
Abstract
The aim of the present study was to assess whether the protective effects of ischemic preconditioning (PC) are associated with activation of the mitochondrial ATP-sensitive potassium channels (mitoKATP) and if there is any relationship between the activity of these channels and the mitochondrial permeability transition pore (MPTP) opening in ischemic-reperfused rat hearts under different nutritional conditions. Langendorff-perfused hearts of fed and 24-h fasted rats were exposed to 25 min of no-flow global ischemia plus 30 min of reperfusion. Fasting accelerated functional recovery and attenuated MPTP opening. The mitoKATP blocker, 5-hydroxydecanoic (HD), did not influence functional recovery and MPTP opening induced by ischemia–reperfusion in the fed hearts but partially reversed the beneficial effects of fasting. PC and the mitoKATP opener, diazoxide (DZ), improved functional recovery, preserved cell viability, and inhibited MPTP opening in both fed and fasted hearts. The protection elicited by PC and DZ on contractile recovery and MPTP opening was reversed by HD, which did not affect cell viability. Altogether, these results argue for a role of mitoKATP and its impact on preservation mitochondrial inner membrane permeability as a relevant factor in the improvement of contractile function in the ischemic-reperfused rat heart. They also suggest that the functional protection elicited by PC may be related to this mechanism.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
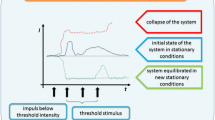
Brief intermittent ischemic periods separated by reperfusion prior to prolonged ischemia result in improved postischemic function and a highly significant reduction in infarct size. Although the protective effects of this phenomenon, called ischemic preconditioning (PC), have been amply described, the mechanisms involved are very complex, with mitochondria playing a key role, as critical mediators of cell survival and death in the setting of cardiac ischemia–reperfusion [4, 23, 35]. Specifically, many of the complex networks of intracellular signaling pathways recruited by PC converge on the mitochondrial permeability transition pore (MPTP), whose irreversible opening at the onset of myocardial reperfusion is a critical event recognized to be important in both necrotic and apoptotic cell death [14, 31, 35]. It is well known that the mitochondrial inner membrane is impermeable to almost all metabolites and ions under physiological conditions, and the MPTP is in a closed conformation. High concentrations of matrix calcium, coupled with oxidative stress, high inorganic phosphate, and adenine nucleotide depletion, conditions that are present in the ischemic-reperfused heart, promote MPTP opening and equilibration of molecules smaller than 1,500 Da, resulting in collapse of the potential difference across the inner mitochondrial membrane that is required to drive oxidative phosphorylation and leading to the impairment of ATP synthesis and necrotic cell death. Osmotic force also results in matrix swelling and ultimately in the rupture of the outer membrane, release of cytochrome c, and apoptotic cell death [4]. Although the structure of the MPTP remains a matter of debate, it is traditionally thought to be formed by an arrangement of the voltage-dependent anion channel in the outer mitochondrial membrane, the adenine nucleotide transporter in the inner membrane, and cyclophilin-D in the matrix. However, evidence has also been reported that ascribes the formation of the pore component to the mitochondrial phosphate carrier. In this model, the adenine nucleotide transporter (ANT) and cyclophilin-D may play a regulatory role. MPTP opening seems to be triggered by Ca2+, which may operate through a conformational change of ANT, facilitated by the binding of mitochondrial cyclophilin-D or through interaction of ANT and the phosphate carrier [33]. The mechanism through which MPTP opening is inhibited by PC remains unclear, although several potential mechanisms have been proposed including opening of mitochondrial ATP-sensitive potassium channels (mitoKATP) [7, 10, 32] and reduced cellular Ca2+ overload, this last effect attributed, at least in part, to inhibition of glycolysis [2, 8]. Similar changes in glucose metabolism may contribute to the beneficial effects of fasting [25]. In this respect, it has been shown that previous fasting, which enhanced triglyceride stores and accelerated oxidation of fatty acids derived from endogenous lipolysis, inhibited glycolysis during ischemia, accelerated contractile recovery, and decreased the extent of MPTP opening in the Langendorff-perfused rat heart subjected to no-flow global ischemia and reperfusion [19]. It has also been reported that PC, which lowered lactate production during ischemia in the hearts of rats fed ad libitum, elicited a more thorough functional protection in this nutritional condition as compared with the fasted hearts. Since the protective effect of PC could be observed in the absence of any change in anaerobic glycolysis in the fasted rats, it appears likely that the effects of PC could also depend on some other mechanisms [34]. On the other hand, it has been demonstrated that the beneficial effects of diazoxide (DZ), which selectively opens mitoKATP in a micromolar range, showed a fairly close similarity to the reported effects of PC. This agent improved the postischemic mechanical function in both nutritional conditions, although this effect was more pronounced in the fed rat hearts where it was accompanied by a decrease in lactate accumulation during ischemia. It preserved cell viability in the fed as well as in the fasted hearts, and interestingly, this cytoprotection was equivalent to that of PC [18].
On the basis of these observations and in order to gain a deeper insight into the mechanisms involved in the protective effects of PC under different nutritional conditions, the goal of the present study was to assess whether the protective effects of PC are associated with activation of the mitoKATP and if there is any relationship between the activity of these channels and the MPTP opening in hearts from fed and fasted rats. The effects of the mitoKATP blocker, 5-hydroxydecanoic (HD), on the cardioprotective actions of PC and DZ in Langendorff ischemic-reperfused hearts from fed and fasted rats were determined in the present study.
Materials and methods
Experimental protocol
The present study conformed to the Guide for the Care and Use of Laboratory Animals (1996, published by National Academy Press, 2101 Constitution Ave. NW, Washington, DC 20055, USA) and Argentine Law No. 14346 concerning animal protection. Female Wistar rats weighing 250–350 g were maintained on a 12-h dark-light cycle and were fed ad libitum or fasted for 24 h. Rats were anesthetized with diethylether, and heparin (250 IU) was injected into the jugular vein. Hearts were excised quickly and cooled in ice-cold saline until contractions stopped. Hearts were then mounted on a modified Langendorff apparatus (Hugo Sachs Elektronik, March-Hugstetten, Germany) and perfused isovolumically at a constant pressure of 70 mmHg with a non-recirculating Krebs–Ringer bicarbonate solution of the following composition (in mmol/L): NaCl, 120; HNaCO3, 25; KCl, 4.8; MgSO4, 1.33; KH2PO4, 1.2; CaCl2, 1.6; Na2EDTA, 0.02; and glucose, 10. The perfusate was gassed with 95 % O2 and 5 % CO2 (pH 7.4) and kept at a constant temperature of 37 °C. After instrumentation, each heart was randomly assigned to one of the following groups: control (C), after a 30-min equilibration period, hearts were subjected to 25 min of global ischemia and 30 min of reperfusion (ischemia was started by shutting off the perfusate flow); PC, PC consisted of 3-min ischemia and 5 min of reperfusion before sustained ischemia; PC + HD, 100 μM HD (Sigma, St Louis, MO, USA) was added to the perfusion medium 7 min before application of PC and maintained throughout the experiment; DZ, 10 μM DZ (Sigma, St Louis, MO, USA) dissolved in dimethyl sulfoxide (DMSO) was added to the perfusion medium 10 min before sustained ischemia and maintained throughout the experiment (the final concentration of DMSO was 0.01 %); DZ + HD, 100 μM HD was added to the perfusion medium 5 min before administration of 10 μM DZ and maintained throughout the experiment; DMSO, 0.01 % DMSO was added to the perfusion medium 10 min before sustained ischemia and maintained throughout the experiment; HD, 100 μM HD was added to the perfusion medium 15 min before sustained ischemia and maintained throughout the experiment.
Measurement of heart function
For measurement of left ventricular pressures, the left atrium was removed, and a latex balloon connected to a pressure transducer was inserted into the left ventricle through the mitral valve. The volume of the balloon was adjusted to obtain left ventricular end-diastolic pressure of 10 mmHg. Values for left ventricular that developed pressure, peak rate of contraction, and peak rate of relaxation were obtained using a digital data acquisition system (Unkel Scope Configuration Program for the PCLabCard Data Acquisition Boards from Advantec, USA; this program was adapted and modified by the technical assistant). Heart rate was measured by means of a counter triggered by the left ventricular-developed pressure pulse. Rate-pressure product was determined by multiplying heart rate by the left ventricular-developed pressure. Only hearts with left ventricular-developed pressure >60 mmHg and heart rate >200 bpm at the end of the equilibration period were included in the study (n = 8/group).
Measurement of cell viability
The hearts were removed at the end of the reperfusion period, frozen, and then cut into six to eight slices (approximately 0.8–1 mm). Following defrosting, slices were incubated at room temperature with 1 % triphenyltetrazolium chloride in phosphate buffer (100 mmol/L, pH 7.4) for 90 min and then fixed in 10 % formaldehyde solution to clearly distinguish stained viable tissue from unstained necrotic tissue. The areas of viable tissue were determined by means of computer morphometry (Scion Image B4, Frederick, MD, USA). Because the hearts had been exposed to global ischemia, the risk area was the total ventricular area minus cavities. Cellular viability was calculated as a percentage of risk area (n = 8/group). For measurement of heart function and cell viability, 96 hearts were successfully perfused and 8 hearts were excluded. One heart was excluded from the C group, two hearts from the PC group, one heart from the HD group, one heart from the PC + HD group, two hearts from the DZ group, and one heart from the DZ + HD group.
Assessment of MPT in situ using mitochondrial 2-deoxy-[3H]-glucose entrapment
This study was performed as described by Griffiths and Halestrap [9]. MPTP opening was assessed using a technique that involved mitochondrial entrapment of 2-deoxy-[3H]-glucose ([3H]-2-DG). [3H]-2-DG enters cells via the glucose transporter and is metabolized to 2-deoxyglucose-6-phosphate, which remains entrapped in the cytosol. This compound does not enter the mitochondria unless the MPTP opens, whereupon it equilibrates rapidly between the cytosol and mitochondrial matrix compartments. Consequently, the extent to which [3H]-2-DG is entrapped within the mitochondria is a reliable indicator of the number of mitochondria that have undergone MPTP opening.
After the stabilization period, hearts (n = 8/group) were perfused for 30 min in the recirculating mode with 40 mL Krebs–Ringer bicarbonate solution that contained 0.5 mmol/L [3H]-2-DG, 370 TBq/mL. Perfusion was then returned to non-recirculating mode with normal medium and was continued in the presence or absence of the different treatments and continued for 15 min before induction of sustained ischemia. This method washes the extracellular [3H]-2-DG from the heart, while cytosolic [3H]-2-DG remains entrapped. At the end of reperfusion, the ventricles were rapidly removed from the hearts, weighed, and homogenized in ice-cold sucrose buffer solution (300 mmol/L sucrose, 10 mmol/L Tris-Cl, 2 mmol/L EGTA, 5 mg/mL bovine serum albumin, pH 7.4). A sample of the homogenate was retained for measurement of the total number of [3H] disintegrations per minute (dpm); this was determined after precipitation of the protein by addition of an equal volume of 5 % (w/v) HClO4. The rest of the homogenate was used for isolation of mitochondria by centrifugation for 2 min at 2,000 g to remove cell debris, followed by centrifugation of the supernatant at 10,000 g for 5 min to sediment the mitochondria. The mitochondrial pellet was then washed three times in sucrose isolation buffer solution without bovine serum albumin and resuspended in a final volume of 2.5 mL isolation buffer solution. A 100-μL portion of the mitochondrial suspension was retained for performance of the citrate synthase assay, and 0.4 mL of 0.5 % HClO4 was added to the remainder to release entrapped [3H]. Protein was precipitated by centrifugation at 8,000 g for 2 min, and the resulting supernatant was counted for radioactivity in 2.5-mL scintillant liquid (Ecolite; MP Biomedicals, Irvine CA, USA). The mitochondrial uptake of [3H]-2-DG was calculated on the basis of the number of dpm measured in the mitochondrial extract. In order to correct for variation between experiments in the loading of hearts with [3H]-2-DG between experiments, dpm/g wet weight of tissue was determined for total homogenate. To correct for variations in the recovery of mitochondria between experiments, the citrate synthase activity in the mitochondrial inner membrane was measured in the mitochondrial fraction using spectrophotometry [30]. Mitochondrial dpm was expressed per unit of this enzyme.
The uptake of [3H]-2-DG, in dpm/unit citrate synthase, was expressed as the ratio with respect to dpm for the entire tissue sample. This ratio should be independent of both the loading of cells with [3H]-2-DG and the recovery of mitochondria.
Two hundred twenty-four hearts were successfully perfused and 19 hearts were excluded. Two hearts were excluded from the C group, three hearts from the PC group, three hearts from the HD group, four hearts from the PC + HD group, three hearts from the DZ group, and four hearts from the DZ + HD group.
Statistical analysis
Values are mean ± SEM. Changes in ventricular contractile functions were compared statistically using a factorial ANOVA followed by the Tukey’s test. Significance was set at p < 0.05.
Results
In agreement with previous reports [18], the baseline values of heart rate, rate-pressure product, peak rate of contraction, and peak rate of relaxation were similar in hearts from fed and fasted rats. The exposure to 25 min no-flow global ischemia led to complete cessation of spontaneous contractions in both fed and fasted rat hearts, and heart rate returned to preischemic values during the 30-min reperfusion. Neither PC nor DZ or HD had any effects on heart rate during ischemia or reperfusion (data not shown). As indicated by rate-pressure product, peak rate of contraction, peak rate of relaxation, and left ventricular end-diastolic pressure (Table 1), the left ventricle function recovered faster in the fasted than in the fed rat hearts, although the recovery reached similar values in both groups toward the end of the experiment. The beneficial effects of fasting were abolished by HD.
Table 1 also shows that PC improved the recovery of all functional parameters, which reached similar values in both nutritional groups. HD abolished protection by PC in both fed and fasted hearts. DMSO did not show effects by itself in a separate experimental test carried out with hearts from fed rats (data not shown). The DZ treatment produced a similar but less dramatic improvement in recovery, and administration of the mitoKATP blocker to DZ-treated hearts abolished this functional protection in both nutritional groups.
Figures 1 and 2 represent mitochondrial entrapment of [3H]-2-DG as an estimate of MPTP opening. In agreement with a previous study [19, 20], exposure to ischemia–reperfusion resulted in an increase in the entrapment of [3H]-2-DG, which was reduced by previous fasting. Given alone, HD did not influence MPTP opening induced by ischemia–reperfusion in the fed hearts but partially reversed the protection afforded by fasting on MPTP opening (Fig. 1). Mitochondrial retention of [3H]-2-DG was significantly reduced by the PC (Fig. 1) and DZ (Fig. 2) treatments in both nutritional conditions. The mitoKATP blocker partially reversed the effect of PC and fully reversed the effect of DZ on the MPTP.

Effects of preconditioning and 5-hydroxydecanoate (100 μM) (HD) on mitochondrial permeability transition pore opening, measured in situ by [3H]-2-DG entrapment. Open bars indicate end of the 30-min equilibration period; filled bars indicate end of the 30-min reperfusion period. C non-preconditioned hearts, PC preconditioned hearts, ischemic preconditioning consisted of 3-min ischemia and 5-min reperfusion before sustained ischemia. HD was given 15 min before the onset of sustained ischemia and remained for the duration of the experiment. Values (means ± SEM, n = 8) are expressed as 105 × ratio of mitochondrial [3H] dpm per unit of citrate synthase to total heart [3H] dpm/g wet weight. *p < 0.05 vs end of the 30-min equilibration period, same treatment, same nutritional state; **p < 0.01 vs end of the 30-min equilibration period, same treatment, same nutritional state; +p < 0.05 vs PC and vs HD end of the 30-min reperfusion period, same nutritional state; ++p < 0.01 vs PC and vs HD end of the 30-min reperfusion period, same nutritional state; &p < 0.05 vs C fed end of the 30-min reperfusion period

The effects of diazoxide 10 μM (DZ) on mitochondrial permeability transition pore opening, measured in situ by [3H]-2-DG entrapment. Open bars indicate end of the 30-min equilibration period; filled bars indicate end of the 30-min reperfusion period. C dimethyl sulfoxide (DMSO) was added to the perfusion medium 10 min before sustained ischemia and remained all over the experiment (the final concentration of DMSO was 0.01 %). DZ was given 10 min before the onset of sustained ischemia and remained for the duration of the experiment. HD was given 15 min before the onset of sustained ischemia and remained for the duration of the experiment. Values (means ± SEM, n = 8) are expressed as 105 × ratio of mitochondrial [3H] dpm per unit of citrate synthase to total heart [3H] dpm/g wet weight. **p < 0.01 vs end of the 30-min equilibration period, same treatment, same nutritional state; ##p < 0.01 vs C and DZ/HD end of the 30-min reperfusion period, same nutritional state; &p < 0.05 vs C fed end of the 30-min reperfusion period
DMSO did not show effects by itself on cell viability in a separate experimental test carried out with hearts from fed rats (data not shown). Consistent with data showing no difference in the percentage of viable myocytes after ischemia–reperfusion between hearts from fed and fasted rats (Fig. 5), retention of cellular [3H]-2-DG (Figs. 3 and 4) and the intact mitochondrial yield assessed by measurement of citrate synthase activity (Table 2) were similar in both nutritional groups. Given alone, HD did not modify any of these parameters. Coinciding with the preservation of cell viability by PC and DZ (Fig. 5) in the hearts from fed and fasted rats, cellular retention of [3H]-2-DG (Figs. 3 and 4) and intact mitochondrial yield (Table 2) were significantly higher in the preconditioned and DZ-treated hearts than in the control ischemic-reperfused hearts in both nutritional groups. These findings were anticipated because all [3H]-2-DG potentially entrapped in the cytosol and mitochondria would have been released from necrotic cells. None of these effects were altered by HD.

The effects of preconditioning and 5-hydroxydecanoate (100 μM) (HD) on total [3H]-2-DG content. Conditions and explanations are the same as in Fig. 1. Values (means ± SEM, n = 8) are expressed as total [3H]-2-DG uptake 103 × dpm/g wet weight. *p < 0.05 vs end of the 30-min equilibration period same treatment, same nutritional state and vs C end of the 30-min reperfusion period, same nutritional state; **p < 0.01 vs end of the 30-min equilibration period, same treatment, same nutritional state; ##p < 0.01 vs C and HD end of the 30-min equilibration period same nutritional state

The effects of diazoxide 10 μM (DZ) on total [3H]-2-DG content. Conditions and explanations are the same as in Fig. 2. Values (means ± SEM, n = 8) are expressed as total [3H]-2-DG uptake 103 × dpm/g wet weight. **p < 0.01 vs end of the 30-min equilibration period, same treatment, same nutritional state; #p < 0.05 vs DZ and DZ/HD end of the 30-min reperfusion period, same nutritional state

Effects of preconditioning, diazoxide, and 5-hydroxydecanoate on cell viability. % cellular viability is expressed as the percentage of risk area. Conditions and explanations are the same as Table 1. **p < 0.01 vs C and HD, same nutritional condition
Discussion
The present data confirm the previously reported protective effects of PC on myocardial performance in the ischemic-reperfused hearts from fed and fasted rats [34]. Consistently also with earlier findings, the DZ treatment produced a similar but less dramatic improvement in recovery [18]. Furthermore, the functional protection elicited by PC and DZ was accompanied by significant inhibition of MPTP opening. It is worth noting that fasting itself elicited improvement of functional recovery and attenuation of MPTP opening [19], while protection by PC and DZ was similar in absolute values in both nutritional conditions, thus the effects appear to be proportionally greater in the fed rat hearts. Regarding the effects of fasting, it should be noted that in contrast to previous investigations [18–21, 26, 27], a recent study has demonstrated detrimental effects of previous fasting on the postischemic recovery of isolated rat heart subjected to no-flow global ischemia–reperfusion [17]. While the latter investigation used buffers supplemented with glucose, insulin, and fatty acids at concentrations that mimic the blood plasma levels found in the fed and fasted states, the others used glucose, fatty acids, and insulin in concentrations similar to fed conditions or glucose as the only energy substrate, suggesting that the disagreements might be explained by the composition of the perfusate solution and the important role of glucose in the recovery of contractile function. Regardless of these discrepancies, present findings provide further support to the idea that interventions that inhibit the opening of the MPTP improve postischemic contractile recovery.
Although the [3H]-2-DG entrapment technique used in this study to evaluate the opening of the MPTP does not measure this opening in the cells that have undergone necrosis during ischemia–reperfusion and have consequently released the [3H]-2-DG trapped in the cytosol and mitochondria to the perfusion medium, thus leading to underestimation of the evaluated phenomenon, it has the advantage of measuring “in situ” the magnitude of the opening of the MPTP occurred in the viable cells remaining at the end of the reperfusion period. This measurement provides valuable information since mitochondria cannot synthesize ATP during the opening of the MPTP due to the free diffusion of H+ and the collapse of the potential difference across the inner mitochondrial membrane, which is accompanied by the hydrolysis of ATP by operation in reverse form of the FoF1ATP synthase [3, 12, 13]. Because the heart depends almost entirely on mitochondrial supply of ATP for the maintenance of reperfusion, inhibition of MPTP opening would improve functional recovery when reperfusion occurs. Both protective effects of PC and DZ were reversed by HD, arguing for a role of mitoKATP and its impact on mitochondrial permeability as a relevant factor in the improvement of contractile function elicited by PC in the ischemic-reperfused rat heart. Although it was not proved in this study, induction of inner membrane depolarization, which in turn would reduce the driving force for Ca2+ uptake by mitochondria and thereby prevent mitochondrial matrix Ca2+ overload, may explain how mitoKATP activation reduces MPTP opening [5, 16, 22, 24, 35]. Reinforcing this idea, Abdallah et al. [1] found that pretreatment of isolated myocytes with DZ generated a slight depolarization of the mitochondrial membrane, which could limit the influx of Ca2+ and thus reduce mitochondrial Ca2+ overload during ischemia–reperfusion.
The present data show similar preservation of cell viability together with similar total cellular retention of [3H]-2-DG and mitochondrial yield, either in the presence or absence of HD in both nutritional groups. On the other hand, PC and DZ treatments were associated with the preservation of cell viability and an increase in total tissue content of [3H]-2-DG, together with a higher yield of intact mitochondria. In contrast with other studies that show that HD reversed the reduction of infarct size by PC and DZ [6, 10, 28], but in agreement with those who found that this agent did not reverse such effect [11, 29], the present data show that HD did not affect the preservation of cell viability or modified cell retention of [3H]-2-DG in the preconditioned and DZ-treated hearts, despite reversing the beneficial effects of these treatments on the MPTP. If the MPTP opens and then subsequently closes, the [3H]-2-DG will remain entrapped even though the mitochondria are resealed [15]. However, while the pore stays open, not only prevents ATP synthesis but also the ATP synthesis, machinery actually goes into reverse and catalyses the hydrolysis of ATP produced by glycolysis or “healthy” mitochondria. Thus, transient opening of MPTP under the present experimental conditions could explain a lower functional recovery without modifications in cell viability or mitochondrial recovery, suggesting that the protection against irreversible cell damage generated by PC and DZ would not be mediated by inhibition of the opening of the MPTP nor would require activation of the mitoKATP in this experimental model. Since MPTP is not only related to necrotic cell death, but its opening also contributes to the activation of apoptosis and autophagy, further studies are required to determine activation of apoptosis-effector caspases and autophagic markers in the ischemic-reperfused heart and the effects of PC and DZ.
In conclusion, these results lend support to the idea that mitoKATP are, at least in part, involved in the inhibition of MPTP opening elicited by fasting and PC and that this is associated with an improvement in functional recovery under the present experimental conditions.
Abbreviations
- ANT:
-
Adenine nucleotide transporter
- C:
-
Control
- DMSO:
-
Dimethyl sulfoxide
- DZ:
-
Diazoxide
- HD:
-
5-Hydroxydecanoic
- [3H]-2-DG:
-
2-Deoxy-[3H]-glucose
- mitoKATP:
-
Mitochondrial ATP-sensitive potassium channels
- MPTP:
-
Mitochondrial permeability transition pore
- PC:
-
Ischemic preconditioning
References
Abdallah Y, Wolf C, Meuter K, Piper HM, Reusch HP, Ladilov Y (2010) Preconditioning with diazoxide prevents reoxygenation-induced rigor-type hypercontracture. J Mol Cell Cardiol 48:270–276
Asimakis GK, Inners-McBride K, Medellin G, Conti VR (1992) Ischemic preconditioning attenuates acidosis and postischemic dysfunction in isolated rat heart. Am J Physiol 263:H887–H894
Baines CP (2009) The mitochondrial permeability transition pore and ischemia-reperfusion injury. Basic Res Cardiol 104(2):181–188
Di Lisa F, Semenzato M, Carpi A, Menazza S, Kaludercic N, Menabò R, Canton M (2010) In: Minotti G (ed) Mitochondrial dysfunction in cell injury and cardiotoxicity in cardiotoxicity of non-cardiovascular drugs. Wiley, Chichester, pp 1–23
Facundo HT, de Paula JG, Kowaltowski AJ (2005) Mitochondrial ATP-sensitive K + channels prevent oxidative stress, permeability transition and cell death. J Bioenerg Biomembr 37(2):75–82
Fryer RM, Eells JT, Hsu AK, Henry MM, Gross GJ (2000) Ischemic preconditioning in rats: role of mitochondrial K(ATP) channel in preservation of mitochondrial function. Am J Physiol 278:H305–H312
Fryer RM, Hsu AK, Gross GJ (2001) Mitochondrial K (ATP) channel opening is important during index ischemia and following myocardial reperfusion in ischemic preconditioned rat hearts. J Mol Cell Cardiol 33:31–34
Gabel S, Cross HR, London RE, Steenbergen C, Murphy E (1997) Decreased intracellular pH is not due to the increased H+ extrusion in preconditioned rat hearts. Am J Physiol 273:H2257–H2262
Griffiths EJ, Halestrap AP (1995) Mitochondrial non specific pores remain closed during cardiac ischemia, but open upon reperfusion. Biochem J 307:93–98
Gross GJ, Peart JN (2003) KATP channels and myocardial preconditioning: an update. Am J Physiol Heart Circ Physiol 285:H921–H930
Grover GJ, Murray HN, Baird AJ, Dzwonczyk S (1995) The KATP blocker sodium 5-hydroxydecanoate does not abolish preconditioning in isolated rat hearts. Eur J Pharmacol 277:271–274
Halestrap AP (2009) What is the mitochondrial permeability transition pore? J Mol Cell Cardiol 46(6):821–831
Hausenloy DJ, Ong SB, Yellon DM (2009) The mitochondrial permeability transition pore as a target for preconditioning and postconditioning. Basic Res Cardiol 104:189–202
Jennings RB (2013) Historical perspective on the pathology of myocardial ischemia/reperfusion injury. Circ Res 113:428–438
Kerr PM, Suleiman MS, Halestrap AP (1999) Reversal of permeability transition during recovery of hearts from ischemia and its enhancement by pyruvate. Am J Physiol 276:H496–H502
Korge P, Honda HM, Weiss JN (2002) Protection of cardiac mitochondria by diazoxide and protein kinase C: implications for ischemic preconditioning. Proc Natl Acad Sci 299:3312–3317
Liepinsh E, Makrecka M, Kuka J, Makarova E, Vilskersts R, Cirule H, Sevostjanovs E, Grinberga S, Pugovics O, Dambrova M (2014) The heart is better protected against myocardial infarction in the fed state compared to the fasted state. Metab Clin Exp 63:127–136
Marina Prendes MG, Rastelli AH, Astudilla C, Fernández MA, Martínez M, Perazzo JC, Testoni G, Savino EA, Varela A (2004) Influence of fasting on the effects of diazoxide in the ischemic-reperfused rat heart. J Physiol Biochem 60:51–58
Marina Prendes MG, González MS, Torresín ME, Hermann R, Pascale NG, Jaitovich MM, Savino EA, Varela A (2009) Involvement of mitochondrial permeability transition, glutathione status, pentose phosphate pathway and oxidative damage in the protective effect of fasting in the ischemic-reperfused rat heart. Clin Exp Pharmacol Physiol 36:637–642
Marina Prendes MG, González MS, Hermann R, Pascale NG, Torresín ME, Jaitovich MM, Savino EA, Varela A (2010) Involvement of the mitochondrial ATP-sensitive potassium channel in the beneficial effects of fasting on the ischaemic-reperfused rat heart. In: Haugen S, Meijer S (eds) Handbook of nutritional biochemistry: genomics, metabolomics and food supply. Nova Science Publishers, United States of America, pp 483–494
Montessuit C, Papageorgiou I, Tardy I, Cantalupi I, Rosenblatt-Velin N, Lerch R (2000) Postischemic recovery of heart metabolism and function: role of mitochondrial fatty acid transfer. J Appl Physiol 89:111–119
Murata M, Akao M, O’Rourke B, Marban E (2001) Mitochondrial ATP sensitive potassium channels attenuate matrix Ca2+ overload during simulated ischemia and reperfusion: possible mechanism of cardioprotection. Circ Res 89:891–898
Ong SB, Gustafsson AS (2012) New roles for mitochondria in cell death in the reperfused myocardium. Cardiovasc Res 94:190–196
O’Rourke B (2004) Evidence of mitochondrial K + channels and their role in cardioprotection. Circ Res 94:420–432
Ramasamy R, Liu H, Cherednichenko G, Schaefer S (2001) Fasting limits the increase in intracellular calcium during ischemia in isolated rat hearts. Basic Res Cardiol 96:463–470
Schaefer S, Ramasamy R (1997) Glycogen utilization and ischemic injury in the isolated rat heart. Cardiovasc Res 35:90–98
Schneider CA, Taegtmeyer H (1991) Fasting in vivo delays myocardial cell damage after brief periods of ischemia in the isolated working rat heart. Circ Res 68:1045–1050
Schultz JE, Qian YZ, Gross GJ, Kukreja RC (1997) The ischemia-selective KATP channel antagonist, 5-hydroxydecanoate, blocks ischemic preconditioning in the rat heart. J Mol Cell Cardiol 29:1055–1060
Schwartz LM, Welch TS, Crago MS (2002) Cardioprotection by multiple preconditioning cycles does not require mitochondrial K(ATP) channels in pigs. Am J Physiol 283:H1538–H1544
Shepherd D, Garland PB (1969) The kinetic properties of citrate synthase from rat liver mitochondria. Biochem J 144:597–599
Sivaraman V, Yellon DM (2014) Pharmacologic therapy that simulates conditioning for cardiac ischemic/reperfusion injury. J Cardiovasc Pharmacol Ther 19:83–96
Sunaga D, Tanno M, Miki T, Kuno A, Kouzu H, Sato T, Ishikawa S, Ogasawara M, Tobisawa T, Miura T (2013) Activation of the mitochondrial ATP-sensitive potassium channel achieves cell protection by promoting re-closure of the mPTP via suppression of GSK-3beta—complex III interaction. Eur Heart J 34:1859
Varanyuwatana P, Halestrap AP (2012) The roles of phosphate and the phosphate carrier in the mitochondrial permeability transition pore. Mitochondrion 12(1):120–125
Varela A, Marina Prendes MG, Testoni G, Vázquez N, Astudilla C, Cerruti S, Savino EA (2002) Influence of fasting on the effects of ischemic preconditioning in the ischemic-reperfused rat heart. Arch Physiol Biochem 110:189–196
Walters AM, Porter GA Jr, Brookes PS (2012) Mitochondria as a drug target in ischemic heart disease and cardiomyopathy. Circ Res 111:1222–1236
Acknowledgments
The authors thank Norma Gladys Infante for the technical assistance. This research was supported in part by grants from Universidad de Buenos Aires and IQUIMEFA-CONICET.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Marina Prendes, M.G., Hermann, R., Torresin, M.E. et al. Role of mitochondrial permeability transition pore and mitochondrial ATP-sensitive potassium channels in the protective effects of ischemic preconditioning in isolated hearts from fed and fasted rats. J Physiol Biochem 70, 791–800 (2014). https://doi.org/10.1007/s13105-014-0347-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13105-014-0347-y