
Abstract
The inclusion of Buddhist mindfulness perspectives in second-generation mindfulness-based interventions (MBIs) offers an opportunity to explore the cultivation of ethical action in MBIs and address concerns about the purported absence of ethics in MBIs. This pilot study examined the relationship between mindfulness and value incongruence following a second-generation MBI, mindfulness-based symptom management (MBSM) that incorporates the Five Skillful Habits (5SH), a value-congruence practice. Sixty-one participants (65.6% female, Mage = 44.5; 34.4% male, Mage = 54.3) attended an 8-week program whose curriculum included the commitment to and practices of ethical and compassionate behaviors that reflected participants’ personal values. The impact of MBSM on mindfulness (Five-Factor Mindfulness Questionnaire (FFMQ)), congruence between ideal values and their lived experience of those values (Spiritual Well-Being Questionnaire (SWBQ)), and relationships between mindfulness and value incongruence were examined. Results indicated that increases in all of the FFMQ factors occurred: Observe (p < .001, d = .52), Describe (p < .01, d = .39), Act with Awareness (p < .001; d = .68), Non-judgment (p < 001, d = .67), and Non-reactivity (p <.001, d = .64). Value incongruence decreased on three of the four factors of the SWBQ: Personal (p < .001; d = − .64), Communal (p < .001; d = − .44), and Environmental (p < .01; d = − .40), with no significant changes occurring in Transcendental value incongruence (p > .10; d = − .21). Change scores for several factors of the FFMQ were significantly correlated with changes in the SWBQ measures. These preliminary results suggested that MBSM was related to shifts in value incongruence. Exploring the relationship between mindfulness and the practice of value-congruent behaviors may clarify the pathway between cultivating awareness and ethical/compassionate action.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
First-generation mindfulness-based interventions (FG-MBIs) such as mindfulness-based stress reduction (MBSR; Kabat-Zinn 2013) and mindfulness-based cognitive therapy (MBCT; Teasdale et al. 2000) have provided moderately effective approaches to treat psychological disorders (Van Dam et al. 2017). In the last 15 years, second-generation MBIs (SG-MBIs) have developed and are distinguished from FG-MBIs in a variety of ways, firstly, by their approach that can be psycho-spiritual in design; their use of a variety of secular meditations (Van Gordon 2017; Van Gordon et al. 2015) with a curriculum that includes Buddhist concepts such as the three poisons, the four immeasurables, compassion, attachment, and the five hindrances (Singh et al. 2013, 2014, 2018) and their explicit exploration of ethics or precepts (Cayoun 2011; Monteiro et al. 2010; Shonin et al. 2014a; Singh et al. 2014, 2018; Van Gordon et al. 2014). More recently, there has been a growing number of studies that investigate the effectiveness of SG-MBIs (Cayoun et al. 2017; Van Gordon 2017).
Conceptually, SG-MBIs focus on the cultivation of mindfulness as articulated in Buddhist traditions from which the secular application of mindfulness was derived: the transformation of the practitioner for their own betterment and that of others (Shonin and Van Gordon 2015; Shonin et al. 2014b; Van Gordon et al. 2015). In Buddhist traditions, the intent of the practice of mindfulness is the cultivation of discernment between wholesome and unwholesome actions through a trifold development of wisdom, ethical conduct, and meditation (Bodhi 2011, 2013). This capacity of discernment forms the base of the ethical arc of Buddhist mindfulness and its trajectory is the cultivation of a virtuous individual through ethical and compassionate thoughts, speech, and actions; a higher-order outcome is the betterment of the community or communities within which the individual lives and has relationships (Harvey 2013; Keown 2001). In Buddhist teachings of mindfulness practice, suffering is alleviated by uprooting the causes of suffering; the intention of a diligent uprooting of these causes is the cultivation of wisdom and compassion for self and others. That is, the core intention of mindfulness is to nurture the mind of love or bodhicitta by transforming unwholesome and unskillful inclinations to wholesome and skillful ones for the good of all beings (Gethin 1992/2001). Specifically, skillfulness in action, or upaya, requires an act to be rooted in wholesome intentions of kindness, generosity, and wisdom and whose outcomes (fruits of the act) are beneficial for others, i.e., not only for the actor (Harvey 2009).
Buddhist ethics are understood as a system of normative and applied ethics, and differ from a Western approach of philosophical theorizing of moral principles (Edelglass 2013). They are a practice of cultivating virtues (Gethin 2011, 2015) and a concomitant requirement in the development of mindfulness (Kabat-Zinn 2005). That is, the Buddhist concept of mindfulness incorporates contemplation of the principles of living ethically, with mindfulness or awareness, and practicing behaviors that are congruent with ethical principles. Both the intention and outcome of an enacted behavior determine whether it is skillful or unskillful (Harvey 2000). However, unless intentions are experienced as unwholesome and the outcome is also experienced as having done harm to others, there remains a risk of continuing to act from the unwholesome roots of anger, greed, and ignorance (see Bodhi 2012; Harvey 2009, for discussion of Anguttara Nikaya, The Tens, Sutta 217, verse 292–296). The translation of AN 217 suggests the awareness and experience of both the intention and its outcome is important in transforming unskillful actions. In fact, this connection of awareness and experiential process is nested in Kabat-Zinn’s secular definition of mindfulness which begins with “the awareness (italics added) that emerges” (2003). The practice of “paying attention, in the present moment, and nonjudgmentally” is therefore in the service of cultivating awareness of “the unfolding experience moment by moment.”
While the cultivation of Buddhist virtues may be an approach consistent with Buddhist definitions of mindfulness, there are complex issues surrounding the use of a Buddhist template of ethics in a Western culture (Lindahl 2015). Clarifying or working with self-chosen values, however, has been suggested as a more culture-consistent approach (Davis 2015) and has been studied among school teachers (Greenberg and Mitra 2015). Still, the concept of values is complex and represents both the process of attaining them, and the endpoints of that process. Values can be viewed as beliefs that motivate a trans-situational process to attain goals (Schwartz 1994). They have been connected to one’s internal moral compass and focus on ideals; however, they also tend to be conflated with attitudes (see Hitlin and Piliavin 2004 for a detailed review). Fitzpatrick et al. (2016) described values and their complex influence on actions concluding that clarification of values is an important direction for current research. They further proposed that values influence actions through a variety of paths: relevance, awareness through psychotherapy or life transitions, personality, and self-control. Congruence of values and behaviors is also related to well-being however, simply endorsing a value does not necessarily predict congruence with that value (Hitlin and Piliavin 2004). Thus, the cultivation of value-congruent behavior requires active participation in the process of value clarification, with goal setting as intermediary stage in the process. ACT (Hayes et al. 2006, 2011) and mindful self-compassion (MSC; Neff and Germer 2013) are two programs that include the practice of identifying and clarifying values in their curriculum. Neff and Germer (2013) described values as an important aspect of knowing how to meet one’s needs and, in turn, self-compassion as a means of sustaining that intention when efforts fall short. Implicit in their definition is the idea that well-being is related to an awareness of the incongruence between values as an aspiration and as lived experience with self-compassion fostering the capacity to face the pain of incongruity. Insofar as the (in)congruence in values is related to well-being (Sagiv and Schwartz 2000), it allows examination of the effectiveness of mindfulness as a cultivation of values and its relationship to wellbeing.
Several studies have explored the relationship between values and mindfulness. Christie et al. (2017) reported that the relationship between mindfulness and well-being was mediated by value-congruent actions. Shapiro et al. (2012) measured moral reasoning and ethical decision-making following an MBSR program and reported that improvements in the two measures were noted only at a 2-month follow-up. In their study, there was no specific practice of moral reasoning or ethical decision-making. Franquesa et al. (2017) compared meditation-naïve participants to meditators with different levels of practice frequency on measures of values and mindfulness. The daily meditators scored higher than the low-frequency groups on measures assessing value-related behaviors; specifically, the composite score that determined whether the participants were living congruently with their values was higher for the daily meditators. There were no diffferences among the low-frequency groups on value-related measures. Fewer studies that used values in a treatment program are available. Malouf et al. (2017) employed a value-based mindfulness group intervention with male jail inmates. Although they reported marginal reductions of recidivism, the relationship of personal values identification appeared to be a relational practice and was not assessed with respect to the outcomes reported. Lomas (2017) described mindfulness-based ethical living, a program in development that will use the 8-week framework of MBSR and will explore the five lay Buddhist precepts.
Although these various studies have examined the effects and relationships of mindfulness to values, there are few studies that have examined the relative shift in personal or relational values as a result of value-related practice in a mindfulness program. The current study examined the relationship between mindfulness and value incongruence following participation in mindfulness-based symptom management (MBSM), an SG-MBI. MBSM included the Five Skillful Habits (5SH), a secularized version of the five lay Buddhist precepts that are presented as ethical themes. Each week, participants choose an ethical theme within which they practiced behaviors relevant to their values and life situation. It was hypothesized that (1) the mindfulness (as measured by self-report questionnaire) would increase following treatment; (2) the participants’ lived experience of their values would increase and value incongruence, measured as the difference between ideal and lived experience of values, would decrease following treatment; and (3) the correlation between changes in mindfulness and value incongruence following treatment would be negative; that is, increases in mindfulness would accompany decreases in value incongruence.
Method
Participants
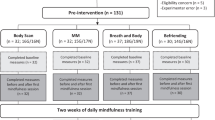
Participants were recruited from ongoing MBSM programs conducted over a 12-month period. Each program was co-facilitated by two healthcare professionals who had completed training in and were certified to teach MBSM; their teaching experience with the MBSM curriculum ranged from 2 to 5 years. Teachers with more experience were typically paired with those with fewer years of experience. All participants registered following an information session that described the program and the study. Of the 74 registrants, four (5%) registered but did not follow through. Of the 70 registrants who began the program, two (3%) declined to participate in the study (but completed the program). Five (7%) withdrew from the program between the first and fourth session, and one participant did not submit the post-program questionnaires. Sixty-two participants completed over 80% of the program and submitted pre- and post-treatment questionnaires although one participant was excluded because of extensive missing data leaving a total of 61. The data for this final cohort of 61 participants were assessed as described below.
Participants were comprised of 21 (34.4%) males and 40 (65.6%) females. Almost half of the participants (45.9%) had completed a degree or diploma program and 32.3% had completed post-graduate studies. The remaining were high school graduates (3.2%) or did not specify an education level (17.7%). The average age of female and male participants was 44.5 (range 25–69) and 54.3 (range 41–70) years, respectively.
Procedure
Mindfulness-Based Symptom Management
Mindfulness-based symptom management (MBSM; Monteiro and Musten 2013; Monteiro et al. 2010) is a program designed to address the reality that suffering is a normal human condition requiring the development of skillful means to enable a more satisfying life and a sense of personal and interpersonal wellbeing. The structure of and practices in the program were adapted from the FG-MBIs, mindfulness-based stress reduction, and mindfulness-based cognitive therapy; the curriculum content was based in Buddhist teachings of mindfulness as somatic awareness and a cultivation of skillful intentions and actions (Analayo 2003; Hanh 2009; Monteiro 2015; Monteiro and Musten 2017). The curriculum cultivates mindfulness through the platforms of body, emotions, sensations, and thoughts (BEST). The Five Skillful Habits, inspired by the Five Mindfulness Trainings taught by Thich Nhat Hanh (2007), form the framework of value-congruent living (5SH; Monteiro et al. 2010). Further, the development of MBSM is based on the view that meditation without an ethical framework is simply sustained attention. Mindfulness without setting the intention to act with compassion and in a way that does no harm is viewed as self-indulgence. In MBSM, a wise mindfulness practice has a moral arc of values that are cultivated through practice; skillfulness is developed by examining the divergence of lived experience from ideal principles (Monteiro and Musten 2017). This perspective integrates Buddhist views of mindfulness as a life-time practice and Western concepts of value cultivation as an increase of congruence between our principles and actions. Thus, MBSM holds the intention of examining the origins of suffering, learning how to be present to what is unfolding, and cultivating actions that are beneficial and congruent with living a skillful and value-based life. The program is delivered in a group format over eight weeks, for 2–2.5 h, and includes one all-day silent retreat mid-way through the program. Weekly home practice includes audio meditations available for download from the program’s website and specific personally chosen behaviors that are practiced in the framework of the Five Skillful Habits. Handouts were distributed at the end of each weekly session; they are standardized across the 8-week programs, describe what was covered in each week’s MBSM session, and list the formal and informal activities to be practiced between sessions. Table 1 outlines the curriculum of MBSM, BEST, and the 5SH practiced for each session. Table 2 provides descriptions and practice examples of each of the 5SH in the context of BEST. These practice examples of behaviors are from previous studies and, in the program, are not prompted by facilitators.
Previous exploratory studies have examined the impact of MBSM on various psychological variables. Nuttall (2009) used the Symptom Checklist (SCL-90-R; Derogatis 1994) to examine the effect of MBSM on the number of symptoms endorsed and the degree of distress associated with the symptoms. The results indicated gender differences and the data were presented separately by gender. Both genders reported reduced number of symptoms and lower distress about the symptoms. Daily functioning improved for both genders with lower impact of symptoms reported post-intervention. Shaw (2012) reported a reduction of emotional exhaustion which is a component of burnout measured by the Maslach Burnout Inventory (MBI; Maslach and Jackson 1981) after participation in MBSM along with increases in all six of the subscales of the Self-Compassion Scale (SCS; Neff 2003). Lee et al. (2016) investigated changes in how therapists experienced their work following an MBSM program, reporting that mindfulness was associated with important relational attitudes and skills of therapists. These included improved reflexive abilities and improvements in emotion regulation of therapists.
Measures
Mindfulness
Mindfulness was assessed using the 39-item Five-Factor Mindfulness Questionnaire (FFMQ; Baer et al. 2006). For this measure, the five subscales of the FFMQ, Observe, Describe, Act with Awareness, Non-judgmental, and Non-reactivity, have low or modest intercorrelations (.15 to .34). Act with Awareness, Non-judgmental, and Non-reactivity contribute incrementally to predicting psychological symptoms and all five factors are correlated in expected directions with psychological wellbeing. Internal consistencies range from .72 to .92 for all five factors (Baer et al. 2008). The FFMQ is widely used to assess the effects of mindfulness programs. While the FFMQ has been shown to be sensitive to changes following mindfulness interventions (Baer et al. 2012), Manuel et al. (2017) commented on issues related to the validity of the FFMQ, which may include its clinical utility and the heterogeneity of the population in the study. One key recommendation of Manuel et al. (2017) was “that the construct of mindfulness is most properly evaluated with the FFMQ in a healthy sample of highly educated individuals” likely because this would most closely correspond to the original sample used to validate the FFMQ.
Spiritual Well-being
Values were assessed using the Spiritual Well-Being Questionnaire (SWBQ; Fisher 2010), a 20-item questionnaire with four factors that reflect four domains of Personal, Communal, Environmental, and Transcendental values. Garssen et al. (2016) have noted that the SWBQ scale is composed of no more than 25% of spiritual and emotional well-being items thus making it less likely to create a tautology with respect to the measurement of spirituality and emotional wellbeing. The four factors reflect the interconnected relationship of self, others, environment, and a personal understanding of the divine/God, respectively. Fisher (2010) views these as values that are developed by the individual and are dependent on the congruence between “expressed and experienced meaning, purpose and values in life at the personal level (p. 107).” Each item is rated using a Likert scale ranging from 1 (very low) to 5 (very high). The items are rated twice: The first time to assess the importance of the item to the individual for an ideal state of spiritual well-being and the second time to assess the degree to which the individual feels the item reflects their actual lived experience. A difference score between the ideal and lived experience ratings is defined as spiritual incongruence experienced by the individual. Incongruence scores were determined for each of the four factors.
The advantage of Fisher’s SWBQ lies in the potential for comparing an individual’s position relative to their own assessment of their ideal spiritual well-being. The discrepancy between their appraisal of their ideal state and their lived experience provides a gauge of the feeling of internal imbalance. The dissonance between the ideal and lived experience measures of each of the factors (Personal, Communal, Environmental, and Transcendental) also provides a lens to the individual’s worldview.
Data Analyses
The following results are based on 61 cases with complete or almost complete data on the questionnaires of interest. One of these participants was missing responses to all of the items on the ideal and actual lived experience Transcendental subscales at both pre- and post-treatment. Hence, all analyses involving these subscale variables involve one fewer case. Any other missing item values (i.e., 5 and 46 in total on the FFMQ and SWBQ, respectively) were replaced by averaging the remaining items on the subscale that were responded to by the corresponding participant. For the SWBQ, ideal versus actual lived experience incongruence scores were derived for each of the four subscales at pre- and post-treatment by subtracting respondents’ lived experience scores from their ideal scores (i.e., ideal–lived experience). All post- versus pre-treatment difference scores were derived by subtracting the pre-treatment scores from the post-treatment scores (i.e., post-treatment–pre-treatment). All post- versus pre-treatment difference scores were examined for outlying differences more than 3 SDs from the mean difference. One outlier each was found for the FFMQ Observing, Non-judgmental, and Non-reactivity subscales and also for the SWBQ Communal and Environmental Ideal subscales. All of the following analyses involving such difference scores were run with and without those outliers present in order to ensure that any statistically significant results obtained did not depend on outlying values.
Three sets of statistical analyses were conducted. The first involved performing dependent sample t tests on the post- versus pre-treatment difference scores (i.e., the change scores) for each of the FFMQ and SWBQ subscale measures. The second involved computing and testing all of the bivariate correlations of the change scores for each of the FFMQ subscales with the corresponding changes in each of the SWBQ subscale measures. Third, in order to determine changes in which set of the five FFMQ subscales best predicted changes in SWBQ value incongruence, four stepwise regression analyses were run with changes in all five FFMQ subscales as the predictors and each of the four pre-value incongruence change measures, in turn, as the outcomes. For the first and second analyses, the Benjamini-Hochberg approach to controlling for false positives when performing a set of multiple hypothesis tests (Benjamini and Hochberg 1995) was employed in order to ensure an overall familywise type I error rate of .05. According to this approach, the resultant p values for each significance test were compared to p values that had been adjusted to account for all of the tests that were performed in each of those analyses.
Results
Treatment Effects
Means and SDs at pre-treatment, post-treatment, and their differences are reported in Table 3 for all of the study measures along with the results of the dependent sample t tests. As Table 3 indicates, significant post- versus pre-treatment increases occurred for all five FFMQ subscales. With respect to the SWBQ measures, significant post- versus pre-treatment changes occurred for the Transcendental ideal subscale (with the changes in the Environmental ideal subscale not actually being significant when comparing its p value to an adjusted Benjamini-Hochberg p value), for all of the actual lived experience subscales, and for all of the incongruence scores except the Transcendental scores. Unlike the other three SWBQ subscales, increases in Transcendental lived experience subscale scores from pre- to post-treatment were accompanied by corresponding increases in Transcendental ideal subscale scores. Note that omitting outlying cases and re-running these analyses did not quantitatively change the results of these tests. As well, a set of supplementary 2 (gender) × 2 (pre- vs. post-treatment) ANOVAs indicated that none of the subscales scores themselves nor any of the post- versus pre-treatment differences depended on gender given that no significant main effects or interactions involving gender were present in any of these analyses.
Correlational Analyses
Bivariate correlation results are provided in Table 4. All correlations in this table with p values below .019 are significant (at the nominal p < .05 level). As Table 4 indicates, changes in all five FFMQ subscales were significantly related to changes in both the Personal lived experience SWBQ subscale scores and the Personal value incongruence SWBQ measures (with the exception of FFMQ factor Describe and Personal value incongruence). Changes in all five FFMQ subscales were significantly related to changes in the Communal lived experience SWBQ subscale scores with changes in the Observe and Non-reactivity subscales also being significantly related to changes in the Communal value incongruence SWBQ measure. As well, changes in the FFMQ Observe, Act with Awareness, and Non-reactivity subscales were significantly related to changes in the Environmental lived experience SWBQ subscale scores with changes in the Observe and Non-reactivity subscales also being significantly related to changes in the Environmental value-incongruence SWBQ measure.
Regression Analyses
For the step-wise multiple regression analysis involving the Personal value-incongruence SWBQ measure, only the change in the FFMQ Non-reactivity subscale was retained as a predictor (β = − .581, p < .001, indicating that changes in the other four FFMQ subscales did not contribute uniquely to changes in this incongruence measure once changes in Non-reactivity had been accounted for). For the analysis involving the Communal value-incongruence SWBQ measure, changes in both the FFMQ Observe and Non-judgmental subscales were retained together as predictors (β = − .467, p < .001 and β = − .263, p < .020, respectively, indicating that changes in the Non-judgmental subscale was the second best unique predictor of changes in this incongruence measure after changes in the Observe subscale had been accounted for). For the analysis involving the Environmental value-incongruence SWBQ measure, only the change in the FFMQ Observe subscale was retained as a predictor (β = − .419, p < .001; indicating that changes in the other four FFMQ subscales did not contribute uniquely to changes in this incongruence measure once changes in Observe had been accounted for. Finally, for the analysis involving the Transcendental value-incongruence SWBQ measure, no predictors were retained.
Discussion
This study measured changes in mindfulness factors, ideal and lived values, and the value incongruence as measured by the difference between ideal and lived values. It also determined the predictive relationship between the mindfulness factors and value incongruence. As hypothesized, ratings on all five factors of mindfulness measured by the FFMQ increased following participation in the MBSM program. As well, ratings of participants’ actual lived experience of the values incorporated within the four SWBQ value domains increased following the MBSM program, whereas corresponding ratings of ideal values within each of these domains remained fairly stable from pre- to post-treatment (with the exception of ideal Transcendental values which increased). As a result, for Personal, Communal, and Environmental values, ideal versus lived experience value incongruence decreased following participation in the MBSM program. Importantly, these decreases in value incongruence were significantly related to increases in a number of factors of the FFMQ. Different mindfulness factors predicted Personal, Communal, and Environmental value incongruence. Non-reactivity best predicted decreased Personal value incongruence; Observe and Non-judgmental predicted a decrease in Communal value incongruence. Observe was a predictor of decreased Environmental value incongruence. None of the factors predicted changes in Transcendental value incongruence.
MBSM, an SG-MBI that incorporates value-awareness and the practice of value-congruent behaviors using the Five Skillful Habits (5SH), builds on the growing number of SG-MBIs that adopt a thematic approach that is different from the approach taken by FG-MBIs (Shonin and Van Gordon 2015; Singh et al. 2014; Van Gordon et al. 2015). The association of MBSM with increased levels of mindfulness adds to previous explorations of changes in various measures following the program (Lee et al. 2016; Nuttall 2009; Pérodeau et al. 2018; Shaw 2012); the positive changes and effect sizes are also consistent with most research findings of increases in mindfulness following participation in MBIs (Goyal et al. 2014; Khoury et al. 2013).
The second hypothesis of this study addressed the relationship of mindfulness and a shift in values following participation in MBSM and using the 5SH. The lived experience of Personal, Communal, Environmental, and Transcendental values as measured in this study changed in the expected direction as participants’ rating indicated increases in their valuing of a meaningful life and intra-relationship, love, forgiveness and trust in others, harmony with the environment, and peace and trust in a divine presence as they defined it for themselves. That the ideal ratings of the same values did not change is noteworthy and may be related to participants expressing high ideals thereby creating a ceiling effect. It would be of interest to determine how high standards, unrealistic personal expectations, and any disappointment in not living to those ideals play a role in personal distress. This would be of particular interest in light of the research showing the effectiveness of mindfulness and mindful self-compassion in addressing these issues (Neff and Dahm 2015).
The third hypothesis examined value incongruences in the domains of Personal, Communal, and Environmental and indicated incongruence decreased for each of these domains as anticipated. The practices of the 5SH comprised weekly behavioral commitments and the subsequent inquiries fostered a non-judgmental curiosity about the participants’ way of meeting their perceived success and failure. That is, while participants committed to a behavioral practice reflecting a valued way of living, they appeared to learn each week that the practice was not necessarily intended to achieve a fixed goal of wellbeing. Rather, the 5SH practices provided an opportunity to examine the consequences of intentional actions, their attention to the task, and their stance to or experience of the outcomes. In general, participants reported that a rigid stance tended to lead to stress and feelings of failure when the behaviors did not have traction; whereas, a curious stance allowed a freedom to explore sustainable ways to engage in the chosen behaviors. In turn, these shifts in self-judgment and reactivity lead to participants viewing their lived experience with more tolerance and acceptance. These findings are consistent with research studies that report the relationship of value incongruence with inter- and intra-well-being (Fisher and Brumley 2008; Fisher et al. 2002; Leiter et al. 2009ab; Sagiv and Schwartz 2000). Christie et al. (2017) described the link between mindfulness and well-being as moderated by values-based action, surmising that wellbeing was enhanced by mindfulness practices through behavioral change. Their conclusions add to the findings of Fitzpatrick et al. (2016), who indicated that value-congruent change involved both cognitive and behavioral factors.
Finally, the relationships between mindfulness and value incongruence suggested that decreases in reactivity and increases in somatic awareness best predict a decrease in value incongruence. Insofar as the items of the FFMQ factor of Non-reactivity reflect emotional regulation, it appeared to predict the incongruence between ideal and lived experience in the Personal domain (aspects of intra-relationship). It is possible that as participants developed stances of equanimity, they were able to be more tolerant of their feelings of guilt or disappointment in themselves. The role of emotional regulation is considered an important factor in models of mindfulness, fostering adaptive processes of reappraisal and reconsolidation (Holzel et al. 2011). Moreover, body or somatic awareness also plays an important role in the development of tolerance of internal distress.
The results from this study linked the mindfulness factors of Observe and Non-judgmental to decreased Communal value incongruence, that is, participants’ lived experience of trust in interpersonal relationships. The connection of the Observe factor and decreased Environmental value incongruence is consistent with the Observe factor’s direct assessment of attention to and awareness of the participants’ engagement with their physical environment. In the FFMQ, the elements of Non-judgmental reflect self-acceptance and those of Observe reflect awareness of body sensations. Holzel et al. (2011) suggested that internal body awareness, which is necessary for empathy (Decety and Jackson 2004), may lead to empathetic responses in relationships. In turn, empathetic relational responses may result in empathy with and a safeness in the presence of others (Gilbert 2005; Gilbert 2000). It is possible that self-acceptance along with direct practice with body sensations (sessions 3–5 of MBSM) resulted in participants being more accurate in interpreting their body sensations and a lowered reactivity to perceptions of threat in social situations. It is important to note that these results relate to a shift in values towards a greater congruence with ideal values. Whether participants themselves attribute a greater experiential sense of congruence to their ease in relationships would require further study.
Buddhist scholars and practitioners have expressed concern that without explicit cultivation of ethics, secularized mindfulness programs can result in a self-focused outcome or be a means of entrenching self-serving practices (Purser 2015; Titmuss 2013). These concerns are based on understanding Buddhist teachings of mindfulness as a discernment of wholesome from unwholesome actions that lead to more skillful approaches to self and others (Gethin 1998, 2015; Harvey 2000; Thanissaro 2012). That is, the practice of mindfulness has a moral arc that incorporates cognitive and behavioral practice.
Secular concepts of mindfulness propose that this cultivation of an ethical stance occurs implicitly through the practice of concentration and subsequent insight (Kabat-Zinn 2003, 2011; Williams and Kabat-Zinn 2013). However, as noted by Amaro (2015), presuming that the cultivation of ethical stances occurs implicitly may be risky. Further, Krageloh (2016) and Monteiro (2016) suggested ethics and morals are not absent in the process as the participants present with their own lived values, morals, and ethical frames. Including awareness of the participants’ values in the pedagogy of MBIs can be an invitation to cultivate wholesome behaviors through value clarification and ultimately, ethical decision-making. Studies have examined the impact of mindfulness on ethical decision-making (Leigh et al. 2005; Malouf et al. 2017; Shapiro et al. 2012; Small 2016) and Franquesa et al. (2017) examined the connection between meditation and an incongruence in values. The effect of mindfulness practice on the clarification of values or the shift in value incongruence can therefore offer an important insight into the interplay between mindfulness and ethics.
Limitations and Future Research Directions
Along with the findings of relationships between mindfulness factors and value incongruences, several factors must be considered that relate to the reliability of the outcomes. All measures were self-report leading to the possibility of correlation inflation due to shared method variance or the presence of response bias (although note that the present results deal with correlations between change scores). Participants typically self-select for participation in a community clinic and, with the increase in popularly available information on mindfulness, arrive with preconceived ideas of how meditation will help or what mindfulness means to them. Although engaging in an MBI program might clarify misperceptions and ambiguities, pre-existing assumptions about the ability of the program to effect change can be a strong demand characteristic that affects the outcomes through placebo or social desirability effects. This study did not include randomized controls as comparison groups for MBSM and the practice of the 5SH; thus, the results cannot confirm causality. All measures were self-report and the behavioral commitments to the themes of the 5SH were not objectively measured nor do they have external validation. However, recent work has provided some evidence that changes in the FFMQ subscales might not be strongly related to the extent of either formal or informal home mindfulness practice over the course of an eight-week MBI (Manuel et al. 2017). Further, the participants’ completion of their chosen behaviors may not have been the primary contribution to well-being as much as their understanding of their experience of practicing value-congruent behaviors. A qualitative investigation of the home practice of the 5SH may offer more information about the way the 5SH function to reduce value incongruence.
While mindfulness trainings offered by FG-MBIs and SG-MBIs result in moderate improvement to mental states, self-care, and connections with others, whether FG-MBIs and SG-MBIs are able to similarly elicit skillful means of preventing harm to oneself and others needs to be determined. Future directions in the study of the relationship between mindfulness training and values, their clarification, and shifts towards congruence are necessary to explore whether and how mindfulness practices can effect change in the ethical posture of individuals. As well, the inclusion of values and ethics in the pedagogy of MBIs can present an opportunity for including more qualitative approaches of understanding the contributors to change. The reliance on self-reports or reports by significant others that measure the frequency of behaviors may not capture the subtle changes, such as insight into and experience of the potential consequences of the participants’ choices. While actuarial measures may provide access to one form of change, including a qualitative approach may offer more insight to the relationship between intentionally acting on ones values and lower value incongruence. Further, because MBIs are predominantly process-oriented, actuarial measures of change may not capture the shifts that occur because of the experiential aspect of the programs. Finally, follow-up and longitudinal studies are required to determine whether the changes in clarifying or making values congruent are stable over time, including how they may evolve with ongoing practice.
References
Amaro, A. (2015). A holistic mindfulness. Mindfulness, 6(1), 63–73.
Analayo. (2003). Satipatthana: the direct path to realization. Birmingham: Windhorse Publications.
Baer, R., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13(1), 27–45.
Baer, R., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., et al. (2008). Construct validity of the Five Facet Mindfulness Questionnaire in meditating and nonmeditating samples. Assessment, 15(3), 329–342.
Baer, R., Carmody, J., & Hunsinger, M. (2012). Weekly change in mindfulness and perceived stress in a mindfulness-based stress reduction program. Journal of Clinical Psychology, 68(7), 755–765.
Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society, Series B (Methodological), 57, 289–300.
Bodhi, B. (2011). What does mindfulness really mean? A canonical perspective. Contemporary Buddhism, 12(1), 19–39.
Bodhi, B. (2012). The numerical discourses of the Buddha: a translation of the Anguttara Nikaya. Boston: Wisdom Publications.
Bodhi, B. (2013). Nourishing the roots: essays on Buddhist ethics. Access to Insight. Retrieved from Access to Insight http://www.accesstoinsight.org/lib/bodhi/wheel259.html.
Cayoun, B. A. (2011). Mindfulness-integrated CBT: principles and practice. Chicester: Wiley-Blackwell.
Cayoun, B. A., Simmons, A., & Shires, A. (2017). Immediate and lasting chronic pain reduction following a brief self-implemented mindfulness-based interoceptive exposure task: a pilot study. Mindfulness. https://doi.org/10.1007/s12671-017-0823-x.
Christie, A. M., Atkins, W. B., & Donald, J. N. (2017). The meaning and doing of mindfulness: the role of values in the link between mindfulness and well-being. Mindfulness, 8(2), 368–378.
Davis, J. H. (2015). Facing up to the question of ethics in mindfulness-based interventions. Mindfulness, 6(1), 46–48. https://doi.org/10.1007/s12671-014-0374-3.
Decety, J., & Jackson, P. L. (2004). The functional architecture of human empathy. Behavioral and Cognitive Neuroscience Reviews, 3, 71–100.
Derogatis, L. R. (1994). Symptom Checklist-90-R: administration, scoring, and procedure manual. Minneapolis: National Computer Systems, Inc..
Edelglass, W. (2013). Buddhist ethics and Western moral philosophy. In S. M. Emmanuel (Ed.), A companion to Buddhist philosophy (pp. 476–490). Chichester: Wiley.
Fisher, J. W. (2010). Development and application of a Spiritual Well-Being Questionnaire called SHALOM. Religions, 1, 105–112.
Fisher, J. W., & Brumley, D. (2008). Nurses’ and carers’ spiritual well being in the workplace. Australian Journal of Advanced Nursing, 25(4), 49–57.
Fisher, J. W., Francis, L. J., & Johnson, P. (2002). The personal and social correlates of spiritual well-being among primary school teachers. Pastoral Psychology, 51(1), 3–11. https://doi.org/10.1023/a:1019738223072.
Fitzpatrick, M., Henson, A., Grumet, R., Poolokasingham, G., Foa, C., Comeau, T., & Prendergast, C. (2016). Challenge, focus, inspiration and support: processes of values clarification and congruence. Journal of Contextual Behavioral Science, 5, 7–15.
Franquesa, A., Cebolla, A., Garcia-Campayo, J., Demarzo, M., Elices, M., Pascual, J. C., & Soler, J. (2017). Meditation practice is associated with a values-oriented life: the meditating role of decentering and mindfulness. Mindfulness, 8(5), 1259–1268. https://doi.org/10.1007/s12671-017-0702-5.
Garssen, B., Visser, A., & de Jager Meezenbroek, E. (2016). Examining whether spirituality predicts subjective well being: how to avoid tautology. Psychology of Religion and Spirituality, 8(2), 141–148.
Gethin, R. (1992/2001). The Buddhist path to awakening: a study of the bodhi-pakkhiya dhamma. Oxford: Oneworld.
Gethin, R. (1998). The foundations of Buddhism. Oxford: Oxford University Press.
Gethin, R. (2011). On some definitions of mindfulness. Contemporary Buddhism, 12(1), 263–279.
Gethin, R. (2015). Buddhist conceptualizations of mindfulness. In K. Brown, J. D. Creswell, & R. M. Ryan (Eds.), Handbook of mindfulness: theory, research, and practice (pp. 34–35). New York: The Guilford Press.
Gilbert, P. (2000). Social mentalities: internal “social” conflict and the role of inner warmth and compassion in cognitive therapy. In P. Gilbert & K. G. Bailey (Eds.), Genes on the couch: explorations in evolutionary psychotherapy (pp. 118–150). New York: Brunner-Routledge.
Gilbert, P. (2005). Compassion and cruelty: a biopsychosocial approach. In P. Gilbert (Ed.), Compassion: conceptualisations, research and use in psychotherapy (pp. 9–74). New York: Routledge.
Goyal, M., Singh, S., Sibinga, E. S., et al. (2014). Meditation programs for psychological stress and well-being: a systematic review and meta-analysis. JAMA Internal Medicine, 174(3), 357–368. https://doi.org/10.1001/jamainternmed.2013.13018.
Greenberg, M., & Mitra, J. (2015). From mindfulness to right mindfulness: the intersection of awareness and ethics. Mindfulness, 6(1), 74–78.
Hanh, T. N. (2007). For a future to be possible: Buddhist ethics for everyday life. Berkeley: Parallax Press.
Hanh, T. N. (2009). Breathe, you are alive! Sutra on the full awareness of breathing. Berkeley: Parallax Press.
Harvey, P. (2000). An introduction to Buddhist ethics. Cambridge: Cambridge University Press.
Harvey, P. (2009). Theravada texts on ethics. In W. Edelglass & J. L. Garfield (Eds.), Buddhist philosophy: essential readings (pp. 375–387). Oxford: Oxford University Press Inc..
Harvey, P. (2013). An introduction to Buddhism: Teachings, history and practices (2nd ed.). Cambridge: Cambridge University Press.
Hayes, S. C., Luoma, J. B., Bond, F. W., Masada, A., & Lillis, J. (2006). Acceptance and commitment therapy: model, processes, and outcomes. Behavior Research and Therapy, 44, 1–25.
Hayes, S. C., Strosahl, K., & Wilson, K. G. (2011). Acceptance and commitment therapy: the process and practice of mindful change (2nd ed.). New York: Guilford Press.
Hitlin, S., & Piliavin, J. A. (2004). Values: reviving a dormant concept. Annual Review of Sociology, 30, 359–393.
Holzel, B. K., Lazar, S. W., Gard, T., Schuman-Olivier, Z., Vago, D. R., & Ott, U. (2011). How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspectives on Psychological Science, 6(6), 537–559.
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: past, present and future. Clinical Psychology: Science and Practice, 10, 144–156.
Kabat-Zinn, J. (2005). Coming to our senses: healing ourselves and the world through mindfulness. New York: Hachette Books.
Kabat-Zinn, J. (2011). Some reflections on the origins of MBSR, skillful means, and the trouble with maps. Contemporary Buddhism, 12(1), 281–306.
Kabat-Zinn, J. (2013). Full catastrophe living: using the wisdom of your body and mind to face stress, pain, and illness. New York: Bantam.
Keown, D. (2001). The nature of Buddhist ethics. New York: Palgrave.
Khoury, B., Lecomte, T., Fortin, G., Masse, M., Therien, P., Bouchard, V., et al. (2013). Mindfulness-based therapy: a comprehensive meta-analysis. Clinical Psychology Review, 33, 763–771.
Krageloh, C. (2016). Importance of morality in mindfulness practice. Counseling and Values, 61, 97–110.
Lee, T., Paré, D., & Monteiro, L. M. (2016). Exploring the experiences of therapists after participating in an intensive mindfulness program. Journal of Counseling and Spirituality, 35(2), 11–36.
Leigh, J., Bowen, S., & Marlatt, A. (2005). Spirituality, mindfulness and substance abuse. Addictive Behaviors, 30, 1335–1341.
Leiter, M. P., Frank, E., & Matheson, T. (2009a). Values, demands, and burnout: perspectives from national survey of Canadian physicians. Paper presented at the American Psychological Association.
Leiter, M. P., Jackson, N. J., & Shaughnessy, K. (2009b). Contrasting burnout, turnover intention, control, value congruence and knowledge sharing between baby boomers and generation X. Journal of Nursing Management, 17(1), 100–109. https://doi.org/10.1111/j.1365-2834.2008.00884.x.
Lindahl, J. (2015). Why right mindfulness might not be right for mindfulness. Mindfulness, 6(1), 57–62. https://doi.org/10.1007/s12671-014-0380-5.
Lomas, T. (2017). Recontextualizing mindfulness: Theravada Buddhist perspectives on the ethical and spiritual dimensions of awareness. Psychology of Religion and Spirituality, 9(2), 209–219.
Malouf, E. T., Youman, K., Stuewig, J., Witt, E. A., & Tangney, J. P. (2017). A pilot RCT of a values-based mindfulness group intervention with jail inmates: evidence for reduction in post-release rick behavior. Mindfulness, 8, 603–614.
Manuel, J. A., Somohano, V. C., & Bowen, S. (2017). Mindfulness practice and its relationship to the five-facet mindfulness questionnaire. Mindfulness, 8, 361–367.
Maslach, C., & Jackson, S. (1981). The measurement of experienced burnout. Journal of Occupational Behavior, 2, 99–115.
Monteiro, L. M. (2015). Dharma and Distress: Buddhist teachings that support psychological principles in a mindfulness program. In E. Shonin, W. Van Gordon, & N. N. Singh (Eds.), Buddhist Foundations of Mindfulness (pp. 181–215). New York: Springer.
Monteiro, L. M. (2016). Implicit ethics and mindfulness: subtle assumptions that MBIs are values-neutral. International Journal of Psychotherapy, 20, 210–224.
Monteiro, L. M., & Musten, R. F. (2013). Mindfulness starts here: an 8-week guide to skillful living. Victoria: Friesen Press.
Monteiro, L. M., & Musten, F. (2017). Mindfulness-based symptom management: mindfulness as applied ethics. In L. Monteiro, J. Compson, & F. Musten (Eds.), Practitioner’s guide to ethics and mindfulness-based interventions. New York: Springer Publications.
Monteiro, L. M., Nuttall, S., & Musten, R. F. (2010). Five skillful habits: an ethics-based mindfulness intervention. Counselling and Spirituality, 29(1), 91–103.
Neff, K. D. (2003). The development and validation of a scale to measure self-compassion. Self and Identity, 2(3), 223–250.
Neff, K. D., & Dahm, K. A. (2015). Self-compassion: what it is, what it does, and how it related to mindfulness. In B. Ostafin, M. Robinson, & B. Meier (Eds.), Handbook of mindfulness and self-regulation. New York: Springer.
Neff, K. D., & Germer, C. K. (2013). A pilot study and randomized controlled trial of the mindful self-compassion program. Journal of Clinical Psychology, 69(1), 28–44.
Nuttall, S. (2009). Mindfulness-based symptom management: a naturalistic study of a new mindfulness-based intervention. Ottawa: (B.A.), University of Ottawa.
Pérodeau, G., Bossé, J., Devault, A., Loranger, C., Morel, C., Roy, M., & Monteiro, L. M. (2018). Les impacts de l’apprentissage de la pleine conscience pour des stagiaires en relation d’aide. In A. Devault & G. Pérodeau (Eds.), Pleine conscience et intervention. Théories et pratiques. Québec: Presses de l'Université Laval.
Purser, R. (2015). Clearing the muddles path of traditional and contemporary mindfulness: a response to Monteiro, Musten, and Compson. Mindfulness, 6(1), 23–45.
Sagiv, L., & Schwartz, S. H. (2000). Value priorities and subjective well-being: direct relations and congruity effects. European Journal of Social Psychology, 30, 177–198.
Schwartz, S. H. (1994). Are there universal aspects in the structure and contents of human values? Journal of Social Issues, 50(4), 19–45.
Shapiro, S. L., Jazaieri, H., & Goldin, P. R. (2012). Mindfulness-based stress reduction effects on moral reasoning and decision making. Journal of Positive Psychology, 7(6), 504–515.
Shaw, C. (2012). MIndfulness-based symptom management and the treatment of burnout. Ottawa: (M.A. Research), Carleton University.
Shonin, E., & Van Gordon, W. (2015). Manager’s experiences of meditation awareness training. Mindfulness, 6, 899–909.
Shonin, E., Van Gordon, W., Dunn, T. J., Singh, N. N., & Griffiths, M. D. (2014a). Meditation awareness training (MAT) for work-related wellbeing and job performance: a randomised controlled trial. International Journal of Mental Health Addiction, 12, 806–823.
Shonin, E., Van Gordon, W., & Griffiths, M. D. (2014b). The emerging role of Buddhism in clinical psychology: toward effective integration. Psychology of Religion and Spirituality, 6(2), 123–137.
Singh, N. N., Lancioni, G. E., Winton, A. S., Karazsia, B. T., & Singh, J. (2013). Mindfulness training for teachers changes the behavior of their preschool students. Research in Human Development, 10(3), 211–233.
Singh, N. N., Lancioni, G., Winton, A., Karazsia, B., Myers, R., Latham, L., & Singh, J. (2014). Mindfulness-based positive behavior support (MBPBS) for mothers of adolescents with autism spectrum disorder: effects on adolescents’ behavior and parental stress. Mindfulness, 5(6), 646–657.
Singh, N. N., Lancioni, G. E., Medvedev, O. N., Meyers, R. E., Chan, J., McPherson, C. L., et al. (2018). Comparative effectiveness of caregiving training in mindfulness-based positive behavior support (MBPBS) and positive behavior support (PBS) in a randomized controlled trail. Mindfulness. https://doi.org/10.1007/s12671-018-0895-2.
Small, C. (2016). Mindfulness, responsibility, ethical judgement and ethical intent: a virtue ethics perspective. Pretoria: (PhD), University of Pretoria.
Teasdale, J., Segal, Z. V., Williams, M., Ridgeway, V. A., Soulsby, J. M., & Lau, M. (2000). Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. Journal of Consulting and Clinical Psychology, 68, 615–623.
Thanissaro, B. (2012). Right mindfulness: memory and ardency on the Buddhist path. Valley Center: Metta Forest Monastery.
Titmuss, C. (2013). The Buddha of mindfulness. The politics of mindfulness. Retrieved from Insight Meditation website: www.christophertitmuss.org.
Van Dam, N. T., van Vugt, M. K., Vago, D. R., Schmalz, L., Saron, C. D., Olendzki, A., et al. (2017). Mind the hype: a critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspectives on Psychological Science, 13(1), 36–61.
Van Gordon, W. (2017). Exploring the applications of second-generation mindfulness-based interventions for improving health and human functioning: a mixed-methods investigation. Nottingham: (PhD), Nottingham Trent University.
Van Gordon, W., Shonin, E., Sumich, A., Sundlin, E. C., & Griffiths, M. D. (2014). Meditation awareness training (MAT) for psychological well-being in a sub-clinical sample of university students: a controlled pilot study. Mindfulness, 5, 381–391.
Van Gordon, W., Shonin, E., & Griffiths, M. (2015). Towards a second generation of mindfulness-based interventions. Australian & New Zealand Joyrnal of Psychiatry, 49(7), 591–592. https://doi.org/10.1177/0004867415577437.
Williams, J. M., & Kabat-Zinn, J. (2013). Mindfulness: diverse perspectives on its meaning, origins and applications. New York: Routledge.
Acknowledgments
The authors thank all the participants of the study and the program teachers who collected the questionnaires. We thank Ms. Shira Blake for preparing the data for analysis and Ms. Jen Soto for copy editing the manuscript.
Author information
Authors and Affiliations
Contributions
LMM and FM designed the study and collaborated in the writing of all drafts. CLS conducted the data analyses, wrote all drafts of the data analyses and results sections, and contributed to the overall final draft.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Monteiro, L.M., Musten, F. & Leth-Steensen, C. Effect of Mindfulness on Value Incongruence: a Pilot Study. Mindfulness 10, 1031–1043 (2019). https://doi.org/10.1007/s12671-018-1044-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-018-1044-7