
ABSTRACT
Mobile applications (apps) offer a novel way to engage children in behavior change, but little is known about content of commercially available apps for this population. We analyzed the content of apps for iPhone/iPad for pediatric weight loss, healthy eating (HE), and physical activity (PA). Fifty-seven apps were downloaded and tested by two independent raters. Apps were coded for: inclusion of the Expert Committee for Pediatric Obesity Prevention's (ECPOP) eight recommended strategies (e.g., set goals) and seven behavioral targets (e.g., do ≥1 h of PA per day), utilization of gaming elements, and general characteristics. Most apps lacked any expert recommendations (n = 35, 61.4 %). The mean number of recommendations among apps that used recommendations was 3.6 ± 2.7 out of 15, 56.1 % (n = 32) apps were classified as games, and mean price per app was $1.05 ± 1.66. Most apps reviewed lacked expert recommendations and could be strengthened by addition of comprehensive information about health behavior change and opportunities for goal setting.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
INTRODUCTION
Recent reports show that 16.9 % of children in the United States are obese and almost 30 % of children are overweight or obese by age 5 years [1, 2], putting them at greater risk for health complications and future weight gain [3, 4]. Among actions recommended by pediatric obesity experts are promotion of healthy eating (HE) and physical activity (PA) [5, 6] as well including the whole family in treatment [7]. Mobile applications (apps) are an engaging way to involve children in health behavior changes, capitalizing on portability and affordability of delivering health information via mobile devices and opportunity to use gaming to make health information entertaining [8, 9]. While most children do not own their own smartphone, parents are heavy app users, with 57 % of app-using parents reporting that they have downloaded apps for their children to use [10]. There is limited data available on mobile phone usage of children under the age of 12 years, but smartphone ownership among teens is growing (23 % of teens aged 12–17 years own a smartphone) [11]. Additionally, smartphones are becoming more widely available, as phone companies are beginning to offer smartphones for free phone upgrades [12–14]. Smartphones also offer an opportunity to extend health interventions to traditionally underserved groups, including Blacks and Latinos, as smartphone ownership of these groups is growing faster than that of Whites [15].
Many health promotion apps are currently available. Two previous studies examined the content of apps for adult weight loss [16] and for smoking cessation [17]. Both reviews found the apps to be lacking in the use of theory- or evidence-informed practices [16, 17]. To our knowledge, there have been no previous systematic analyses of the content of apps for pediatric weight loss, HE, and PA. A systematic content analysis of apps was conducted using recommendations of the 2007 Expert Committee for Pediatric Obesity Prevention (ECPOP) [5]. The ECPOP was made of representatives from 15 national health care organizations, including the American Medical Association and the Centers for Disease Prevention and Control; a steering committee appointed scientists and clinicians to three writing groups that subsequently reviewed existing literature and provided recommendations for prevention and treatment of pediatric obesity [5]. In 2007, the ECPOP published a set of recommendations for the prevention and treatment of pediatric obesity that build off the original ECPOP suggestions from 1995, incorporating evidence-based research as well as supplemental recommendations from clinical practice experiences where evidence-based research was unavailable [5].
The present analysis examines the content of mobile apps for the prevention and treatment of pediatric obesity (children/teens < 18 years) through weight loss, HE, and PA to determine if strategies and behavioral targets of the ECPOP are promoted [5]. Additionally, information on price, user ratings, and use of gaming principles were collected to obtain a rough assessment of acceptability of the apps to consumers as well as how engaging they might be to a child (e.g., more or less like a video game).
METHODS
A listing of apps available on the iTunes store was collected on June 12, 2012 using the Power Search function and selecting “any device” to find apps for iPhone/iPad. iTunes was selected as the platform for analysis, as it has significantly more apps than Android marketplace or other app repositories [18].
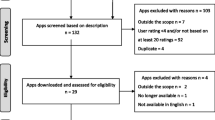
To find apps that were marketed for pediatric weight loss, the search terms “children,” “kids,” “teen,” “family,” and “weight loss” were used in the health/fitness and education categories. Initial searches yielded few results (n = 6); thus, the search terms were broadened to include two critical behaviors for weight loss: HE and PA. To ensure inclusion of any app pertaining to HE and PA for children, several search terms were used including: “children,” “kids,” “teen,” or “family” with addition of “exercise” or “physical activity” (to capture PA-related apps) and “diet” or “healthy eating” (to capture HE-related apps) (e.g., “family healthy eating”), yielding 158 apps. Supplemental searches were conducted in the Google search engine (www.google.com) to verify that iTunes searches yielded a comprehensive view of apps available. Google searches used the same search terms as above with addition of “iPhone apps” and yielded an additional seven apps, which appeared on the first page of the search result in a prominent area (i.e., they were not buried in a website and could be found easily by a parent searching for apps) (for a total of n = 171 apps).
Search terms were selected to mimic the type terms a parent might search for in iTunes, and they yielded apps that were not necessarily claiming to be health-related, although some of them did claim to help improve HE, etc. However, this mixture of the intended apps for an iTunes search and the additional information that comes along with it is a realistic picture of the experience of the average customer.
Of the 171 apps found, 110 were excluded from further analysis (not in English, content unrelated to weight loss/HE/PA, and not targeting children/teens), 61 apps were reviewed further, and descriptive information about each app was collected from its iTunes store page. Apps offering free and for-purchase versions were rated as separate apps (n = 9) in case two versions contained different information (as per the protocols of previous app analyses) [16, 17]. Apps that fit initial inclusion criteria (in English, focused on weight loss/HE/PA, and targeted children/teens) were downloaded from iTunes between June 18 and 28, 2012. Four additional apps were excluded at this point, as they were no longer available.
Apps were reviewed and coded by two independent raters (trained in health promotion) for inclusion of recommendations of the ECPOP (scored 1 for presence and 0 for absence of each recommendation) [5]. Recommendations include: eight intervention strategies (calculate and plot BMI over time, assess motivation to make changes, use motivational interviewing, tailor strategies to a specific case, set goals/limits, examine environmental influences, involve the whole family, and combine multiple behavior changes) and seven behavioral targets (reduce sugar-sweetened beverages, consume greater than or equal to nine servings of fruits and vegetables per day, decrease TV time, eat breakfast every day, cook at home, eat together at the table, and do greater than or equal to 1 h/day of PA) [5]. Overall summary scores were calculated for each app (out of 15) as well as for HE criteria only for HE-specific apps (out of 13) and PA criteria only for PA-related apps (out of 10). The raters met to discuss the scoring criteria, rated five apps, discussed initial coding and then coded all apps; initial inter-rater agreement was 94.9 %. After comparing initial coding of the apps, raters met to resolve discrepancies; final ratings were reached by consensus.
General information about the apps was collected from the content of each app and its iTunes description page, including: target behavior, price, age appropriateness rating (assigned by iTunes based on the age appropriateness of the content: “4+,” “9+,” “12+,” or “17+”) [19], target age range (if indicated by app developers), and compatible devices. User satisfaction was assessed through the apps' user ratings on iTunes (not available for all apps) and is reported for the app overall and for the current version along with the number of users that have rated the app. Ratings are on a five-point scale, from 1 star (worst) to 5 stars (best); average ratings are reported in whole and half stars. Connection to social media was assessed through the iTunes description page and content of the app. Apps were rated as connecting users to social media if they facilitated a connection to a third-party social media outlet (e.g., Facebook) or connected users to a social network for building community around the app itself (e.g., an online community for users).
Apps were classified as games if they adhered to the four criteria defined by game design expert, McGonigal, including having a goal, rules, and feedback that the user voluntarily accepts [20]. These criteria have also been adopted by the journal, Games for Health, due to their ability to distinguish between activities that merely simulate health and those that provide rules and other game-like aspects [21].
RESULTS
A summary of the results of the content analysis is presented in Table 1. Of the 57 apps reviewed, 61.4 % (n = 35) did not utilize any of the recommended strategies or behavioral targets. The most recommendations used by a single app was six, by HyperAnt [22]; apps that focused on both HE and PA included the most recommendations (3.1 ± 2.0). The most frequently used recommendations were: setting goals/limits (n = 16), reducing sugar-sweetened beverages (n = 9), and increasing fruit and vegetable consumption (n = 8). However, no apps promoted the following recommendations: assess motivation to make changes, use motivation interviewing, focus beyond the individual, decrease TV time, and eat breakfast every day. Table 2 shows a summary of the number of apps that utilized each expert recommendation.
Descriptive characteristics of the 57 apps are presented in Table 3. Of the apps reviewed, 52.6 % (n = 30) targeted HE, 35.1 % (n = 20) targeted PA, and 12.3 % (n = 7) targeted both HE and PA; apps that targeted weight tracking were coded as “both” (since weight is influenced by both HE and PA). The mean price per app was $1.05 ± 1.66 (n = 29 were free); all 57 were given a “4+” age appropriateness rating by iTunes, indicating that they “contain no objectionable material” [19]. A few apps (n = 15) reported the developer's suggested user age for the app, which ranged from 1 to 19 years old. Most apps were compatible with iPhone and iPad (n = 50); five apps were only compatible with iPad. Average user ratings from iTunes were reported for 27 apps, mean user rating for the current version was 3.9 ± 0.8 out of 5, (based on an average of 38.8 ± 52.0 user ratings), and app price and user ratings were not statistically significantly related to number of expert recommendations used by the app (p = 0.64 and p = 0.42, respectively). Only 15.8 % (n = 9) of the apps connected users with social media, and most of these simply provided a link to the app's own Facebook page for users to “like” the page. Applying McGonigal's definition of a game [20], 56.1 % (n = 32) of the apps were classified as games. Table 4 (supplemental information) lists all of the apps by name, along with a summary of the number of expert recommendations they used, and descriptive information about the content of the apps.
DISCUSSION
Overall, few of the apps reviewed used expert-recommended strategies and behavioral targets in their approach to assist with the promotion of pediatric weight loss, HE, and PA. Consistent with adult literature on weight loss [16] and for smoking cessation [17], the average number of expert recommendations used in the apps was low (overall mean = 1.1 ± 1.6). Given the wide range of recommendations coded, it was surprising that the majority of apps (n = 35, 61.4 %) did not employ any of the 15 strategies or behavioral targets [5].
From this review, it is apparent that mobile apps are very capable of promoting some of the expert recommendations for HE and PA, including setting goals/limits and reducing sugar-sweetened beverage consumption. However, other recommendations were completely absent, likely because they are not areas of behavior change that app developers have thought of targeting. For example, motivational interviewing techniques were not used by any of the apps, though pilot work from weight loss interventions in women have shown that motivational interviewing can be successfully implemented through website interaction [23]. Few apps (n = 6) utilized the strategy of combining multiple behavior changes by targeting HE and PA, despite the fact that apps that provide more services to customers are likely more valuable to them and an app that targets multiple behavior changes takes the burden off the consumer to find supplemental apps. Ideally, apps would promote multiple recommendations, including a combination of strategies and behavioral targets.
Additionally, most of the apps that were advertised as promoting PA did not require the user to do the recommended action (e.g., jump). The user could simply shake her hand to move the game along instead of moving her body as the game advertised. Two apps (Cool Skipping and Cool Skipping Lite [24]) actually instructed the user about how she could use her hand to move the phone instead of jumping. There were a just four PA apps that required the user to actually move location by utilizing the global positioning system (GPS) location of the phone (and thus could not be “tricked” by moving the phone in one's hand).
The app market for weight loss, HE, and PA apps can be confusing for consumers because of the limited information on the iTunes description pages about the content of the apps. In our initial searches for weight loss apps for children, we found very few results (n = 6), suggesting that parents looking for tools to help their children might have difficulty.
Another issue with the use of technology to assist in health behavior change, such as pediatric obesity prevention and treatment, is that most young children (e.g., ages 4–7 years) do not have their own mobile devices. This means that it is important to target parents both for searching for health promotion apps as well as incorporating parents in the activities of the apps themselves. Apps that can involve parents, either through allowing parents to support achievements by the child in HE and PA or by having the parent participate with the child, is important.
A few apps stood by receiving high scores for inclusion of expert recommendations; HyperAnt (free) used the most expert recommendations of any app—three intervention strategies and three behavioral targets [22]. The app is a set of “Hyper Activity Cards” that gives kids ideas for health and fitness activities in a range of areas including HE, PA, and sleep [22]. The app received a high score because it covers multiple domains, involves parents, and includes information about HE and PA targets (eliminating sugar-sweetened beverages, eating lots of fruits and vegetables, and engaging in at least 1 h of PA) [22]. While the app provided a lot of information (and more than most of the apps), it was a very engaging app. HyperAnt does not require any feedback from the user, it just pushes out information, which eliminates user interaction with the app, including taking away the opportunity for the user to set goals and self-monitor their behaviors. Additionally, it does not meet the criteria of being a game and connect users to social media.
The next highest score for an app was 5 (Ideserve2), but this app was no longer available in the US when the analysis was completed. A few apps received scores of 4, including Smash Your Food HD ($2.99)/Smash Your Food Free (free). This app focuses on the high fat/sugar/salt content of popular processed foods [25] and received an Honorable Mention in First Lady Michelle Obama's “Apps for Healthy Kids” national competition, which encouraged innovative and informative apps for kids and their parents [26, 27]. Smash Your Food tells kids what their recommended daily serving sizes are for fat/sugar/salt and then asks them to guess the content of popular foods. After the child guesses, the app shows the food being smashed and reveals the true fat/sugar/salt content of the food alongside the child's guess and her daily recommended intake. Smash Your Food also offers an email service to involve parents in the learning process and update them on their child's progress in the game [28]. While entertaining, Smash Your Food could be improved by including nutrition tips along with the game, for example, a message about increasing fruit and vegetable consumption or eating meals at home could be incorporated into the screens associated with an unhealthy fast food item.
The lack of health content and concrete recommendations in the apps reviewed, including apps with high scores (e.g., HyperAnt and Smash Your Food), highlights the need for collaboration between a diverse group of experts in order to produce better apps. While we did not test efficacy of the apps reviewed in the present analysis, to determine if they might catalyze behavior change, it is unlikely that they would produce much change, given the lack of substantive content we saw. There is a need for widespread efficacy test of mobile apps that are designed to support behavior change and support health improvement. This could take shape in the development of the apps, including more interdisciplinary work between health behavior researchers with mobile app developers, as well as health promotion practitioners and evaluators to design research programs that empirically test apps.
Limitations of the present analysis include the focus on apps for iPhone and iPad. Restricting the analysis to one operating system offered a comprehensive snapshot of what is available to consumers, although future studies could look at an exhaustive survey of the mobile app market (including apps for the Android and Windows platforms). However, iTunes has significantly more apps than Android marketplace or other app repositories [18] and was, therefore, chosen as a starting sample for the present analysis. Another limitation of the present analysis was the use of user ratings of the apps, as there were so few apps with information available (n = 27) and it is impossible to know what aspects of the app the ratings were based on (likely varies between individuals). Further, due to the rapidly evolving landscape of mobile technologies, the apps available to consumers can change quickly. In the time between when apps targeting HE and PA in children were identified and when they were downloaded (<1 month), four apps were no longer available and had to be excluded from further analysis. Despite these limitations, the present analysis has many strengths. First, researchers downloaded, tested, and reviewed all apps analyzed. Second, content analysis was based on expert recommendations, and apps were coded by two independent raters. Finally, to our knowledge, this is the first analysis of apps for pediatric weight loss, HE, and PA.
Overall, the present analysis provides a comprehensive picture of the mobile apps available for iPhone/iPad that are found using a search for pediatric obesity through weight loss, HE, and PA (e.g., the kind of search a parent might conduct on the iTunes store). Most apps were void of expert-recommended strategies; this disconnect between the evidence-based suggestions and what is promoted in apps and other health products may be adding to the confusion of consumers as to what they should be doing to help their families get healthier. The apps tested present a huge lost opportunity for the provision of solid, evidence-based strategies and recommendations for health change, with a group of people demonstrating interest and initiative to make changes (by downloading the apps). Additionally, despite research showing that parents are a crucial part of pediatric obesity prevention and treatment (including the promotion of HE [29] and PA [30]), most apps did not target parents/families, instead focusing solely on the individual child. Future efforts for the prevention and treatment of pediatric obesity must look beyond the individual and attempt to change elements of the social and physical environments that can promote or inhibit behavior change. App developers and public health practitioners should work collaboratively to integrate evidence-based practices and expert recommendations in apps so that technologies marketed as health-promoting tools can promote substantive behavior changes.
References
Cl O et al. Prevalence of obesity and trends in body mass index among us children and adolescents, 1999–2010. JAMA: The Journal of the American Medical Association. 2012;307(5):483-490.
2010 Pediatric Nutrition Surveillance, Summary of Growth Indicators by Age (Children Aged <5 Years), Centers for Disease Control and Prevention's Pediatric and Pregnancy Nutrition Surveillance System, Editor 2010: Atlanta.
Freedman DS. et al. Cardiovascular risk factors and excess adiposity among overweight children and adolescents: The Bogalusa Heart Study. J Pediatr. 2007;150(1):12-17 e2.
Singh AS. et al. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes Rev. 2008;9(5):474-88.
Barlow SE. The Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics. 2007;120(Supplement 4):S164-S192.
Whitlock, E.P., et al., Effectiveness of weight management interventions in children: A targeted systematic review for the USPSTF. Pediatrics. 2010.
Epstein LH. Wrotniak BH. Future directions for pediatric obesity treatment. Obesity (Silver Spring). 2010;18(Suppl 1):S8-12.
Boushey CJ. et al. Use of technology in children's dietary assessment. Eur J Clin Nutr. 2009;63(Suppl 1):S50-7.
The Health Educator's Social Media Toolkit, Office of the Associate Director for Communication, Editor 2011, Centers for Disease Control and Prevention: Atlanta.
Purcell K, Half of adult cell phone owners have apps on their phones in Pew Research Center's Internet & American Life Project. Washington, D.C.;2011.
Lenhart, A., Teens, smartphones & texting, in Pew Research Center's Internet & American Life Project. Washington, D.C.;2012.
Free phones, free cell phones, smartphones, & mobile devices from AT&T. 2012 [cited 2012 September 8]; Available from: https://www.att.com/shop/wireless/devices/freephones.html.
MetroPCS resuscitating $40 plan for 4G LTE smartphones. 2012 [cited 2012 September 8]; Available from: http://www.cnet.com/8301-17918_1-57370479-85/metropcs-resuscitating-$40-plan-for-4g-lte-smartphones/.
Smith, G. Smartphones bring hope, frustration as substitute for computers Huffington Post. 2012.
Smith A., Nearly half of American adults are smartphone owners in The Pew Research Center's Internet & American Life Project Washington, D.C;2012
Breton E, Fuemmeler B, Abroms L. Weight loss—There is an app for that! But does it adhere to evidence-informed practices? Translational Behavioral Med. 2011;1(4):523-529.
Abroms LC. et al. iPhone apps for smoking cessation: A content analysis. Am J Prev Med. 2011;40(3):279-85.
Lookout Mobile Security, App Genome Report—February 2011, 2011.
iTunes. Application ratings. 2012 [cited 2012 June 20]; Available from: http://itunes.apple.com/WebObjects/MZStore.woa/wa/appRatings.
McGonigal J. Reality is Broken: Why Games Make Us Better and How They Can Change the World Vol. 1. New York: New York Penguin Press; 2011.
Ferguson B. The emergence of games for health. Games for Health J. 2012;1(1):3.
Wireframe, L. Hyperant™ HyperActivity™ cards. 2012 [cited 2012 September 24]; Available from: http://itunes.apple.com/us/app/hyperant-hyperactivity-cards/id512140657?mt=8.
Webber KH, Tate DF, Quintiliani LM. Motivational interviewing in internet groups: A pilot study for weight loss. J Am Diet Assoc. 2008;108(6):1029-32.
Cool Skipping Lite. 2012 [cited 2012 July 17]; Available from: http://itunes.apple.com/app/id486603558.
Food N'Me. SmashYourFood. 2012 [cited 2012 September 8]; Available from: http://smashyourfood.foodnme.com/en/.
Apps for Healthy Kids. 2010 [cited 2012 September 8]; Available from: http://appsforhealthykids.com/.
Rules—Apps for healthy kids. 2010 [cited 2012 September 8]; Available from: http://appsforhealthykids.com/rules.
Food N'Me. For parents—SmashYourFood. 2012 [cited 2012 September 8]; Available from: http://smashyourfood.foodnme.com/en/for-parents/.
Patrick H, Nicklas TA. A review of family and social determinants of children's eating patterns and diet quality. J Am Coll Nutr. 2005;24(2):83-92.
Wilson DK. et al. Neighborhood and parental supports for physical activity in minority adolescents. Am J Prev Med. 2011;41(4):399-406.
Acknowledgments
No funding was received for this research.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Implications
Practice: Mobile applications based on expert-recommended strategies and behavioral targets could be powerful tools in the prevention and treatment of pediatric obesity through weight loss, healthy eating, and physical activity, but they must undergo proper efficacy testing before they are recommended by clinicians.
Policy: Health-focused applications should be passed through a third-party rating system that will communicate to consumers whether the applications include expert recommendations and if they have undergone efficacy testing.
Research: Collaborative research is needed to ensure that evidence-based practices and expert recommendations are integrated into technologies marketed as health-promoting tools.
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(PDF 27.6 kb)
About this article
Cite this article
Schoffman, D.E., Turner-McGrievy, G., Jones, S.J. et al. Mobile apps for pediatric obesity prevention and treatment, healthy eating, and physical activity promotion: just fun and games?. Behav. Med. Pract. Policy Res. 3, 320–325 (2013). https://doi.org/10.1007/s13142-013-0206-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13142-013-0206-3