
Abstract
Objectives
Excessive stress has become a common health concern that may result in deleterious physical and psychological conditions. Mindfulness has emerged as a practice that may buffer stress reactivity and researchers have progressively used an empirically validated laboratory protocol, the Trier Social Stress Test, to elicit stress reactivity to examine the buffering capacity of mindfulness. This systematic review aims to (1) summarize the literature on the effects of mindfulness interventions (MI) on stress reactivity measured via the Trier Social Stress Test (TSST), and (2) examine methodological variability across this literature and how variations in methodology may be influencing stress reactivity outcomes.
Methods
Various databases (PubMed, PsycINFO, MEDLINE, and PsycArticles) were systematically searched to identify MI studies that included stress reactivity to the TSST as a dependent outcome.
Results
Six out of 13 studies with physiological variables and seven out of 10 studies with self-report variables demonstrated the stress-buffering effects of MI on acute stress induction. Participant populations, differences in control groups, MI protocols, intervention dosage, and the number of TSST administrations seem to influence the stress-buffering effects of MI.
Conclusions
The ability of MI to buffer stress reactivity seems to be robust when measured via self-report, but stress-buffering effects are less clear for physiological measures. There is evidence that variations in study methodology may influence stress reactivity outcomes; the type of mindfulness practice and the dosage of practice seem to be particularly influential. Further research is necessary to more accurately characterize the relation between MI and stress reactivity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
In the past 30 years, excessive stress has been considered a significant public health concern. As early as 1979, the Office of United States Public Health identified stress as being a source of serious physical and psychological health conditions, including exhaustion, cognitive decline, depressive symptoms, anxiety, avoidance behaviors, negative social relationships, and mental health disorders (Everly and Lating 2013; Juster et al. 2010). Unfortunately, stress is a frequent and common experience for many people. Stress is often defined as the interpretation of potentially threatening stimuli exceeding perceived resources (Lazarus and Folkman 1984). Individual propensity and capacity to respond to acute stressors have been labeled stress reactivity (Linden et al. 1997). Maladaptive responses to these stressors, including both excessive and blunted responses, can lead to poor psychological and physical health outcomes (Dickerson and Kemeny 2004; Schneiderman et al. 2005). Excessive stress reactivity responses are associated with a host of negative health outcomes (Everly and Lating 2013). Interventions that are able to reduce the stress reactivity response (i.e., buffer against excessive stress reactivity) are needed.
Mounting evidence indicates that mindfulness interventions (MI) may alter stress reactivity, thus offering a novel solution to stress as a public health problem; however, additional high-quality research is required to characterize and understand the underlying mechanism driving the stress-buffering effect (Brown et al. 2015). Recent theoretical developments by Creswell and Lindsay (2014) posit that mindfulness buffers against the effects of stress by dually mitigating stress appraisals (cognitive, “top-down” pathway) and biological reactivity to stressors (physiological “bottom-up” pathway). For instance, researchers have found that mindfulness training has reduced self-reported responses to stress reactivity (Creswell et al. 2014), and that it has reduced biological reactivity (i.e., bottom-up stress-buffering) to acute stress induction (Engert et al. 2017). Based on both of these mechanisms, the mindfulness stress-buffering hypothesis also suggests that these stress-buffering effects account for the positive effects of MI on health (Creswell and Lindsay 2014). In order to scientifically evaluate the potential of MI to alter stress reactivity, standardized and replicable methods to induce the physiological stress response are necessary. Two bodily systems that are often considered in the stress response are the hypothalamic-pituitary-adrenal (HPA) axis and the cardiovascular system. Activation of the HPA axis sets off a number of physiological reactions that result in the release of cortisol, and activation of the cardiovascular system results in increased heart rate and blood pressure, all of which have a robust literature base as markers of sympathetic activation (Allen et al. 2016; Dickerson and Kemeny 2004). One way to study acute physiological and psychological stress reactivity is by using a standardized laboratory task to mimic psychosocial stress that an individual may experience (Dickerson and Kemeny 2004). Consequently, the Trier Social Stress Test (TSST) was developed, and it has since become the most widely used “gold standard” for inducing an acute stress response in a standardized manner across a variety of populations (Dickerson and Kemeny 2004; Kirschbaum et al. 1993). Briefly, the TSST protocol consists of laboratory confederates directing a participant to prepare and deliver a speech and complete a series of math calculations in a socially stressful environment. The speech and math questions are delivered before confederates and in front of a video camera, and participants are instructed that their recorded performance is being evaluated by experts in non-verbal communication. Although the field of stress research has made use of a highly standardized methodology to examine the effects of stress (e.g., wide adoption of the TSST), methodological issues have been noted in mindfulness research. Specifically, critiques of the field have discussed that much research has failed to report on the type of practice and length of time spent practicing, and MI studies often do not make use of robust active control conditions (Davidson and Kaszniak 2015). Further, the lack of robust active control conditions can impede the synthesis of the research results. It can be difficult to parse out the effects of a mindfulness intervention when matched with an inadequate control condition. For instance, it can become unclear as to whether participants experienced adverse effects from the inadequacy of the control condition rather than an amelioration under the intervention condition. These limitations may be due to the fact that it is a relatively new field, and many initial questions have yet to be answered, so much of the research is still in the exploratory stages. However, when it comes to testing theories (e.g., the mindfulness stress-buffering hypothesis), a methodology that increases standardization, replicability, and comparability across research laboratories is critical to collect reliable evidence to support (or disprove) such theories.
The potential for MI to buffer stress reactivity to a standardized and widely used laboratory stress induction protocol like the TSST has garnered interest among mindfulness researchers. However, there are currently no reviews synthesizing and critically analyzing the effects of MI on a comparable stress induction task, such as the TSST. Therefore, this systematic review aims to (1) summarize the MI literature that has used the TSST to measure stress reactivity, (2) evaluate the ability of MI to buffer stress reactivity via both physiological and self-report variables, (3) examine any methodological variability in this literature base to determine aspects that may moderate the effectiveness of MI in buffering stress reactivity, and (4) use these findings to provide recommendations to enhance future mindfulness stress-buffering research.
Methods
Literature Search Strategy
The literature search was conducted in the electronic databases PsycINFO, PubMed, PsychArticles, and MEDLINE, and included the search terms “mindfulness,” “TSST,” and “Trier Social Stress Test.” Reference lists of studies were also manually searched and relevant papers were added. Papers were identified and considered for this review until January 2019. The inclusion criteria consisted of papers that were peer-reviewed, published in English, and included a mindfulness intervention and a control condition. Studies were also required to have implemented the intervention prior to stress induction via the Trier Social Stress Test. Studies that reported the use of a modified TSST were acceptable as long as they contained the two defining elements of both a public speaking task and a math task that were performed in front of live confederate evaluators. The studies also needed to evaluate at least one measure of stress reactivity (e.g., cortisol, heart rate, self-reported stress) at multiple time points (i.e., before and after the TSST) to assess baseline to peak stress reactivity in response to the stressor. Papers were excluded if the selected participants were experienced meditators due to the potential confound of the effects long-term training with effects of an intervention, and due to the potential selection bias of conducting research among this sample (e.g., long-term meditators may represent a non-normative group regardless of their meditation practice). Studies were also excluded if they only used one of the two evaluative stressors present in the TSST (i.e., public speaking task or math task only). This decision was made based on Dickerson and Kemeny’s (2004) conclusion that stress reactivity to the TSST is most robust among studies that included both the speech and math components.
Study Selection and Data Extraction
After studies were gathered, duplicates were excluded and titles and abstracts of search results were reviewed to determine the study eligibility for a full-text review. Two authors independently read the remaining papers and excluded papers that did not meet the aforementioned criteria. All discrepancies during this process were discussed among all authors until consensus was reached. Sample sizes, participant characteristics, intervention type, stress reactivity measures, and outcomes were then extracted from the remaining studies.
The studies were also coded for methodological characteristics, including the use of a control group, type of MI protocol implemented, and intervention dosage. Control conditions were coded based on the designations created by Felver et al. (2016). To be considered a “full-active control” the study was required to incorporate both a didactic (e.g., presentation of content material) and an experiential (e.g., attention training) component. To be considered a “semi-active control” the study included only one component (i.e., didactic or experiential). Both full-active and semi-active control groups were also required to match the length of the MI in order to be considered in these categories. Studies that had controls with neither an experiential or didactic component were coded as “not-active controls.”
All studies reported at least one aspect of MI dosage. The three primary measures of MI dosage included intervention session frequency, intervention time per session, and total intervention duration. Intervention session frequency was measured by the number of sessions included in the MI protocol and was reported in the form of session numbers and days. Intervention time per session was measured by the minutes per session. Total intervention duration was measured as the length of time (i.e., days and weeks) that the intervention lasted.
Results
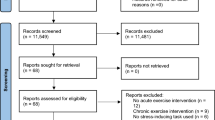
The initial search resulted in 75 papers. Duplicates were removed (n = 39) and five additional articles were removed based on title and abstract reviews if they were clearly unrelated to MI and TSST research. This left 31 articles for full-text analysis. Of these papers, eight were excluded for not assessing an intervention, two were removed for not using a TSST, two were removed for not including a control group, one was removed for not using a TSST post-intervention, one was removed because it used the same dataset as a previous paper, and one was eliminated due to a lack of stress reactivity measurement. One final paper was excluded because the subjects of the study were experienced meditators. The full selection process for this review is detailed in Fig. 1. The first and second authors independently performed data extraction and achieved an inter-rater reliability (IRR) of 97.4%. Disputes between coders were discussed until consensus was reached. Characteristics of the 15 studies included are summarized in Table 1.

Flow diagram (PRISMA) for the study selection process. MM: conceptualized and primarily wrote the manuscript. EH & JF: collaborated with the conceptualization, writing, and editing of the manuscript. All authors approved the final version of the manuscript for submission
A summary of the coded data from the selected studies are provided in Table 2. All studies measured effects of MI on stress reactivity to the TSST. Studies included one or more stress reactivity measures, including both physiological and self-report measures. Three of 12 studies with neuroendocrine measures, four of six studies with cardiovascular measures (e.g., HRV, blood pressure), and seven of 10 studies with self-report measures demonstrated stress buffering effects of MI.
Gender and age varied widely across studies. While most studies examined mixed-sex subjects, three studies experimented with female only subjects (20%). Participant age ranged from 18 years old (Cruess et al. 2015) to 60 years old (Kemeny et al. 2012) with an average age of 34.2 (SD = 11.5) across studies that reported on age. Methodology also varied considerably across studies, particularly in participant population characteristics, use of an active control group, MI protocol, intervention dosage, and number of TSST administrations. These variations will be discussed in detail and considered as potential moderators of MI effectiveness (see “Methodological Variations”) in this review.
The majority of the studies examined psychophysiological markers of stress (n = 13, 87%). Cortisol was the most common dependent variable examined among the psychophysiological measures and was measured in 12 out of 15 studies (80%). Other psychophysiological variables included salivary alpha-amylase (n = 3, 20%), cardiovascular measures (n = 6, 40%), and inflammatory biomarkers (n = 4, 27%). A large percentage of the studies (n = 10, 67%) included self-report measures in their studies. The following section summarizes the literature that has employed the TSST to measure stress reactivity, organized by outcome variables.
Neuroendocrine Measures
A total of 12 studies (80%) examined neuroendocrine measures. All 12 studies measured cortisol reactivity, and three also measured salivary-alpha amylase (sAA) reactivity to the TSST. Cortisol reactivity and sAA reactivity both refer to the increase from baseline levels (pre-TSST) to peak levels (post-TSST). Samples for peak cortisol levels were taken on average 25.1 min (SD = 6.6) after the onset of the TSST, with one study sampling much earlier (13 min post-onset; Cruess et al. 2015) and one study sampling much later (~ 40 min post-onset; Robert-McComb et al. 2015). Additionally, one study reported cortisol results in area under the curve (AUC) units rather than change in baseline to peak levels (Hoge et al. 2018). Samples for peak sAA levels were taken on average 12.7 min (SD = 2.5) after the onset of the TSST.
Three of the 12 studies (25%) indicated significant group differences in cortisol reactivity in the expected direction (i.e., MI buffered cortisol reactivity). In examining the Mindfulness-Based Relapse Prevention (MBRP) program for adults with stimulant use disorders, Glasner-Edwards et al. (2017) found that the MI group demonstrated significantly lower cortisol levels than the intervention group at the conclusion of the post-intervention TSST. Other researchers have indicated decreased cortisol reactivity for stressed adults in the MI group when compared with the two control groups (Lindsay et al. 2018). Engert et al. (2017) demonstrated decreased cortisol reactivity in a community sample for three out of the four MI groups in the study when compared with a no-training control group.
One study demonstrated a trend toward stress-buffering effects of MI effects on cortisol reactivity. Robert-McComb et al. (2015) examined a mindfulness-based movement intervention for female university students and found a trend decrease in cortisol in the MI group when compared with that in the control. The trend was not significant, but the authors discussed that this could have been due to the study being underpowered (N = 17 participants).
Six studies (46%) found no decrease in cortisol reactivity between MI and control groups (Arch et al. 2014; Basso et al. 2019; Hoge et al. 2018; Nyklíček et al. 2013; Pace et al. 2009; Rosenkranz et al. 2013). Two studies (15%) reported differences in cortisol reactivity in the unexpected direction (i.e., control group demonstrated less cortisol reactivity than the MI group). Creswell et al. (2014) found that the mindfulness group had increased cortisol reactivity to the TSST relative to the control condition. Notably, this was in contrast to significant decreases in self-reported stress reactivity in the MI group. To explore these unexpected results, they examined participants based on pre-existing dispositional mindfulness and separated participants into high and low dispositional mindfulness groups. Subsequently, they identified that participants who were low in pre-existing levels of dispositional mindfulness and then received mindfulness meditation training had the greatest cortisol reactivity to the TSST. Additionally, Cruess et al. (2015) found increased cortisol reactivity in the MI group when compared with a somatic relaxation control group. However, there were no differences between the MI group and a second, non-active control group in the same study, indicating that differences may be due to the effectiveness of the somatic-relaxation intervention and not necessarily indicative of heightened reactivity due to MI training.
Three out of 15 studies (20%) examined salivary alpha-amylase, and only one demonstrated that MI buffered sAA reactivity. Arch et al. (2014) found significantly lower sAA levels in the MI group compared with those in the control group after stress induction. Cruess et al. (2015) and Engert et al. (2017) did not find significant differences for sAA between groups.
Cardiovascular Measures
A total of 6 out of 15 studies (40%) examined cardiovascular measures. One of the six studies (17%) examined heart rate, four (67%) examined heart rate variability (HRV) and/or respiratory sinus arrhythmia (RSA), and four (67%) examined blood pressure. Heart rate reactivity and blood pressure reactivity both refer to the increase from baseline levels (pre-TSST), to peak levels (during the TSST). HRV and RSA reactivity refer to the decrease from baseline levels (pre-TSST) to lowest levels (during the TSST).
The one study that examined heart rate reactivity found no significant group differences when comparing the MI groups and the control group (Engert et al. 2017). One of the four studies examining HRV or RSA reported stress-buffering effects of MI. Importantly with these variables, decreased levels of HRV or RSA are indicative of increased stress reactivity. Arch et al. (2014) demonstrated stress buffering effects of MI on RSA (i.e., RSA stayed at the same level during the TSST and RSA decreased in the control group) during the speech preparation task, but not during the speech or math tasks.
Three studies did not identify differences in RSA or HRV between groups (Engert et al. 2017; Kemeny et al. 2012; Nyklíček et al. 2013). However, upon further analysis, Kemeny et al. (2012) demonstrated that individuals who reported more MI home practice evidenced buffered RSA reactivity to the TSST relative to those that did not practice as much and relative to the control group.
Out of the four studies that examined systolic blood pressure (SBP) and diastolic blood pressure (DBP) as dependent variables, two studies demonstrated significant stress buffering effects. Lindsay et al. (2018) found that the mindfulness training group demonstrated reduced systolic blood pressure (SBP) reactivity compared to two control groups. Nyklíček et al. (2013) indicated that there were significant differences in blood pressure reactivity between the MI and waitlist group.
Creswell et al. (2014) did not find any differences between MI and control groups for SBP or DBP reactivity to the TSST. Similarly, Kemeny et al. (2012) did not find group differences in SBP and DBP reactivity; however, when the mindfulness practice was taken into consideration, individuals with increased practice demonstrated decreased blood pressure reactivity during the TSST.
Inflammatory Biomarkers
Among the 15 studies, a total of four studies (24%) examined inflammatory biomarkers as measures of stress reactivity. Inflammatory reactivity refers to the increase from baseline levels (pre-TSST) to peak levels (post-TSST) of the biomarkers.
Hoge et al. (2018) measured IL-6 and TNF-α levels and found significantly reduced stress reactivity in the MI group compared with that in the control group for all three variables. Pace et al. (2009) examined IL-6 and found no initial group differences in IL-6 reactivity; however, when the authors incorporated mindfulness practice into the analyses, increased practice time was correlated with decreased IL-6 reactivity in the MI group. Similarly, Rosenkranz et al. (2013) found no differences for inflammatory reactivity in blister fluid levels (looking at IL-8 and TNF-α) between groups, but when examining increased practice time, participants in the MI group demonstrated significantly lower post-TSST TNF-α levels compared with the control group. Finally, Engert et al. (2017) indicated no significant group differences in C-Reactive protein or IL-6 reactivity.
Self-Report
Self-report measures were used to evaluate aspects of stress reactivity by administering the measures prior to and following the TSST. Ten of the 15 studies (67%) examined self-report stress reactivity outcomes. These measures included the State-Trait Anxiety Inventory (STAI; n = 5), Subjective Units of Distress Scale (SUDS; n = 2), the Profiles of Mood States (POMS; n = 1), and visual analogue scales (n = 3). Self-reported stress reactivity refers to the increase in self-reported stress from baseline (pre-TSST) to peak stress (either during or immediately after TSST). Overall, seven of the 10 studies (70%) demonstrated stress buffering effects of MI via self-report.
Summary
The previous section summarized the results of the literature that has examined stress reactivity among participants faced with the TSST. Table 2 provides a summary of the studies included in this systematic review. The studies varied in the number of stress reactivity measures, including both physiological and self-report measures. Four of 12 studies with neuroendocrine measures, three of six studies with cardiovascular measures, one of four studies with inflammation measures, and seven of 10 studies with self-report measures demonstrated stress buffering effects of MI. Two studies with cortisol showed effects of MI in the unexpected direction. Other methodological variables are important to examine to account for variability that may be impacting the current literature base and the reported results.
Methodological Variations
To better understand the variability across the 15 studies in this review, this section aims to examine variations in methodological characteristics and how they influence results across studies. These characteristics include participant population, control conditions, mindfulness protocols, intervention dosage, and number of TSST administrations. These characteristics will be considered as moderators for cortisol reactivity, cardiovascular reactivity, and self-reported stress reactivity. The goal of this section is to identify elements that may influence MI in buffering stress reactivity. These results will be used to inform recommendations included in the final section.
Participant Populations
The population characteristics are quantified in this section to better understand the types of groups examined in the stress reactivity literature that use the TSST. The reviewed studies aimed to address stress reactivity among both clinical and non-clinical populations. Out of the 15 studies, four studies (27%) examined clinical populations and the remaining studied normative groups (n = 11, 73%). Studies examining clinical populations were varied with the targeted groups including individuals with generalized anxiety disorder (GAD; Hoge et al. 2013, 2018), adults with stimulant use disorder (Glasner-Edwards et al. 2017), and recurrent unipolar depression (Britton et al. 2012). Among the healthy individuals, there was heterogeneity in terms of age and demographic characteristics. Almost half of the studies examining normative populations targeted college students (n = 5, 45%). Other healthy populations included non-clinical school teachers, (Kemeny et al. 2012) and community volunteers (Engert et al. 2017) among others.
Moderating Effects of Participant Populations
For cortisol, one out of two studies (50%) in clinical populations and two out of nine studies (22%) in normative populations evidenced decreased cortisol reactivity in MI groups compared to controls. Two studies (22%) with normative populations evidenced increased cortisol reactivity in the MI compared to a control group. When considering the studies in normative populations only, two out of four (50%) of studies in community samples demonstrated buffering effects of MI on cortisol, while no studies in college populations (n = 5) demonstrated stress buffering effects of MI. Notably, the two studies that demonstrated increased cortisol reactivity in the MI group were in college populations.
None of the studies examining cardiovascular outcomes (n = 6) were in clinical populations. For the studies in normative populations, two out of the four studies (50%) with community samples, and one of the two studies (50%) in college samples demonstrated buffering effects of MI on cardiovascular measures.
For the 10 studies that included self-report measures of stress reactivity, three were in clinical populations and seven were in healthy populations. All three studies (100%) in clinical populations evidenced decreased self-reported stress reactivity in MI groups compared to controls, and four out of seven (57%) studies in healthy populations evidenced decreased self-reported stress reactivity. When considering the studies in normative populations only, two out of three (67%) of studies in community samples and two of the four studies (50%) in college populations demonstrated stress buffering effects of MI on self-reported stress reactivity.
Control Conditions
As previously stated, the studies were coded for their adherence to a full-active control if the researchers included both an experiential and didactic component and the control was matched in length. The paper was coded with a semi-active control if the study included only one component (i.e., didactic or experiential) and was matched in length. Studies in which the control did not include either component were considered to have not-active control groups.
Out of the 15 studies, seven of the studies (47%) met the criteria for utilizing full-active control conditions. Three studies (20%) included a semi-active control matched for either experiential or didactic component content. The five remaining studies included a not-active control.
Moderating Effects of Control Group Type
For cortisol, two out of the six (33%) studies with full active controls, one out of the three studies (33%) that implemented a semi-active control, and one out of the three studies (33%) that implemented a non-active control demonstrated stress buffering effects on cortisol reactivity in the MI group. For cardiovascular outcomes, two out of the three studies (67%) that implemented a full-active control, and one out of three (33%) of studies that implemented a not-active control demonstrated stress buffering effects on cardiovascular reactivity. No studies including cardiovascular outcomes implemented a semi-active control. For self-reported stress reactivity, five out of the six studies (83%) that implemented a full-active control, neither study (0%) that implemented a semi-active control, and both studies (100%) that implemented a not-active control demonstrated stress buffering effects of MI on self-reported stress reactivity.
Mindfulness Protocols
Nine studies (60%) implemented an empirically validated, manualized MI protocol. Of these studies, four studies implemented mindfulness-based stress reduction (MBSR; Kabat-Zinn 1990). Three studies implemented one of the following: mindfulness-based cognitive therapy (MBCT; Segal et a., 2002), mindfulness-based relapse prevention (MBRP; Bowen et al. 2011), and Cognitively-Based Compassion Training (CBCT; Pace et al. 2009). Two additional studies (12%) used a manualized intervention that the authors of the studies developed, including Mindful Based Movement (MBM; Robert-McComb et al. 2015) and the ReSource Protocol (Engert et al. 2017). The remaining four studies implemented a variety of mindfulness practices (e.g., body scan, breath awareness).
Moderating Effects of Mindfulness Protocols
For cortisol, two out of the seven (29%) studies that implemented manualized interventions and one out of the five studies (20%) did not implement a manualized intervention demonstrated stress buffering effects on cortisol reactivity in the MI group. For cardiovascular outcomes, one out of the two studies (50%) that implemented a manualized intervention, and two out of four (50%) of studies that did not implement manualized interventions demonstrated stress buffering effects on cardiovascular reactivity. For self-reported stress reactivity, four out of the five studies (80%) that implemented a manualized intervention and three out of five studies (60%) that did not implement a manualized intervention demonstrated stress buffering effects of MI on self-reported stress reactivity.
Intervention Dosage
Intervention dosage varied across studies. The total number of MI sessions ranged from one to eight sessions. The average intervention time per session ranged from 5 min to 5 h and 25 min. Total intervention duration ranged from 1 day to 6 months.
Intervention session frequency was defined as the number of sessions contained within the MI protocol. MI frequency was reported in the number of sessions. The majority of studies (n = 11, 73%) implemented eight or more sessions, one study (7%) implemented six sessions, and three studies (20%) implemented interventions with three or fewer sessions. The session number was reported separately from additional retreats and home practice. Even greater variation existed among the inclusion of additional home practice or retreats, which account for further MI practice above and beyond the stated intervention session frequency. Out of the 15 studies, 13 studies (87%) included aspects of homework, and 4 studies (27%) included retreats, diminishing the clear operationalization of a “session.”
Intervention time per session was defined as the minutes and hours of each individual session. Two studies did not formally disclose the length of each MI session. For the studies that did report these details, the average length of a single MI session ranged from 5 min (Arch et al. 2014) to 5 h and 25 min (Kemeny et al. 2012). As previously discussed, the inclusion of homework and retreat sessions impacted the intervention time per session due to the additional inclusion of time spent in MI related activities.
Total intervention duration was defined as the length of time in days, weeks, or months that the sessions lasted for the entirety of the MI protocol. The duration ranged from 1 day (Cruess et al. 2015) to 6 months (Engert et al. 2017). Most of the studies (n = 8, 53%) took place over the course of 8 weeks. One study (7%) had multiple MI conditions, ranging from 3 to 6 months. Three studies (20%) lasted from 2 to 6 weeks, and three studies (20%) lasted less than a week.
Moderating Effects of Intervention Dosage
For cortisol, three out of the 11 studies (27%) that implemented interventions with six or more sessions demonstrated stress buffering effects on cortisol reactivity in the MI group. None of the studies that lasted three or fewer sessions demonstrated these effects; conversely, two out of the three studies (67%) with three or fewer sessions demonstrated effects in the unexpected direction. For cardiovascular outcomes, two out of four studies (50%) with eight or more sessions, and one out of two studies (50%) with three or fewer sessions demonstrated stress buffering effects on cardiovascular reactivity in the MI group. For self-report, four out of seven studies (57%) with six or more sessions, and two out of three studies (67%) with three or fewer sessions demonstrated stress buffering effects on self-reported stress reactivity in the MI group.
TSST Administrations
The number of the TSST administrations varied across studies from one to three administrations. Eight studies (53%) employed one TSST at post-intervention. Five studies (33%) implementing the TSST twice, once before the intervention, and once after. Two studies (13%) implemented three TSST sessions, one pre-intervention, one post-intervention, and one at a follow-up time point. Of the nine studies that used repeated (i.e., two or three) TSST administrations, six reported making modifications to subsequent administrations in order to reduce risk of sensitization or desensitization to the test.
Moderating Effects of TSST Administrations
The moderating characteristic in this section will consider whether studies used one TSST administration or multiple (i.e., two or three) administrations. For cortisol, two out of the eight studies (25%) that implemented one TSST, and one out of four studies (25%) that implemented multiple TSSTs demonstrated stress buffering effects on cortisol reactivity in the MI group. For cardiovascular outcomes, two out of the four studies (50%) that implemented one TSST, and one out of two studies (50%) that implemented multiple TSSTs demonstrated stress buffering effects on cardiovascular reactivity. For self-report, four out of the seven studies (57%) that implemented one TSST, and all three studies (100%) that implemented multiple TSSTs demonstrated stress buffering effects on self-reported stress reactivity.
Discussion
This review synthesizes and considers how MI may buffer laboratory induced stress reactivity via the TSST. The 15 studies in this review included one or more stress reactivity measures, including both physiological and self-report measures. The following section consolidates and interprets the findings in the result section to examine the effects of MI on the TSST. The majority of the studies in this review measured stress reactivity with multiple variables, and some of the results of this review are promising. However, despite some promising findings and previous meta-analytical findings demonstrating positive effects of MI on self-reported stress (Chiesa and Serretti 2009; Khoury et al. 2015), this review cannot unequivocally confirm both aspects of the mindfulness stress buffering hypothesis (i.e., top-down and bottom-up mechanisms of stress buffering) without further research.
Much of the promising stress-buffering findings in this review were demonstrated via self-reported stress reactivity, with seven of the 10 studies examining stress reactivity via self-report measures showing evidence that MI buffered stress reactivity. Psychological researchers have long understood and considered the limitations of subjective self-report measures (Furnham 1986), which is one of the reasons for moving toward obtaining more objective physiological evidence for the stress buffering effects of mindfulness. Regardless, these results still lend support to the top-down aspect of the mindfulness stress-buffering hypothesis (Creswell and Lindsay 2014), as they indicate that participants’ perceptions of stress were lower overall in the MI group when compared with those in the control group.
For the bottom-up aspect of the stress-buffering hypothesis (i.e., measured via physiological variables) results were more ambiguous. Twenty-five percent of cortisol findings, 33% of sAA, 50% cardiovascular measures, and 25% of studies examining inflammatory biomarkers (i.e., IL-6, IL-8, TNF-α) demonstrated stress-buffering effects of MI. These variations in effects may be due to the fact that neuroendocrine, cardiovascular, and inflammatory variables are measures of different underlying bodily systems, and thus, are differentially affected by mindfulness training. Additionally, the methodological variations across studies may be influencing the results.
The mixed results could have also indicated that the bottom-up stress-buffering effects of MI were more nuanced. For example, studies have shown that dispositional levels of mindfulness (Brown et al. 2012) and self-compassion (Luo et al. 2018) both influence stress reactivity to the TSST. Further exploration of such variables could potentially uncover interaction effects for the studies in this review. Additionally, three studies in this review that found no initial differences reported intervention effects emerged when taking into account the amount of practice time that participants reported (Kemeny et al. 2012; Pace et al. 2009; Rosenkranz et al. 2013), indicating that time engaged with the mindfulness practice may be a more predictive variable for buffering stress reactivity than solely completing a mindfulness program. In fact, a recent meta-analysis demonstrated small but significant effects of home practice on intervention outcomes for MI (Parsons et al. 2017). This may indicate that even a relatively limited amount of experience (e.g., an 8-week program) can contribute to physiological changes if participants fully engage with the material. Further standardization for collecting and reporting home practice time throughout MI may provide valuable information about the stress-buffering effects of mindfulness.
Implications of Unexpected Findings
Two studies in this review demonstrated effects in the unexpected direction for cortisol (i.e., MI groups either showed greater stress reactivity than control groups or they showed increased in stress reactivity from pre- to post-intervention). Upon further review of these results, several hypotheses to these unexpected directions could be made. Creswell et al. (2014) compared stress reactivity between an MI group and an attention training control group after a brief three-session (25 min per session) intervention, and the MI group showed greater cortisol reactivity compared to the control group post-intervention (although the MI group did evidence decreased self-reported stress reactivity). When researchers incorporated dispositional levels of mindfulness in the analyses, they demonstrated that participants with initially low levels of mindfulness who were in the MI group showed greater stress reactivity responses measured via cortisol (Creswell et al. 2014). This may indicate that brief mindfulness training may be better able to influence stress appraisals, but may not be enough time to see biological stress reactivity effects for individuals who do not start out with a higher dispositional level of mindfulness, and perhaps a more intensive or longer intervention (e.g., eight-week MBSR) may be more helpful. Additionally, the authors hypothesized that increases in stress reactivity after such a brief MI may have reflected greater effort in learning the practices at the beginning of a mindfulness intervention, an idea that has been echoed in recent literature (Tang et al. 2015).
Cruess et al. (2015) also demonstrated cortisol reactivity results in the unexpected direction with a brief intervention that included one 15–20-min session prior to employing the TSST. In this study, there were three groups: an enhanced mindfulness intervention group (i.e., the MI group), a somatic-relaxation control group, and an attention training control group. Interestingly for such a brief intervention, the authors decided to implement a mindfulness practice incorporating the ability to decenter from unpleasant thoughts, a practice that is traditionally taught in more advanced courses throughout a longer mindfulness intervention (e.g., session 5 out of 8 in MBSR). Additionally, authors showed decreased cortisol reactivity compared to the other groups for the somatic-relaxation intervention group, where participants were instructed to focus on different feelings in the body, which is similar to a mindfulness practice known as the body scan (Cruess et al. 2015). Therefore, the results of this study may have actually shown stress-buffering effects for brief mindfulness of the body practice, but not for a brief decentering of thoughts practice for participants that have no mindfulness experience.
It is notable that both of the unexpected results were in very brief mindfulness interventions, indicating that dosage may be an important factor in how MI may influence the stress response. A discussion on the variations in dosage and how this may act as a moderator for MI is discussed subsequently.
Methodological Variations
Across the studies included in this review, there was heterogeneity in many areas of the methodology, including population characteristics, control conditions, MI protocols, intervention dosage, and number of TSST administrations. Each of these variables were considered as potential moderators of stress reactivity results from studies that implemented cortisol, cardiovascular, and self-report measures.
Participants, Control Groups, and TSST Administrations
Two potential patterns emerged when considering population characteristics. Firstly, all three studies in clinical populations that implemented self-report measures demonstrated stress buffering effects, while 57% (i.e., four out of seven) demonstrated these effects in normative populations. This may be because clinical populations are already dealing with additional stressors related to their condition, and according to the mindfulness stress buffering account, higher-stress populations were likely to benefit from MI more so than less stressed populations (Creswell and Lindsay 2014). The second potential pattern emerged within the normative populations. Five studies that examined college student populations were compared with four studies in community populations. None of the studies in college populations demonstrated stress buffering results of MI via cortisol (in fact, the two studies demonstrated effects in the unexpected direction were in this group), while two of the four in community populations demonstrated stress buffering effects on cortisol. Related to the idea that more stressed participants benefit more from MI, perhaps community samples could be more stressed than college samples. Notably, one of the community samples was specifically with stressed adults (Lindsay et al. 2018). Another potential reason for these differences may be the nature of the TSST itself. College students may not have had a typical job interview experience yet, and thus, the TSST may not be as ecologically valid or as stressful in this population. For this reason, researchers have developed a measure more specifically for adolescents, in which the speaking task consists of pretending to introduce yourself to a new classroom (Yim et al. 2015). This could be more stressful for college populations as well, and group differences could emerge under greater stress.
Results across studies did not seem to vary as a function of the type of control condition implemented. This could indicate that when MI is effective, the effects are robust enough to see differences regardless of whether they are compared to a waitlist, semi-active, or full-active control. However, given the heterogeneity of control conditions in this review, and the general lack of attention to utilizing methodologically rigorous active control conditions in the mindfulness literature in general (Tang et al. 2015), it is possible that individuals in the control condition may have experienced adverse effects that obfuscate a clear interpretation of results obtained from mindfulness conditions.
Lastly, the use of repeated TSST administrations in this literature base may have been influential on the self-reported stress reactivity results. All three studies that examined self-reported stress reactivity to repeated TSST administrations demonstrated reduced stress reactivity, whereas four out of seven studies that implemented only one TSST demonstrated reduced stress reactivity via self-report. This may indicate that learning MI skills may be helpful for situation in which you have some idea of what to expect. Importantly, five out of the seven studies that used repeated TSST administrations took steps to modify the task (e.g., changing the speech topic) after the first administration to mitigate practice effects. However, Dickerson and Kemeny (2004) discuss that the aspects of the TSST that make it so effective at inducing a stress response are the social evaluation and the unpredictability. By using repeated administrations, even with some modifications, the unpredictability factor is arguably decreased.
Mindfulness Protocols, Active Ingredients, and Dosage
Broadly, differences in MI protocols did not seem to moderate the effectiveness of MI. There were no obvious differences between studies that implemented manualized interventions and studies that did not. There may be several reasons for this lack of difference. It appears that only two studies that implemented a manualized intervention discussed fidelity monitoring (Glasner-Edwards et al. 2017; Hoge et al. 2013), but they did not report results on intervention fidelity. There have been recent calls in MI research to increase fidelity monitoring and reporting in mindfulness research, and a tool has now been developed specifically for this field (Kechter et al. 2019).
Although only three studies implemented MI protocols that were very brief (three sessions or less), there were differences among these studies’ worth noting. As previously discussed, two of these studies demonstrated effects of MI in the unexpected direction. One of these studies implemented mindfulness practices consisting of decentering of thoughts compared to a somatic-relaxation control condition, which is similar to the mindfulness practice of a body scan. The somatic-relaxation demonstrated reduced cortisol reactivity when compared with the decentering of thoughts practice. The other study with unexpected effects implemented practices consisting of breath awareness, body awareness, and open awareness of emotions an thoughts (Cruess et al. 2015). The third brief intervention study demonstrated stress buffering effects of a self-compassion focused MI protocol on sAA reactivity, RSA reactivity, and self-reported reactivity (Arch et al. 2014). This may indicate that certain types of mindfulness practice (e.g., self-compassion or body scan practice) may be more conducive to producing stress buffering effects after only a short time, whereas other practices may produce effects in the unexpected direction, at least in the beginning phase. Further evidence for this idea is present within the large-scale study by Engert et al. (2017). The two 3-month MI conditions in this study demonstrated differential effects. The 3-month affective MI group (consisting of loving-kindness meditation and dyad meditations) demonstrated reduced cortisol reactivity, whereas the 3-month Presence MI group (consisting of attention and awareness meditations) did not demonstrate these effects. This may indicate a stress-buffering capability of feeling-cultivation practices like self-compassion or loving-kindness that is not present in other forms of contemplative practice.
Another study from this review that examined differential effects of different components of MI practice. Lindsay et al. (2018) evaluated differences between three groups: an open monitoring practice group, an open monitoring and acceptance practice group, and an attention control training group. They demonstrated that the acceptance component was crucial for influencing stress reactivity; cortisol and systolic blood pressure reactivity was significantly lower in the monitoring and acceptance training group when compared with that in the other two groups. This idea is elucidated in the recently developed Monitor and Acceptance Theory (MAT; Lindsay and Creswell 2017), in which authors discuss the importance of acceptance in addition to the attentional training components of mindfulness. Studies replicating methods that directly compare different ingredients of MI will allow researchers to understand which are the active ingredients that leading to stress buffering effects.
The intervention dosage ranged significantly across studies. All studies demonstrating decreases in cortisol reactivity implemented interventions with eight or more sessions. Conversely, studies with three or fewer sessions either demonstrated no effects on cortisol reactivity or increased cortisol reactivity when compared to controls. This lends evidence to the idea that it may initially take greater cognitive resources to learn to implement a mindfulness practice (at least for certain types of mindfulness practice), and stress-buffering benefits are more likely after practicing consistently for a period of time. Indeed, this idea is not novel has been discussed in recent research (Tang et al. 2015). However, there are still many questions related to dosage. In this review, one of the studies that demonstrated reduced cortisol reactivity implemented 15 sessions over just 2 weeks (Lindsay et al. 2018). Consequently, the number of sessions may be more important than the number of weeks. Additionally, three studies consisting of longer interventions initially demonstrated no effects on cortisol; however, when incorporating practice time they indicated that the increased practice led to stress-buffering effects (Kemeny et al. 2012; Pace et al. 2009; Rosenkranz et al. 2013). Perhaps the willingness to engage with the material outside of sessions is more important than how many weeks the intervention lasts.
For cardiovascular and self-reported stress reactivity, dosage did not seem to have a moderating effect in this sampling of studies. These results suggest that the evaluation of shorter interventions may benefit from cardiovascular and self-report variables as a means to better measure group differences. With more research examining interventions ranging from very brief sessions, to MI protocols lasting a few weeks, to standard eight-week protocols, and even to studies examining steady mindfulness practice for many years, researchers may be able to determine the possibility of a dosage-response effect of MI on stress reactivity.
Limitations, Future Research, and Recommendations
This review evaluated the mindfulness stress buffering effects of MI on stress reactivity via implementation of the TSST. One limitation of this systematic review was the relatively small pool of papers that were appropriate for the review. However, as research continues to emerge, a meta-analysis will be an appropriate avenue to continue this research inquiry. Another limitation is that this study only selected meditation naïve participants, and thus limited the potential of this review to understand the effects of long-term meditation training on stress reactivity. Future research may consider including studies that focused on more experienced meditators to elucidate how experienced meditators respond to acute stress. One limitation in the studies reviewed is that the existing body of research did not thoroughly account for expectancy or placebo effects. Future research in this domain should carefully consider how participants expectations for stress reduction may have influenced their psychophysiological output during the TSST.
Although there are promising results to be gleaned from this review, there are a host of potential avenues to strengthen the research in relation to MI and stress reactivity. Based on the findings of this review, recommendations for future MI and TSST research are as follows:
Increase Methodological Rigor
It is recommended that researchers employ a full-active control condition. This will allow researchers to examine how the MI differs from a full-active control condition that contains congruous elements such as time spent practicing, teacher availability, group participation, and other elements that are common in an intervention. Based on this review, there appeared to be no differences in the ability to see intervention effects whether studies employed a full-active control or a waitlist. For guidance, a well-matched active control to MBSR is found in MacCoon et al. (2012).
Report Aspects of MI Protocols in Detail
Fully discussing the components and implementation of each MI protocol is critical in pulling apart the different ingredients inherent in MI practice (e.g., breathing, attention) that may allow for increased understanding of the aspects that lead to intervention effects. The results from this review indicates that type of MI may influence stress reactivity, particularly when considered together with intervention length (dosage). It is also recommended to report time spent completing mindfulness home practice and the participant’s adherence to the recommended practice, since practice time was a significant moderating variable in several of the studies in this review.
Examine a Range of MI Dosages
Based on this review, longer interventions may be more effective at reducing neuroendocrine reactivity to acute stress, but this may also depend on the type of MI implemented. Conducting studies on a variety of different dosage levels with varied MI practices will allow us to better understand the role of dosage for each type of practice. Additionally, including long-term effects of MI practice will be valuable in adding to our understanding of the accumulation of practice on physiological outcome variables.
Incorporate Psychophysiological Variables
While research in psychophysiology entails greater demands both in resources and time compared with research using self-report, it is recommended to include psychophysiological variables as much as possible. The results of this review indicate that different physiological systems appear to respond to different doses of MI and physiology often shows different responses than MI. More research with neuroendocrine, cardiovascular, and inflammatory variables will allow us to characterize how MI affects each.
The ability of MI to buffer stress reactivity seems to be robust when measured via self-report, but stress buffering effects are less clear for physiological measures. There is evidence that variations in study methodology (i.e., variations in participant populations, MI protocols, intervention dosage, and number of TSST administrations) may influence stress reactivity outcomes. The type of mindfulness practice and the dosage of practice seem to be particularly influential for stress reactivity outcomes. Further research is necessary to more accurately characterize the relation between MI and stress reactivity, and to understand what aspects of MI may lead to stress buffering effects.
References
* denotes study included in systematic review
Allen, A. P., Kennedy, P. J., Dockray, S., Cryan, J. F., Dinan, T. G., & Clarke, G. (2016). The trier social stress test: principles and practice. Neurobiology of Stress, 6, 113–126. https://doi.org/10.1016/j.ynstr.2016.11.001.
*Arch, J. J., Brown, K. W., Dean, D. J., Landy, L. N., Brown, K., & Laudenslager, M. L. (2014). Self-compassion training modulates alpha-amylase, heart rate variability, and subjective responses to social evaluative threat in women. Psychoneuroendocrinology, 42, 49–58. https://doi.org/10.1016/j.psyneuen.2013.12.018.
*Basso, J. C., McHale, A., Ende, V., Oberlin, D. J., & Suzuki, W. A. (2019). Brief, daily meditation enhances attention, memory, mood, and emotional regulation in non-experienced meditators. Behavioural Brain Research, 356, 208–220. https://doi.org/10.1016/j.bbr.2018.08.023.
Bowen, S., Chawla, N., & Marlatt, G. A. (2011). Mindfulness-based relapse prevention for addictive behaviors: A clinician’s guide. Guilford Press.
*Britton, W. B., Shahar, B., Szepsenwol, O., & Jacobs, W. J. (2012). Mindfulness-based cognitive therapy improves emotional reactivity to social stress: results from a randomized controlled trial. Behavior Therapy, 43(2), 365–380. https://doi.org/10.1016/j.beth.2011.08.006.
Brown, K. W., Weinstein, N., & Creswell, J. D. (2012). Trait mindfulness modulates neuroendocrine and affective responses to social evaluative threat. Psychoneuroendocrinology, 37(12), 2037–2041. https://doi.org/10.1016/j.psyneuen.2012.04.003.
Brown, K. W., Creswell, J. D., & Ryan, R. M. (2015). Handbook of mindfulness: theory, research, and practice. New York, NY: Guilford.
Chiesa, A., & Serretti, A. (2009). Mindfulness-based stress reduction for stress management in healthy people: a review and meta-analysis. The Journal of Alternative and Complementary Medicine, 15(5), 593–600. https://doi.org/10.1089/acm.2008.0495.
Creswell, J. D., & Lindsay, E. K. (2014). How does mindfulness training affect health? A mindfulness stress buffering account. Current Directions in Psychological Science, 23(6), 401–407. https://doi.org/10.1177/0963721414547415.
*Creswell, J. D., Pacilio, L. E., Lindsay, E. K., & Brown, K. W. (2014). Brief mindfulness meditation training alters psychological and neuroendocrine responses to social evaluative stress. Psychoneuroendocrinology, 44, 1–12. https://doi.org/10.1016/j.psyneuen.2014.02.007.
*Cruess, D. G., Finitsis, D. J., Smith, A.-L., Goshe, B. M., Burnham, K., Burbridge, C., & O’Leary, K. (2015). Brief stress management reduces acute distress and buffers physiological response to a social stress test. International Journal of Stress Management, 22(3), 270–286. https://doi.org/10.1037/a0039130.
Davidson, R. J., & Kaszniak, A. W. (2015). Conceptual and methodological issues in research on mindfulness and meditation. The American Psychologist, 70(7), 581–592. https://doi.org/10.1037/a0039512.
Dickerson, S. S., & Kemeny, M. E. (2004). Acute stressors and cortisol responses: a theoretical integration and synthesis of laboratory research. Psychological Bulletin, 130(3), 355–391. https://doi.org/10.1037/0033-2909.130.3.355.
*Engert, V., Kok, B. E., Papassotiriou, I., Chrousos, G. P., & Singer, T. (2017). Specific reduction in cortisol stress reactivity after social but not attention-based mental training. Science Advances, 3(10), e1700495.
Everly, G. S., & Lating, J. M. (2013). A clinical guide to the treatment of the human stress response (3rd ed.). New York: Springer-Verlag.
Felver, J. C., Celis-de Hoyos, C. E., Tezanos, K., & Singh, N. N. (2016). A systematic review of mindfulness-based interventions for youth in school settings. Mindfulness, 7(1), 34–45. https://doi.org/10.1007/s12671-015-0389-4.
Furnham, A. (1986). Response bias, social desirability and dissimulation. Personality and Individual Differences, 7(3), 385–400. https://doi.org/10.1016/0191-8869(86)90014-0.
*Glasner-Edwards, S., Mooney, L. J., Ang, A., Garneau, H. C., Hartwell, E., Brecht, M.-L., & Rawson, R. A. (2017). Mindfulness based relapse prevention for stimulant dependent adults: a pilot randomized clinical trial. Mindfulness, 8(1), 126–135. https://doi.org/10.1007/s12671-016-0586-9.
*Hoge, E. A., Bui, E., Marques, L., Metcalf, C. A., Morris, L. K., Robinaugh, D. J., Worthington, J. J., Pollack, M. H., & Simon, N. M. (2013). Randomized controlled trial of mindfulness meditation for generalized anxiety disorder: effects on anxiety and stress reactivity. The Journal of Clinical Psychiatry, 74(8), 786–792. https://doi.org/10.4088/JCP.12m08083.
*Hoge, E. A., Bui, E., Palitz, S. A., Schwarz, N. R., Owens, M. E., Johnston, J. M., Pollack, M. H., & Simon, N. M. (2018). The effect of mindfulness meditation training on biological acute stress responses in generalized anxiety disorder. Psychiatry Research, 262, 328–332. https://doi.org/10.1016/j.psychres.2017.01.006.
Kabat-Zinn, J (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. Delacorte Press.
Juster, R.-P., McEwen, B. S., & Lupien, S. J. (2010). Allostatic load biomarkers of chronic stress and impact on health and cognition. Neuroscience and Biobehavioral Reviews, 35(1), 2–16. https://doi.org/10.1016/j.neubiorev.2009.10.002.
Kechter, A., Amaro, H., & Black, D. (2019). Reporting of treatment fidelity in mindfulness-based intervention trials: a review and new tool using NIH behavior change consortium guidelines. Mindfulness, 10(2), 215–233. https://doi.org/10.1007/s12671-018-0974-4.
*Kemeny, M. E., Foltz, C., Cavanagh, J. F., Cullen, M., Giese-Davis, J., Jennings, P., Rosenberg, E. L., Gillath, O., Shaver, P. R., Wallace, B. A., & Ekman, P. (2012). Contemplative/emotion training reduces negative emotional behavior and promotes prosocial responses. Emotion, 12(2), 338–350. https://doi.org/10.1037/a0026118.
Khoury, B., Sharma, M., Rush, S. E., & Fournier, C. (2015). Mindfulness-based stress reduction for healthy individuals: a meta-analysis. Journal of Psychosomatic Research, 78(6), 519–528. https://doi.org/10.1016/j.jpsychores.2015.03.009.
Kirschbaum, C., Pirke, K. M., & Hellhammer, D. H. (1993). The ‘trier social stress test’—a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology, 28(1–2), 76–81. https://doi.org/10.1159/000119004.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. Springer Publishing Company.
Linden, W., Earle, T. L., Gerin, W., & Christenfeld, N. (1997). Physiological stress reactivity and recovery: conceptual siblings separated at birth? Journal of Psychosomatic Research, 42(2), 117–135. https://doi.org/10.1016/S0022-3999(96)00240-1.
Lindsay, E. K., & Creswell, J. D. (2017). Mechanisms of mindfulness training: monitor and acceptance theory (MAT). Clinical Psychology Review, 51, 48–59. https://doi.org/10.1016/j.cpr.2016.10.011.
*Lindsay, E. K., Young, S., Smyth, J. M., Brown, K. W., & Creswell, J. D. (2018). Acceptance lowers stress reactivity: dismantling mindfulness training in a randomized controlled trial. Psychoneuroendocrinology, 87, 63–73. https://doi.org/10.1016/j.psyneuen.2017.09.015.
Luo, X., Qiao, L., & Che, X. (2018). Self-compassion modulates heart rate variability and negative affect to experimentally induced stress. Mindfulness, 9(5), 1522–1528. https://doi.org/10.1007/s12671-018-0900-9.
MacCoon, D. G., Imel, Z. E., Rosenkranz, M. A., Sheftel, J. G., Weng, H. Y., Sullivan, J. C., Bonus, K. A., Stoney, C. M., Salomons, T. V., Davidson, R. J., & Lutz, A. (2012). The validation of an active control intervention for mindfulness based stress reduction (MBSR). Behaviour Research and Therapy, 50(1), 3–12. https://doi.org/10.1016/j.brat.2011.10.011.
*Nyklíček, I., Mommersteeg, P. M., Van Beugen, S., Ramakers, C., & Van Boxtel, G. J. (2013). Mindfulness-based stress reduction and physiological activity during acute stress: a randomized controlled trial. Health Psychology, 32(10), 1110–1113. https://doi.org/10.1037/a0032200.
*Pace, T. W., Negi, L. T., Adame, D. D., Cole, S. P., Sivilli, T. I., Brown, T. D., Issa, M. J., & Raison, C. L. (2009). Effect of compassion meditation on neuroendocrine, innate immune and behavioral responses to psychosocial stress. Psychoneuroendocrinology, 34(1), 87–98. https://doi.org/10.1016/j.psyneuen.2008.08.011.
Parsons, C. E., Crane, C., Parsons, L. J., Fjorback, L. O., & Kuyken, W. (2017). Home practice in mindfulness-based cognitive therapy and mindfulness-based stress reduction: a systematic review and meta-analysis of participants’ mindfulness practice and its association with outcomes. Behaviour Research and Therapy, 95, 29–41. https://doi.org/10.1016/j.brat.2017.05.004.
*Robert-McComb, J. J., Cisneros, A., Tacón, A., Panike, R., Norman, R., Qian, X.-P., & McGlone, J. (2015). The effects of mindfulness-based movement on parameters of stress. International Journal of Yoga Therapy, 25(1), 79–88. https://doi.org/10.17761/1531-2054-25.1.79
*Rosenkranz, M. A., Davidson, R. J., Maccoon, D. G., Sheridan, J. F., Kalin, N. H., & Lutz, A. (2013). A comparison of mindfulness-based stress reduction and an active control in modulation of neurogenic inflammation. Brain, Behavior, and Immunity, 27(1), 174–184. https://doi.org/10.1016/j.bbi.2012.10.013.
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2002). Mindfulness-based cognitive therapy for depression: A new approach to preventing relapse. Guilford Press.
Schneiderman, N., Ironson, G., & Siegel, S. D. (2005). Stress and health: psychological, behavioral, and biological determinants. Annual Review of Clinical Psychology, 1, 607-628.
Tang, Y. Y., Hölzel, B. K., & Posner, M. I. (2015). The neuroscience of mindfulness meditation. Nature Reviews Neuroscience, 16(4), 213–225. https://doi.org/10.1038/nrn3916.
Yim, I. S., Quas, J. A., Rush, E. B., Granger, D. A., & Skoluda, N. (2015). Experimental manipulation of the trier social stress test-modified (TSST-M) to vary arousal across development. Psychoneuroendocrinology, 57, 61–71. https://doi.org/10.1016/j.psyneuen.2015.03.021.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Morton, M.L., Helminen, E.C. & Felver, J.C. A Systematic Review of Mindfulness Interventions on Psychophysiological Responses to Acute Stress. Mindfulness 11, 2039–2054 (2020). https://doi.org/10.1007/s12671-020-01386-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-020-01386-7