
Abstract
This study investigated the effects of a 6-week adapted mindfulness-based stress reduction (MBSR) intervention on the psychological health and well-being of college students. The experimental group participants were students and faculty (N = 19) who signed up for the mindfulness-based class, and the control group participants (N = 25) were interested in the class but were unable to sign up in time to enroll. Participants were surveyed three times on a range of self-report psychological variables including symptoms of psychological distress, emotional awareness, self-control, day-to-day mindfulness, and subjective vitality. A control group took the same surveys but did not receive any treatment. The adapted-MBSR intervention significantly reduced psychological distress in the experimental group participants as compared to the control group (p = .027, η 2 = .161) and significantly increased self reported mindful awareness (p = .028, η 2 = .160), self-control (p = .007, η 2 = .216), and subjective vitality (p = .001, η 2 = .293), while meta-mood was not affected (p = .314, η 2 = .055). We concluded that MBSR has wide-ranging positive effects on college students, and would be beneficial as a campus stress reduction and preventative mental health intervention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The college years are a crucial and challenging developmental period, both for the formation of habits that lead to success and well-being later in life and for learning to cope with stress and the occurrence of psychological difficulties (Hunt and Eisenberg 2010; Mowbray et al. 2006). Stress, defined as the pattern of responses that an individual makes to stimulus events that disturb his/her equilibrium and exceed his/her ability to cope (Shahrokh and Hales 2003), is high among college populations (Regehr et al. 2013; D’Zurilla and Sheedy 1991), and can trigger underlying vulnerabilities for many psychological disorders (Clark et al. 1999) due to the fact that most disorders have their first onset by age 24 (Kessler et al. 2005).
The stress in college students associated with transitioning away from home and into adulthood, establishing new peer groups, and coping with academic pressures has been correlated with lower course grades (Struthers et al. 2000), decreased social and general problem solving ability (D’Zurilla and Sheedy 1991), illegal drug and alcohol abuse (Seiffge-Krenke 1990), unsafe sexual behavior, and psychosomatic symptoms such as persistent lack of energy, headaches, and asthma (Winkelman 1994; Zaleski et al. 1998).
Furthermore, chronic stress can lead to severe mental and physical disorders such as depression, substance abuse, cardiovascular disease, and cancer (Pearlin and Schieman 2005). Epidemiological data indicate that psychological disorders and stress-related problems are highly prevalent among college students, and have been steadily increasing in their prevalence and severity over time (Gallagher 2013; Zivin et al. 2009). A two-year longitudinal study of the prevalence of mental health problems in college found that over one third of the student population had a mental health problem at each cross section, and over half of students had a mental health problem at least once in 2 years (Zivin et al. 2009). In a large-scale national assessment, more than one-third of undergraduates reported “feeling so depressed it was difficult to function” at least once in the previous year, while nearly one in ten reported “seriously considering committing suicide” in the previous year (American College Health Association 2008). Eating and substance abuse disorders are also widely prevalent in college students (Woods et al. 2010), and self-injurious behavior poses severe problems as well (Whitlock et al. 2006).
Because treatment costs are high for these potentially lifelong psychological problems, preventative treatment and early intervention strategies are needed to help students reduce stress and prevent the onset of mental illness. However, the education and treatment provided by student counseling services for mental health problems is currently not meeting student needs for a variety of reasons (Mowbray et al. 2006). Negative connotations associated with counseling services are still highly prevalent among college students and may prevent many students from seeking help (Eisenberg et al. 2009). Of 1300 college students from 26 campuses with an apparent mental health problem, only 36 % had received treatment in the past year (Eisenberg et al. 2011). The implications of this phenomenon are that students with mood, anxiety, and substance abuse disorders fail to seek early treatment, which can exacerbate the severity of their condition (Hingson et al. 2006; Post and Leverich 2006; Ryan 2003). For those who are actively receiving care, the costs associated with individual therapy sessions are a concern given the financial burden of student loans and the difficulty in maintaining full-time employment while one is a student (Mowbray et al. 2006).
College students coping with psychological disorders also confront many problems in their studies, such as maintaining concentration, remembering details, meeting deadlines under pressure, executive functioning, and maintaining attendance (Mowbray et al. 2006). These problems may lead to adverse educational outcomes and eventual dropout from college (Kessler et al. 1995). Clearly, an intervention that could both reduce psychological distress while also increasing factors that lead to greater well-being and academic success would be beneficial for colleges. Qualities such as self-control, defined as the ability to override ones responses even when feeling a strong urge to the contrary in order to behave consistently with ones goals (Baumeister et al. 2006; Bowlin and Baer 2011), and emotional regulation are skills that could improve student academic and life success while helping students respond more adaptively to the sources of stress around them (Pritchard and Wilson 2003).
Recently, interventions using mindfulness have gained prominence in mainstream psychology and could provide a potential solution to many of the problems outlined above. Mindfulness has become incorporated into a number of well-known mental health interventions because of numerous studies demonstrating its positive effects on human health and well-being and ability to reduce a range of stress-related physical and psychological problems (Shapiro and Carlson 2009; Hofmann et al. 2010; Grossman et al. 2004). Mindfulness meditation is an integral part of these interventions and combines attentional training with the development of insight into one’s experience.
Mindfulness-based stress reduction (MBSR) is an 8-week group intervention that was originally designed for hospital patients with chronic stress-related illness or pain (Kabat-Zinn 2003; Kabat-Zinn 1990). Participants in MBSR are expected to commit to daily meditation exercises for the duration of the course, and sessions consist of guided meditations, collective inquiry into the present moment of experience, didactic presentations on mindful coping strategies, and open discussion (McCown et al. 2011; Shapiro and Carlson 2009).
Mindfulness-based interventions may be able to provide a cheap, effective, and multidimensional solution to many of the physical and mental health problems encountered at college, while simultaneously improving student’s well-being and ability to self-regulate attention, affect, and behavior, factors that could lead to better academic success (Hall 1999; Astin 1997; Bowlin and Baer 2011; Collard et al. 2008). Because mindfulness-based interventions are taught in a group psycho-educational setting, they have the potential to increase access to psychological treatment for college students. Furthermore, mindfulness-based training is advantageous for both clinical and non-clinical populations (Chiesa and Serretti 2009), and therefore when stress reduction, attentional training, and increased well-being are emphasized rather than mental health, stigma concerning enrollment may be reduced. Finally, given that mindfulness-based interventions teach more adaptive coping mechanisms for a variety of life circumstances, these interventions could prevent the onset of serious mental illnesses that emerge in this age demographic.
Mindfulness-based interventions have a wide range of evidence to support their use in the treatment of numerous problems in both clinical and non-clinical populations. However, research on mindfulness-based interventions for non-clinical student populations is less common. A meta analysis by Chiesa and Serretti (2009) found only ten studies published before 2008 that used healthy participants, and while more research was needed to confirm the effects, it concluded that MBSR reduced stress, anxiety, and ruminative thinking, and enhanced empathy and self compassion. A study by Oman et al. (2008) found that meditation-based stress management practices reduced stress and enhanced forgiveness among college undergraduates. Additionally, Deckro et al. (2002) found that a 6-week collegiate modified mind/body intervention significantly reduced psychological distress, state anxiety, and perceived stress. Both studies suggest that mindfulness be used as a preventative college health intervention. Additional studies have been done with nursing students (Mackenzie et al. 2006; Beddoe and Murphy 2004; Kang et al. 2009) and with therapists in training (Shapiro et al. 2007), finding decreases in anxiety, stress, negative affect, and burnout, and increases in empathy, well-being, and self-compassion. A recent 8-week program called mindfulness-based coping with university life (MBCUL) has been developed at the University of Northampton, UK, that is specifically tailored to university students, and a preliminary non-randomized study found significant changes in perceived stress, anxiety, and depression in student participants (Lynch et al. 2011). A follow-up randomized study confirmed the previous results, and found a significant increase in positive reappraisal among participants in the intervention (Walach et al. 2008).
In addition to efforts to bring mindfulness to higher education in the form of a mental health intervention, a growing movement in academics is incorporating meditation and first-person approaches into education as a complement to traditional third-person approaches to learning (Bush 2011). Educators are not only interested in the calming and stress-reducing effects of mindfulness, but also in the cognitive benefits in areas like attention, memory, and executive functioning that can be provided (Bush 2011). Studies have found that mindfulness practice leads to increases in executive attention (Flook et al. 2010; Jha et al. 2007), academic performance in adolescents (Franco et al. 2010) and African American college students (Hall 1999), and self-control (Astin 1997; Bowlin and Baer 2011). Astin (1997) found that MBSR significantly increased self-control using the Shapiro Control Inventory (SCI), and Bowlin and Baer (2011) found a correlation between self-control and dispositional mindfulness using the Tangney Self Control Scale (SCS). The construct of self-control is of interest because studies show that it is correlated with higher grade point average, better adjustment (less psychopathology, higher self-esteem), less binge eating and alcohol abuse, better interpersonal skills, secure attachment style, and better emotional responses (Tangney et al. 2004). However, very few studies have investigated its relationship to mindfulness.
Traditional MBSR programs involve a serious time commitment: eight 2.5-h classes, one full-day retreat, and 45 min of meditation practice per day (McCown et al. 2011). While high doses of meditation are likely to provide better results, the amount of time commitment that is required in the original program is an obstacle for busy populations such as college students and for non-clinical populations in general who may be less motivated to do the practices. As a result of this and the strong success of MBSR interventions in general, recent studies have started to analyze the effects of shortened mindfulness interventions in order to determine if smaller doses can still result in significant improvements (Bergen-Cico et al. 2013; Josefsson et al. 2012).
The results of shortened MBSR interventions are few and somewhat mixed, and are mostly conducted on university students. A study by Bergen-Cico et al. (2013) found that a brief 5-week MBSR intervention integrated into an academic course increased self-reported mindfulness and self compassion but did not have a significant effect on trait anxiety. Jain et al. (2007) found a significant reduction in psychological distress and an increase in positive states of mind in students after only four 1.5-h sessions lasting one-month total; however, no significant differences were found between the mindfulness intervention and an active relaxation intervention for psychological distress and positive mood states. Josefsson et al. (2012) did not find significant effects for anxiety, depression, decentering, or executive attention in an adult working population between an active relaxation control group and a 4-week mindfulness intervention consisting of two 45-min classes per week, while Klatt et al. (2008) reduced the duration of classes to 1 hour and daily meditations to 20 min in a 6-week course with working adults without a full-day retreat, and found significant reductions in perceived stress and increases in self-reported mindfulness and sleep quality. Finally, Mackenzie et al. (2006) found significant effects for burnout, relaxation, and life satisfaction in nursing students after a 4-week mindfulness intervention. Due to the irregularity of the total program lengths, class durations, quantities of daily meditation, and measures used for shortened interventions, more studies are needed to determine what effects can be expected from each dosage level.
The present research was conducted in order to examine the efficacy of a shortened mindfulness-based intervention (MBSR adapted) taught to a non-clinical student population. As such, this research aimed to assess the effectiveness of teaching such a class in a college environment, thus contributing to the literature on non-clinical college mindfulness interventions and shortened mindfulness interventions. The constructs that were investigated reflect a dual focus on psychological distress (which as a general construct encompasses stress, anxiety, and depression), in the area of mental health, and self-control, emotional intelligence, and subjective vitality, in the area of positive psychology. Self-control was chosen for its relation to academic success and adaptive functioning. Emotional intelligence and subjective vitality were included as an exploratory analysis of other constructs that could be related to mindfulness training.
Thus, this study hypothesized that the mindfulness-based intervention would 1) decrease general psychological distress, 2) result in increased self-reported self-control, 3) result in greater self-reported emotional intelligence, 4) result in greater self-reported subjective vitality, 5) result in increased self-reported day-to-day mindfulness and finally, 6) these effects would be related to the total amount of time that participants practiced the formal meditation exercises.
Method
Participants
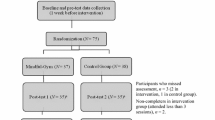
Participants in the intervention (N = 19) were 18 students and one faculty member at Beloit College who expressed interest in mindfulness and signed up for the class. The class was offered to anyone on a first come, first serve basis. Eighty-four percent of the participants were female (N = 16) and 16 % were male (N = 3) with an M age of 21.1 (M = 19.7 without the faculty member). Two additional faculty members and one student took the class but opted out of the study. A control group (N = 25) was formed from a mixture of students who expressed interest in the class or in mindfulness in general but did not sign up or were unable to take the class (N = 20), with some other participants who did not express interest in mindfulness (N = 5). Control participants consisted of students and one administrative staff member and were 52 % female (N = 13) and 48 % male (N = 12), with a M age of 21.4 (M = 20.04 without the staff member).
Fifteen out of the 19 students in the class had never regularly practiced meditation before, and four had limited to moderate experience with meditation. Likewise, 21 participants in the control group had never regularly practiced meditation before, and four had limited to moderate experience. Three control participants and one class participant (all students) dropped out of the study, and they were not included in the analysis. Overall, 19 individuals completed the study from the mindfulness-based intervention group, and 25 individuals completed the study from the control group. See Fig. 1 for a participant flow diagram. The Beloit College Institutional Review Board approved this study.

Participant flow
Procedure
Participants underwent a 6-week mindfulness class adapted from the MBSR curriculum in the first half of the spring semester 2012. This course met once per week for 2-hour sessions, and participants were expected to practice daily exercises in conjunction with the course. Each session involved a mixture of in-class meditations, discussions, lectures, and group activities. Participants were encouraged to practice 30-min meditations at home five days per week, which were recorded by the teachers, in addition to informal mindful exercises (e.g., mindful eating), worksheets (pleasant and unpleasant events calendar, difficult communications), and some optional writing prompts. The full-day retreat was omitted from the intervention.
The curriculum was based upon the MBSR curriculum, as taught in McCown et al. (2011) and Kabat-Zinn (1990) and also using Stahl et al. (2010), but was adapted so as to fit into six sessions. The first class introduced mindfulness, the attitude of beginner’s mind, and the body scan practice, which was the formal practice for the week. The second class was themed habitual reactions and acceptance, and introduced the sitting meditation practice, which was alternated with the body scan for the weekly homework. The third class was about being present in the face of stress and included a didactic presentation by a psychologist on stress reactivity. Mindful yoga was introduced in this class and alternated with the body scan for the daily practice. The fourth class was based on thoughts and emotions, and introduced the expanding awareness meditation, which was alternated with mindful yoga for homework. The fifth class delved into working with difficult emotions, and included a presentation on the anger continuum and a mindful self-inquiry into emotions, with the daily practice being a continuation of the expanding awareness meditation alternated with any other practice of their choice. The sixth and final class dealt with interpersonal relationships and loving-kindness. It covered passive, assertive, and aggressive behaviors, interpersonal mindfulness, the loving kindness meditation practice, and a closing reflection.
In general, the first half of the 2-h class involved didactic or group activities, and the second half consisted of an experiential introduction to the formal meditation technique for that week, consisting of between 30 and 45 min of meditation per class. The class took place in a large basement classroom with fluorescent lighting and a humming sound from the heating system. The students meditated using chairs.
The course was taught by William Conover, M.Div, the Spiritual Life Program Director, and Nicholas Canby, a Program Assistant for the Spiritual Life Program. Before teaching the class, both teachers had experience teaching a weekly mindfulness meditation to students, faculty, and staff, and had also taught some large one-day workshops on mindfulness. In addition, both teachers had personal meditation experience and daily practices, and William Conover had extensive experience working with this age group and setting.
Advertising for the course began in the fall semester with the use of campus flyers and emails, and by contacting people who had attended shorter previous mindfulness events. Interested students were instructed to email the teachers to sign up. The class was full by the end of the fall semester with a total of 22 participants (three faculty and 19 students). Faculty and staff were included in the class because, as the first full MBSR-based class offered at the college, one of the aims of the class was to introduce mindfulness to the college in general. Two of the faculty were from the psychology department and did not participate in the research, and one faculty from the art department participated in the research.
The control group was formed at the same time. A list of people who had expressed interest either in taking the class or in mindfulness in general was compiled, and these people were emailed to request their participation in the research. Those who replied were included. In addition, participation in the control group was advertised on the campus email in order to increase the numbers. Two control group sessions were held to introduce control participants to the research, sign consent forms, and complete the first self-report surveys. The control group did nothing more than complete the self-report surveys.
Incentives, in the form of $10 gift certificates to Pizza Hut ®, were provided by the psychology department to participants in both the class and the control group.
This study used a 2 × 3 quasi-experimental factorial design with one between-participants independent variable with two levels (MBSR or control group) and one within-participants independent variable with three levels (pre-intervention survey, mid-intervention survey, and post-intervention survey). Dependent variables included a range of self-report surveys, introduced below, in addition to the average days per week that participants practiced the meditation exercises (self-reported), and the number of classes that participants attended.
Measures
Five self-report survey measures were used to address the outcomes of the study. The Brief Symptom Inventory (BSI; Derogatis 1975) is a shorter version of the SCL-90-R (Derogatis 1975; Derogatis 1977), and contains 53 questions aimed at addressing psychological symptoms of distress. The scale contains nine subscales, which are somatization, obsession-compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. In addition, three global indices of distress summarize the results: the global severity index (GSI; α = .95), the positive symptom distress index, and the positive symptom total (Derogatis and Melisaratos 1983). Of these, the global severity index is considered to be the most sensitive indicator of the respondent’s level of distress, and provides a general summary of results from the test (Derogatis 1975). The GSI and all of the nine subscales were calculated and used in this study.
The Mindful Attention Awareness Scale, (MAAS; Brown and Ryan 2003; α = .87) measures self-reported trait mindfulness as defined by attention/awareness to the present moment. It contains 15 questions about day-to-day mindful awareness, and does not measure mindful intentions or attitudes. Due to the fact that true mindfulness cannot be assessed through a self-report questionnaire, the results of this measure should not be confused with mindfulness in general.
The Brief Self Control Scale (SCS; Tangney et al. 2004; α = .85) contains 13 items meant to address individual differences in self-control. Self-control is defined as “the capacity to change and adapt the self so as to produce a better, more optimal fit between self and world” (Tangney et al. 2004, p.275). This is accomplished by one’s ability to manage or inhibit internal and/ or behavioral responses and impulses. The test is significantly correlated with academic success (.39 correlation with GPA), and is negatively correlated with alcohol problems (−.32 correlation with the Michigan Alcohol Screening Test), and eating disorders, which are considered impulse control problems.
The Trait Meta-Mood Scale (TMMS; Salovey et al. 1995) is a measure of emotional intelligence with three subscales and a total inventory. The subscales measure individual differences in attention to feelings (attention, α = .78), the clarity of emotional experience (clarity, α = .80), and beliefs about prolonging pleasant mood states and ending unpleasant states (repair, α = .62). It contains 30 questions total, and these are summed up in a total inventory. Participants are asked about their level of agreement with a range of statements pertaining to emotions.
The Subjective Vitality Scale (Ryan and Frederick 1997; α = .84) measures “one’s conscious experience of possessing energy and aliveness” (p. 2), and contains seven items that are associated with general well-being. People with high subjective vitality feel alive and alert. In accordance with the suggestions from the factor analysis of the scale by Bostic et al. (2000), only six items were used in the analyses. The test is considered a measure of general wellness, and is positively correlated with self-esteem and self-actualization, and negatively correlated with psychopathology.
Meditation logs, in addition to these self-report measures, participants filled out weekly practice logs recording the frequency and amount of time that they practiced the meditation exercises each week. In addition, the midpoint and end-of-class surveys asked participants to self-report the average number of days per week that they had practiced meditation since filling out the last survey. Only the latter statistic was used for analysis because participants did not consistently complete and turn in their practice logs.
These five self-report surveys were completed by the class and control group three times throughout the intervention: at the beginning, midpoint and end. The MBSR group completed the first set of surveys at the preliminary class on January 18th, and the control group filled out the same surveys at two meetings during the same week. All participants signed IRB-approved consent forms and the first (pre-intervention) survey was administered in paper form. Each survey contained all of the self-report measures previously introduced, in addition to basic demographic information and a question about previous meditation experience. The control group surveys were identical to the class surveys except that they asked participants if they had been interested in taking the class and if they were interested in mindfulness in general. Each participant received a participant number for his or her confidentiality, and used this number as identification when filling out the surveys. The completed questionnaires were kept in a locked cabinet for the purpose of confidentiality.
The second set of surveys was distributed online between the third and fourth class to both the class and control group. This survey was exactly the same as the first survey except that it asked participants how many days on average per week they had practiced the meditations since filling out the first survey. The final survey was also distributed online, and was sent out just after the last class to both the class and control group. This survey was identical to the second survey except that it also asked class participants how many classes they had attended, and whether they felt that they had benefited significantly from the course, in addition to two open-ended questions asking for reflections and feedback.
Data Analysis
Scoring was calculated with excel and then data was analyzed with SPSS. An alpha level of .05 was used for all statistical tests, and all statistical tests were two-tailed. Preliminary analyses were used to investigate baseline characteristics. Independent sample t tests and chi-square tests were used to test for differences between the MBSR and control group at baseline.
The hypothesized pattern of results for this study was an interaction between group (MBSR class versus control group) and time (pre-intervention, mid-intervention, and post-intervention) for each of the survey variables (GSI, SCS, TMMS, SVS, MAAS). Two-way mixed model analyses of variance were used to test for this interaction for each survey variable. The within subjects variable in these tests was Time, and the between subjects variable was group. Secondary analyses used one-way repeated measures analyses of variance to test for the effects of Time on each group separately, and one-way analyses of variance to test for the main effect of Group while collapsing across the variables of Time.
Finally, change scores were calculated by subtracting the pre-intervention scores from the post-intervention scores, and these were used to test for significant correlations between survey variables. All measures of correlational significance are based on two-tailed bivariate tests.
Results
Results indicate that the non-randomized design of this study resulted in the class and control group being non-equivalent at baseline. A chi-square test found that gender was not evenly distributed in the groups \( \chi \) 2 = 4.98, p < .05, with more women in the intervention and more men in the control group. t tests of baseline data revealed that there was not a significant difference between groups at baseline for the GSI (t(42) = 1.561, p = .126), the SCS (t(42) =−1.901, p = .064), the SVS (t(42) =−1.853, p = .071), or the MAAS (t(42) =−1.369, p = .123). However, for all of these variables, a pattern of results emerged in which the baseline of the control group was roughly equivalent to the midpoint of the class, indicating that the control group had a trend toward less psychopathology, more self control, more subjective vitality, and more mindfulness than the intervention group at baseline.
On average, each student attended M = 4.92 classes (SD = .75) out of the six total. The mean self-reported average days per week that students meditated during the first half was M = 3.95 (SD = 1.42) days per week and during the second half was M = 3.39 (SD = 1.58) days per week, with a total course average number of days per week that students practiced of M = 3.67 (SD = 1.41) days per week.
Significant results were achieved on all of the surveys but one. Table 1 summarizes the mean scores across time and group and the percentage change from pre- to post measurements.
The hypothesis that the intervention would decrease general psychological distress was supported. The General Symptom Inventory (GSI) of the Brief Symptom Inventory had a significant group × time interaction effect F(2,41) = 3.928, p = .027, η 2 = .161, indicating that the intervention succeeded in decreasing psychological distress in the class participants as compared to the control group. A repeated measures ANOVA testing for the effects of Time on GSI for only the intervention group was significant F(2,36) = 10.815, p < .0005, η 2 = .375, meaning that the mindfulness-based class significantly decreased general psychological distress. A repeated measures ANOVA testing for the effects of Time on GSI in the control group was not significant F(2,48) = 1.634, p = .206, η 2 = .064, showing that, as expected, the control group did not change significantly over time. The main effect of Group, however, was not significant F(1,42) = .009, p = .925, η 2 = .000, which appears to be due to the non-equivalent pre-treatment values of this variable.
The hypothesis that the intervention would increase self reported self-control was also supported. The Tangney Self Control Scale (SCS) had a significant group × time interaction effect F(2,41) = 5.648, p = .007, η 2 = .216, indicating that the intervention succeeded in increasing self-control in the class participants as compared to the control group. A repeated measures ANOVA testing for the effects of Time on SCS in the intervention group was significant F(2,36) = 8.72, p = .001, η 2 = .326, showing that the mindfulness-based class significantly increased self-control. A repeated measures ANOVA testing for the effects of time on SCS in the control group was not significant F(2,48) = .288, p = .751, η 2 = .012, meaning that, as expected, the control group did not change significantly over time. The main effect of Group, like the GSI, was not significant F(1,42) = .234, p = .631, η 2 = .006 due to the same pattern of results.
The hypothesis that the intervention would increase self-reported emotional intelligence was not supported. The Trait Meta Mood Scale (TMMS) did not have a significant group × time interaction effect F(2,41) = 1.193, p = .314, η2 = .055 so no further tests were performed.
The hypothesis that the intervention would increase self reported subjective vitality was supported. The Subjective Vitality Scale (SVS) had a significant group × time interaction effect F(2,41) = 8.482, p = .001, η 2 = .293 indicating that the mindfulness-based class succeeded in increasing subjective vitality in the class participants as compared to the control group. A one-way repeated measures ANOVA testing for the effects of time on this variable in only the intervention group was significant F(1.53,36) = 3.649, p = .05, η 2 = .169, meaning that the mindfulness-based class significantly increased subjective vitality. A repeated measures ANOVA testing for the effects of time on SVS in the control group was not significant F(2,48) = .121, p = .886, η 2 = .005, meaning that, as expected, the control group did not change significantly over time. Like the other variables, the main effect of the group was not significant F(1,42) = 1.7, p = .199, η 2 = .039 because of a similar pattern of results.
The hypothesis that the intervention would increase self-reported day-to-day mindfulness was supported. The Mindful Attention Awareness Scale (MAAS) had a significant group × time interaction effect F(2,41) = 3.896, p = .028, η 2 = .160 indicating that the intervention succeeded in increasing day-to-day mindfulness in the class participants as compared to the control group. A one-way repeated measures ANOVA testing for the effects of time on MAAS in only the intervention group was significant F(2,36) = 4.416, p = .019, η 2 = .197, showing that the mindfulness-based class significantly increased day to day mindful awareness. A repeated measures ANOVA testing for the effects of time on MAAS in the control group was not significant F(2,48) = .1.13, p = .331, η 2 = .045, showing that, as expected, the control group did not change significantly over time. Like the other variables, the main effect of group was not significant F(1,42) = .014, p = .906, η 2 = .000 due to a similar pattern of results.
The hypothesis that the results would be related to the total amount of time that participants practiced the formal meditation exercises was not directly supported, although there was evidence approaching significance of a meditating relationship between meditation time, self-reported mindfulness, and the other survey results. The average amount of days per week that participants in the class practiced the meditation exercises (self-reported) was not significantly correlated with the change in GSI scores r = .266, p = .272, change in SCS scores r = .295, p = .219, or change in SVS scores r = .275, p = .254. However, the correlation with the change in MAAS scores approached significance, r = .453, p = .051, indicating that the number of days in which the participants practiced formal meditation was related to a change in self-reported day-to-day mindfulness. The change in MAAS scores was significantly correlated with the change in GSI scores r = .510, p = .026, which provides evidence for a mediating relationship of self-reported day-to-day mindfulness, as measured by the MAAS, between formal meditation practice and symptom reduction. The change in MAAS scores was not significantly correlated with the change in SCS scores r = .418, p = .075, or the change in SVS scores r = .447, p = .055, although these still represent moderate relationships.
When participants were asked at the end of the course if they felt that they had gotten something significant out of the course, 17 out of 19 replied yes. When asked “If yes, how so? If no, why not?” responses included the following: “I think it gave me the tools to use in times when I’m feeling stressed. Although I wasn’t able to utilize the tools every day, I now know how and when to use them,” “This course has helped me to manage anger in a way that has been very useful,” and “I can see clearly how much I’ve changed. I am becoming able to be aware of my feelings, have more confidence and self-control ability.” These comments clearly show that many participants considered the intervention significant and felt personally changed by it. The two students who replied that they did not get anything out of the course said that “I benefitted because this class made me think about mindfulness more in my daily life than I normally would, and I have a lot of valuable resources from the hand outs that were given, but I would have benefitted more if I had done practices every day for the whole 6 weeks,” and “The meditations made me feel anxious and I didn’t feel like I got much out of the 2 hour block on Wednesday nights”. When asked for suggestions, some students recommended a room with less intense lighting in the future and expressed that having the class late in the evening interfered with their ability to focus. All of these comments were from students and were selected by the authors.
Discussion
The research findings indicate that this 6-week mindfulness-based intervention significantly decreased psychological symptomatology and increased self-control, subjective vitality, and self-reported mindful awareness. The effects on psychopathology and mindfulness are consistent with the findings of other researchers, and demonstrate that a shortened intervention with a non-clinical population can have a large effect size on psychological distress. These findings are similar to the results of Jain et al. (2007), which also reduced psychological distress with a large effect size using the same measure in a shortened MBSR intervention in medical, pre-med, and nursing students. Other studies that did not find significant effects for psychological distress (including anxiety and depression) in shortened mindfulness interventions did not use the same measure (Bergen-Cico et al. 2013; Josefsson et al. 2012), so the lack of significance could have been due to the sensitivity of the measurement, differing constructs being measured, or differing elements in the adapted interventions.
The findings related to self-control build on the cross-sectional correlational results of Bowlin and Baer (2011) using the same self control measure but this time within a longitudinal design. The implications of this finding are that mindfulness interventions can be used to increase the adaptive functioning of participants, thus having implications for academic achievement and work productivity. Self-control is also correlated with less alcohol abuse and binge eating, and better relationships and interpersonal skills (Tangney et al. 2004).
The intervention-related increase on the Subjective Vitality Scale helps us understand what positive qualities mindfulness-based training may enhance. Body energy and vitality are often associated with good health, and have played a central role in systems of traditional medicine and spiritual practice from all over the world (Ryan and Frederick 1997). It is interesting to note this as meditation and yoga originally come from such traditions. Furthermore, persistent lack of energy is associated with high stress levels, and in this way subjective vitality describes the opposite effect. Lastly, subjective vitality is related to general well-being and self-motivation (Ryan and Frederick 1997).
It is unclear why the class did not affect the Trait Meta Mood Scale since mindfulness-based training is known to impact emotional regulation, but it may be due to the nature of the survey, or the adaptation or short duration of the intervention. While Brown and Ryan (2003) found a significant correlation between the MAAS and the TMMS, this study did not find a significant correlation between the TMMS and any other measure.
The results, like other recent studies (Bergen-Cico and Cheon 2013), also support the hypothesis of Carmody and Baer (2008) that increases in mindfulness mediate the relationship between meditation practice and symptom reduction as the correlational relationships that were found are indicative of this relationship. Unlike Carmody and Baer, this study used the MAAS to measure mindfulness as opposed to the Five Factor Mindfulness Questionnaire, so these results replicate their results using a different survey measure. The present study measured meditation practice time by asking participants to self-report the average number of days that they practiced meditation in each half of the class, a rather inaccurate measure. Thus, more accurate measurements of practice time would likely have led to stronger correlations.
This study represents an attempt to bring mindfulness-based training to college students who are interested in becoming psychologically healthier. In this context, mindfulness-based training offers a range of benefits. It can be used as a preventative treatment to inoculate participants from serious mental illness, as a way to teach students general life coping mechanisms, and as a way to reduce college stress. It can also be used to improve college emotional health and well-being, including energy and vitality, and finally as a way to increase students’ levels of adaptive functioning and ability to succeed in school.
Limitations and methodological weaknesses were present in this study. The lack of randomization between groups resulted in differences between the intervention and control groups. The two groups differed on gender composition, and while not statistically significant, the intervention tended toward higher levels of psychological distress and lower levels of self-control, subjective vitality, and self-reported mindfulness than the control group.
This pattern of results resulted in significant main effect differences not being found between the class and the control group for any of the variables, because the control group was roughly equivalent to the mid-point time of the class and consequently was not significantly different from the pre-intervention or post-intervention measurements. Given the nature of the enrollment procedure, it is not surprising that those who first signed up showed more symptomatology at intake than the control participants did, but at the close of the study they showed fewer symptoms, resulting in a significant interaction. The fact that five control participants were not interested in mindfulness and the others were less motivated to sign up for the class may be indicative of a lack of psychopathology or stress. However, even with this weakness, the effects are still strong, as by the end of the class, the class group had lower levels of psychopathology and higher levels of self-control, self-reported mindfulness, and subjective vitality than the control group, showing a complete reversal of the pre-intervention trend.
Another limitation is that the group setting and attention were not controlled for. A better design would have employed an active control group that was also engaged in a group intervention, but one that was not mindfulness-based. In the present study, it cannot be known for certain whether the effects are primarily from the mindfulness-training component or from the support and attention of the class. The study also suffered from potential demand characteristics or expectancy effects. Participants in the class implicitly knew that they were expected to improve on the surveys over time and expected that the class would help them with their problems. They may have also wanted to please the researchers when filling out surveys, thus exaggerating the effects. Likewise, the control group knew that it was a control group, and thus did not share these expectancy effects. Finally, while all of the self-report measures that were used in the study have high reliability and validity and were published in peer reviewed journals, self-report measures in general are less reliable than behavioral or physiological measures. Self-report measures are subjective, and depend on the accuracy and truthfulness of participant’s responses. Thus, responses could have reflected biases caused by the demand characteristics and expectancy effects.
Future research is needed to further study the effects of shortened and non-clinical MBSR interventions in order to understand optimal dosage levels for functional but brief interventions. Studies that disassemble MBSR and evaluate its components could be useful in determining the most important aspects to keep when forming brief MBSR interventions. The findings in this study should also be replicated in studies with more participants using active control groups. Finally, we recommend that more studies focus on the academic and cognitive effects of mindfulness so as to better understand how mindfulness can be integrated into higher education and the classroom.
References
American College Health Association. (2008). National College Health Assessment: Reference Group Data Report, Spring 2008. Baltimore, MD: American College Health Association.
Astin, J. A. (1997). Stress reduction through mindfulness meditation. Effects on psychological symptomatology, sense of control, and spiritual experiences. Psychotherapy and Psychosomatics, 66, 97–106.
Baumeister, R. F., Galliot, M., DeWall, C. N., & Oaten, M. (2006). Self-regulation and personality: how interventions increase regulatory success, and how depletion moderates effects of traits on behavior. Journal of Personality, 74, 1773–1801.
Beddoe, A. E., & Murphy, S. O. (2004). Does mindfulness decrease stress and foster empathy among nursing students? The Journal of Nursing Education, 43(7), 305–312.
Bergen-Cico, D., & Cheon, S. (2013). The mediating effects of mindfulness and self-compassion on trait anxiety. Oxford: Mindfulness. Advance online publication.
Bergen-Cico, D., Possemato, K., & Cheon, S. (2013). Examining the efficacy of a brief mindfulness-based stress reduction (brief MBSR) program on psychological health. Journal of American College Health, 61(6), 348–360.
Bostic, T. J., Rubio, D. M., & Hood, M. (2000). A validation of the subjective vitality scale using structural equation modeling. Social Indicators Research, 52(3), 313–324.
Bowlin, S. L., & Baer, R. A. (2011). Relationships between mindfulness, self-control, and psychological functioning. Personality and Individual Differences, 52, 411–415.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822–848.
Bush, M. (2011). Mindfulness in higher education. Contemporary Buddhism: An Interdisciplinary Journal, 12(1), 183–197.
Carmody, J., & Baer, R. A. (2008). Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. Journal of Behavioral Medicine, 31, 23–33.
Chiesa, A., & Serretti, A. (2009). Mindfulness-based stress reduction for stress management in healthy people: a review and meta-analysis. Journal of Alternative and Complementary Medicine, 15(5), 593–600.
Clark, D. A., Beck, A. T., & Alford, B. A. (1999). Scientific foundations of cognitive theory and therapy of depression. New York: John Wiley.
Collard, P., Avny, N., & Boniwell, I. (2008). Teaching mindfulness based cognitive therapy (MBCT) to students: the effects of MBCT on the levels of mindfulness and subjective well-being. Counselling Psychology Quarterly, 24(1), 323–336.
Deckro, G. R., Ballinger, K. M., Hoyt, M., Wilcher, M., Dusek, J., Myers, P., & Benson, H. (2002). The evaluation of a mind/body intervention to reduce psychological distress and perceived stress in college students. Journal of American College Health, 50(6), 281.
Derogatis, L. R. (1975). Brief symptom inventory. Baltimore, MD: Clinical Psychometric Research.
Derogatis, L. R. (1977). The SCL-R-90 manual I: scoring, administration, and procedures for the SCL-90. Baltimore, MD: Clinical Psychometric Research.
Derogatis, L. R., & Melisaratos, N. (1983). The brief symptom inventory: an introductory report. Psychological Medicine, 13(3), 595–605.
D’Zurilla, T. J., & Sheedy, C. F. (1991). Relation between social problem-solving ability and subsequent level of psychological stress in college students. Journal of Personality and Social Psychology, 61(5), 841–846.
Eisenberg, D., Downs, M., & Golberstein, E. (2009). Stigma and help-seeking for mental health among college students. Medical Care Research and Review, 66, 522–541.
Eisenberg, D., Hunt, J., Speer, N., & Zivin, K. (2011). Help seeking for mental health on college campuses: review of evidence and next steps for research and practice. Journal of Nervous and Mental Disease, 199(5), 301–308.
Flook, L., Smalley, S. L., Kitil, J. M., Galla, B. M., Kaiser-Greenland, S., Locke, J., Ishijima, E., & Kasari, C. (2010). Effects of mindful awareness practices on executive functions in elementary school children. Journal of Applied School Psychology, 26(1), 70–95.
Franco, C., Mañas, I., Cangas, A. J., & Gallego, J. (2010). The applications of mindfulness with students of secondary school: results on the academic performance, self-concept and anxiety. Communications in Computer and Information Science, 111, 83–97.
Gallagher, R. P. (2013). National survey of college counseling centers, section one: 4 year directors (Monograph Series Number 9U). Inc: The International Association of Counseling Services.
Grossman, P., Niemann, L., Schmidt, S., & Walach, H. (2004). Mindfulness based stress reduction and health benefits A meta-analysis. Journal of Psychosomatic Research, 57, 35–43.
Hall, P. D. (1999). The effect of meditation on the academic performance of African American college students. Journal of Black Studies, 29(3), 408–415.
Hingson, R. W., Heeren, T., & Winter, M. R. (2006). Age of alcohol-dependence onset: associations with severity of dependence and seeking treatment. Pediatrics, 118, 755–763.
Hofmann, S. G., Sawyer, A. T., Witt, A. A., & Oh, D. (2010). The effect of mindfulness-based therapy on anxiety and depression: a meta-analytic review. Journal of Consulting and Clinical Psychology, 78(2), 169–183.
Hunt, J., & Eisenberg, D. (2010). Mental health problems and help-seeking behavior among college students. Journal of Adolescent Health, 46, 3–10.
Jain, S., Shapiro, S. L., Swanick, S., Roesch, S. C., Mills, P. J., Bell, I., & Schwartz, G. E. R. (2007). A randomized controlled trial of mindfulness meditation versus relaxation training: Effects on distress, positive states of mind, rumination, and distraction. Annals of Behavioral Medicine, 33(1), 11–21.
Jha, A. P., Krompinger, J., & Baime, M. J. (2007). Mindfulness training modifies subsystems of attention. Cognitive, Affective, & Behavioral Neuroscience, 7, 109–119.
Josefsson, T., Lindwall, M., & Broberg, A. G. (2012). The effects of a short-term mindfulness based intervention on self-reported mindfulness, decentering, executive attention, psychological health, and coping style: examining unique mindfulness effects and mediators. Mindfulness, 5, 18–35.
Kabat-Zinn, J. (1990). Full catastrophe living: using the wisdom of your body and mind to face stress, pain and illness. New York: Delacourt.
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: past, present, and future. Clinical Psychology: Science and Practice, 10, 144–156.
Kang, Y. S., Choi, S. Y., & Ryu, E. (2009). The effectiveness of a stress coping program based on mindfulness meditation on stress, anxiety, and depression experienced by nursing students in Korea. Nurse Education Today, 29, 538–543.
Kessler, R. C., Demler, O., Frank, R. G., Olfson, M., Pincus, H. A., & Walters, E. E. (2005). Prevalence and treatment of mental disorders, 1990 to 2003. The New England Journal of Medicine, 352(24), 2515–2523.
Kessler, R. C., Foster, C. L., Saunders, W. B., & Stang, P. E. (1995). The American Journal of Psychiatry, 152, 1026–1032.
Klatt, M. D., Buckworth, J., & Malarkey, W. B. (2008). Effects of low-dose mindfulness-based stress reduction (MBSR-ld) on working adults. Health Education & Behavior, 36(3), 601–614.
Lynch, S., Gander, M., Kohls, N., Kudielka, B., & Walach, H. (2011). Mindfulness-based coping with university life: a non-randomized wait-list-controlled pilot evaluation. Stress and Health, 27, 365–375.
Mackenzie, C. S., Poulin, P. A., & Seidman-Carlson, R. (2006). A brief mindfulness-based stress reduction intervention for nurses and nurse aides. Applied Nursing Research, 19(2), 105–109.
McCown, D., Reibel, D., & Micozzi, M. S. (2011). Teaching mindfulness: a practice guide for clinicians and educators. New York: Springer.
Mowbray, C., Megivern, D., Mandiberg, J. M., Strauss, S., Stein, C. H., Collins, K., & Lett, R. (2006). Campus mental health services: recommendations for change. American Journal of Orthopsychiatry, 76(2), 226–237.
Oman, D., Shapiro, S. L., Thoresen, C. E., Plante, T. G., & Flinders, T. (2008). Meditation lowers stress and supports forgiveness among college students: a randomized controlled trial. Journal of American College Health, 56, 569–578.
Pearlin, L. I., & Schieman, S. (2005). Stress, health, and the life course: some conceptual perspectives. Journal of Health and Social Behavior, 46, 205–219.
Post, R. M., & Leverich, G. S. (2006). The role of psychosocial stress in the onset and progression of bipolar disorder and its comorbidities: the need for earlier and alternative modes of therapeutic intervention. Developmental Psychopathology, 18, 1181–1211.
Pritchard, M. E., & Wilson, G. S. (2003). Using emotional and social factors to predict student success. Journal of College Student Development, 44(1), 18–28.
Regehr, C., Glancy, D., & Pitts, A. (2013). Interventions to reduce stress in university students: a review and meta-analysis. Journal of Affective Disorders, 148, 1–11.
Ryan, N. D. (2003). Child and adolescent depression: short-term treatment effectiveness and long-term opportunities. International Journal of Methods in Psychiatric Research, 12, 44–53.
Ryan, R. M., & Frederick, C. (1997). On energy, personality, and health: subjective vitality as a dynamic reflection of well-being. Journal of Personality, 65, 529–565.
Salovey, P., Mayer, J. D., Goldman, S. L., Turvey, C., & Palfai, T. P. (1995). Emotional attention, clarity, and repair: exploring emotional intelligence using the trait meta-mood scale. In J. W. Pennebaker (Ed.), Emotion, disclosure, & health (pp. 125–154). Washington, DC, US: American Psychological Association.
Seiffge-Krenke, I. (1990). Coping style in adolescence: a cross-cultural study. Journal of Cross-Cultural Psychology, 21, 351–377.
Shahrokh, N. C., & Hales, R. E. (2003). American psychiatric glossary. Washington, DC: American Psychiatric Pub.
Shapiro, S. L., Brown, K. W., & Biegel, G. M. (2007). Teaching self-care to caregivers: effects of mindfulness-based stress reduction on the mental health of therapists in training. Training and Education in Professional Psychology, 1, 105–115.
Shapiro, S. L., & Carlson, L. E. (2009). The art and science of mindfulness: integrating mindfulness into psychology and the helping professions. Washington, DC: American Psychological Association.
Stahl, B., Goldstein, E., Kabat-Zinn, J., & Santorelli, S. (2010). A mindfulness-based stress reduction workbook. Oakland, CA: Harbinger.
Struthers, C. W., Perry, R. P., & Menec, V. H. (2000). An examination of the relationship among academic stress, coping, motivation, and performance in college. Research in Higher Education, 41, 581–592.
Tangney, J. P., Baumeister, R. F., & Boone, A. L. (2004). High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. Journal of Personality, 72, 271–324.
Walach, H., Lynch, S., & Marie-Louise, G. (2008). Mindfulness-based coping with university life (MBCUL): a randomised wait-list controlled study [supplement 1]. European Journal of Integrative Medicine, 1, 40–41.
Whitlock, J. L., Powers, J. L., & Eckenrode, J. (2006). The virtual cutting edge: the internet and adolescent self-injury. Developmental Psychology, 42, 407–417.
Winkelman, M. (1994). Culture shock and adaptation. Journal of Counseling and Development, 73(2), 121–126.
Woods, A. M., Racine, S. E., & Klump, K. L. (2010). Examining the relationship between dietary restraint and binge eating: differential effects of major and minor stressors. Eating Behaviors, 11, 276–280.
Zaleski, E. H., Levey-Thors, C., & Schiaffino, K. M. (1998). Coping mechanisms, stress, social support, and health problems in college students. Applied Developmental Science, 2(3), 127.
Zivin, K., Eisenberg, D., Gollust, S. E., & Golberstein, E. (2009). Persistence of mental health problems and needs in a college student population. Journal of Affective Disorders, 117, 180–185.
Acknowledgments
In memory of Ian Cameron, a powerful light and inspiration for us all, who tragically passed away on June 29th, 2013. Many thanks to Willoughby Britton and her lab for encouraging and supporting the creation of this publication and offering feedback. Many thanks to Gregory Buchanan, who consistently offered his expert guidance to this project from the start, and to William Conover for his practical training and vision. Thank you to all of the participants in the study, who willingly donated their time in filling out the surveys. Thank you to the Beloit College Psychology department for providing an excellent education and for supporting this research.
Author information
Authors and Affiliations
Corresponding author
Additional information
Ian M. Cameron is deceased.
Rights and permissions
About this article

Cite this article
Canby, N.K., Cameron, I.M., Calhoun, A.T. et al. A Brief Mindfulness Intervention for Healthy College Students and Its Effects on Psychological Distress, Self-Control, Meta-Mood, and Subjective Vitality. Mindfulness 6, 1071–1081 (2015). https://doi.org/10.1007/s12671-014-0356-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-014-0356-5