept in healthcare sector that enables to predict individual predisposition before onset of the disease, to provide targeted preventive measures and create personalized treatment algorithms tailored to the person. Replacing the delayed intervention by predictive medicine tailored to the person, the reactive by preventive medicine and the disease by wellness, this integrative approach of PPPM is considered as the medicine of the future [35]. In this context, the approach of the burnout syndrome in the PPPM paradigm is possible, it is even mandatory, as long as it can be studied as a pathological entity characterized by a predictable occurrence and evolution, allowing even a preventive approach and a personalized therapy. The inclusion of the burnout syndrome in the pathologies that can be approached from the point of view of this concept is also highlighted by the establishment of “Environment and Health Psychology” as a specialized professional section among the prioritized medical fields of the European Association for Predictive, Preventive and Personalized Medicine.
The systematic approach of the burnout syndrome will support the same objective of the EPMA: primarily to produce an evidence-based consensus for sustainable guidelines in predictive medicine together with targeted prevention in healthy individuals, persons at-risk and stratified patient groups with manifest diseases and secondly, to provide advice to stratified patient groups and institutions, using the assessment and intervention tools of health psychology, too [36].
Finally, representing not only innovative biomedical sciences but also advanced healthcare services focusing on the patient’s needs and the optimal solutions for society as a whole, the PPPM concept includes global healthcare benefits and creation of new institutions to facilitate the development of PPPM services in healthcare [37]. As an innovative technology to be implemented in personalized medicine, the therapeutic intervention should be applied before the disease symptoms appear [38].
Starting from a previous study [5] in which there were identified the personality traits of the employees predisposed to burnout and the relation between them and certain characteristics of their work, the research continues with a group psychotherapy intervention for nurses identified with medium or high levels of burnout, using as methods the classic psychodrama and the identification of their cognitive and emotional coping strategies.
Psychodrama is a psychodynamic group therapy, in which the inner world of the individual is explored through action. The patient is encouraged to talk about the important relationships in his life, in order to reveal the unconscious contents, relieving the psychic tension. In psychodynamic psychotherapies, expressive therapy by means of insight (which has the effect of alleviating the symptoms, including those of the burnout syndrome) and supportive therapy (determining the immediate relief of the suffering) are used. The active involvement of the whole person, not just the mind or the body (as in other therapies), facilitates raising awareness of the disharmonious relationship between the two. In this way, the alleviation of the physical or mental symptoms present in the case of burnout syndrome, too, can be obtained [39]. Moreover, emphasizing increasing spontaneity and creativity, the psychodrama therapy leads to a more flexible and varied adaptation to the needs and demands of life, including the workplace.
The founder of this psychotherapeutic method, the psychiatrist Jacob Levy Moreno, one of the pioneers of group psychotherapy, believed that the main goal of psychodrama is to achieve a specific therapeutic framework, using as a model life with its ways of living, starting with its universal elements. Convinced of its therapeutic valences, he saw in psychodrama an effective method of expression, relief, self-knowledge and communication, both verbal and non-verbal.
Many researches unequivocally demonstrated that group therapy is a highly effective type of psychotherapy, especially because it offers significant benefits to participants. Also, it was scientifically highlighted that the level of burnout is lower when the subjects (so also the nurses) choose to actively share their feelings, dissatisfactions, and personal frustrations with colleagues. Groups have the effect of reducing feelings of isolation, of promoting collegial support, professionalism and commitment. These support groups provide practical advice and information for those in similar difficult situations, thus highlighting the fact that their problems are not unique and solutions can be found to problems that are common to several subjects [39].
Feedback on the performance of the professional act is the factor that proved to be most strongly related to job (in)satisfaction. Nurses usually receive very little fair and helpful feedback on their professional activity [40] so that, in addition to expressing their feelings directly, increasing self-confidence and experiencing new interpersonal behaviours, participants receive and provide support and feedback within the group [39].
The techniques specific to psychodrama facilitate the nurses’ description of their experiences with certain patients and, in particular, the identification of the central emotion generated by this interaction. Psychodrama helps nurses understand themselves, explore the others’ perspective and connect their own thoughts or feelings with those of their patients, thus becoming an effective tool in addressing communication issues that arise in healthcare [41].
By implementing a psychological empowerment programme based on psychodrama, the authors of a study noticed the improvement of adaptive mechanisms and perceptions in the workplace. There was also a decrease in the nurses’ level of exhaustion and fatigue [42]. The psychodrama activities enhanced the participants’ ability to develop creative solutions to problems and their conflict management skills. In addition, nurses who participated in such programmes developed their capacity for introspection and empathy. Programmes based on psychodrama techniques also had a positive effect on the characteristics of the workplace, in the sense of enhancing communication, solidarity, responsibility among colleagues and increasing job satisfaction [42].
Moreno believed that individuals are influenced by the society in which they live and work, and that, in their turn, they influence this society [39]. The interaction between the nurse and the patients, respectively their families, is a major feature of the nurse profession, as nurses face a number of emotional, psychological and behavioural states. For this reason, it is essential for nurses to develop the ability to interact with patients in creative and spontaneous ways that enable safe and effective healthcare.
The objectives of the study
The study investigates the extent to which the participation of nurses in the therapy group determines the decrease of the burnout levels and of the anxiety and depressive states; at the same time, we followed the extent to which the participation in the therapy sessions produced changes in the participants’ coping strategies and in the nurses’ perception regarding the usefulness of such groups in hospitals and their desire to participate in them.
Research questions
Are psychodrama psychotherapeutic techniques effective in reducing burnout, anxiety and depression?
Can the participation of nurses in the therapy group lead to changes in the coping strategies used?
Material and method
An experimental design (pilot study) was used, the independent variable being represented by the participation or non-participation of the nurses in the psychotherapeutic sessions. The dependent variables are the levels of anxiety, depression and burnout and the emotional or cognitive coping strategies.
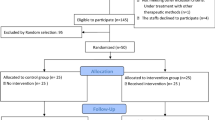
The participants were selected from a previous study conducted on 192 nurses, based on their scores for Copenhagen Burnout Inventory-the Romanian version (CBI-R) [4, 43]. From this sample, we selected 23 participants identified with medium (scores higher than 2.32 for the total burnout score for CBI-R) or high (scores higher than 3.01 for the total burnout score for CBI-R) levels of burnout manifestations, and who, in addition, expressed their desire to participate in the study. For the clinical study, there were 23 nurses grouped in two samples: an experimental one, consisting of 11 nurses who attended the therapy sessions, and a control one, consisting of 12 nurses who did not receive any intervention. The study was conducted between 07 June and 14 August 2018 with 150-min weekly meetings. After obtaining the consent of the group members and informing them about the purpose of the study, all 10 therapy sessions were video recorded. Also, the members of the group were assured of observing the confidentiality of the data obtained. The questionnaires were administered pre- and post-intervention both to the experimental group and to the control one, at the same time intervals. The nurses participating in the study were at that time working in the County Clinical Emergency Hospital Brasov.
The mean age of the study participants, both in the control group and in the experimental group, was 41 years old (Table 1).
Ethical aspects and rules regarding participation in the therapy group
The rules established from the beginning referred to the presentation by the participants of their own thoughts, opinions, in the sense of their personal use and not resorting to generalizations. Also, the group members had to express their opinion clearly, concretely, sincerely and directly in front of the group colleagues and not to “transfer” the discussions outside the therapy group. It was explained to the attending nurses that maintaining confidentiality was extremely important in order to create a safe environment for the therapeutic labour in the context where, in situations that could have a high therapeutic impact, an increased trust in the group was absolutely necessary.
From the beginning, it was specified that their evolution as participants will be monitored by video recordings and the data obtained will be analysed and used, possibly in publications, but without the possibility for anyone to be identified directly or indirectly. Regarding the expected behaviour in the group, the participants were encouraged to provide support to group members when necessary, to ask questions, to share their own thoughts and feelings with the others. If they were asked to share their impressions about each other or about the situations and experiences presented in the group, it was explained that it should be done in a constructive, direct and honest way, without criticism or judgments. Another important aspect that was emphasized right from the first meeting was the need for regular attendance and active participation in therapy sessions, as an expression of the involvement, respect and importance shown by the participants in the group.
Instruments
Burnout was measured through the Copenhagen Burnout Inventory - the Romanian version which contains 18 items on a 5-point Likert scale. The questionnaire has three dimensions and the Cronbach’s alpha coefficient is higher than .90 for each dimension [43]. The personal burnout dimension refers to the personal exhaustion, the degree of physical and mental fatigue experienced by the person. The work-related burnout dimension represents the degree of perceived physical and psychological fatigue related to the professional activity. The patient-related burnout dimension refers to the degree of physical and mental fatigue and exhaustion perceived by the affected person as being related to their work with clients/patients.
Anxiety was measured with the Catell Anxiety Scale, a 40-item questionnaire that identifies the overt (symptomatic) anxiety and the covert anxiety: internal tension, emotional instability, lack of self-confidence and the appearance of fears or different psychosomatic manifestations [44]. The items are divided into 4 sections. The Q3 factor indicates the degree of integration or non-integration of the individual depending on the development of their self-awareness. The C factor refers to the strength of the Ego, the ability of the individual to control themselves, to recognize their feelings and tensions and to express them in a realistic and adaptive way. The weak Ego is incapable of self-control and uses multiple maladaptive defences that are also associated with anxiety. The L Factor refers to the appearance of the feeling of social insecurity and paranoid tendencies that generate anxiety. The Q4 Factor—the ergic tension represents the degree to which anxiety is caused by unsatisfied pressures, needs, impulses, of any kind. High scores on this scale are associated with behaviours characterized by emotionality, tension, irritability and nervousness [44]. The O Factor is known to represent depressive anxious guilt. The guilt combined with self-blame is caused by the pressures of the Super Ego, which subsequently generates the state of anxiety and depression.
Depression was measured with the Zung Depression Scale. The scale is composed of 20 items and covers three areas: affectivity, somatic symptoms and psychological symptoms. Each item is scored on a 4-point Likert scale depending on the frequency of the symptom (1 = never or rarely, 2 = sometimes, 3 = often, 4 = most times) [45].
The coping mechanisms are measured with the Cognitive-Emotional Coping Questionnaire (CERQ). CERQ identifies a person’s cognitive coping strategies after experiencing certain situations or events with negative impact. The questionnaire can identify to what extent a person is using adaptive or maladaptive coping strategies. The 36 items cover nine scales: self-blame, acceptance, rumination, positive refocusing, refocusing on planning, positive reassessment, putting into perspective or thoughts that minimize the severity of the event, catastrophizing, and, ultimately, blaming others. The items are scored on a 5-point Likert scale (1 = almost never; 2 = sometimes; 3 = usually, 4 = often; 5 = almost always) [46].
Description of the activities carried out within the group
The first meeting aimed at the mutual acquaintance of the participants, the development of group cohesion through specific techniques and the creation of a group atmosphere necessary for opening, self-disclosure and work with intrapsychic contents. Also, during this session, the participants were asked to fill in the questionnaires presented as research tools.
The second meeting aimed, in addition to increasing group cohesion, at the development of communication skills and the creation of intense and positive relationships between the group members. Some specific techniques used during this meeting were aimed at highlighting the central feeling experienced by the group members in specific situations and to work later on it. What the subject experienced through the actor Self and the reflections on what they experienced (of the observant Self) are brought together in the field of their consciousness. They have insights, they clarify their feelings, they realize their unmet needs and desires, living fulfilments of these desires and needs and reflecting on those experiences.
The third meeting had as main objectives the inter-knowledge and the development of communication and self-analysis skills. Also, during this meeting, there were held activities to develop the capacity of introspection, to identify their own creative capacities and personal resources needed to activate them in various problematic situations (family, professional). As other meetings, the session ended with the final feedback in which the group members shared their opinions, experiences, emotions about the experience lived in that psychodrama session.
The fourth session aimed for the participants to find “anchors”, to find or become aware of the support network and to learn strategies of relaxation in stressful situations.
In the fifth psychodrama session, the development of communication skills, the ability to empathize, the construction of new behavioural models through psychodrama techniques and the identification of alternative ways of solving problems in the professional environment were pursued. For the group members, this meeting was “revealing”, “relaxing”, “liberating”, and “disturbing”, which allowed them to declare that they left the group activity with “desire to return”, “wiser”, with “feelings of trust” or “peace”.
In the sixth session, we presented to the group members a material on what the burnout syndrome means, how it can be recognized, about its causes and about its consequences at the organizational level and especially at the individual level. Also, the prevention and intervention modalities that can be used from the starting moment of this syndrome were presented. Before the presentation, the nurses were asked if they knew what the burnout syndrome was. Surprisingly, we discovered that only one participant in the 11 could answer the question.
The seventh session had as main objective the development of (family, professional) problem solving strategies, including the offering of new perspectives by the other participants. Also, in this psychodrama session, we aimed to encourage free expression, communication and social interaction.
The eighth session aimed at the inter-knowledge, the development of trust among the group members, introspection and reflection, the development of communication skills, awareness and improvement of relationships in the professional environment. In addition to developing certain skills needed in the nursing profession, we also wanted to highlight, raise awareness and improve relationships in the workplace. To this end, the group members were encouraged to reflect on their professional environment and the relationships with colleagues or hierarchical superiors.
The ninth session had as main objective the learning of relaxation and meditation techniques. The application of these methods had the role of teaching the participants certain relaxation techniques in order to calm down during tense situations and to restore their personal emotional balance. The experience of this psychodrama session was for the members of the group “awakening”, “emotional”, “revealing”. “Disturbing, stirring, moving ... It’s like when you disturb the water that has apparently been quiet, but eventually the disorder calms down, it settles in another order ....” The group members said that they left the meeting with feelings of “sadness”, “melancholy”, “relief because I also told others how I feel”, with “exhaustion” or “an experience I may never have again and I do not want to forget it too soon!”.
The tenth session represented the final phase of the self-knowledge and personal development group.
The main purpose of this session was to explore the final feelings from the participants’ perspective and the group as a whole, but also the leader of the study in his dual quality, as therapist and researcher. Although the purpose of this last meeting was to end the group’s activity on an optimistic, cheerful note, it was again emphasized that this profession, being a nurse, was extremely emotionally consuming and that nurses had a huge need for support and good emotional management.
Starting from each participant’s motivation, expectations, objectives to be part of this psychodrama group, revealed in the first meeting, it was identified to what extent they were met during the sessions. The group members were given the opportunity to think about the experiences they had in the group, about the feelings and emotions they had during the activities carried out during the psychodrama sessions and to what extent these experiences offered positive learning, changes of perspective, new beliefs and to what extent the activities carried out within the group helped them in the medical profession. The meeting ended with the completion of the questionnaires.
Statistical analysis
In order to determine the differences between the pre-test and post-test for the variables involved in the researsch, we used Wilcoxon non-parametric tests. Mann-Whitney tests were used to test the equivalence of the control and the experimental groups in the pretest phase.
Results
The analysis of the differences between pre- and post-intervention phases for the burnout syndrome
Mann-Whytney tests were used to determine if the two groups, control and experimental were equivalent before the intervention and to control the selection bias. The results showed that there no significant differences between the two groups, except for one variable, rumination, with higher values for the experimental group (Table 2). Because the intervention programme did not focuse specifically on copig strategies, we did not control for this difference in the comparison between the two groups in the post-test phase. However, future studies could examine more deeply the role of rumination on burnout.
To highlight the differences between pre- and post-intervention phases for the burnout syndrome, in each of the two groups studied (the experimental group and the control group), the Wilcoxon test for paired samples was used (Table 3).
The results showed that within the control group, in which no intervention was performed, the level of burnout experienced by the nurses participating in the study remained unchanged in all three specific dimensions and, implicitly, in the total burnout. However, in contrast to the control group, in the experimental group, which benefited from a specialized intervention by applying, in ten intervention sessions, the techniques specific to classical psychodrama, it was found that the level of burnout decreased for two dimensions: personal burnout and the burnout generated by work conditions. However, differences could not be detected either in relation to the burnout generated by the patients or to the total burnout.
The analysis of the differences between the pre- and post-intervention phases for depression
Regarding the depression symptomatology, the Wilcoxon test for paired samples revealed that in the experimental group the depression level was lower after the intervention programme was completed, while in the control group the results remained constant, with no statistically significant differences (Table 4).
Obviously, the structured exercises, the interaction between the group members, who, during the psychodrama therapy sessions, offered each other a great wealth of information, psychological support and visible patterns of behaviour, causing the change in disposition and the diminishing of the participants’ negative emotions contributed to these results.
The analysis of the differences between the pre- and post-intervention phases for coping strategies
Regarding the cognitive and emotional coping strategies used by the nurses in the two groups, the Wilcoxon test showed that for the experimental group there were no significant differences between pre- and post-intervention except for two out of the nine analysed dimensions: positive refocusing and catastrophizing, characterized by less relevant values (Table 5).
In addition to the changes obtained in the experimental group, the results showed that the intrevention allowed the nurses to perceive more clearly the value of the positive elements in their social and professional environment and to diminish the importance of the elements that sometimes seem to have catastrophically influence on their existence. In order to achieve significant changes in coping strategies, taking into account the mean age of participants (some mechanisms are more difficult to change with age), a significantly larger number of sessions would probably be necessary.
The analysis of the differences between the pre- and post-intervention phases for anxiety
The results highlighted some changes that occurred in the post-intervention phase only for four of the eight analysed dimensions of the anxiety: self-awareness, ergic tension, veiled anxiety and general anxiety (Table 6).
A possible explanation could be supported by the fact that some activities within the psychodrama sessions were aimed at increasing self-awareness. Awareness of feelings, thoughts, vulnerabilities, limits, things that motivate us determines a more objective perception of one’s own personality, an increase of the emotional intelligence and empathy, so much needed aspects, in the professional environment, too. The low score on the dimension of ergic tension, which refers to the degree to which anxiety is caused by unmet pressures, needs, or impulses, may suggest that in addition to spontaneity, intuition and creativity in choosing activities, the environment of the sessions also plays an important role. In the study, this environment was designed and prepared to be secure, containable and facilitating for meeting the other members in an empathetic and supportive way, as proved by the results obtained.
The analysis of the usefulness of the psychodrama techniques as seen by the members of the experimental group
The analysis regarding the usefulness of the psychotherapeutic sessions through the methods of classical psychodrama included an evaluation based on an original questionnaire designed by the authors of this study. Thus, an increased proportion, represented by 10 out of the total of the 11 subjects of the experimental group, considered that, to a great and to a very great extent, the techniques used in the psychodrama sessions contributed significantly to their self-knowledge and personal development, that the activity in the psychodrama group met their needs and expectations mentioned prior to the start of this activity and that the objectives they set for joining the group were met. In an equally important proportion, 9 of the 11 subjects considered that “to a great and to a very great extent” the group contributed to the identification of alternative ways of solving personal dilemmas or internal conflict. Maximum adherence (11 out of 11 subjects) was obtained by the perception that the group intervention through the classical psychodrama method would be beneficial to nurses with burnout (Table 7). The results obtained from the analysis of the questionnaire are also supported by those obtained from the content analysis of the 10 psychodrama sessions and the feedback received directly at the end of each activity.
Discussion
Our study showed that the psychodynamic psychotherapy is an efficient method to reduce burnout in healthcare professionals, improving not only the levels of work burnout but also the personal burnout. Our results are in line with previous research showing that interventions including mindfulness techniques, stress management techniques or cognitive behavioural techniques could lead to better communication skills and more efficient coping strategies which, in turn, could predict lower levels of burnout [47]. More specifically, the combination of techniques used during the intervention is convergent with the findings revealed by a recent metanaalysis, showing that the holistic, person-directed intervention is efficient for the reduction of the healthcare profesionals’ burnout [48]. The results of our study also revealed that the intervention was efficient to reduce the general level of depression and anxiety, participants in the experimental group having lower levels of anxiety and depression. Our results are sustained by previous research showing that burnout and anxiety could be associated and that individuals who are more prone to experiencing higher levels of anxiety (trait anxiety) are more likely to develop burnout as well [49]. Some of the coping strategies also changed after the intervention, catastrophizing being less reported in the experimental group than in the control group. However, unexpectedly positive refocusing seems to be also less used in the experimental group.
This study is an argument for the usefulness and efficiency of psychotherapeutic interventions by using classic psychodrama for nurses with burnout. There are not many studies using psychodrama for the reduction of burnout among nurses, which makes it dificult to compare our results with those reported in other studies. However, a few recent studies showed that psychodrama could lead to the improvement of adaptive mechanisms in the workplace and to lower levels of fatigue and exhaustion [42] and to enhance nursing students’ communication skills, attitudes towards dying patients, and reflection [50].
Taking into account that recent studies highlighted that psychotherapeutic interventions in burnout also have economic benefits, it can be considered that psychodrama used in such situations leads to a real cost-effectiveness advantage. Regarding the financial benefits of initiatives which may reduce the incidence of depressive disorders, anxiety and burnout and promote work functioning [51], cost-benefit analysis demonstrated that preventive intervention in the work setting of the nurses and physicians might be cost-saving from a business point of view [52]. By reducing symptoms of mental health complaints, burnout interventions are, consequently, paramount to organizational productivity [53]. It was highlighted that burnout can effectively be reduced with moderate levels of investment, these findings suggesting substantial economic value for policy and organizational expenditures for burnout reduction programmes for the medical staff [54]. Organizational investment in strategies aimed at reducing burnout among nurses is needed, and if successful, likely to have a positive return on investment and benefit nursing-sensitive quality of care indicators [11]. For this reason, standardized multi-dimensional cohort studies in search of potential cost-effective work-place intervention targeted to maintain a sustainable workforce must be conducted in the early future [55]. Despite the benefits which occur from a cost-benefit analysis of any phenomenon, we did not approach this criterion concerning the burnout syndrome, considering that it is a subject (aspect) that is worth a much more applied further study.
The criteria used in our study to assess the burnout related evolution of the nurses individually, but also of the group as a whole, were part of both a quantitative analysis (represented by questionnaires) and a qualitative analysis. Within the latter, there were analysed and observed: (a) the nurses’ level of participation and involvement, (b) the group cohesion, (c) the atmosphere in the group, from the beginning to the end of the sessions, (d) the group members’ reaction to the techniques used, (e) the manifestation of initiatives and (f) the availability to provide emotional support for the nurses in the group.
The difference between the high degree of adherence found in this group and the nurses’ initial lack of interest in participating in such specialized interventions is a real paradox. This fact can be explained by the lack of education and confidence regarding this kind of psychological interventions, by the lack of the precedent regarding the knowledge of the results of such interventions or by the existence of the induced fear that the need for a psychologist can be interpreted negatively.
In choosing the techniques used, each of the group members’ needs were taken into account, needs that were specified during the first meeting and which were observed during the meetings, as well as the needs of the group as a dynamic system and also a thematic group. The group activities aimed at increasing the cohesion between the participants, stimulating spontaneity (to reduce anxiety) and interconnection, developing communication skills, empathy necessary for the subjects in the medical profession. Also, the group members participated in activities where they learned relaxation techniques, adaptive coping strategies in order to cope with various stress-generating situations, including in the workplace. Through the use of psychodrama techniques in various activities, the aim was to break certain dysfunctional patterns of thinking and behaviour noticed in the group members, to explore the experiences and to highlight the central feeling in certain situations and, of course, to identify adaptive ways of reaction. It was noticed that with the techniques used, the participants showed openness, involvement in role-playing games and, especially, in activities of offering emotional support.
The intense activity during the therapy sessions generated a relatively high and rapid level of self-disclosure and a strong emotional involvement, often with intense emotional discharges. At the end of the psychodrama sessions, the participants most often confessed that they were experiencing relaxation, contentment and the desire to return. The emotional catharsis, not infrequently encountered in the group as a result of the activities carried out and which usually occurs as a result of repressed and blocked negative emotions for a longer period of time, represented for the group members a “release”, a “discharge” with curative effect. The apparent state of tension, of agitation, followed by the free expression of feelings can offer the chance to enter a path of balance, recognition, acceptance and finally integration.
As the studies on the burnout syndrome highlighted the fact that the support group was extremely important in its prevention [56,57,58], the activities were also chosen in this regard, using the techniques and methods specific to psychodrama. During the activities, some group members showed a strong need for appreciation, valorization and security that they would receive interpersonal support in various situations in the professional or family environment. In this paradigm, the staging of the “social atom” was aimed at giving each group member access to another lifestyle, another way of thinking and perceiving certain things or another way of reporting to the world and the environment.
Each member’s behaviour and interactions in the group could provide data on their social patterns and the way they interact with others thus recreating within the group the same interpersonal universe in which they actually live [39]. This activity highlighted the existence of love, of joy, but also of tense, dysfunctional, conflictual relationships that needed to be worked on in some group members’ families. An imbalance in the family life, of course, attracts frustration and dissatisfaction, eventually affecting the professional activity.
It is known that each person has an emotional or psychological vulnerability, most often caused by the adoption of inappropriate beliefs or attitudes arising from experiences or interactions with others and as effects of these interactions. These emotional vulnerabilities, in the presence of certain psychosocial factors (family or workplace conflicts, overwork, time pressure, etc.), can lead to burnout. Starting from this argument, we chose to approach this topic in the psychodrama group.
The “professional atom” activity highlighted once again the fact that there were strained relationships between colleagues in the workplace and, moreover, a lack of support of the team from the chief nurse. From the statements of the nurses present in the psychodrama group, it was found that the patients’ dissatisfaction was mainly generated by the accommodation conditions of the public hospital and the long waiting time for consultations. This exercise also highlighted the fact that the feelings of dissatisfaction, frustration or nervousness in the workplace of the nurses participating in the psychodrama group were mostly generated by the problems in the medical system, represented mainly by the continuous lack of personnel, by the high level of work load and the lack of certain materials and medicines, all of which could generate medical errors and dissatisfaction among patients.
Other determinants of stress and dissatisfaction were the relationships with the patients’ relatives and with certain categories of patients who, either were “suspicious of the manoeuvres performed”, or behaved “aggressively and disrespectfully towards the nurse”. Specifically, it was noted that even within the medical team, the relationships were not very harmonious, meaning that often the doctors “scold the nurse unfairly and in the presence of the patient” or “they do not adopt any attitude and involvement in alleviating the situation when the dissatisfied patient is unfairly accusing the nurse”.
The exercise also highlighted the fact that there were situations when the relations between the nurses who graduated from higher education and those who graduated from post-secondary schools were tense, too. This fact is also determined by the fact that, in Romania, although the first nurses with higher education entered the labour market in 2009, in hospitals there is still no job description adapted so as to consecrate the difference between the two categories of nurses, not only from a salary point of view, as they exist today, but also from the point of view of their responsibilities and duties.
As evidenced in this group, most of the problems identified have causes related to the organization or to a defective medical system as a whole. However, in the context in which all nurses work in the same system, with the same dysfunctions, one may ask the question why, still, some medical professionals develop burnout and others do not? As studies show [59, 60], the answer can be found in the fact that at the individual level there may be vulnerabilities, frustrations, maladaptive coping mechanisms, insufficient communication skills.
Because, unfortunately, an entire system cannot be changed quickly, especially if it depends on many factors, often independent of the nurse’s activity, many of the activities carried out within the group, focused on self-knowledge, on personal development, on the development of certain skills absolutely necessary for the nurse in the profession that they perform under the present conditions and on the awareness of the fact that if a real change was desired, the change had to come from within each individual.
All of these painful realities need to be managed properly, because in the long run, they can affect the nurses’ emotional health and the quality of care that nurses are supposed to provide.
Although the number of sessions was limited, these meetings were meant for the nurses to benefit not only from the identification or awareness of certain intrapsychic conflicts, but also to “feel” the benefits of this group, by learning some techniques that can be applied in everyday life after the completion of the psychodrama sessions. For this reason, nurses learned relaxation, breathing, imagery or mindfulness techniques. By becoming aware of their own thoughts, emotions and sensations and by learning some mechanisms of their effective management, the effect obtained was beneficial for both those directly involved in the therapeutic process and those around them.
Being a themed group, with a limited duration, only certain facets of the participants’ personality structure could be reached. However, this group provided extraordinary opportunities to raise awareness and address some difficulties or problems, to stimulate and challenge on the cognitive, behavioural and, especially, emotional level. Moreover, the nurses who joined this group met with their resources, fears, wishes, doubts, dreams in a warm, secure, supportive environment, without prejudice or criticism, thus succeeding to overcome existing anxiety and blockages.
The decrease in the level of personal burnout can be argued by the fact that the techniques and activities carried out within the therapy group led to a deeper awareness and efficient management of personal problems.
The lower levels of burnout caused by the work conditions measured after the intervention even if no objective changes were made at their work place could be explained by the fact that the nurses who participated in the group either were able to reinterpret differently the situations or they were influenced by the “Hawthorne effect” which explains the influence of the group on the individual. The Hawthorne effect refers to behavioural and attitudinal changes that occur when people are “under the spotlight” or when they are part of a group, demonstrating that the strongest motivation is not that of a financial nature, but an emotional one, represented by the feeling of involvement or the attention paid to them. This type of motivation gives the members of such groups an increase in their confidence so that they can cope with different situations and that they can more easily overcome the contextual factors. On the other hand, the control group did not receive any intervention, the psychodrama therapy being tested against no intervention at all instead of being tested against an intervention distinct from psychodrama, which is also a weakpoint and limits the informative value on the effect of PPPM.
Another limitation of this study involves the volunteer bias, given the fact that the assignment of the participants in the experimental group was not random, they volunteered to participate in the research project which represents a threat to the external validity of our study. However, given the length of the intervention and the necessity of the active involvement of the participants in the psychoterapuetical process, the voluntary opt-in consent was crucial in order to avoid experimental mortality.
The main limitation of the experimental study is the size of the sample taken in the study. This situation is due to the fact that, in order to be able to work effectively, the number of subjects participating in group therapy is usually limited to 8–10 members [39].
Future research directions
As future directions of research, it is desired to carry out a comparative analysis for other categories of medical professionals regarding the level of occurrence of the burnout syndrome. In order to identify to a greater extent the changes induced to the subjects by participation in such activities, it is desired to use within the group therapy other evaluation tools, too and also to carry out an evaluation within 3 months of completion of the intervention, to observe to which extent the acquisitions obtained by the group members are maintained after participating in the group therapy through the classical psychodrama method. Another future research direction would be to test the psychodrama therapy against other types of interventions, in order to determine its efficienty.
Conclusions
By combining individual and organizational interventions, positive results can be obtained in reducing the burnout scores. Therefore, the actions that include changes in the environmental factors within the workplace along with stress management programmes and the multidisciplinary approach under the PPPM concept can be promising solutions for managing burnout.
The innovative study highlighted the fact that the activities carried out within the group by using specific techniques, in conjunction with the influence of the group itself on the participants, generated changes in attitudes and perceptions, showing that the motivation of emotional nature, the attention paid or the feeling of involvement made the group’s subjects overcome more easily the contextual factors and lower levels in the burnout generated by the work and the personal burnout were registered. The nurses’ participation in the therapy group led to a decrease in negative emotions, changes in the depressive mood and a decrease in anxiety level.
The activities carried out in the group showed a lack of knowledge of the burnout phenomenon in the sections where the nurses worked. In order to prevent the onset of the burnout syndrome, firstly, it is necessary to inform and organize courses on this topic in hospitals. Nurses receiving information about the burnout syndrome, the structured exercises and the “group” in its dynamics provided extraordinary opportunities of raising awareness, addressing the various difficulties faced by participants and of cognitive, behavioural and, especially, emotional stimulation. In addition to optimizing professional relationships, nurses learned relaxation and meditation strategies, developing their social, communication and self-analysis skills.
The positive messages and feedback formulated by the nurses present in the group, as well as the concrete results obtained, showed that the group therapy using the classical psychodrama method can be an effective solution in the prophylaxis or treatment of the burnout syndrome.
References
Montero-Marín J, Araya R. Understanding burnout according to individual differences: ongoing explanatory power evaluation of two models for measuring burnout types. BMC Public Health. 2012;12:922. https://doi.org/10.1186/1471-2458-12-922.
Karodia T. Psychometric properties of the burnout inventory. University of Pretoria. 2007, pp.2–25. https://repository.up.ac.za/bitstream/handle/2263/30563/dissertation.pdf?sequence=1. Accessed 15 Jan 2020.
Jonsdottir IH, Sjörs DA. Mechanisms in endocrinology: endocrine and immunological aspects of burnout: a narrative review. Eur J Endocrinol. 2019;180(3):R147–58. https://doi.org/10.1530/EJE-18-0741.
Grigorescu S, Cazan A, Grigorescu D, Rogozea L. The role of the personality traits and work characteristics in the prediction of the burnout syndrome among nurses—a new approach within predictive, preventive, and personalized medicine concept. EPMA J. 2018;9:355–65. https://doi.org/10.1007/s13167-018-0151-9.
Bianchi R, Schonfeld I, Laurent E. Is it time to consider the “burnout syndrome” a distinct illness? Front Public Health. 2015;3:158. https://doi.org/10.3389/fpubh.2015.00158.
World Health Organization 2019 https://www.who.int/mental_health/evidence/burn-out/en/. Accessed 6 Feb 2020.
Shackleton N, Bonell C, Jamal F, Allen E, Mathiot A, Elbourne D, et al. Teacher burnout and contextual and compositional elements of school environment. J Sch Health. 2019;89(12):977–93. https://doi.org/10.1111/josh.12839.
McLean D, Eklund K, Kilgus SP, Burns MK. Influence of teacher burnout and self-efficacy on teacher-related variance in social-emotional and behavioral screening scores. Sch Psychol. 34(5):503–11. https://doi.org/10.1037/spq0000304.
Parrello S, Ambrosetti A, Iorio I, Castelli L. School burnout, relational, and organizational factors. Front Psychol. 2019;10:1695. https://doi.org/10.3389/fpsyg.2019.01695.
Molero Jurado M, Pérez-Fuentes M, Gázquez Linares JJ, Márquez M, Martínez AM. Burnout risk and protection factors in certified nursing aides. Int J Environ Res Public Health. 2018;15(6):1116. https://doi.org/10.3390/ijerph15061116.
Dyrbye LN, Shanafelt TD, Sinsky C, Cipriano PF, Ommaya JA, Colin P, et al. Burnout among health care professionals: a call to explore and address this underrecognized threat to safe, high-quality care. Natl Acad Med. 2017. https://doi.org/10.31478/201707b.
Dyrbye LN, Shanafelt TD, Johnson P, Johnson A, Satele D, West C. A cross-sectional study exploring the relationship between burnout, absenteeism, and job performance among American nurses. BMC Nurs. 2019;18:57. https://doi.org/10.1186/s12912-019-0382-7.
Aronsson G, Theorell T, Grape T, Hammarström A, Hogstedt C, Marteinsdottir I, et al. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health. 2017;17:264. https://doi.org/10.1186/s12889-017-4153-7.
Grigorescu S, Grigorescu D, Rogozea L. Psihosocial factors generators of burnout in the public health system. J Med Brasov. 2016:4–10 ISSN1841–0782. http://webbut.unitbv.ro/jmb/JMB%202016%20nr%201/01_02_referat_burnout.pdf. Accessed 4 Feb 2020.
Vidotti V, Ribeiro RP, Galdino MJQ, Martins JT. Burnout syndrome and shift work among the nursing staff. Rev Lat Am Enfermagem. 2018;26:e3022. https://doi.org/10.1590/1518-8345.2550.3022.
Sánchez-Cruz J, Mugártegui-Sánchez S. Burnout syndrome among family physicians. Rev Med Inst Mex Seguro Soc. 2013;51(4):428–31.
Pradas-Hernández L, Ariza T, Gómez-Urquiza JL, Albendín-García L, De la Fuente EI, Cañadas-De la Fuente GA. Prevalence of burnout in paediatric nurses: a systematic review and meta-analysis. PLoS One. 2018;13(4):e0195039. https://doi.org/10.1371/journal.pone.0195039.
Zubairi AJ, Noordin SH. Factors associated with burnout amongresidents in a developing country. Ann Med Surg. 2016;6:60–3. https://doi.org/10.1016/j.amsu.2016.01.090.
López-López IM, Gómez-Urquiza JL, Cañadas GR, De la Fuente EI, Albendín-García L, Cañadas-De la Fuente GA. Prevalence of burnout in mental health nurses and related factors: a systematic review and meta-analysis. Int J Ment Health Nurs. 2019;28(5):1032–41. https://doi.org/10.1111/inm.12606.
Chen S, Lin S, Ruan Q, Li H, Wu S. Workplace violence and its effect on burnout and turnover attempt among Chinese medical staff. Arch Environ Occup Health. 2016;71(6):330–7. https://doi.org/10.1080/19338244.2015.1128874.
Molina-Praena J, Ramirez-Baena L, Gómez-Urquiza JL, Cañadas GR, De la Fuente EI, Cañadas-De la Fuente GA. Levels of burnout and risk factors in medical area nurses: a meta-analytic study. Int J Environ Res Public Health. 2018;15(12):2800. https://doi.org/10.3390/ijerph15122800.
Stehman CR, Zachary T, Gershaw R, Kellogg R. Burnout, drop out, suicide: physician loss in emergency medicine, part I. West J Emerg Med. 2019;20(3):485–94. https://doi.org/10.5811/westjem.2019.4.40970.
Patel RS, Bachu R, Adikey A, Malik M, Shah M. Factors related to physician burnout and its consequences: a review. Behav Sci (Basel). 2018;8(11):98. https://doi.org/10.3390/bs8110098.
West CP, Dyrbye LN, Shanafelt TD. (Mayo Clinic, Rochester, MN; and Stanford University Medical Center, Stanford, CA, USA). Physician burnout: contributors, consequences and solutions (Review). J Intern Med 2018; 283:516–529. https://doi.org/10.1111/joim.12752.
Medeiros de Oliveira S, Alcantara Sousa L, Gadelha M, Nascimento VB. Prevention actions of burnout syndrome in nurses: an integrating literature review. Clin Pract Epidemiol Ment Health. 2019;15:64–73. https://doi.org/10.2174/1745017901915010064.
Alan H. Rosenstein. Hospital administration response to physician stress and burnout. Hospital Practice. 2019;47(5):217–20. https://doi.org/10.1080/21548331.2019.1688596.
Ashraf F, Ahmad H, Shakeel M, Aftab S, Masood A. Mental health problems and psychological burnout in Medical Health Practitioners: a study of associations and triadic comorbidity. Pak J Med Sci. 2019;35(6):1558–64. https://doi.org/10.12669/pjms.35.6.444.
Ovchinnikov YV, Palchenkova MV, Kalachev OV. Burnout syndrome: diagnosis, principles of treatment, prophylaxis. Voen Med Zh. 2015;336(7):17–24.
McCormack H, MacIntyre T, O'Shea D, Herring MP, Campbell MJ. The prevalence and cause(s) of burnout among applied psychologists: a systematic review. Front Psychol. 2018;9:1897. https://doi.org/10.3389/fpsyg.2018.01897.
Panagioti M, Geraghty K, Johnson J, Zhou A, Panagopoulou E, Chew-Graham C, et al. Association between physician burnout and patient safety, professionalism, and patient satisfaction: a systematic review and meta-analysis. JAMA Intern Med. 2018;178(10):1317–30. https://doi.org/10.1001/jamainternmed.2018.3713.
De Vente M, Olff M, Van Amsterdam JG, Kamphuis JH, Emmelkamp PM. Physiological differences between burnout patients and healthy controls: blood pressure, heart rate, and cortisol responses. Occup Environ Med. 2003;60:54–61. https://doi.org/10.1136/oem.60.suppl_1.i54.
Onen Sertoz O, Tolga Binbay I, Koylu E, Noyan A, Yildirim E, Elbi MH. The role of BDNF and HPA axis in the neurobiology of burnout syndrome. Prog Neuropsychopharmacol Biol Psychiatry. 2008;32(6):1459–65. https://doi.org/10.1016/j.pnpbp.2008.05.001.
Gulen B, Serinken M, Eken C, Karcıoglu Ö, Kucukdagli OT, Kilic E, et al. Serum S100B as a surrogate biomarker in the diagnoses of burnout and depression in emergency medicine residents. Acad Emerg Med. 2016;23(7):786–9. https://doi.org/10.1111/acem.12973.
Golubnitschaja O, Costigliola V. Promoting predictive, preventive and personalised medicine in global scale: the EPMA World Congress 2011. EPMA J. 2011;2(Suppl 1):1–3. https://doi.org/10.1007/s13167-011-0106-x.
Golubnitschaja O, Costigliola V. EPMA summit 2014 under the auspices of the presidency of Italy in the EU: professional statement. EPMA J. 2015;6:4. https://doi.org/10.1186/s13167-015-0026-2.
Golubnitschaja O, Baban B, Boniolo G, et al. Medicine in the early twenty-first century: paradigm and anticipation - EPMA position paper 2016. EPMA J. 2016;7:23. https://doi.org/10.1186/s13167-016-0072-4.
Golubnitschaja O, Costigliola V, Grech G. EPMA world congress: traditional forum in predictive, preventive and personalised medicine for multi-professional consideration and consolidation. EPMA J. 2017;8(Suppl 1):S1–S54. https://doi.org/10.1007/s13167-017-0108.
Golubnitschaja O, Costigliola V. General report & recommendations in predictive, preventive and personalised medicine 2012: white paper of the European Association for Predictive, Preventive and Personalised Medicine. EPMA J. 2012;3(1):14. https://doi.org/10.1186/1878-5085-3-14.
Yalom I, Leszcz M. Tratat de psihoterapie de grup. Editura Trei, Romania, București; 2008, ISBN 978-973-707-213-9.
Sexton JB, Adair KC, Leonard MW, et al. Providing feedback following leadership WalkRounds is associated with better patient safety culture, higher employee engagement and lower burnout. BMJ Qual Saf. 2018;27(4):261–70. https://doi.org/10.1136/bmjqs-2016-006399.
Oflaz F, Meriç M, Yuksel Ç, Ozcan CT. Psychodrama: an innovative way of improving self-awareness of nurses. J Psychiatr Ment Health Nurs. 2011;18(7):569–75. https://doi.org/10.1111/j.1365-2850.2011.01704.x.
Özbaş AA, Tel H. The effect of a psychological empowerment program based on psychodrama on empowerment perception and burnout levels in oncologynurses: psychological empowerment in oncology nurses. Palliat Support Care. 2015;14(4):393–401. https://doi.org/10.1017/S1478951515001121.
Grigorescu S, Cazan AM, Grigorescu D, Rogozea L. Assessing professional burnout among hospital nurses using the Copenhagen Burnout Inventory. Acta Medica Transilvanica. 2018;4 ISSN 2285–7079. http://www.amtsibiu.ro/Arhiva/2018/Nr4-en/Grigorescu.pdf.
Minulescu M. Psihodiagnoza modernă -Chestionarele de personalitate. Editura Fundației România de Mâine, București; 2004, pp 122–131. ISBN 973-582-802-2.
Vrasti R. Măsurarea sănătății mentale- Scalele de evaluare a depresiei. 2008 http://www.vrasti.org/evaluarea%20depresiei.pdf. Accessed 20 Feb 2020.
Garnefski N, Kraaij V, Spinhoven P. Manualul de utilizare a chestionarului de coping cognitiv și emoțional. Editura ASCR. 2002. ISBN 978-606-8244-0307.
Patel RS, Sekhri S, Bhimanadham NN, Imran S, Hossain S. A review on strategies to manage physician burnout. Cureus. 2019;11(6):e4805. https://doi.org/10.7759/cureus.4805.
Wiederhold BK, Cipresso P, Pizzioli D, Wiederhold M, Riva G. Intervention for physician burnout: a systematic review. Open Med (Wars). 2018;13:253–63. https://doi.org/10.1515/med-2018-0039.
Koutsimani P, Montgomery A, Georganta K. The relationship between burnout, depression, and anxiety: a systematic review and meta-analysis. Front Psychol. 2019;10:284. https://doi.org/10.3389/fpsyg.2019.00284.
Beauvais AM, Özbaş AA, Wheeler K. End-of-life psychodrama: Influencing nursing students’ communication skills, attitudes, emotional intelligence and self-reflection. J Psy Nurs. 2019;10(2):103–10. https://doi.org/10.14744/phd.2019.96636.
Noben C, Smit F, Nieuwenhuijsen K, Ketelaar S, Gärtner F, Boon B, et al. Comparative cost-effectiveness of two interventions to promote work functioning by targeting mental health complaints among nurses: pragmatic cluster randomised trial. Int J Nurs Stud. 2014;51(10):1321–31. https://doi.org/10.1016/j.ijnurstu.2014.01.017.
Noben C, Evers S, Nieuwenhuijsen K, Ketelaar S, Gärtner F, Sluiter J, et al. Protecting and promoting mental health of nurses in the hospital setting: is it cost-effective from an employer’s perspective? Int J Occup Med Environ Health. 2015;28(5):891–900. https://doi.org/10.13075/ijomeh.1896.00465.
Bretland RJ, Thorsteinsson EB. Reducing workplace burnout: the relative benefits of cardiovascular and resistance exercise. PeerJ. 2015;3:e891. https://doi.org/10.7717/peerj.891.
Han S, Shanafelt TD, Sinsky CA, Awad KM, Dyrbye LN, Fiscus LC, et al. Estimating the attributable cost of physician burnout in the United States. Ann Intern Med. 2019;170(11):784–90. https://doi.org/10.7326/M18-1422.
Lui JNM, Andres EB, Johnston JM. Presenteeism exposures and outcomes amongst hospital doctors and nurses: a systematic review. BMC Health Serv Res. 2018;18(1):985. https://doi.org/10.1186/s12913-018-3789-z.
Fiorilli C, Benevene P, De Stasio S, Buonomo I, Romano L, Alessandro P, et al. Teachers’ burnout: the role of trait emotional intelligence and social support. Front Psychol. 2019;10 https://www.frontiersin.org/articles/10.3389/fpsyg.2019.02743/full. Accessed 25 Feb 2020.
Kim B, Jee S, Lee J, An S, Lee SM. Relationships between social support and student burnout: a meta-analytic approach. Stress Health. 2018;34:127–34. https://doi.org/10.1002/smi.2771.
Ben-Zur H, Michael K. Burnout, social support, and coping at work among social workers, psychologists, and nurses. Soc Work Health Care. 2007;45(4):63–8.
Arrogante Maroto Ó, Aparicio-Zaldívar EG. Tools to face burnout in nursing: social support, resilience and coping strategies. Rev Enferm. 2017;40(3):10–7.
Li L, Ai H, Gao L, Zhou H, Liu X, Zhang Z, et al. Moderating effects of coping on work stress and job performance for nurses in tertiary hospitals: a cross-sectional survey in China. BMC Health Serv Res. 2017;17:401. https://doi.org/10.1186/s12913-017-2348-3.
Acknowledgements
We acknowledge that the development of the research was authorized by the nurses who participated in this study and the research team would like to thank the management team of the Emergency County Hospital Brasov for their cooperation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest. All authors approve the content of the manuscript and have contributed significantly to the research and the writing of the manuscript.
Ethical approval
The research did not involve any risk for the participants. All ethical guidelines were followed as required for conducting human research. The procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional research, the study being approved to be run by the manager of the Emergency County Hospital Brasov, where the study was conducted and by the Committee for Ethical Research of Transylvania University of Brasov (Ethical approval number 06.2/2017). The research was also consistent with the ethical guidelines of The College of Psychologists in Romania. The research complies with the provisions of the Declaration of Helsinki (as revised in Brazil 2013). All the participants gave their informed consent for the research and their anonymity was preserved.
Authorship statement
The authors certify their contribution to this manuscript, as follows: study design (SG, LMR); data collection (SG, ODG) and analysis (SG, AMC); manuscript writing (SG, ODG, AMC).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Grigorescu, S., Cazan, AM., Rogozea, L. et al. Original targeted therapy for the management of the burnout syndrome in nurses: an innovative approach and a new opportunity in the context of predictive, preventive and personalized medicine. EPMA Journal 11, 161–176 (2020). https://doi.org/10.1007/s13167-020-00201-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13167-020-00201-6