
Abstract
Measuring the construct, component processes, and practice of mindfulness remains challenging. This ecological momentary assessment (EMA) study was a pilot parallel group randomized controlled trial of a brief mindfulness practice (Brief-MP) intervention on self-reported mindfulness and performance-based cognition. Adult community smokers were randomly assigned to a Brief-MP or Control (sham meditation) group. Participants carried a personal digital assistant (PDA) for 2 weeks and were instructed to initiate 20 min of meditation (or control) training on the PDA daily, and to complete an assessment of mindfulness and cognition immediately afterwards. Additionally, participants completed assessments at random times up to four times per day. Primary outcome variables were feasibility and acceptability, state and trait mindfulness, a decentered perspective to depressive stimuli, and attentional bias to smoking stimuli. Thirty-seven participants provided EMA data totaling 1874 assessments. Fifteen of 18 Brief-MP participants completed over 75 % of mindfulness trainings in the field. The majority of Brief-MP participants endorsed favorable descriptions of the intervention: “acceptable,” and “willing to recommend to a friend”. Linear Mixed Model analyses on EMA data revealed that, over time, Brief-MP (vs. Control) increased self-reported Curiosity and Decentering assessed by the Toronto Mindfulness Scale. Brief-MP did not change trait mindfulness or cognition. In sum, Brief-MP administered in the field was acceptable and increased state mindfulness.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mindfulness originated in the Buddha’s teachings dating from the sixth century B.C.E. in India. It has been defined as “bare attention…the mind is trained to remain in the present, open, quiet, and alert, contemplating the present event” (Bodhi 2011). Western psychologists defined mindfulness as an inherent feature of human consciousness that can vary markedly between and within individuals, ranging from a highly mindful state to a highly habitual, automatic, or mindless state. Dispositional, or trait, mindfulness refers to an individual’s natural propensity towards mindfulness in everyday life (Brown and Ryan 2003). Mindfulness has also been described as a state of intentionally attending to one’s moment to moment experience with a non-judgmental orientation (Bishop et al. 2004). Mindfulness practice has been shown to improve a variety of psychological disorders such as anxiety, depression, and addiction (Baer 2003; Khoury et al. 2013; Vollestad et al. 2012; Wanden-Berghe et al. 2010; Zgierska et al. 2009).
Measuring the construct of mindfulness in experimental settings remains challenging. Conceptualizations of mindfulness in self-report measures vary greatly from measure to measure and are based on the questionable assumption that individuals can accurately report on their subjective experience (Brown et al. 2007; Grossman 2008). Additionally, few studies measure the quantity and quality of meditation practice. A review paper of mindfulness-based interventions showed that less than one quarter of studies examined associations between practice and clinical outcome. Further, studies that did examine associations between practice and outcome predominantly used a correlational, rather than experimental, approach (Vettese et al. 2009).
Most mindfulness studies have been conducted in laboratory settings. Ecological momentary assessment (EMA) involves assessing phenomena at the moment they occur in a person’s natural environment. Assessments may be done at random times (“random assessments”; RAs) or after having performed certain tasks such as mindfulness practice. Data from EMA studies are highly detailed and can reveal patterns of change within a few hours of each assessment (e.g., Epstein et al. 2009; Shiffman and Waters 2004). EMA can be easily administered using mobile devices programmed to randomly prompt a person to complete assessments (e.g., through beeping), and compliance can be closely monitored (Stone et al. 2002).
Mobile technologies have rarely been used in mindfulness studies. Bricker and colleagues administered an 8-week Acceptance and Commitment Therapy intervention via smartphone to smokers, demonstrating adherence and improved quit rates (Bricker et al. 2014). Geschwind et al. (2011) used EMA to repeatedly assess affect, reward experience, and pleasantness of activities during a Mindfulness-Based Cognitive Therapy intervention and demonstrated increases in positive affect and activity pleasantness during the intervention. Hill and Updegraff (2012) reported a relationship between laboratory-assessed mindfulness and emotion lability in adolescents that was mediated by emotion differentiation assessed during EMA. Levesque and Brown (2007) demonstrated that laboratory-assessed dispositional mindfulness moderated the effect of an implicit autonomy orientation on perceived autonomy assessed during EMA. However, to our knowledge, EMA has not been used to repeatedly assess state mindfulness during a mindfulness-based intervention. Clinically, administering mindfulness practice on a mobile device may introduce mindfulness practice to people who cannot attend in-person classes.
EMA also allows for the real-time study of component processes of mindfulness using performance-based cognitive tasks. Shapiro et al. (2006) proposed a model of mindfulness composed of three fundamental components: intention, attention, and attitude. Intention describes the purpose or motivation supporting one’s practice. Attention consists of attending to moment-to-moment experience. Attitude refers to the qualities one brings to attention such as compassion or non-judgment. A decentered perspective, one quality of a mindful attitude, refers to viewing negative thoughts and feelings as impermanent mental events rather than as valid representations of reality or central elements of the self (Teasdale 2004). Subscales of self-report measures of mindfulness have been used to measure decentering (Feldman et al. 2010; Fresco et al. 2007a, b; Lau et al. 2006); however, few attempts have been made to measure the construct directly. Waters et al. (2009) reported a negative association between dispositional mindfulness and a decentered perspective to depression cues, measured using the self-identification Implicit Association Test (IAT).
We chose to study attentional bias to represent the attention component of mindfulness. Attentional bias is an important cognitive mechanism in anxiety disorders, depressive disorders, and drug addiction (Browning et al. 2012; Field and Cox 2008; Franken 2003; Robinson and Berridge 1993; Van Bockstaele et al. 2014). Individuals with a high attentional bias tend to automatically attend to concern-related stimuli (e.g., threat cues in anxiety disorders and drug-related cues in addictions). Eight-week mindfulness training courses have been largely ineffective in changing attention processes; however, comparisons of attention in experienced meditators and novice- or non-meditators repeatedly showed significant differences (Chisea et al. 2011). Attentional bias has been modified using brief cognitive interventions (Field and Eastwood 2005; Kerst and Waters 2014), suggesting that it may be more easily manipulated than other attentional processes. One study has reported an effect of mindfulness training on attentional bias (Garland et al. 2010).
The purpose of the current study was to examine the feasibility of a brief mindfulness practice intervention (Brief-MP) administered on a mobile device, including examining acceptability, the effect of the intervention on self-reported state and trait mindfulness, and the effect of the intervention on proposed cognitive mechanisms of mindfulness (decentered perspective and attentional bias). The study was conducted in smokers in order to concurrently examine the effect of the intervention on variables related to smoking. The effect of Brief-MP on smoking has been published elsewhere (Ruscio et al. 2015). Additionally, in this population, mindfulness has been linked to cognition (Waters et al. 2009) and there is a large extant EMA literature (Shiffman et al. 2008). We hypothesized that Brief-MP (vs. control) would be feasible and acceptable to participants, would increase state and trait mindfulness, would increase a decentered perspective to depressive stimuli (measured using the depression Implicit Association Test; D-IAT), and would decrease attentional bias to smoking stimuli (measured using the modified Visual Probe (VP) task).
Method
Participants
Forty-four cigarette smokers (23 women (52.3 %), 21 men (47.7 %), mean age = 44.81, SD = 12.55) were recruited from the Washington D.C. metropolitan area using flyers, public transportation- and web-based advertisements. As described in Ruscio et al. (2015), participants were eligible if they were 18–65 years old and smoked at least 10 cigarettes per day for at least 2 years. Participants were excluded if they reported impaired hearing, if their expired carbon monoxide (CO) reading was below 10 parts per million (ppm) at orientation, if they used tobacco products other than cigarettes, or if they were receiving smoking cessation treatment (counseling and/or medication). Participants received compensation for attending laboratory visits (orientation session, $50; visits 2 and 3, $15 each), completing meditations ($5/meditation), and completing each PDA assessment ($1/assessment) (maximum compensation = $215). Federal civilian employees and members of the military were not eligible to receive compensation.
Procedures
Visit 1
Eligible participants attended a 2-h screening session (visit 1) during which informed consent was obtained from all individual participants included in the study. Expired carbon monoxide (CO) levels and saliva samples were also obtained at visit 1. Participants with expired CO in breath of ≥10 ppm were randomly assigned to the experimental (Brief-MP) or the control condition (sham mindfulness meditation) under double-blind conditions. Next, participants completed a demographic and smoking history questionnaire, as well as a battery of self-report measures assessing state mindfulness, trait mindfulness, and decentering/dis-identification. Then, participants completed two measures of attentional bias (VP task) and a task measuring implicit associations (D-IAT).
After completing the cognitive tasks, participants were provided with two handouts describing the potential utility of mindfulness for smokers, as well as instructions on how to implement mindfulness meditation into their daily routine (e.g., deciding on a time and place for daily meditation). Researchers were available to answer any questions participants had about mindfulness and study procedures. Participants received training in how to complete RAs on the PDA, meditation trainings, and post-meditation assessments (see below). Participants were then taken to a quiet room where they listened to a 20-min meditation (Brief-MP) or a sham meditation (Control) on their PDA and completed a post-meditation assessment (described later).
EMA Procedures
Participants carried the PDA around with them as they went about their daily lives. The PDAs were programmed to prompt the participants four times per day at random times to complete state mindfulness assessments and one of the cognitive measures (D-IAT or modified VP) in counterbalanced order. Participants were also instructed to initiate a Meditation Assessment (MA) immediately after completing a meditation.
Visit 2
Participants returned to the laboratory one week after the first session. At visit 2, they completed self-report measures of state and trait mindfulness, and decentering/dis-identification. After listening to a 20-minute meditation or sham meditation, participants completed a post-meditation assessment consisting of a state mindfulness questionnaire and the D-IAT and the modified VP task.
Visit 3
An additional week later, participants returned to the laboratory for their final assessments (visit 3). They completed the same measures as in visit 2, as well as an acceptability questionnaire. Participants were debriefed and offered smoking cessation resources.
Mindfulness Intervention
Participants were randomly assigned to the Brief-MP condition (12 males, 12 females) or a control condition consisting of sham mindfulness meditations (10 males, 10 females). The participant blind was successful with 11 of 18 (61.1 %) Brief-MP participants and 8 of 13 (61.5 %) Control participants reporting that they believed themselves to be in the meditation group at the end of the study. All participants were instructed to use their PDA to complete one meditation session per day. In line with the brief mindfulness meditation literature, both meditation and control recordings lasted 20 min (Bowen and Marlatt 2009; Rogojanski et al. 2011; Wenk-Sormaz 2005; Zeidan et al. 2009, 2010). The experimental group completed five different guided meditations, four of which were based on the structure of a Vipassana insight meditation program. This 4-week program starts with a mindfulness of breath, followed by mindfulness of body, emotions, and thoughts (Moore 2008). The meditation scripts used in the present study were adapted from mindfulness meditations used in previous smoking studies (Brewer et al. 2010; Brewer et al. 2011), as well as informed by brief mindfulness procedures from previous research (Papies et al. 2012). Furthermore, the mindfulness of emotions meditation included components of the RAIN (Recognize, Accept, Investigate, Non-identification) technique (Brach 2012). All meditation scripts (for both groups) were reviewed by an expert and edited according to his feedback (Dr. Judson Brewer, Assistant Professor of Psychiatry; Medical Director, Yale Therapeutic Neuroscience Clinic; and principal investigator for an RCT of Mindfulness Training for smoking cessation; Brewer et al. 2011).
During visit 1, participants experienced their first mindfulness meditation by means of an “urge-surfing” technique (Bowen and Marlatt 2009). This procedure guided participants through a series of cue-exposures teaching them to become aware of and “ride” through fluctuations in urge intensity as opposed to fighting or giving into them. Participants were instructed to complete a meditation once per day using their PDA. If they chose to meditate multiple times in 1 day, that day’s meditation track was repeated. If participants did not meditate on a given day, the missed track was presented the next day. Participants completed two cycles of meditations one through five in order. After the tenth day, the meditation recordings were presented in counterbalanced order.
Control Condition
The control condition consisted of five recordings that were intended to be sham-meditations. The recordings matched the active condition for length and content (attending to urges, the breath, the body, thoughts, and emotions, respectively). Where the meditation condition instructed participants to focus their attention and maintain a non-judgmental, curious stance towards their inner experience, the control condition encouraged participants to let their minds wander in thought and to judge different aspects of their experience (see Ruscio et al. 2015 for more detail).
Laboratory Self-Report Measures
Acceptability
At visit 3, participants were asked to complete the following four items using a Likert scale (0 to 4). “Overall, did you like this program, meaning you found it acceptable?” (Acceptable); “Was meditating 20 minutes per day reasonable?” (Reasonable); “How likely are you to recommend this program to a friend?” (Recommend); “How likely would you be to volunteer for a similar program that continues for up to one month?” (Volunteer).
Demographics/Smoking History Questionnaire
This is a 35-item questionnaire that included questions about demographic information (e.g., age, income) and smoking history (e.g., number of previous quit attempts, years smoked).
Experiences Questionnaire
The 11-item Decentering Subscale from the Experiences Questionnaire (Fresco et al. 2007a) was used to measure self-reported decentering or dis-identification with content of negative thinking. Participants rated items on a scale of 1 (never) to 5 (all the time). The Decentering Subscale has been shown to have adequate internal consistency (Cronbach’s α = 0.83; Fresco et al. 2007b).
Mindfulness Attention Awareness Scale
The 15-item Mindful Attention Awareness Scale (MAAS; Brown and Ryan 2003) was used to assess trait mindfulness (Cronbach’s α = 0.82; Brown and Ryan 2003). Each item was rated on a six-point Likert scale (1 (almost always) to 6 (almost never)). The MAAS total score was calculated as the mean of the 15 items (minimum score = 1, maximum score = 6). The MAAS total score has been shown to correlate with several well-being constructs, discriminate between individuals who practice meditation and those who do not, and predict well-being outcomes in a clinical sample (Brown and Ryan 2003). The MAAS was selected for the present study because previous research had reported an association between MAAS scores and an implicit cognitive measure of a decentered perspective (Waters et al. 2009).
Toronto Mindfulness Scale
The Toronto Mindfulness Scale (TMS; Lau et al. 2006) assessed state mindfulness. The TMS is a 13-item self-report questionnaire with two subscales: curiosity (TMS-Cur) and decentering (TMS-Decen). Each item was rated on a five-point Likert scale ranging from 0 (not at all) to 4 (very much). TMS-Cur and TMS-Decen scores have been shown to increase with increasing mindfulness meditation experience and during the course of an 8-week Mindfulness-Based Stress Reduction Course. TMS-Decen scores were shown to predict clinical outcomes (Lau et al. 2006). In the current study, the TMS was administered to participants at random assessments throughout the day, a novel use of this instrument. The reliability of TMS-Cur and TMS-Decen assessed during EMA was good (Cronbach’s alpha = 0.91 and 0.88, respectively).
Laboratory Cognitive Measures
Depression Implicit Association Test
On the D-IAT, participants were asked to respond rapidly by pressing a certain PDA key for items representing two concepts (e.g., the concepts “depressed” + “me”), and with a different PDA key for items from two other concepts (e.g., the concepts “not depressed” + “not me”) (task 1). In task 2, the assignment of one concept was switched such that “not depressed” + “me” shared a common key-response, and “depressed” + “not me” shared the other response. The idea underlying the IAT is that it is easier to perform the button pressing task when the two concepts are strongly associated in memory than when the two concepts are unrelated (de Houwer 2002). The IAT effect is the difference in reaction times (RTs) on task 1 vs. task 2. This difference is interpreted as a measure of the relative strength of mental associations. In the present example, it indicates whether associations are stronger between “depressed” and “me,” and “not depressed” and “not me,” than between “not depressed” and “me,” and “depressed” and “not me” (Waters et al. 2009). Lower (more negative) scores (i.e., faster responses when “depression” is paired with “not me” compared to when “depression” is paired with “me”) are interpreted as indicating a more detached perspective to depression. That is, stronger mental associations between “depressed” and “me,” and “not depressed” and “not me,” represents a mindless state where little distance exists between an individual’s sense of self and negative (specifically depressive) contents of consciousness. Similarly, stronger mental associations between “not depressed” and “me,” and “depressed” and “not me,” are thought to represent a mindful state, characterized by a decentered perspective to negative (specifically depressive) contents of consciousness.
The D-IAT administered on the PDA had four blocks: (1) first block of task 1 (e.g., depressed + me/not depressed + not me); (2) second block of task 1; (3) first block of task 2 (e.g., not depressed + me/depressed + not me); (4) second block of task 2. At each assessment, participants were randomly assigned to one of four IATs: (a) depressed-me first, depressed on left; (b) depressed-me first, depressed on right; (c) not depressed-me first, not depressed on left; (d) not depressed-me first, not depressed on right. The “depressed” words were sad, lonely, hopeless, guilty, unhappy, discouraged, gloomy, low, depressed, and failure. The “not depressed” words were content, joyful, happy, cheerful, pleased, fun, merry, funny, excited, and positive. “Me” words included I, me, and mine. “Not me” words included they, them, and other.
On each trial, a stimulus (word) was presented in the center of the PDA screen. On the top of the screen were reminders of the categories assigned to each PDA key for the current task. Participants responded by pressing either a “L” key or a “R” key on the PDA. They were instructed to respond as quickly and as accurately as possible. The program randomly selected words such that the sequence of trials alternated between the presentation of a depressed/not depressed word and the presentation of a me/not me word. If the participant responded correctly, the next trial was initiated after an inter-trial interval of 150 ms. If the participant made an error, a red “X” appeared below the stimulus and remained there until the participant corrected their response. A scoring algorithm was used that involves dividing the IAT effect (difference in mean RTs on tasks 1 and 2) by the pooled standard deviation of RTs (Greenwald et al. 2003). The resulting IAT effect, D, is similar to an effect-size measure (see Greenwald et al. for more detail).
Visual Probe Task
The visual probe task (VP) is a widely used measure of attentional bias (Field and Cox 2008) and was assessed at visit 1 only. Participants are presented with a fixation cross followed by a pair of pictures, a smoking-related and a neutral picture presented side by side of the PDA screen for 500 ms. Next, a dot probe was presented on either the right or the left side of the screen. Participants were instructed to respond as quickly as possible by pressing the right or left button on the PDA that corresponds to the location of the probe. The probe replaced the smoking-related picture on half the trials and the neutral picture on half of the trials. Participants completed 80 trials. Stimulus sets used in the present study were taken from Kerst and Waters (2014). RTs were computed from trials with correct responses. To reduce the influence of RT outliers (Ratcliff 1993), RTs less than 100 ms were discarded. Attentional bias was computed as the median RT on trials where the probe replaced the neutral picture minus median RT on trials where the probe replaced the neutral picture. Positive attentional bias scores therefore reflect faster responses on probes that replace smoking pictures.
Modified Visual Probe Task
In the modified visual probe (mVP) task used in this study, and administered at all laboratory visits, participants completed the VP task as described above but were informed that in each pair of pictures one picture would be smoking-related and one would be neutral. Furthermore, they were instructed to try to attend away from the smoking-related picture throughout the task. The modified instruction set was used to try to capture attentional control fostered during mindfulness practice. The mVP task was scored in the same way as the VP task, with more positive scores reflecting faster responses on probes that replace smoking pictures.
Ecological Momentary Assessment
At each RA and MA, participants completed the TMS on the PDA. They also completed either the D-IAT or the modified VP on the PDA (order counterbalanced across assessments).
Data Analytic Strategy
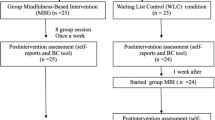
Of the 44 participants randomized to a condition, 37 provided data from at least one EMA assessment, 34 provided laboratory data from at least one of visits 2 and 3, and 32 completed the study. To compute compliance on completion of trainings in the field, non-laboratory assessment days from day 1 to day 15 were used. Laboratory assessment days were excluded because participants were instructed to meditate in the laboratory.
The primary analyses used linear mixed models (LMM) (PROC MIXED in SAS) which allow for different numbers of observations between subjects, account for clustering of data by subject, and are relatively robust to violations of the assumption that the errors are normally distributed (Jacqmin-Gadda et al. 2007). All tests were two-tailed (alpha = 0.05). All analyses included baseline measures of the dependent variable as a covariate in the model.
To analyze the effect of Group on EMA data, Day in study (within-subject) was entered as a continuous variable, along with Group (between-subject: Brief-MP vs. Control) and Assessment Type (within-subject: three levels: RA vs. “valid” MA vs. “invalid” MA). Valid MAs were defined as participant-initiated assessments that were completed within 60 s after the Brief-MP (or control) training. Invalid MAs were all other participant-initiated assessments. The main effect of Group, Group × Day interaction, and Group × Assessment Type interaction were tested for all dependent variables. Each dependent variable was analyzed in a separate model. For all models, we used a random (subject-specific) intercept and an autoregressive model of order 1 for the residuals within subjects. Day was treated as a random effect in the model (slopes were allowed to vary) if the p value for the covariance parameter estimate (for Day) was less than 0.1 (Fitzmaurice et al. 2011). LMMs used data from all participants who completed at least one EMA assessment (n = 37).
To analyze the effect of Group on laboratory data, Visit was entered as a categorical variable (two levels: visit 2 vs. visit 3). The main effects of Group and the Group × Visit interaction term were tested. As with EMA data, each dependent variable was analyzed in a separate model. LMMs on laboratory data used data from all participants who completed at least one laboratory visit post-intervention (n = 34).
Results
Participants’ mean age was 44.81 (SD = 12.55) and 52.27 % were female. The majority (68.18 %) self-identified as Black; 29.55 % self-identified as White and 2.27 % as Other. They reported smoking on average 16.11 cigarettes (SD = 7.36) per day. Descriptive statistics for this sample are presented in more detail in Ruscio et al. (2015). Brief-MP and Control participants did not differ by age, sex, or race. Brief-MP and Control participants also did not differ in measures of baseline mindfulness including MAAS scores. One participant was not compensated due to ineligibility per federal law.
As reported in Ruscio et al. (2015), participants in the Brief-MP and Control groups completed an average of 32.8 (SD = 14.9) and 25.8 (SD = 17.7) RAs, respectively, F(1, 35) = 1.70, p = 0.20, and completed an average of 24.0 (SD = 25.4) and 17.8 (SD = 10.6) MAs, respectively, F(1, 35) = 0.88, p = 0.36.
Completion of Trainings in the Field
Brief-MP completers (n = 18) completed 82.87 % (95 % CI [71.19 %, 94.55 %]) of trainings on non-laboratory assessment days. Fifteen of the 18 Brief-MP participants (83.3 %) completed at least 75 % of trainings. Control completers (n = 14) completed a mean of 41.67 % (95 % CI [25.43 %, 57.90 %]) on non-laboratory assessment days. When including meditations conducted in the laboratory, Brief-MP participants completed an average of 13.1 trainings (SD = 3.23) and Control participants completed an average of 7.2 trainings (SD = 4.44), F(1, 30) = 18.6, p < 0.001.
Completion of Meditation Assessments
Participants in the Brief-MP group (n = 18) completed 92.59 % (95 % CI [83.50 %, 100.00 %]) of MAs in the laboratory and 65.57 % (95 % CI [51.07 %, 80.06 %]) of MAs in the field within 60 s of the end of meditation training. Control participants (n = 13, laboratory; n = 12, field) completed 78.21 % (95 % CI [60.10 %, 96.31 %]) of MAs in the laboratory and 70.62 % (95 % CI [50.52 %, 90.72 %]) of MAs in the field within 60 s.
Acceptability of Intervention
On the “Acceptable” item, 16 of 18 Brief-MP participants (88.9 %) and 13 of 13 control participants (100 %) responded either “3—Somewhat acceptable” or “4—Very acceptable.” On the “Reasonable” item, 17 of 18 Brief-MP participants (94.4 %) and 10 of 13 Control participants (76.9 %) responded either “3—a little reasonable” or “4—very reasonable.” On the “Recommend” item, 15 of 18 Brief-MP participants (83.3 %) and 12 of 13 Control participants (92.3 %) reported that they were “3—quite likely” or “4—very likely” to recommend the program to a friend. Interestingly, control participants (vs. Brief-MP) had higher mean ratings on this item, F(1, 29) = 6.36, p = 0.02. On the “Volunteer” item, 16 of 18 Brief-MP participants (88.9 %) and 11 of 13 Control participants (84.6 %) responded “3—quite likely” or “4—very likely”.
Effect of Brief-MP on Trait and State Mindfulness
Summary statistics are presented in Table 1. An LMM conducted on MAAS scores yielded a non-significant effect of Group and a non-significant Group × Visit interaction (Table 2). The same was true for an LMM conducted on EQ-Decentering scores.
LMMs conducted on TMS-Cur in the laboratory yielded a non-significant effect of Group and a non-significant Group × Visit interaction. LMM conducted on EMA data (TMS-Cur) revealed a significant Group × Day interaction (Table 2, Fig. 1). There was no significant effect of Day for the Brief-MP group, F(1, 19) = 1.86, PE = 0.07, SE = 0.05, p = 0.19, or for the Control group, F(1, 16) = 2.03, PE = −0.12, SE = 0.09, p = 0.17, but the significant interaction reveals that the two slopes were significantly different. When analyzing data from the second week, there was a significant main effect of group, F(1, 792) = 4.31, PE = 2.89, SE = 1.39, p = 0.04, with higher scores in the Brief-MP group.

Mean (±1 SE) of TMS (Toronto Mindfulness Scale) ratings on the Curiosity scale by Group and Day. Data are aggregated over all available assessments
For TMS-Decen, a LMM in the laboratory yielded a non-significant effect of Group and a non-significant Group × Visit interaction. However, a LMM conducted on EMA data revealed a significant Group × Day interaction (Table 2, Fig. 2). There was a significant effect of Day for the Brief-MP group, F(1, 19) = 9.07, PE = 0.20, SE = 0.07, p = 0.007, meaning that TMS-Decen scores increased over time in the Brief-MP Group. There was no effect of Day for the Control group, F(1, 16) = 0.47, PE = −0.07, SE = 0.10, p = 0.50. When analyzing data from the second week, there was a significant main effect of Group, F(1, 792) = 4.01, PE = 2.95, SE = 1.47, p = 0.05, with higher scores in the Brief-MP group.

Mean (±1 SE) of TMS (Toronto Mindfulness Scale) ratings on the Decentering scale by Group and Day. Data are aggregated over all available assessments
Effect of Brief-MP on Cognition
On the modified VP task (visit 1), participants exhibited an attentional bias (−41.0 ms, SD = 75.4) that was significantly different from the attentional bias assessed on the standard VP task (visit 1) (M = 17.3 ms, SD = 93.4), F(1, 42) = 6.98, p = 0.01, suggesting that participants were able follow the instruction to shift their attention away from the smoking picture (leading to faster responses on probes that replaced neutral pictures). However, LMMs conducted on laboratory and EMA attentional bias scores revealed no significant main effects of Group, as well as no significant Group × Visit and Group × Day interactions (Table 2), suggesting that the ability to shift attention was not different in the two groups during subsequent training.
LMMs conducted on laboratory and EMA D-IAT scores also revealed no significant main effects of Group, as well as no significant Group × Visit and Group × Day interactions (Table 2).
Discussion
The main findings of the study were as follows. First, the intervention was feasible. There was good adherence to home meditation practice in the mindfulness group and high ratings on acceptability in both groups. Second, the intervention increased state—but not trait—mindfulness. Third, the intervention did not influence the cognitive measures. These findings are discussed in more detail below.
As noted earlier, adherence to at home meditation was good in the Brief-MP group. Interestingly, adherence was poorer in the Control group. This was true even though the Control group reported that the control intervention was acceptable. The meaning of these data is not clear. The difference in adherence between the two groups could be viewed as a limitation in that the two groups received different “doses” of the meditations. On the other hand, the superior adherence of the Brief-MP group may indicate that the positive effects of Brief-MP influenced participants to continue practicing, which could be interpreted as a strength. Future studies could increase compensation for completing practices, which could reduce the difference in adherence rates between the two groups.
The intervention increased state mindfulness (TMS—Curiosity score and TMS—Decentering score) in the Brief-MP group (vs. Control) over time, but did not increase trait mindfulness (MAAS score). The absence of a Group by Assessment Type interaction indicates that the effect of Brief-MP was not different at random assessments and post-meditation assessments. This suggests that the effect of the intervention on state mindfulness generalizes beyond the immediate post-training period to other times of the day.
One explanation for the finding that the intervention changed state, but not trait mindfulness is that state and trait mindfulness exist on a continuum with state mindfulness being easier to change. It is possible that the experimental manipulation was strong enough to change state mindfulness but not trait mindfulness. A stronger experimental manipulation may be required to change both. For example, one study reported pre-post changes in both state and trait mindfulness following an 8-week Mindfulness-Based Stress Reduction course (Carmody et al. 2008).
State and trait mindfulness may also be conceptually distinct. The MAAS items focus on measuring a single factor that broadly captures the degree to which one is attentive and aware of one’s experiences or surroundings regardless of conceptual or experiential exposure to mindfulness (e.g., “I tend to walk quickly to get where I’m going without paying attention to what I experience along the way”; Brown and Ryan 2003). The TMS measures a two-factor construct, including decentering (e.g., “I was more concerned with being open to my experiences than controlling or changing them”) and curiosity (e.g., “I was curious about my reactions to things”; Lau et al. 2006). The intervention may have been better suited to change state (vs. trait) mindfulness. Participants were led through formal sitting practices. Participants were not explicitly instructed to apply skills cultivated during meditation practice to their daily lives. Because the urge-surfing meditation included the use of cigarettes to provoke cravings, it arguably had the clearest application to daily living. Nonetheless, even in that recording, participants were taught urge-surfing without being explicitly encouraged to practice it in their lives. Changing the intervention to teach and encourage participants to use smaller moments of mindfulness throughout the day in addition to formal sitting practice may yield changes to trait mindfulness in addition to state mindfulness.
Alternatively, the differential results may be due to limitations in self-report measures of mindfulness in general and limitations of the MAAS in particular. Grossman (2011) identified several limitations of self-report mindfulness measures including lack of a gold standard measure for the construct, questionable content validity, and substantial divergence among trait mindfulness measures. The MAAS in particular may be limited by conflating the absence of inattention with the presence of mindfulness (Grossman 2011). A more comprehensive self-report trait measure, such as the Five Factor Mindfulness Questionnaire (Baer et al. 2008), may have performed better. Measuring changes in cognitive processes during mindfulness training offers another lens through which to understand this complex phenomenon.
Analyses did not support hypothesized changes in cognition, including attentional bias and a decentered perspective to depression-related stimuli. This is a relatively new area of study with only one study providing evidence of changes to attentional bias to alcohol-related stimuli in alcohol-dependent individuals following a longer course of mindfulness training Garland et al. (2010). No studies are currently available that document the effect of mindfulness practice on the depression-IAT. Additional weeks of mindfulness practice may be required to observe an effect on cognition.
Limitations
The study had a number of limitations. First, the study was primarily a feasibility study with low power to detect small and small-to-medium effect sizes in the population. A larger sample size may be necessary to demonstrate the hypothesized changes on trait mindfulness and cognition. Second, the audio recordings used in this study were created by an individual with knowledge of mindfulness, but without a well-established personal daily practice. Additionally, audio recordings offered a standardized but weaker experimental manipulation than a live group intervention. Live groups offer greater context, a shared experience, and the opportunity to ask questions that are absent in the one-way communication of a recording. Third, during the VP task, participants were asked to voluntarily attend away from smoking stimuli. While the modified instructions were intended to measure attentional control, they also were a departure from previous versions of the task (e.g., Garland et al. 2010) making comparisons to previous research difficult. Fourth, 12 of 44 participants (27 %) did not complete the study. We cannot rule out that subject attrition lead to subtle differences in the characteristics of the individuals in the two groups, and that these between-group differences may have contributed to the observed findings, although completers and non-completers did not differ in baseline characteristics (Ruscio et al. 2015). Subject attrition may also reduce the generalizability of study findings. Fifth, the data were collected in non-treatment seeking smokers. We cannot be certain that the results would generalize to different populations. Sixth, adherence to the protocol was higher in the active condition compared to the control condition. Nonetheless, the control was successful in blinding participants (Ruscio et al. 2015). Overall, the results must be interpreted cautiously pending replication.
Strengths and Implications
The use of a mobile device for both intervention and assessment has a number of advantages. Regarding the delivery of the intervention, the PDA’s recording the date and time of when participants initiated meditation practices is superior to retrospective self-reports of meditation practices that are affected by poor memory or demand characteristics. The intervention was self-administered in participants’ natural environment in a format that could be rapidly and easily disseminated. It could provide increased access to beneficial effects of a mindfulness practice to people without access to longer and more rigorous mindfulness-based interventions. Clinically, while self-administered brief interventions probably do not confer as strong a benefit as training in a group setting, they may result in smaller benefits for a greater number of people. Further, people who experience positive benefits from a brief intervention may seek out more extensive mindfulness training. The control condition, described in detail by Ruscio et al. (2015), successfully blinded participants to group, resulted in lower adherence rates than the experimental condition, and could be easily changed in future studies to isolate specific mechanisms of mindfulness of interest. Regarding assessment, while other studies have measured changes in mindfulness, no other study has randomly sampled state mindfulness several times a day over the course of 2 weeks in the natural environment, and no other studies have examined cognition in the field.
Future Directions
Conducting this pilot trial resulted in several ideas for improving the Brief-MP intervention. Using a group in-person format, whether initially or once per week, would likely result in a more powerful initial experience of mindfulness and provide the opportunity to ask questions prior to home practice. As discussed above, having a more experienced meditator create the recordings may increase the strength of the intervention. Meditations could also be augmented with suggestions for how to apply mindfulness to daily life. Future studies could also identify subgroups of smokers that may respond especially well to a mindfulness-based intervention. Additionally, future research may examine the conceptual distinctions between mindfulness and related constructs such as emotion regulation. The use of EMA to examine changes in state and trait emotion regulation in relation to state and trait mindfulness may provide valuable insight into the relationship between these two similar yet distinct constructs.
References
Baer, R. A. (2003). Mindfulness training as a clinical intervention: a conceptual and empirical review. Clinical Psychology: Science and Practice, 10(2), 125–143. doi:10.1093/clipsy.bpg015.
Baer, R. A., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., Walsh, E., et al. (2008). Construct validity of the Five Facet Mindfulness Questionnaire in meditating and nonmeditating samples. Assessment, 15(3), 329–342. doi:10.1177/1073191107313003.
Bishop, S. R., Lau, M. A., Shapiro, S. L., Carlson, L. E., Anderson, N. D., Carmody, J., et al. (2004). Mindfulness: a proposed operational definition. Clinical Psychology: Science and Practice, 11(3), 230–241. doi:10.1093/clipsy.bph077.
Bodhi, B. (2011). The Noble Eightfold Path: the way to the end of suffering http://www.accesstoinsight.org/lib/authors/bodhi/waytoend.html. Accessed 13 Oct 2011
Bowen, S., & Marlatt, A. (2009). Surfing the urge: brief mindfulness-based intervention for college student smokers. Psychology of Addictive Behaviors, 23(4), 666–671. doi:10.1037/a0017127.
Brach, T. (2012). Working with difficulties: the blessings of RAIN http://www.tarabrach.com/articles/RAIN-WorkingWithDifficulties.html. Accessed 11 July 2012
Brewer, J. A., Bowen, S., & Chawla, N. (2010). Mindfulness training for addictions: smoking edition. Obtained through personal communication with the author
Brewer, J. A., Mallik, S., Babuscio, T. A., Nich, C., Johnson, H. E., Deleone, C. M., & Rounsaville, B. J. (2011). Mindfulness training for smoking cessation: results from a randomized controlled trial. Drug and Alcohol Dependence, 119(1), 72–80. doi:10.1016/j.drugalcdep.2011.05.027.
Bricker, J. B., Mull, K. E., Kientz, J. A., Vilardaga, R., Mercer, L. D., Akioka, K. J., & Heffner, J. L. (2014). Randomized, controlled pilot trial of a smartphone app for smoking cessation using acceptance and commitment therapy. Drug and Alcohol Dependence, 143, 87–94. doi:10.1016/j.drugalcdep.2014.07.006.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822–848. doi:10.1037/0022-3514.84.4.822.
Brown, K. W., Ryan, R. M., & Creswell, J. D. (2007). Mindfulness: theoretical foundations and evidence for its salutary effects. Psychological Inquiry, 18(4), 211–237. doi:10.1080/10478400701598298.
Browning, M., Holmes, E. A., Charles, M., Cowen, P. J., & Harmer, C. J. (2012). Using attentional bias modification as a cognitive vaccine against depression. Biological Psychiatry, 72(7), 572–579. doi:10.1016/j.biopsych.2012.04.014.
Carmody, J., Reed, G., Kristeller, J., & Merriam, P. (2008). Mindfulness, spirituality, and health-related symptoms. Journal of Psychosomatic Research, 64, 393–403. doi:10.1016/j.jpsychores.2007.06.015.
Chisea, A., Calati, R., & Serretti, A. (2011). Does mindfulness training improve cognitive abilities? A systematic review of neuropsychological findings. Clinical Psychology Review, 31, 449–464. doi:10.1016/j.cpr.2010.11.003.
De Houwer, J. (2002). The Implicit Association Test as a tool for studying dysfunctional associations in psychopathology: strengths and limitations. Journal of Behavior Therapy and Experimental Psychiatry, 33(2), 115–133. doi:10.1016/S0005-7916(02)00024-1.
Epstein, D. H., Willner-Reid, J., Vahabzadeh, M., Mezghanni, M., Lin, J.-L., & Preston, K. L. (2009). Real-time electronic diary reports of cue exposure and mood in the hours before cocaine and heroin craving and use. Archives of General Psychiatry, 66(1), 88–94. doi:10.1001/archgenpsychiatry.2008.509.
Feldman, G., Greeson, J., & Senville, J. (2010). Differential effects of mindful breathing, progressive muscle relaxation, and loving kindness meditation on decentering and negative reactions to repetitive thoughts. Behaviour Research and Therapy, 48(10), 1002–1011. doi:10.1016/j.brat.2010.06.006.
Field, M., & Cox, W. M. (2008). Attentional bias in addictive behaviors: a review of its development, causes, and consequences. Drug and Alcohol Dependence, 97, 1–20. doi:10.1016/j.drugalcdep.2008.03.030.
Field, M., & Eastwood, B. (2005). Experimental manipulation of attentional bias increases the motivation to drink alcohol. Psychopharmacology, 183(3), 350–357. doi:10.1007/s00213-005-0202-5.
Fitzmaurice, G. M., Laird, N. M., & Ware, J. H. (2011). Applied longitudinal analysis. Hoboken: Wiley.
Franken, I. H. A. (2003). Drug craving and addiction: integrating psychological and neuropsychopharmacological approaches. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 27(4), 563–579. doi:10.1016/S0278-5846(03)00081-2.
Fresco, D. M., Moore, M. T., van Dulmen, M. H. M., Segal, Z. V., Ma, S. H., Teasdale, J. D., et al. (2007a). Initial psychometric properties of the Experiences Questionnaire: validation of a self-report measure of decentering. Behavior Therapy, 38, 234–246. doi:10.1016/j.beth.2006.08.003.
Fresco, D. M., Segal, Z. V., Buis, T., & Kennedy, S. (2007b). Relationship of posttreatment decentering and cognitive reactivity to relapse in major depression. Journal of Consulting and Clinical Psychology, 75, 447–455. doi:10.1037/0022-006X.75.3.447.
Garland, E. L., Gaylord, S. A., Boettiger, C. A., & Howard, M. O. (2010). Mindfulness training modifies cognitive, affective, and physiological mechanisms implicated in alcohol dependence: results of a randomized controlled pilot trial. Journal of Psychoactive Drugs, 42(2), 177–192. doi:10.1080/02791072.2010.10400690.
Geschwind, N., Peeters, F., Drukker, M., van Os, J., & Wichers, M. (2011). Mindfulness training increases momentary positive emotions and reward experience in adults vulnerable to depression. A randomized controlled trial. Journal of Consulting and Clinical Psychology, 79(5), 618–628. doi:10.1037/a0024595.
Greenwald, A. G., Nosek, B. A., & Banaji, M. R. (2003). Understanding and using the implicit association test: I. An improved scoring algorithm. Journal of Personality and Social Psychology, 85(2), 197. doi:10.1037/0022-3514.85.2.197.
Grossman, P. (2008). On measuring mindfulness in psychosomatic and psychological research. Journal of Psychosomatic Research, 64, 405–408. doi:10.1016/j.jpsychores.2008.02.001.
Grossman, P. (2011). Defining mindfulness by how poorly I think I pay attention during everyday awareness and other intractable problems for psychology’s (re)invention of mindfulness: comment on Brown et al. (2011). Psychological Assessment, 23(4), 1034–1040. doi:10.1037/a0022713.
Hill, C. L. M., & Updegraff, J. A. (2012). Mindfulness and its relationship to emotional regulation. Emotion, 12(1), 81–90. doi:10.1037/a0026355.
Jacqmin-Gadda, H., Sibillot, S., Proust, C., Molina, J. M., & Thiébaut, R. (2007). Robustness of the linear mixed model to misspecified error distribution. Computational Statistucs & Data Analysis, 51(10), 5142–5154. doi:10.1016/j.csda.2006.05.021.
Kerst, W., & Waters, A. J. (2014). Attentional retraining administered in the field reduces smokers’ attentional bias and craving. Health Psychology, 33(10), 1232–1240. doi:10.1037/a0035708.
Khoury, B., Lecomte, T., Fortin, G., Masse, M., Therien, P., Bouchard, V., et al. (2013). Mindfulness-based therapy: a comprehensive meta-analysis. Clinical Psychology Review, 33(6), 763–771. doi:10.1016/j.cpr.2013.05.005.
Lau, M. A., Bishop, S. R., Segal, Z. V., Buis, T., Anderson, N. D., Carlson, L. E., et al. (2006). The Toronto Mindfulness Scale: development and validation. Journal of Clinical Psychology, 62(12), 1445–1467. doi:10.1002/jclp.20326.
Levesque, C., & Brown, K. W. (2007). Mindfulness as a moderator of the effect of implicit motivational self-concept on day-to-day behavioral motivation. Motivation and Emotion, 31(4), 284–299. doi:10.1007/s11031-007-9075-8.
Moore, P. (2008). Introducing mindfulness to clinical psychologists in training: an experiential course of brief exercises. Journal of Clinical Psychology in Medical Settings, 15, 331–337. doi:10.1007/s10880-008-9134-7.
Papies, E. K., Barsalou, L. W., & Custers, R. (2012). Mindful attention prevents mindless impulses. Social Psychological and Personality Science, 3(3), 291–299. doi:10.1177/1948550611419031.
Ratcliff, R. (1993). Methods for dealing with reaction time outliers. Psychological Bulletin, 114, 510–532. doi:10.1037//0033-2909.114.3.510.
Robinson, T. E., & Berridge, K. C. (1993). The neural basis of drug craving: an incentive-sensitization theory of addiction. Brain Research Reviews, 18(3), 247–291. doi:10.1016/0165-0173(93)90013-P.
Rogojanski, J., Vettese, L. C., & Antony, M. M. (2011). Coping with cigarette cravings: comparison of suppression versus mindfulness-based strategies. Mindfulness, 2, 14–26. doi:10.1007/s12671-010-0038-x.
Ruscio, A. C., Muench, C., Brede, E., & Waters, A. J. (2015). Effect of brief mindfulness practice on self-reported affect, craving, and smoking: a pilot randomized controlled trial using ecological momentary assessment. Nicotine & Tobacco Research. doi: 10.1093/ntr/ntv074
Shapiro, S. L., Carlson, L. E., Astin, J. A., & Freedman, B. (2006). Mechanisms of mindfulness. Journal of Clinical Psychology, 62(3), 373–386. doi:10.1002/jclp.20237.
Shiffman, S., & Waters, A. J. (2004). The nicotine dependence syndrome scale: a multidimensional measure of nicotine dependence. Nicotine & Tobacco Research, 6(2), 327–348. doi:10.1080/1462220042000202481.
Shiffman, S., Stone, A. A., & Hufford, M. R. (2008). Ecological momentary assessment. Annual Review of Clinical Psychology, 4, 1–32. doi:10.1146/annurev.clinpsy.3.022806.091415.
Stone, A. A., Shiffman, S., Schwartz, J. E., Broderick, J. E., & Hufford, M. R. (2002). Patient non-compliance with paper diaries. British Medical Journal, 324, 1193–1194. doi:10.1136/bmj.324.7347.1193.
Teasdale, J. D. (2004). Mindfulness-based cognitive therapy. In J. Yiend (Ed.), Cognition, emotion, and psychopathology: theoretical, empirical, and clinical approaches (pp. 270–289). Cambridge: Cambridge University Press.
Van Bockstaele, B., Verschuere, B., Tibboel, H., De Houwer, J., Crombez, G., & Koster, E. H. W. (2014). A review for current evidence for the causal impact of attentional bias on fear and anxiety. Psychological Bulletin, 140(3), 682. doi:10.1037/a0034834.
Vettese, L. C., Toneatto, T., Stea, J. N., Nguyen, L., & Wang, J. J. (2009). Do mindfulness meditation participants do their homework? And does it make a difference? A review of the empirical evidence. Journal of Cognitive Psychotherapy: An International Quarterly, 23(3), 198–225. doi:10.1891/0889-8391.23.3.198.
Vollestad, J., Nielsen, M. B., & Nielsen, G. H. (2012). Mindfulness- and acceptance-based interventions for anxiety disorders: a systematic review and meta-analysis. British Journal of Clinical Psychology, 51(3), 239–260. doi:10.1111/j.2044-8260.2011.02024.x.
Wanden-Berghe, R., Sanz-Valero, J., & Wanden-Berghe, C. (2010). The application of mindfulness to eating disorders treatment: a systematic review. Eating Disorders: The Journal of Treatment and Prevention, 19(1), 34–48. doi:10.1080/10640266.2011.533604.
Waters, A. J., Reitzel, L. R., Cinciripini, P., Li, Y., Marcus, M. T., Vidrine, J. I., & Wetter, D. W. (2009). Associations between mindfulness and implicit cognition and self-reported affect. Substance Abuse, 30(4), 328–337. doi:10.1080/08897070903252973.
Wenk-Sormaz, H. (2005). Meditation can reduce habitual responding. Alternative Therapies, 2(2), 42–58.
Zeidan, F., Gordon, N. S., Merchant, J., & Goolkasian, P. (2009). The effects of brief mindfulness meditation training on experimentally induced pain. The Journal of Pain, 11(3), 199–209. doi:10.1016/j.jpain.2009.07.015.
Zeidan, F., Johnson, S. K., Diamond, B. J., Zhanna, D., & Goolkasian, P. (2010). Mindfulness meditation improves cognition: evidence of brief mental training. Consciousness and Cognition, 19(2), 597–605. doi:10.1016/j.concog.2010.03.014.
Zgierska, A., Rabago, D., Chawla, N., Kushner, K., Koehler, R., & Marlatt, A. (2009). Mindfulness meditation for substance use disorders: a systematic review. Substance Abuse, 30(4), 266–294. doi:10.1080/08897070903250019.
Acknowledgments
This research was supported by Uniformed Services University of the Health Sciences grant number TO72NR awarded to Aimee C. Ruscio.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Ruscio, A.C., Muench, C., Brede, E. et al. Administration and Assessment of Brief Mindfulness Practice in the Field: a Feasibility Study Using Ecological Momentary Assessment. Mindfulness 7, 988–999 (2016). https://doi.org/10.1007/s12671-016-0538-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-016-0538-4