
Abstract
Our purpose was to examine the relationship of mindfulness with weight status, physical activity, screen time, diet (fruit, vegetable, and junk food intake), and health-related quality of life in children living in a low-socioeconomic status community. Children (N = 754; 8–13 years) completed surveys, and height and weight were measured. Regression analysis evaluated the relationship of mindfulness with weight status (body mass index percentile), physical activity, screen time, diet, health-related quality of life, and dummy-coded moderator race, grade, and sex. Average mindfulness was 23.4 ± 9.5 and was higher in black children (24.4 ± 9.3) vs. multi-racial/other children (22.1 ± 9.7), boys (24.2 ± 9.2) vs. girls (22.6 ± 9.8), and in sixth (25.1 ± 9.4) vs. fifth (23.0 ± 9.2) or fourth (21.9 ± 9.8) graders. Overall, the model was significant (adjusted R 2 = 0.201, P < .001). Grade level (fourth grade, β = −0.163, P = .002 and fifth grade, β = −0.144, P = .007), junk food intake (β = −0.160, P = .001), and parent- and autonomy-related (β = −0.136, P = .017) and psychological quality of life (β = 0.416, P < .001) were associated with mindfulness. Psychological and parent- and autonomy-related quality of life and junk food intake accounted for a small percentage of variance in mindfulness, with parent-related quality of life contributing in the unexpected direction. Mindfulness may have benefits not captured in this study, but more research is needed on its relationship with health variables.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
According to the United States Census Bureau, 41.6% of Flint, MI residents live in poverty compared to 16.2% of residents statewide (United States Census Bureau 2015a, b). Children living in low socioeconomic environments report poorer diet, characterized by lower fruit and vegetable intake and greater junk food intake, than those living in higher socioeconomic status environments (Darmon and Drewnowski 2008; Rasmussen et al. 2006). These children also participate in less physical activity and more screen time (Drenowatz et al. 2010; Hanson and Chen 2007; Tandon et al. 2012). Together, these unfavorable health behaviors partially explain why children living in low socioeconomic environments are more likely to be overweight or obese compared to children of higher socioeconomic status (Ogden et al. 2010; Wang and Lim 2012; Zhang 2006). Children living in low-socioeconomic status environments are also exposed to high amounts of stress, which can result in stimulation of the sympathetic nervous system and other adverse endocrine responses (Bradley and Corwyn 2002; Chen et al. 2002; Lupien et al. 2001). Further, children living in low-socioeconomic status environments report lower health-related quality of life (Von Rueden et al. 2006). In sum, these factors create a negative health environment in which children who already face much adversity are at an increased risk for myriad negative health outcomes.
Despite the increased risk for negative health outcomes, Chen and Miller (2012) described how some children living in low socioeconomic environments develop a “shift-and-persist” attitude in which they find ways to regulate their emotions, maintain optimism, lessen their risk for unfavorable health outcomes, and thrive in spite of adversity. The authors noted the need to identify practices that promote resilience and develop this shift-and-persist mindset, but require few resources (e.g., time, money) (Chen and Miller 2012). Mindfulness, defined as paying attention on purpose, being aware of the moment, and accepting one’s feelings and thoughts, has been recognized as a feasible method for promoting resilience in school children and identified as a low-cost intervention tool for treating chronic pain and aggression in adults (Kabat-Zinn 1982, 1994; Meiklejohn et al. 2012; Mendelson et al. 2010; Singh et al. 2008; Van der Gucht et al. 2015). In youth, mindfulness during everyday life, as well as mindfulness meditation or mindfulness-based stress reduction, has been related to lower stress levels and greater feelings of calmness, self-acceptance, and improved behavior (Bluth et al. 2016; Broderick and Metz 2009; Van de Weijer-Bergsma et al. 2014). These findings have been supported in both minority and urban youth (Liehr and Diaz 2010; Mendelson et al. 2010; Sibinga et al. 2016).
In recent years, researchers, educators, clinicians, and laypeople have become increasingly interested in mindfulness and its potential benefits (Burke 2010). More mindful children have greater academic competence, overall quality of life, self-esteem, happiness, and resiliency, while exhibiting less externalizing behaviors, depression, impulsivity, cognitive inflexibility, and anxiety (Greco et al. 2011; Renshaw and O’Malley 2014; Tan and Martin 2012). In adults, mindfulness has been related to health-related outcomes, like physical activity, diet, weight status, and health-related quality of life (Gilbert and Waltz 2010; Moor et al. 2013; Roberts and Danoff-Burg 2010). However, there are a few studies that have found no relationship between mindfulness and health-related outcomes (Grinnell et al. 2011; Moor et al. 2013). Conceptually, it is understandable that mindfulness may be related to health outcomes. A person who is intentionally aware of thoughts and emotions as they arise may act less impulsively and be able to self-regulate negative thoughts and feelings, which could have positive effects on dietary and physical activity behaviors (Renshaw and O’Malley 2014). Researchers have also demonstrated that more mindful adults are better able to discern the duration of various tasks compared to less mindful adults, so more mindful individuals may be more aware of the length of time they have been participating in screen time (Wittmann et al. 2014). If results from adult studies can be generalized to children, the acceptance of one’s thoughts and feelings should improve health-related quality of life in multiple domains, including at school, and in peer or parent relationships. Positive health behaviors, like more physical activity, less screen time, healthy diet, and improved quality of life could then be associated with more favorable weight status, a relationship that has been supported in adults (Camilleri et al. 2015).
While previous studies, namely in college-aged samples, have demonstrated promising relationships between mindfulness and health behaviors, there are some conflicting findings in the literature and similar research has not been performed with children. If mindfulness is related to health outcomes, promotion of mindfulness could provide a low-cost intervention in at-risk or low-socioeconomic status populations. Therefore, the purpose of this study was to examine the relationship of mindfulness with weight status, physical activity, screen time, diet, and health-related quality of life in children living in a low-socioeconomic status community. We hypothesized that mindfulness would be positively related to physical activity, fruit intake, vegetable intake, and all health-related to quality of life subscales, but inversely related to junk food intake, body mass index (BMI) percentile, and screen time.
Method
Participants
Children fourth to sixth grade (N = 754) in nine participating schools in Flint, MI in the Fall of 2014 (Table 1) completed surveys for this study. As an indicator of socioeconomic status, the percentage of children in fourth to sixth grade at these schools receiving free or reduced lunch was obtained for the 2014–2015 school year (Michigan Department of Education 2015). We did not have access to individual free or reduced lunch status. This study was conducted as part of an existing project (Crim Fitness Foundation programming) and as such, was approved as program evaluation by the Institutional Review Board approval.
Procedure
All measurements were completed by trained undergraduate and graduate students in the Fall of 2014 at the children’s schools. In a private location, height and weight were measured. In their regular classroom, children completed the following surveys: Child and Adolescent Mindfulness Measure (Greco et al. 2011), Physical Activity Questionnaire for Children (Crocker et al. 1997), School Physical Activity and Nutrition Survey (Hoelscher et al. 2003), and the KidsScreen-27 (Ravens-Sieberer et al. 2014) read out loud by the research staff and teachers. Children self-reported their age, sex, grade, and race.
Measures
Height was measured to the nearest 0.1 cm by a portable stadiometer (Shorr Board, Olney, MD) and weight was measured to the nearest 0.1 kg by a digital scale (Seca 770, Hanover, MD). BMI (kg/m2) was used to classify subjects as healthy weight (<85th percentile) or overweight (≥85th percentile) according to age- and sex-specific growth charts available from the Centers for Disease Control (CDC) (Kuczmarski et al. 2000).
Mindfulness
The Child and Adolescent Mindfulness Measure has been validated in children and adolescents aged 10–17 years and includes ten reverse-coded items, with a maximum score of 40 points, and a higher score indicating the participant is more mindful (Greco et al. 2011). Participants rated their responses from 0 (never true) to 4 (always true). While we included a definition of mindfulness prior to the survey questions, none of the questions requires the participant to know or understand the definition. Although it has been deemed unidimensional, the survey encompasses three facets of mindfulness: (1) observing (noticing internal phenomena), (2) acting with awareness (present moment awareness), and (3) accepting without judgment (non-judgmental awareness). Example items are “I push away thoughts that I don’t like” and “I get upset with myself for having certain thoughts.” The convergent validity of this measure has been demonstrated by correlating it with other constructs known to be related to mindfulness, including being positively related to quality of life, social skills, and academic competence and inversely related to somatic complaints, internalizing symptoms, externalizing behavior, thought suppression, and psychological inflexibility (Greco et al. 2011). Internal consistency (reliability) of this survey has been demonstrated, with a Cronbach’s alpha of 0.80, 0.84, and 0.87 in three studies (Bluth and Blanton 2014; Greco et al. 2011; Kuby et al. 2015). In the current study, Cronbach’s alpha was 0.80.
Physical Activity and Screen Time
The Physical Activity Questionnaire for Children (PAQ-C) includes nine items, with a maximum score of five points, and a higher score was indicative of a higher habitual physical activity level (Crocker et al. 1997). This survey has been validated against other recall methods, monitors, and interviews (Kowalski et al. 1997). Test-retest reliability after 1 week was adequate in males (r = 0.75) and females (r = 0.82) (Crocker et al. 1997). In the current study, Cronbach’s alpha was 0.71.
Participants also self-reported their typical screen time (hours) on an average weekday and weekend day. Then, average daily screen time was calculated as a weighted average of weekday screen time (multiplied by five) and weekend screen time (multiplied by two), divided by seven (Montoye et al. 2013).
Dietary Variables
The School Physical Activity and Nutrition Survey included 25 items with a maximum score of 3 points each and a higher score indicating greater intake for that item (Hoelscher et al. 2003). Single items described vegetable and fruit intake, and a junk food intake was calculated based on six items, with an overall maximum possible score of 18 points (Montoye et al. 2013). In previous research by Penkilo et al. (2008), the test-retest reliability of self-reported food intake ranged from r = 0.66 to r = 0.97, with fruits and vegetables attaining r = 0.79 and r = 0.73, respectively. Correlation between 24-h recall and reported intake via this survey revealed correlations from r = 0.32 to 0.68, with fruit and vegetables attaining r = 0.53 and r = 0.57, respectively (Hoelscher et al. 2003).
Health-related Quality of Life
The Kidscreen-27 included 27 items across four quality of life dimensions, including psychological well-being, autonomy and parent relations, social support and peers, and school environment (Ravens-Sieberer et al. 2014). Similar to Dey et al. (2013), scores were standardized to a maximum of 100 points for each subscale with higher scores being favorable and indicating greater perceived quality of life. The reliability of this measure has been demonstrated, with Cronbach’s alpha > 0.70 across each of the subscales (Ravens-Sieberer et al. 2014). In the current study, Cronbach’s alpha varied from 0.68 (psychological well-being) to 0.82 (peer support).
Data Analyses
One-way ANOVA, with Tukey’s post hoc tests when applicable, was used to determine differences in mindfulness by grade, sex, weight status, and race. Regression analysis was used to evaluate the relationship of mindfulness with weight status (BMI percentile), physical activity, screen time, diet, health-related quality of life, and dummy-coded moderator race (reference black), grade (reference sixth grade), and sex (reference male), with significance at P < .05. The assumptions of normality (histograms and Q-Q plots of all variables), presence of linear relationships between mindfulness and the independent variables (scatter plots), lack of multi-collinearity (correlations and variance inflation factor), and homoscedasticity (scatter plot of residuals) were verified.
Results
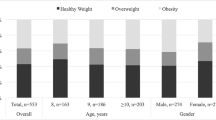
A description of the sample (N = 754) is outlined in Table 1. The sample was predominantly male (53.0%), black (56.2%), and healthy weight (56.0%). On average, schools in this sample offered free or reduced lunch to 85.5 ± 10.3% of fourth to sixth grade students during the 2014–2015 school year, with a range of 60.0 to 100.0% (Michigan Department of Education 2015).
Average mindfulness was 23.4 ± 9.5 and was higher in black children (24.4 ± 9.3) vs. multi-racial/other children (22.1 ± 9.7), boys (24.2 ± 9.2) vs. girls (22.6 ± 9.8), and in sixth (25.1 ± 9.4) vs. fifth (23.0 ± 9.2) or fourth (21.9 ± 9.8) graders. Descriptive statistics for the independent variables are provided in Table 2. Results of the regression analysis are outlined in Table 3. Overall, the model was significant (adjusted R 2 = 0.201, P < .001). Being in fourth grade (β = −0.163, P = .002) or fifth grade (β = −0.144, P = .007) compared to sixth grade, junk food intake (β = −0.160, P = .001) and parent- and autonomy-related (β = −0.136, P = .017) and psychological quality of life (β = 0.416, P < .001) were associated with mindfulness. All reported coefficients are standardized and thus can be interpreted as the change in mindfulness for every one standard deviation increase in the independent variable after controlling for all other independent variables.
Discussion
The purpose of this study was to determine if mindfulness was related to personal characteristics (i.e., sex, grade, race, weight status), health behaviors, or health-related quality of life. Our main finding was that mindfulness was positively related to psychological quality of life, but inversely related to parent- and autonomy-related quality of life, junk food intake, and being in fourth or fifth grade compared to sixth grade. Thus, our hypotheses were not confirmed as many health outcomes were not related to mindfulness (weight status, physical activity, screen time, vegetable or fruit intake, peer-related and school-related quality of life), and one was related in an unexpected direction (parent- and autonomy-related quality of life).
Physical Activity, Screen Time, and Weight Status
In contrast to our null findings, mindfulness has been positively related with physical activity in college-aged samples (Roberts and Danoff-Burg 2010). It may be that this relationship is age-specific or different in those living in low-socioeconomic status environments. In adults, exercise is typically a choice and being more accepting of one’s thoughts would allow one to begin or continue exercise even when uncomfortable. For example, a mindful adult who thinks “I don’t want to do this anymore,” would then recognize that feeling, but understand that thinking that way does not mean she or he should quit exercising; one can simply accept it as a thought and let it pass. However, children do not participate in exercise in the traditional sense (e.g., continuous bout, for health benefits), but rather, more sporadic activity, physical education class, or team-based sports, so the relationship with mindfulness may not exist. Further, this relationship may be mediated by other variables, such as the relationship with stress in college-aged samples (Roberts and Danoff-Burg 2010). Overall, our study did not support the relationship between physical activity and mindfulness found in previous studies of adult samples.
However, other studies support our findings. Grinnell et al. (2011) reported no relationship between mindfulness and physical activity and Moor et al. (2013) found that mindful eating, specifically, and physical activity were not related in college samples. It is possible that our study and other studies found no relationship because particular aspects of mindfulness are related to physical activity, and they were not captured in this study. For example, a study of college students demonstrated very weak correlations between specific mindfulness subscales and physical activity, with differences by sex (Gilbert and Waltz 2010). The “observe” mindfulness subscale was related to moderate and vigorous physical activity in males (R 2 = 0.07 and 0.05), but the “describe” subscale was predictive of moderate physical activity in females (R 2 = 0.03) and the “act with awareness” subscale was predictive of vigorous physical activity for females (R 2 = 0.03), although the correlation coefficients were all very low (Gilbert and Waltz 2010). More research is needed that uses a facet-level mindfulness scale as physical activity may be related to specific aspects of mindfulness, but not other.
We also reported no relationship between mindfulness and average daily screen time. While this has not been studied previously, previous research has supported that more mindful adults are better able to perceive time than less mindful adults (Wittmann et al. 2014). However, it has been suggested that a person can be mindful in one area (e.g., mindful eating), but not in another. So, it may be that screen time and mindfulness during screen time activities, but not overall mindfulness, are related. For example, the Child and Adolescent Mindfulness Measure asks children to respond to the statement “At school, I walk from class to class without noticing what I’m doing,” but a more specific question for screen time may be “While I’m watching television, I lose track of how many episodes I watch.” Therefore, generic scales like the one used in this study do not account for this possibility (Hulbert-Williams et al. 2014). Finally, while surveys provide useful context about the type of sedentary behavior in which children participate, their validity has been called in to question, so recall bias could mask the relationship between variables (Lubans et al. 2011). Definitive conclusions regarding the relationship between screen time and mindfulness cannot be made at this time.
In the current study, mindfulness was not related to weight status, as determined by BMI. This is in contrast to a prior study in a large sample of adults (N = 63,628) that found an inverse relationship between weight status and mindfulness (Camilleri et al. 2015). The null relationship in the current study is not surprising since important correlates of weight status, including physical activity, screen time, and fruit and vegetable intake, were also unrelated to mindfulness (Maples et al. 2012). While mindfulness may have health benefits not measured in our study, our results indicate that mindfulness may not be a pertinent point of intervention in the fight against childhood obesity.
Dietary Variables
Most prior research on the relationship between mindfulness and dietary variables has been conducted in college-aged students. In contrast to our findings, mindfulness has been positively related to daily vegetable and fruit intake (Gilbert and Waltz 2010; Roberts and Danoff-Burg 2010). But, similar to our study, mindfulness has also been found to be unrelated in college-aged samples (Grinnell et al. 2011). While Gilbert and Waltz (2010) reported significant relationships between specific subscales of mindfulness with vegetable or fruit intake, the relationships were weak (R 2 = 0.05). In contrast to our hypothesis, we found that mindfulness was unrelated to both vegetable and fruit intake. It is possible that these children, or their families in charge of purchasing food, have little choice in food and are simply surrounded by insufficient fruits and vegetables (Beaulac et al. 2009; United States Department of Agriculture 2016). For example, in Genesee County (Flint, MI is the county seat), 29.9% of residents have low access to a grocery store (United States Department of Agriculture 2015). Alternatively, these disparate findings could be an age-related difference. Adults have more autonomy over their food choices than children, so the relationships between dietary variables and mindfulness may be more apparent. Lastly, these differences could be due to the difficulty children have with dietary recall.
Our hypothesis of an inverse relationship between mindfulness and junk food intake was supported. While we found no studies that have focused on the relationship between junk food intake and mindfulness, other dietary variables have been related to mindfulness. For example, mindfulness has been inversely related to binge eating in college-aged samples (Gilbert and Waltz 2010; Roberts and Danoff-Burg 2010). Researchers attribute the inverse relationship between mindfulness and unfavorable eating habits to the regulation of the emotional component of eating (Hulbert-Williams et al. 2014). As such, those who are more mindful better regulate their emotions and thus, are less susceptible to negative eating habits. More research to confirm the relationship between mindfulness and junk food intake is justified, but again, should account for specific aspects of mindfulness and not rely on an overall mindfulness score.
Health-related Quality of Life
Previous research has demonstrated that mindfulness was positively related to overall quality of life in fifth and tenth graders (Greco et al. 2011). Our study investigated four specific health-related quality of life domains and found that mindfulness was positively related to psychological quality of life, inversely related to parent- and autonomy-related quality of life, and unrelated to peer-related and school-related quality of life. The strongest association with mindfulness in the current study was psychological quality of life. Numerous studies have demonstrated that mindfulness is positively related to psychological health, including greater optimism, happiness, positive affect, decreased depression, anxiety, and feelings of sadness in both children and adults (Greco et al. 2011; Keng et al. 2011; Renshaw and O’Malley 2014; Tan and Martin 2012). However, less is known about the other subscales of quality of life.
In contrast to our finding that mindfulness was inversely related to parent- and autonomy-related quality of life, previous research has described how mindfulness in parents can improve the parent-child dyad through increased empathy, acceptance, and communication (Coatsworth et al. 2010). Similarly, mindfulness in adults can aid in the development of empathy in couples, but this, again, may be an age-related difference between adults and children (Block-Lerner et al. 2007; Wachs and Cordova 2007). Importantly, the parent- and autonomy-related quality of life subscale covers many facets, including two questions on autonomy, three questions on the parent relationship, and two questions on financial resources. It is possible that mindfulness can bring awareness to one’s suffering and unhappiness, resulting in lower quality of life scores. Similarly, children could use lack of mindfulness as a coping strategy when they are dissatisfied with their home life (Miller 2010). Finally, specific aspects of mindfulness, like accepting your thoughts and feelings, may be positively related to parent- and autonomy-related quality of life, but others, like observing or perceiving your thoughts, could be inversely related and this could be reflected in our results.
In our study, mindfulness had no association with peer-related or school-related quality of life. It was particularly surprising that school-related quality of life was unrelated to mindfulness as it was the only context specifically mentioned in the Child and Adolescent Mindfulness Measure, and both scales specifically ask the child about his/her ability to pay attention. As previously described, mindfulness may not translate across contexts, so it was expected that the presence of context-specific questions would illuminate the relationship between school-related quality of life and mindfulness. Similarly, a relationship may have been demonstrated for peer-related quality of life if the questionnaire had focused more on settings involving peers. Other aspects of mindfulness not included, like the ability to describe one’s feelings and thoughts, may be better related to peer-related quality of life subscales. In contrast to our findings, previous research has demonstrated that after mindfulness training, children were rated as more prosocial by their peers and increased their peer acceptance overall (Schonert-Reichl et al. 2015). Results may have differed in our study due to the use of self-reported variables instead of peer-reported variables. While mindfulness has been related to higher overall quality of life, our findings suggest this positive relationship may not exist across all subscales of quality of life.
Mindfulness
Our outcome variable in this study was mindfulness, measured by the Child and Adolescent Mindfulness Measure. Researchers may be concerned that the Child and Adolescent Mindfulness Measure is not culturally appropriate (i.e., differences in language and interpretation) for this racially diverse, low-socioeconomic status sample. The average mindfulness score in our sample (23.4) was slightly lower or comparable to previous research, but we reported some group differences not found by other researchers. For example, Tan and Martin (2012) demonstrated no difference between males (26.9) and females (26.2) who completed the Child and Adolescent Mindfulness Measure. In the validation study for this scale, Greco et al. (2011) observed no difference in mindfulness by sex (23.3 in males vs. 22.4 in females), or by race (23.4 in white vs. 20.7 in black children) or grade in school (22.3 in fifth and sixth grade vs. 24.5 in ninth and tenth graders). Bluth and Blanton (2014) reported similar average mindfulness scores (23.0) in an urban high school sample. However, Bluth et al. (2016) demonstrated slightly higher mindfulness values in an at-risk, racially diverse sample (27.1), but the sample was also older (high school). In our study, differences in mindfulness by race and sex were small, and statistical significance may have been a function of the large sample size (N = 754). Moreover, the effect of race and sex disappeared once entered in to the regression, which controlled for other variables. However, if future research shows similar group differences, this could have important implications for when and in whom the most benefits could be elicited from a mindfulness intervention.
Strengths and Limitations
There were several limitations to this study. Recall or social desirability bias could be an issue with any self-report measure (Klesges et al. 2004). Second, the focus on a large, diverse, low-socioeconomic status sample is both a strength and a limitation. Results from this sample may not be generalizable to other populations. Further, reliability of the questionnaires was established in samples very different from that of the current study. For example, Moore et al. (2007) demonstrated that compared to a sample of white children (Cronbach’s alpha = 0.75), the reliability of the PAQ-C in a sample of black children (Cronbach’s alpha = 0.56) was much lower, although Cronbach’s alpha in our study was 0.71.
Lastly, there are no “good” or “bad” numbers for mindfulness, which makes it difficult to interpret our results in light of what is a practically significant difference in mindfulness. There are numerous assessments of mindfulness, and each includes or excludes different aspects of mindfulness (Bergomi et al. 2013). Some researchers have suggested that relating an overall mindfulness score to other variables may be difficult because facets of mindfulness may be differentially related to the target variable (Baer et al. 2006). Therefore, there is a possibility that individual facets of mindfulness are related to health outcomes, but the overall score from the mindfulness measure did not capture those specific facets. Future research should use a measure of mindfulness that delineates individual facets and should also measure variables closely related to mindfulness, like stress and self-regulation. We did not conduct facet-level analysis of mindfulness due to the large number of surveys children in this study had to complete. These measures were not included to limit undue burden to the participants. There has also been some debate on whether mindfulness can even be measured via questionnaire (Grossman 2008; Rosch 2007). Grossman (2011) posited that a requisite amount of mindfulness may be necessary to meaningfully respond to questions regarding one’s mindfulness. Despite this, it is also suggested that mindfulness occurs naturally and as such, should be measurable in all people even if they are unfamiliar with the construct (Brown and Ryan 2004).
Mindfulness may have health benefits aside from known cognitive and psychological variables. Our study provided important, novel information about the relationship between mindfulness and health outcomes in children. Our preliminary findings support that mindfulness was positively related to psychological quality of life and inversely related to junk food intake and parent- and autonomy-related quality of life. However, our study only examined cross-sectional associations. More research needs to be done to see if implementing a mindfulness intervention has an effect on these health-related variables. It is evident that more research is needed using facet-level analysis of mindfulness before widespread implementation of mindfulness intervention for improvement of these health variables.
References
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13(1), 27–45.
Beaulac, J., Kristjansson, E., & Cummins, S. (2009). A systematic review of food deserts, 1966–2007. Preventing Chronic Disease, 6(3), A105.
Bergomi, C., Tschacher, W., & Kupper, Z. (2013). The assessment of mindfulness with self-report measures: existing scales and open issues. Mindfulness, 4(3), 191–202.
Block-Lerner, J., Adair, C., Plumb, J. C., Rhatigan, D. L., & Orsillo, S. M. (2007). The case for mindfulness-based approaches in the cultivation of empathy: does nonjudgmental, present-moment awareness increase capacity for perspective-taking and empathic concern? Journal of Marital and Family Therapy, 33(4), 501–516.
Bluth, K., & Blanton, P. W. (2014). Mindfulness and self-compassion: exploring pathways to adolescent emotional well-being. Journal of Child and Family Studies, 23(7), 1298–1309.
Bluth, K., Campo, R. A., Pruteanu-Malinici, S., Reams, A., Mullarkey, M., & Broderick, P. C. (2016). A school-based mindfulness pilot study for ethnically diverse at-risk adolescents. Mindfulness, 7(1), 90–104.
Bradley, R. H., & Corwyn, R. F. (2002). Socioeconomic status and child development. Annual Review of Psychology, 53(1), 371–399.
Broderick, P. C., & Metz, S. (2009). Learning to BREATHE: a pilot trial of a mindfulness curriculum for adolescents. Advances in School Mental Health Promotion, 2(1), 35–46.
Brown, K. W., & Ryan, R. M. (2004). Perils and promise in defining and measuring mindfulness: observations from experience. Clinical Psychology: Science and Practice, 11(3), 242–248.
Burke, C. A. (2010). Mindfulness-based approaches with children and adolescents: a preliminary review of current research in an emergent field. Journal of Child and Family Studies, 19(2), 133–144.
Camilleri, G. M., Méjean, C., Bellisle, F., Hercberg, S., & Péneau, S. (2015). Association between mindfulness and weight status in a general population from the NutriNet-Santé study. PloS One, 10(6), e0127447.
Chen, E., & Miller, G. E. (2012). “Shift-and-persist” strategies why low socioeconomic status isn’t always bad for health. Perspectives on Psychological Science, 7(2), 135–158.
Chen, E., Matthews, K. A., & Boyce, W. T. (2002). Socioeconomic differences in children's health: how and why do these relationships change with age? Psychological Bulletin, 128(2), 295.
Coatsworth, J. D., Duncan, L. G., Greenberg, M. T., & Nix, R. L. (2010). Changing parent’s mindfulness, child management skills and relationship quality with their youth: results from a randomized pilot intervention trial. Journal of Child and Family Studies, 19(2), 203–217.
Crocker, P., Bailey, D. A., Faulkner, R. A., Kowalski, K. C., & McGRATH, R. (1997). Measuring general levels of physical activity: preliminary evidence for the physical activity questionnaire for older children. Medicine and Science in Sports and Exercise, 29(10), 1344–1349.
Darmon, N., & Drewnowski, A. (2008). Does social class predict diet quality? The American Journal of Clinical Nutrition, 87(5), 1107–1117.
Dey, M., Landolt, M. A., & Mohler-Kuo, M. (2013). Assessing parent–child agreement in health-related quality of life among three health status groups. Social Psychiatry and Psychiatric Epidemiology, 48(3), 503–511.
Drenowatz, C., Eisenmann, J. C., Pfeiffer, K. A., Welk, G., Heelan, K., Gentile, D., et al. (2010). Influence of socio-economic status on habitual physical activity and sedentary behavior in 8-to 11-year old children. BMC Public Health, 10(1), 1.
Gilbert, D., & Waltz, J. (2010). Mindfulness and health behaviors. Mindfulness, 1(4), 227–234.
Greco, L. A., Baer, R. A., & Smith, G. T. (2011). Assessing mindfulness in children and adolescents: development and validation of the Child and Adolescent Mindfulness Measure (CAMM). Psychological Assessment, 23(3), 606.
Grinnell, S., Greene, G., Melanson, K., Blissmer, B., & Lofgren, I. E. (2011). Anthropometric and behavioral measures related to mindfulness in college students. Journal of American College Health, 59(6), 539–545.
Grossman, P. (2008). On measuring mindfulness in psychosomatic and psychological research. Journal of Psychosomatic Research, 64(4), 405–408.
Grossman, P. (2011). Defining mindfulness by how poorly I think I pay attention during everyday awareness and other intractable problems for psychology’s (re) invention of mindfulness: comment on Brown et al. (2011). Psychological Assessment, 23(4), 1034–1040.
Hanson, M. D., & Chen, E. (2007). Socioeconomic status and health behaviors in adolescence: a review of the literature. Journal of Behavioral Medicine, 30(3), 263–285.
Hoelscher, D. M., Day, R. S., Kelder, S. H., & Ward, J. L. (2003). Reproducibility and validity of the secondary level school-based nutrition monitoring student questionnaire. Journal of the American Dietetic Association, 103(2), 186–194.
Hulbert-Williams, L., Nicholls, W., Joy, J., & Hulbert-Williams, N. (2014). Initial validation of the mindful eating scale. Mindfulness, 5(6), 719–729.
Kabat-Zinn, J. (1982). An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. General Hospital Psychiatry, 4(1), 33–47.
Kabat-Zinn, J. (1994). Wherever you go, there you are: mindfulness meditation in everyday life. New York: Hyperion Books.
Keng, S.-L., Smoski, M. J., & Robins, C. J. (2011). Effects of mindfulness on psychological health: a review of empirical studies. Clinical Psychology Review, 31(6), 1041–1056.
Klesges, L. M., Baranowski, T., Beech, B., Cullen, K., Murray, D. M., Rochon, J., et al. (2004). Social desirability bias in self-reported dietary, physical activity and weight concerns measures in 8- to 10-year-old African-American girls: results from the Girls health Enrichment Multisite Studies (GEMS). Preventive Medicine, 38(Supplement), 78–87.
Kowalski, K. C., Crocker, P., & Faulkner, R. A. (1997). Validation sf the physical activity questionnaire for older children. Pediatric Exercise Science, 9(4), 174–186.
Kuby, A. K., McLean, N., & Allen, K. (2015). Validation of the Child and Adolescent Mindfulness Measure (CAMM) with non-clinical adolescents. Mindfulness, 6(6), 1448–1455.
Kuczmarski, R. J., Ogden, C. L., Guo, S. S., Grummer-Strawn, L. M., Flegal, K. M., Mei, Z., et al. (2002). 2000CDC growth charts for the United States: methods and development. Vital and Health Statistics Series 11, (246), 1–190.
Liehr, P., & Diaz, N. (2010). A pilot study examining the effect of mindfulness on depression and anxiety for minority children. Archives of Psychiatric Nursing, 24(1), 69–71.
Lubans, D. R., Hesketh, K., Cliff, D., Barnett, L., Salmon, J., Dollman, J., et al. (2011). A systematic review of the validity and reliability of sedentary behaviour measures used with children and adolescents. Obesity Reviews, 12(10), 781–799.
Lupien, S. J., King, S., Meaney, M. J., & McEwen, B. S. (2001). Can poverty get under your skin? Basal cortisol levels and cognitive function in children from low and high socioeconomic status. Development and Psychopathology, 13(03), 653–676.
Maples, J. M., Fitzhugh, E. C., Costello, C. A., Moustaid-Moussa, N., Basset, D. R., Spence, M. L., et al. (2012). Physical activity, screen time, and prevalence of overweight/obesity among adolescents in a creative, problem-solving program. Food and Nutrition Sciences, 3(04), 568.
Meiklejohn, J., Phillips, C., Freedman, M. L., Griffin, M. L., Biegel, G., Roach, A., et al. (2012). Integrating mindfulness training into K-12 education: fostering the resilience of teachers and students. Mindfulness, 3(4), 291–307.
Mendelson, T., Greenberg, M. T., Dariotis, J. K., Gould, L. F., Rhoades, B. L., & Leaf, P. J. (2010). Feasibility and preliminary outcomes of a school-based mindfulness intervention for urban youth. Journal of Abnormal Child Psychology, 38(7), 985–994.
Michigan Department of Education (2015). Free and reduced lunch counts. https://www.mischooldata.org/Other/DataFiles/StudentCounts/HistoricalFreeAndReducedLunchCounts.aspx.
Miller, P. H. (2010). Theories of developmental psychology (5th ed.). New York: Worth Publishers.
Montoye, A. H., Pfeiffer, K. A., Alaimo, K., Betz, H. H., Paek, H.-J., Carlson, J. J., et al. (2013). Junk food consumption and screen time: association with childhood adiposity. American Journal of Health Behavior, 37(3), 395–403.
Moor, K. R., Scott, A. J., & McIntosh, W. D. (2013). Mindful eating and its relationship to body mass index and physical activity among university students. Mindfulness, 4(3), 269–274.
Moore, J. B., Hanes, J. C., Jr., Barbeau, P., Gutin, B., Treviño, R. P., & Yin, Z. (2007). Validation of the Physical Activity Questionnaire for Older Children in children of different races. Pediatric Exercise Science, 19(1), 6–19.
Ogden, C. L., Lamb, M. M., Carroll, M. D., & Flegal, K. M. (2010). Obesity and socioeconomic status in children and adolescents: United States, 1988–1994 and 2005-2008. NCHS Data Brief, 51, 1–8 National Center for Health Statistics.
Penkilo, M., George, G. C., & Hoelscher, D. M. (2008). Reproducibility of the school-based nutrition monitoring questionnaire among fourth-grade students in Texas. Journal of Nutrition Education and Behavior, 40(1), 20–27.
Rasmussen, M., Krølner, R., Klepp, K.-I., Lytle, L., Brug, J., Bere, E., et al. (2006). Determinants of fruit and vegetable consumption among children and adolescents: a review of the literature. Part I: quantitative studies. International Journal of Behavioral Nutrition and Physical Activity, 3(1), 22.
Ravens-Sieberer, U., Herdman, M., Devine, J., Otto, C., Bullinger, M., Rose, M., et al. (2014). The European KIDSCREEN approach to measure quality of life and well-being in children: development, current application, and future advances. Quality of Life Research, 23(3), 791–803.
Renshaw, T. L., & O’Malley, M. D. (2014). Cultivating mindfulness in students. Handbook of Positive Psychology in the Schools, 245–259.
Roberts, K. C., & Danoff-Burg, S. (2010). Mindfulness and health behaviors: is paying attention good for you? Journal of American College Health, 59(3), 165–173.
Rosch, E. (2007). More than mindfulness: when you have a tiger by the tail, let it eat you. Psychological Inquiry, 18(4), 258–264.
Schonert-Reichl, K. A., Oberle, E., Lawlor, M. S., Abbott, D., Thomson, K., Oberlander, T. F., et al. (2015). Enhancing cognitive and social–emotional development through a simple-to-administer mindfulness-based school program for elementary school children: a randomized controlled trial. Developmental Psychology, 51(1), 52.
Sibinga, E. M., Webb, L., Ghazarian, S. R., & Ellen, J. M. (2016). School-based mindfulness instruction: an RCT. Pediatrics, 137(1), e20152532.
Singh, N. N., Lancioni, G. E., Winton, A. S., Singh, A. N., Adkins, A. D., & Singh, J. (2008). Clinical and benefit–cost outcomes of teaching a mindfulness-based procedure to adult offenders with intellectual disabilities. Behavior Modification, 32(5), 622–637.
Tan, L., & Martin, G. (2012). Taming the adolescent mind: preliminary report of a mindfulness-based psychological intervention for adolescents with clinical heterogeneous mental health diagnoses. Clinical Child Psychology and Psychiatry, 18(2), 300–312.
Tandon, P. S., Zhou, C., Sallis, J. F., Cain, K. L., Frank, L. D., & Saelens, B. E. (2012). Home environment relationships with children’s physical activity, sedentary time, and screen time by socioeconomic status. International Journal of Behavioral Nutrition and Physical Activity, 9(88), 10.1186.
United States Census Bureau, U. S. C. (2015a). Michigan QuickFacts. http://www.census.gov/quickfacts/table/PST045215/26,2629000.
United States Census Bureau, U. S. C. (2015b). Flint, MI QuickFacts. http://www.census.gov/quickfacts/table/PST045215/2629000.
United States Department of Agriculture (2015). Food Environment Atlas. http://www.ers.usda.gov/data-products/food-environment-atlas/go-to-the-atlas.aspx.
United States Department of Agriculture (2016). Food Access Research Atlas. http://www.ers.usda.gov/data-products/food-access-research-atlas/go-to-the-atlas.aspx.
Van de Weijer-Bergsma, E., Langenberg, G., Brandsma, R., Oort, F. J., & Bögels, S. M. (2014). The effectiveness of a school-based mindfulness training as a program to prevent stress in elementary school children. Mindfulness, 5(3), 238–248.
Van der Gucht, K., Takano, K., Van Broeck, N., & Raes, F. (2015). A mindfulness-based intervention for economically disadvantaged people: effects on symptoms of stress, anxiety, and depression and on cognitive reactivity and overgeneralization. Mindfulness, 6(5), 1042–1052.
Von Rueden, U., Gosch, A., Rajmil, L., Bisegger, C., & Ravens-Sieberer, U. (2006). Socioeconomic determinants of health related quality of life in childhood and adolescence: results from a European study. Journal of Epidemiology and Community Health, 60(2), 130–135.
Wachs, K., & Cordova, J. V. (2007). Mindful relating: exploring mindfulness and emotion repertoires in intimate relationships. Journal of Marital and Family Therapy, 33(4), 464–481.
Wang, Y., & Lim, H. (2012). The global childhood obesity epidemic and the association between socio-economic status and childhood obesity. International Review of Psychiatry, 24(3), 176–188.
Wang, Y., & Zhang, Q. (2006). Are American children and adolescents of low socioeconomic status at increased risk of obesity? Changes in the association between overweight and family income between 1971 and 2002. The American Journal of Clinical Nutrition, 84(4), 707–716.
Wittmann, M., Peter, J., Gutina, O., Otten, S., Kohls, N., & Meissner, K. (2014). Individual differences in self-attributed mindfulness levels are related to the experience of time and cognitive self-control. Personality and Individual Differences, 64, 41–45.
Acknowledgements
We would like to thank the Crim Fitness Foundation for supporting this project and Dr. James Pivarnik, who provided edits to this manuscript.
Author information
Authors and Affiliations
Contributions
KC: analyzed the data and drafted/revised the manuscript. KP: study conception and revised the manuscript. KY: data collection and revised the manuscript. AT: data collection and revised the manuscript. JF: project management and revised the manuscript. SS: project management and revised the manuscript.
Corresponding author
Ethics declarations
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of Interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Clevenger, K.A., Pfeiffer, K.A., Yee, K.E. et al. Mindfulness and Children’s Physical Activity, Diet, Quality of Life, and Weight Status. Mindfulness 9, 221–229 (2018). https://doi.org/10.1007/s12671-017-0765-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-017-0765-3