
Abstract
The objective of this study was to compare the acute effects of hatha yoga and mindfulness meditation on executive function and mood. Using a within-subjects experimental design, 31 moderately experienced hatha yoga practitioners (mean age 27.71 ± 8.32) completed three counterbalanced sessions: hatha yoga (conscious movement and meditation), meditation (mindfulness of breath, emotions, thoughts, and body sensations), and a reading control task. Executive function was assessed using the Stroop task at baseline and at two follow-up points (5 and 10 min post-session). Self-reported mood was measured using the Profile of Mood States (POMS) at baseline and immediately following each session. Findings indicated that hatha yoga (p = .002) and meditation (p = .044) both resulted in significantly improved Stroop performance, though the two conditions did not differ significantly from each other (p = .728). The cognitive benefits in both cases were evident at the 10-min post-session delay but not at the 5-min post-session delay. With respect to mood outcomes, hatha yoga (p < .001) and meditation (p = .050) both resulted in significantly improved POMS total mood scores. Hatha yoga and meditation did not differ significantly from each other in regard to POMS total mood (p = .079), though hatha yoga showed significantly greater benefits on the vigor-activity subscale (p = .006). Overall, findings suggest that acute bouts of hatha yoga and mindfulness meditation benefit executive function and mood to a similar degree.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Yoga is an ancient Indian practice which traditionally aims to cultivate mind-body awareness and higher states of consciousness (Bryant 2009). Hatha yoga is the most common style of yoga practiced in Western societies, and involves mindful physical posturing, breathing exercises, and meditation (Muktibodhananda 2012). A survey of a nationally representative sample estimated that approximately 21 million US citizens practiced hatha yoga in 2012 (Cramer et al. 2016); this represents a tripling of the number of hatha yoga practitioners in a 15-year span (1998–2012; Saper et al. 2004). These statistics suggest that hatha yoga is becoming an increasingly popular modality of exercise in North America.
Meditation is another common complementary practice in Western societies (Clarke et al. 2015), and can be defined as mental training which engages attentional and emotion-regulation abilities through (self- or other-) guided focus on specific objects, intentions, or internal and external environments (Raffone and Srinivasan 2010; Tang et al. 2015). Mindfulness meditation specifically has been operationalized as the practice of non-judgemental observation of present moment thoughts, emotions, and body sensations with openness and acceptance (Bishop et al. 2004). Mindfulness meditation can be practiced on its own or as integrated with physical posturing, as is the case with hatha yoga (Shelov et al. 2009).
Over the past decade, both modalities of hatha yoga and mindfulness meditation have garnered much interest because of their potential for improving cognitive functions (e.g., attention, memory, executive function (EF)). EFs are a set of cognitive abilities that allow for self-regulation of thought, emotions, and behaviors, and most typically involve inhibitory control, mental flexibility, and working memory (Miyake and Friedman 2012). Experimental studies have revealed improvements in inhibitory control following 20 min of hatha yoga and mindfulness meditation in undergraduate samples (Gothe et al. 2013; Wenk-Sormaz 2005). Systematic reviews have also concluded that both hatha yoga and mindfulness meditation practices are promising methods for improving EF (Luu and Hall 2016; Chiesa et al. 2011).
Although the mindfulness meditation literature base is slightly more robust than hatha yoga’s, both face major methodological limitations such as significant variability in intervention delivery methods, participant populations, and cognitive outcome measures, thus making it difficult to draw definitive conclusions. Moreover, both evidence bases appear to lack investigations of acute practice. More rigorous studies of high methodological quality are needed in order to further clarify the EF benefits of acute hatha yoga and mindfulness meditation. Likewise, studies are needed that allow for an examination of the potential influences of physical posturing within mindfulness practices. That is, does the use of physical movement in mindfulness practice, such that utilized in hatha yoga, influence its cognitive effects?
Hatha yoga and mindfulness meditation have also been of increasing interest to mental health professionals, with their broad implications for improving mood outcomes. Mindfulness meditation is used in many psychotherapeutic modalities including dialectical behavior therapy (Robins et al. 2001), and mindfulness-based stress reduction (Samuelson et al. 2007), by which mindfulness practices are employed to accept, tolerate, and reduce distressing affective states (Bishop et al. 2004). Reviews have concluded that mindfulness-based therapeutic interventions are moderately beneficial for improving anxiety and mood symptoms (Hofmann et al. 2010), decreasing emotional reactivity (Keng et al. 2011), and preventing depressive relapse (Fjorback et al. 2011). Likewise, studies suggest that hatha yoga is a beneficial adjunctive treatment modality for various mood disorders (Lin et al. 2011) involving psychological distress (Chong et al. 2011; Streeter et al. 2012), anxiety (Kirkwood et al. 2005), trauma (Telles et al. 2012), and depression (Cramer et al. 2013).
All withstanding, there is yet reason to believe that cognitive and mood benefits are not entirely separable. It has been theorized that reductions in negative mood states (i.e., distress, anxiety) following hatha yoga may mitigate disruptions to certain cognitive functions (Nangia and Malhotra 2012; Rocha et al. 2012). Moreover, some mood dimensions map clearly onto cognitive functions themselves and may represent alternative operationalizations of them. For instance, Stuss (2011) identifies alerting and orienting as one of the primary functions of the prefrontal cortex, and this has a close conceptual link with the mood dimension of vigor-activity. Yet many existing studies examine hatha yoga and mindfulness meditation effects on broader mood dimensions (e.g., positive and negative affect). Investigation of the acute effects of hatha yoga and mindfulness meditation on specific mood dimensions that are theoretically linked (or not) to prefrontal functions might be illuminating.
Using a within-subjects experimental design, the aim of this study was to compare the acute effects of mindfully practiced hatha yoga and mindfulness meditation on its own on cognitive and mood outcomes. It was hypothesized that both hatha yoga and mindfulness meditation would improve EF and mood. It was further hypothesized these effects would comparatively be stronger for hatha yoga, based on the notion that moving through complex physical postures may help augment the attentional processes essential to engaging in mindfulness practices.
Method
Participants
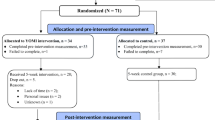
Thirty-one healthy adult females aged 18–48 were recruited through advertisements placed in yoga studios, cafes, and a major university campus between June 2014 and July 2015. To be eligible, participants must have had 4 months to 5 years of prior hatha yoga experience. Naïve practitioners were excluded in order to ensure that hatha yoga poses could be completed to an acceptable criterion (i.e., holding postures with correct and safe alignment while maintaining a steady breathing rhythm) without extensive instruction, and to reduce the possibility of performance anxiety (Eysenck, Derakshan, Santos, and Calvo 2007). Experts at hatha yoga were excluded due to the possibility of ceiling effects, i.e., advanced hatha yoga and meditation practitioners pre-emptively maintain superior cognitive functioning and emotion-regulation at baseline (Froeliger, Garland, Modlin, and McClernon 2012; Moore and Malinowski 2009), and to enhance generalizability of findings to everyday hatha yoga practitioners. This experiential timeframe was chosen as a general guide to identify moderately skilled hatha yoga practitioners.
Table 1 presents participant demographic information. Participants were a mix of university students (n = 18) and community members (n = 13) with an age range of 21–46 (M = 27.71, SD = 8.32). Body mass index was predominantly in the normal range (M = 21.12, SD = 2.19); four were mildly underweight, and none were overweight or obese. The majority of participants were Caucasians with a university level of education.
Procedures
Pre-screen Measures
Eligible participants were tested in three laboratory sessions for 1 h each set at 1 week apart. Participants received an e-mail reminder to abstain from alcohol and caffeinated beverages 3 h prior to each laboratory session. All sessions were held during the same time in evening slots of either 4:00–5:00 p.m., 5:00–6:00 p.m., or 6:00–7:00 p.m. Upon arrival to the first laboratory session, participants completed the Physical Activity Readiness Questionnaire to ensure that they could safely perform physical activity (Canadian Society for Exercise Physiology 2002). Participants then completed a hatha yoga and meditation experience questionnaire of which they identified the approximate years of prior training they maintained (i.e., 4 months–1 year, 1–2 years, 2–3 years, or 3–5 years).
Conditions
Each participant completed three 25-min counterbalanced sessions of hatha yoga, meditation, and a control task of reading yoga culture magazines. Exercise sessions were taught privately by a certified yoga instructor in the Prevention Neuroscience Laboratory at the University of Waterloo. Participants were provided with a yoga mat, props (i.e., cork yoga blocks and bolster), and a water bottle. The hatha yoga condition consisted of mindfulness meditation followed by conscious movement through postures, and final resting corpse pose to conclude. See Table 2 for session details and Appendix A (Supplementary Materials) for the hatha yoga teaching script. To encourage mindfulness practice throughout the class, participants were reminded to focus their attention on their breath and body sensations at least once in every posture. Moreover, participants were told that they should feel a balance of effort and ease throughout the class where a steady breath pattern could be maintained. If a posture was observed to be too strenuous for the participant, a more easeful alternative was offered (i.e., knees lowered down onto the mat during plank pose).
In the meditation condition, participants lay supine and were guided through mindfulness practices. See Table 2 for session details and Appendix B (Supplementary Materials) for the mindfulness meditation teaching script. The meditation began with instructions for the participant to become a non-judgemental third person observer. This was followed by a present moment grounding exercise by becoming aware of the qualities of the breath. Participants were then asked to note their emotions and thoughts with openness and acceptance. Afterwards, they were guided through a body scan, where they were to note feelings and sensations in specified body parts. During the control condition, participants were given several yoga culture magazines of which they casually browsed through.
Measures
Executive Function
The Stroop task (Stroop 1992) was used as the primary measure of EF, specifically the inhibitory control facet (Miyake and Friedman 2012). The Stroop task is a reliable and valid measure of inhibitory control (Wostmann et al. 2013; Homack and Riccio 2004). It is also among the most commonly used measure for quantifying EF effects of exercise in acute bout studies (Etnier and Chang 2009). The version used in the current study was a variant of the version used by Miyake et al. (2000) and delivered through E-Prime software (Psychology Software Tools, Inc). Following 10 practice trials, participants received a mixed block of trials consisting of 12 congruent color words (i.e., color words are displayed in the same color as their semantic meaning), 60 incongruent color words (i.e., color words are displayed in a different color as their semantic meaning), and 72 strings of colored asterisks. Interference scores were calculated as incongruent trial reaction time − asterisk trial reaction time, with scores reverse coded such that higher values indicated stronger inhibitory abilities. The Stroop task was completed at baseline and 5 and 10 min post-sessions.
Mood
The Profile of Mood States-2 Adult Short (POMS) is a 35-item standardized questionnaire used to measure mood. In addition to the total mood score, the POMS yields seven specific dimensions of mood: friendliness, vigor-activity, tension-anxiety, anger-hostility, fatigue-inertia, confusion-bewilderment, and depression-dejection (McNair, Lorr, and Droppleman 1992). The POMS-2A Short is adapted from the original 65-item POMS and is an efficient yet dependable means to identify mood state (Heuchert and McNair 2014). Cronbach alphas were computed based on the current study’s data for each of the POMS subscales and revealed strong internal consistencies, as follows: friendliness (.897), vigor-activity (.922), tension-anxiety (.858), anger-hostility (.967), fatigue-inertia (.920), and confusion-bewilderment (.810). The depression-dejection subscale demonstrated poor reliability, possibly because of invariance on the helplessness item (.204); when this item was removed, reliability increased to acceptable levels (.838). Subsequent analyses utilized this updated version of the scale. Participants were presented a list of words which describe mood (e.g., nervous, good-natured, vigorous) and asked to describe to what extent they were feeling the certain emotion in the present moment. Negatively affective words were coded as 0 = not at all to −4 = extremely. Conversely, positive affect words were coded as 0 = not at all to 4 = extremely. Answers were tallied to yield a score for total mood (containing all dimensions) and individually separate dimensions. Mood was measured at baseline and immediately after each session.
Data Analyses
Data analyses were performed using IBM SPSS Statistics 22.0 software. Prior to the primary analyses, outliers—defined as values exceeding 3× the interquartile range—were identified on the Stroop variable (n = 3). Outliers were dropped and multiple imputation using SPSS was employed to replace the missing values. In the primary analyses, two-way repeated-measures analyses of variances (ANOVAs) were performed using Stroop interference and POMS scores as dependents in separate analyses, with both time and condition as within-subjects variables. This was followed up by repeated-measures ANOVAs which disseminated the simple effects of time for each condition. Lastly, Fisher’s LSD post hoc tests were used to compare the effects of condition against each other.
Results
Prior to our main analysis, repeated-measures ANOVAs were conducted to examine the effects of session order. For Stroop performance, there were no significant session order effects at baseline, F(2, 60) = 1.15, p = .320; 5 min post-session, F(2, 60) = 1.63, p = .205; or 10 min post-session, F(2, 60) = 0.42, p = .660. Likewise for POMS total mood, there were no significant session order effects at baseline, F(2, 60) = 0.63, p = .540, and immediately post-session, F(2, 60) = 2.15, p = .125. These findings indicate that counterbalancing was successful.
Stroop Performance
Table 3 presents the means and standard deviations for Stroop interference. An omnibus 3 (time: baseline, 5 min post-session, 10 min post-session) × 3 (condition: hatha yoga, meditation, control) repeated-measures ANOVA was first conducted to examine differences in Stroop interference by time and condition. There was a significant main effect of time, F(2, 60) = 4.91, p = .011, but not condition, F(2, 60) = 0.21, p = .810. These effects were qualified by a significant interaction between time and condition, F(2, 60) = 2.79, p = .029.
Three repeated-measures ANOVAs were then conducted to examine the main effects of time for each condition separately. Significant improvements in Stroop performance were observed for hatha yoga, F(2, 60) = 7.14, p = .002, and meditation, F(2, 60) = 3.28, p = .044, but not control, F(2, 60) = 0.36, p = .700. To further examine time effects, repeated-measures ANOVAs were completed to examine condition effects from baseline to 5 min post-session and baseline to 10 min post-session separately. From baseline to 5 min post-session, there were no significant improvements on Stroop performance for hatha yoga, F(1, 30) = 2.55, p = .120; meditation, F(1, 30) = 2.66, p = .110; or control, F(1, 30) = .31, p = .580. However, significant improvements in Stroop performance emerged from baseline to 10 min post-session for both hatha yoga, F(1, 30) = 16.88, p < .001, d = .79, and meditation, F(1, 30) = 4.921, p = .034, d = .55, but not control, F(1, 30) = .738, p = .400, d = .17.
To compare the effects of condition to each other from baseline to 10 min post-session, Stroop interference change scores were computed and then subjected to Fisher’s LSD post hoc tests. Results revealed that hatha yoga was not significantly more beneficial than meditation (p = .728), but was significantly more beneficial than control (p = .048). Meditation was also significantly more beneficial than control (p = .048).
Mood
Table 4 presents the means and standard deviations for the POMS total mood and subscale scores. Changes in POMS total score were compared across conditions using an omnibus 2 (time: baseline, post-session) × 3 (condition: hatha yoga, meditation, control) repeated-measures ANOVA; there was a significant main effect of time, F(1, 30) = 16.28, p = .001, and condition, F(2, 60) = 5.69, p = .005. The above main effects were qualified by a significant time-by-condition interaction, F(2, 60) = 4.47, p = .016.
Three repeated-measures ANOVAs were then conducted to examine the main effects of time for each condition separately. There were significant improvements in total mood following hatha yoga, F(1, 30) = 20.39, p < .001, d = .61, and meditation, F(1, 30) = 4.16, p = .050, d = .32, but not control, F(1, 30) = 1.54, p = .220, d = .12. To compare the effects of condition to each other, POMS total mood change scores were computed and then subjected to Fisher’s LSD post hoc tests. Results revealed that hatha yoga was not significantly more beneficial than meditation (p = .079) but was significantly more beneficial than control (p = .006). Meditation was not significantly more beneficial than control (p = .284).
Changes in mood for each of the POMS subscales were analyzed using separate 2 × 3 ANOVAs. There were no significant time-by-condition interaction effects for the POMS subscales: friendliness, F(2, 60) = 1.65, p = .200; tension-anxiety, F(2, 60) = 0.22, p = .140; anger-hostility, F(2, 60) = 2.36, p = .103; fatigue-inertia, F(2, 60) = 2.12, p = .129; confusion-bewilderment, F(2, 60) = 0.333, p = .718; and depression-dejection, F(2, 60) = 0.632, p = .540. However, there was a significant time-by-condition interaction for the vigor-activity subscale, F(2, 60) = 8.16, p = .001.
To decompose these findings, repeated-measures ANOVAs were conducted to examine the main effects of time for each condition separately. Significant increases in energy levels were found following hatha yoga, F(1, 30) = 4.32, p = .046, but not meditation, F(1, 30) = 1.61, p = .214. Significant decreases in energy were found following the control task, F(1, 30) = 8.15, p = .008. Once again, to compare the effects of condition against each other, vigor-activity change scores were computed and then subjected to Fisher’s LSD post hoc comparisons. Results showed that hatha yoga was significantly more beneficial than meditation (p = .006) and control, (p = .001). Meditation was not significantly more beneficial than control (p = .438).
Discussion
The current study examined the acute effects of hatha yoga versus mindfulness meditation on EF and mood, using a within-subjects experimental design. Results revealed that 25 min of hatha yoga and mindfulness meditation significantly improved EF task performance. These effects emerged following a 10-min, but not a 5-min, post-session delay. Though hatha yoga presented a greater overall effect, EF improvements via hatha yoga and mindfulness meditation did not significantly differ from each other. Furthermore, total mood immediately improved following both hatha yoga and mindfulness meditation. Hatha yoga exhibited a marginal advantage for improving mood compared to mindfulness meditation, mostly driven by the vigor-activity dimension of the POMS. This study suggests that a single session of hatha yoga and mindfulness meditation may have similar cognitive and mood benefits for moderately experienced hatha yoga practitioners.
The current findings are largely consistent with other studies examining the benefits of hatha yoga and mindfulness meditation. For instance, prior studies found that acute hatha yoga improved inhibitory control in healthy and clinical samples (Gothe et al. 2013; Sandroff et al. 2015). Likewise, acute mindfulness meditation has also been shown to restore inhibitory abilities following a self-regulatory fatigue manipulation (Friese, Messner, and Schaffner 2012). However, one study which examined the effects of 25 min of mindfulness meditation did not find any significant benefits for attention and working memory (Johnson et al. 2015). The 10-min delay in effects observed in the current study was not unexpected given that a prior meta-analysis on acute exercise (i.e., a component of hatha yoga) reported that the most cognitive benefits appear to occur during the 11–20-min post-exercise period (Chang et al. 2012). With respect to the meditation component of both interventions, one theory might posit that meditation-induced sedative effects may need to subside before the cognitive benefits are discernible.
Regarding mood, prior studies have shown that a single session of hatha yoga improved POMS scores in psychiatric inpatients (Lavey et al. 2005) and decreased psychological distress in healthy university students (West et al. 2004). One study reported that 15 min of hatha yoga significantly decreased psychological and physiological markers of stress in office workers (Melville et al. 2012). Furthermore, 1 h of meditation was found to increase positive affect and decrease negative affect in experienced meditators (Harte et al. 1995). A more recent study found that acute mindfulness meditation was significantly beneficial for improving mood on almost all POMS dimensions (Johnson et al. 2015).
The current study did not find specific benefit associated with the addition of the physical activity, but it could be that the posing did bring some minor benefit that was offset by dilution of the mindfulness experience. The findings were not entirely consistent with a synergistic interpretation as we hypothesized, given that the hatha yoga condition did not produce significantly more cognitive benefit than mindfulness meditation alone. It might be useful to understand the current findings with reference to the relative dose of mindfulness imposed by direct practice (i.e., the meditation condition) versus more indirect practice (i.e., the hatha yoga condition). It could be argued that the body posing could somewhat dilute the experience of mindfulness or, on the contrary, amplify it by providing a concrete focus for the practitioner. Future studies could assess and examine the relative amount of immersion produced by each condition and determine whether there were group differences in the “dose” of mindfulness received.
Given the observed effects on cognition and mood that seemed general across both hatha yoga and meditation, it is important to consider potential neural mechanisms. Understanding the mechanisms by which hatha yoga and meditation similarly benefit cognitive processes might be useful in determining how to prescribe and individualize to maximize brain health benefits. Some possibilities include increases in blood flow to the brain, improved blood oxygenation, increases in brain-derived neurotropic factor, HPA-axis modulation, acute stress reduction, autonomic nervous system regulation, increases in gamma-aminobutyric acid, or a combination of any of these (Streeter et al. 2012; Tang et al. 2015). Some of these effects are shared with proposed mechanisms of action for longer-term meditation practice (Tang et al. 2015); however, future research will be required to unpack these biological pathways.
Strengths of the current study included the use of a stringent within-subjects experimental design, standardization of time of day and other variables that might influence response to conditions, and the novel comparison of hatha yoga and mindfulness meditation to each other to identify the specific contribution of the physical preparatory components to any observed effects. Additionally, this study examined the particular timeline of which the cognitive and mood effects emerged.
Limitations
Despite these strengths, there were several limitations to the current study. First, performance biases were inevitable, as it is difficult to blind participants to interventions of this nature. Motivational effects may have also been present as participants were interested in hatha yoga and meditation at baseline. Second, our results are limited in generalizability due to a relatively homogenous sample of primarily educated, Caucasian females of middle to high socioeconomic status. It should likewise be noted that the generalizability of the current findings to group settings has yet to be demonstrated, given that the current sessions were individually taught in a private setting. Logistical limitations also precluded the use of longer hatha yoga and meditation sessions; the 25-min session duration used in the current study would be considered relatively short when compared to typical Western public classes which are approximately 60 to 90 min in length. The effect of duration is unclear, though it is possible that our use of shorter sessions may have led to an under-estimation of the effect of hatha yoga, meditation, or both on the outcomes of interest. In fact, these findings are promising in that even short practices may be effective at improving EF and mood outcomes.
There are several directions for future investigation. The current sample was comprised of primarily experienced hatha yoga practitioners. It is therefore unclear to what extent more novice practitioners would experience similar mood and cognitive benefits. For instance, it is possible that experienced practitioners may more or less readily experience synergy between the physical posing and cognitive meditative components in hatha yoga. This is ultimately an empirical question and could be explored in future studies by recruiting experience-diverse samples. In addition, future studies would do well to examine the influence of clinical status, temperamental factors, and baseline cognitive function on hatha yoga and meditation-related brain and mood benefits.
References
Bryant, E. F. (2009). The yoga sutras of Patañjali: a new edition, translation, and commentary. New York, NY: North Point Press.
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., & Devins, G. (2004). Mindfulness: a proposed operational definition. Clinical Psychology: Science and Practice, 11(3), 230–241.
Canadian Society of Exercise Physiologists. PAR-Q Forms (2002). Retrieved from http://www.csep.ca/CMFiles/publications/parq/par-q.pdf .
Chang, Y. K., Labban, J. D., Gapin, J. I., & Etnier, J. L. (2012). The effects of acute exercise on cognitive performance: a meta-analysis. Brain Research, 1453, 87–101.
Chiesa, A., Calati, R., & Serretti, A. (2011). Does mindfulness training improve cognitive abilities? A systematic review of neuropsychological findings. Clinical Psychology Review, 31(3), 449–464.
Chong, C. S. M., Tsunaka, M., Tsang, H. W. H., Chan, E. P., & Cheung, W. M. (2011). Effects of yoga on stress management in health adults: a systematic review. Alternative Therapies in Health and Medicine, 17(1), 32–38.
Clarke, T. C., Black, L. I., Stussman, B. J., Barnes, P. M., & Nahin, R. L. (2015). Trends in the use of complementary health approaches among adults: United States, 2002–2012. National Health Statistics Reports, 79, 1–16.
Cramer, H., Lauche, R., Langhorst, J., & Dobos, G. (2013). Yoga for depression: a systematic review and meta-analysis. Depression and Anxiety, 30, 1068–1083.
Cramer, H., Ward, L., Steel, A., Lauche, R., Dobos, G., & Zhang, Y. (2016). Prevalence, patterns, and predictors of yoga use: results of a U.S. nationally representative survey. American Journal of Preventative Medicine, 50(2), 230–235.
Etnier, J. L., & Chang, Y. K. (2009). The effect of physical activity on executive function: a brief commentary on definitions, measurement issues, and the current state of the literature. Journal of Sport and Exercise Psychology, 31(4), 469–483.
Eysenck, M. W., Derakshan, N., Santos, R., & Calvo, M. G. (2007). Anxiety and cognitive performance: attentional control theory. Emotion, 7(2), 336–353.
Fjorback, L. O., Arendt, M., Ørnbøl, E., Fink, P., & Walach, H. (2011). Mindfulness-based stress reduction and mindfulness-based cognitive therapy—a systematic review of randomized controlled trials. Acta Psychiatrica Scandinavica, 124(2), 102–119.
Friese, M., Messner, C., & Schaffner, Y. (2012). Mindfulness meditation counteracts self-control depletion. Consciousness and Cognition, 21(2), 1016–1022.
Froeliger, B. E., Garland, E. L., Modlin, L. A., & McClernon, F. J. (2012). Neurocognitive correlates of the effects of yoga and meditation practise on emotion and cognition: a pilot study. Frontiers in Integrative Neuroscience, 6(48), 1–11.
Gothe, N., Pontifex, M. B., Hillman, C., & McAuley, E. (2013). The acute effects of yoga on executive function. Journal of Physical Activity and Health, 10(4), 488–495.
Harte, J. L., Eifert, G. H., & Smith, R. (1995). The effects of running and meditation on beta-endorphin, corticotropin-releasing hormone and cortisol in plasma, and on mood. Biological Psychology, 40, 251–265.
Heuchert, J. P., & McNair, D. M. (2014). Profile of mood states second edition. Journal of Psychological Assessment, 32(3), 273–277.
Hofmann, S. G., Sawyer, A. T., Witt, A. A., & Oh, D. (2010). The effect of mindfulness-based therapy on anxiety and depression: a meta-analytic review. Journal of Consulting and Clinical Psychology, 8(2), 169–183.
Homack, S., & Riccio, C. A. (2004). A meta-analysis of the sensitivity and specificity of the Stroop Color and Word Test with children. Archives of Clinical Neuropsychology, 19(6), 725–743.
Johnson, S., Gur, R. M., David, Z., & Currier, E. (2015). One-session mindfulness meditation: a randomized controlled study of effects on cognition and mood. Mindfulness, 6(1), 88–98.
Keng, S. L., Smoski, M. J., & Robins, C. J. (2011). Effects of mindfulness on psychological health: a review of empirical studies. Clinical Psychology Review, 31(6), 1041–1056.
Kirkwood, G., Rampes, H., Tuffrey, V., Richardson, J., & Pilkington, K. (2005). Yoga for anxiety: a systematic review of the research evidence. British Journal of Sports Medicine, 39(12), 884–891.
Lavey, R., Sherman, T., Mueser, K. T., Osborne, D. D., Currier, M., & Wolfe, R. (2005). The effects of yoga on mood in psychiatric inpatients. Psychiatric Rehabilitation Journal, 28(4), 399–402.
Lin, K. Y., Hu, Y. T., Chang, K. J., Lin, H. F., & Tsauo, J. Y. (2011). Effects of yoga on psychological health, quality of life, and physical health of patients with cancer: a meta-analysis. Evidence-based Complementary and Alternative Medicine, 2011, 1–12.
Luu, K., & Hall, P. A. (2016). Hatha yoga and executive function: a systematic review. Journal of Alternative and Complementary Medicine, 22(2), 125–133.
McNair, D. M., Lorr, M., & Droppleman, L. F. (1992). Revised manual for the profile of mood states. San Diego: Educational and Industrial Testing Services.
Melville, G. W., Chang, D., Colagiuri, B., Marshall, P. W., & Cheema, B. S. (2012). Fifteen minutes of chair-based yoga postures or guided meditation performed in the office can elicit a relaxation response. Evidence-based Complementary and Alternative Medicine, 2012, 1–9.
Miyake, A., & Friedman, N. P. (2012). The nature and organization of individual differences in executive functions four general conclusions. Current Directions in Psychological Science, 21(1), 8–14.
Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D. (2000). The unity and diversity of executive functions and their contributions to complex frontal lobe tasks: a latent variable analysis. Cognitive Psychology, 41(10), 49–100.
Moore, A., & Malinowski, P. (2009). Meditation, mindfulness and cognitive flexibility. Consciousness and Cognition, 18(1), 176–186.
Muktibodhananda, S. (2012). Hatha Yoga Pradipika. New Delhi, IN: Sri Satguru Publications.
Nangia, D., & Malhotra, R. (2012). Yoga, cognition and mental health. Journal of the Indian Academy of Applied Psychology, 38(2), 262–269.
Raffone, A., & Srinivasan, N. (2010). The exploration of meditation in the neuroscience of attention and consciousness. Cognitive Processing, 11(1), 1–7.
Robins, C. J., Ivanoff, A. M., & Linehan, M. M. (2001). Dialectical behavior therapy. In W. J. Livesley (Ed.), Handbook of personality disorders: theory, research, and treatment (pp. 437–459). New York, NY: The Guilford Press.
Rocha, K. K., Ribeiro, A. M., Rocha, K. C., Sousa, M. B., Albuquerque, F. S., Ribeiro, S., & Silva, R. H. (2012). Improvement in physiological and psychological parameters after 6 months of yoga practice. Consciousness and Cognition, 21(2), 843–850.
Samuelson, M., Carmody, J., Kabat-Zinn, J., & Bratt, M. A. (2007). Mindfulness-based stress reduction in Massachusetts correctional facilities. The Prison Journal, 87(2), 254–268.
Sandroff, B. M., Hillman, C. H., Benedict, R. H., & Motl, R. W. (2015). Acute effects of walking, cycling, and yoga exercise on cognition in persons with relapsing-remitting multiple sclerosis without impaired cognitive processing speed. Journal of Clinical and Experimental Neuropsychology, 37(2), 209–219.
Saper, R. B., Eisenberg, D. M., Davis, R. B., Culpepper, L., & Phillips, R. S. (2004). Prevalence and patterns of adult yoga use in the United States: results of a national survey. Alternative Therapies in Health and Medicine, 10(2), 44–49.
Shelov, D. V., Suchday, S., & Friedberg, J. P. (2009). A pilot study measuring the impact of yoga on the trait of mindfulness. Behavioural and Cognitive Psychotherapy, 37(5), 595–598.
Stroop, J. R. (1992). Studies of interference in serial verbal reactions. Journal of Experimental Psychology: General, 121(1), 15–23.
Streeter, C. C., Gerbarg, P. L., Saper, R. B., Ciraulo, D. A., & Brown, R. P. (2012). Effects of yoga on the autonomic nervous system, gamma-aminobutyric-acid, and allostasis in epilepsy, depression, and post-traumatic stress disorder. Medical Hypothesis, 78(5), 571–579.
Stuss, D. T. (2011). Functions of the frontal lobes: relation to executive functions. Journal of the International Neuropsychological Society, 17(6), 759–765.
Tang, Y. Y., Holzel, B. K., & Posner, M. I. (2015). The neuroscience of mindfulness meditation. Nature Reviews Neuroscience, 16, 213–225.
Telles, S., Singh, N., & Balkrishna, A. (2012). Managing mental health disorders resulting from trauma through yoga: a review. Depression Research and Treatment, 2012, 1–9.
Wenk-Sormaz, H. (2005). Meditation can reduce habitual responding. Alternative Therapies in Health and Medicine, 11(2), 42–58.
West, J., Otte, C., Geher, K., Johnson, J., & Mohr, D. C. (2004). Effects of hatha yoga and African dance on perceived stress, affect, and salivary cortisol. Annals of Behavioral Medicine, 28(2), 114–118.
Wostmann, N. M., Aichert, D. S., Costa, A., Rubia, K., Moller, H. J., & Ettinger, U. (2013). Reliability and plasticity of response inhibition and interference control. Brain and Cognition, 81(1), 82–94.
Acknowledgements
The authors thank University of Waterloo Applied Health Science faculty members Dr. John Mielke and Dr. Richard Staines, for their valuable inputs to the project design; Prevention Neuroscience Laboratory members Cassandra Lowe, Fahd Munir, and Petar Grkinic for their assistance in data collection; and yoga studios Moksha Yoga Waterloo and Queen Street Yoga for their valued support in the recruitment process.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Office of Research Ethics at the University of Waterloo and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Luu, K., Hall, P.A. Examining the Acute Effects of Hatha Yoga and Mindfulness Meditation on Executive Function and Mood. Mindfulness 8, 873–880 (2017). https://doi.org/10.1007/s12671-016-0661-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-016-0661-2