
Abstract
Undergraduate and graduate students show elevated levels of stress and could thus benefit from mindfulness interventions, but the best way to teach mindfulness has not been established. The present study compared a stress management program that used formal meditations and informal practice (Mindful Stress Management; MSM) to one that used brief mindfulness exercises and informal practice (Mindful Stress Management-Informal; MSM-I), and a wait-list control. MSM participants exhibited significant within-group changes on all measures, and when compared to the wait-list control, greater levels of mindfulness, decentering, and self-compassion, as well as lower stress. Students in MSM-I had significant within-group changes on a subset of measures, and greater mindfulness and self-compassion compared to the wait-list. MSM participants showed more improvement in self-compassion, psychological inflexibility, and stress than did those in MSM-I. Mediational analyses found increases in one facet of mindfulness and self-compassion, and decreases in worry mediated reductions in stress for MSM participants, while no mediator reached significance for MSM-I. Finally, no significant relation between amount of formal meditation and informal practice and reductions in psychological distress or increases in mindfulness was found. Results suggest that a program with formal meditations and informal practice may be a more promising intervention for university student stress than one with brief mindfulness exercises and informal practice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Undergraduate and graduate students consistently experience elevated levels of stress due to academic, social, and financial pressures. In an undergraduate sample, 50.8 % of students reported being “often” or “always” stressed (Britz and Pappas 2010). Likewise, medical students, residents, and graduate science students all demonstrated significantly higher scores on a measure of psychological distress than the norm for a stratified random sample of community non-patients (Toews, Lockyer, Dobson, and Brownell 1993). Elevated levels of stress adversely affect psychological and physical health (Schneiderman, Ironson, and Siegel 2005), and a survey of undergraduate and graduate students found stress to be the most commonly reported impediment to academic performance (American College Health Association 2004). University students could thus benefit from stress reduction interventions.
Bishop et al. (2004) characterize mindfulness as maintaining attention on immediate experience, while taking an orientation of openness, acceptance, and curiosity. Mindfulness-based stress reduction (MBSR) was originally developed as a treatment for reducing the enduring stress that accompanies chronic pain (Kabat-Zinn 1982, 1990). It has since been demonstrated to be an effective treatment for anxiety and mood disorders (Hofmann, Sawyer, Witt, and Oh 2010), and a meta-analysis concluded that MBSR significantly reduced stress in healthy populations (Chiesa and Serretti 2009). Furthermore, improvements in symptoms of anxiety, depression, and panic made during MBSR are maintained at follow-up as long as 3 years after the intervention (e.g., Miller, Fletcher, and Kabat-Zinn 1995). When used with university students, MBSR has led to reductions in stress, anxiety, and depression (Shapiro, Brown, Thoresen, and Plante 2011; Shapiro, Schwartz, and Bonner 1998). Accordingly, mindfulness-based interventions appear to be well-suited to reduce stress in student populations, and may help students maintain those gains throughout their academic careers.
Almost all studies of MBSR efficacy incorporating assessment of mindfulness have demonstrated significant pretest-to-posttest increases in mindfulness (e.g., Vøllestad, Sivertsen, and Nielsen 2011). In addition, research evaluating MBSR has also established a relationship between changes in trait mindfulness and other outcome variables, such as decreased psychological distress (e.g., R. W. Brown and Ryan 2003). Moreover, increased mindfulness has been shown to mediate reductions in stress (Nyklíček and Kuijpers 2008; Shapiro, Oman, Thoresen, Plante, and Flinders 2008). Additional variables such as self-compassion, rumination, worry, and psychological inflexibility have been found to mediate reductions in depressive symptoms in several mindfulness-based interventions (Kuyken et al. 2010; Morton, Snowdon, Gopold, and Guymer 2012; van Aalderen et al. 2012), but no study has examined their ability to mediate decreases in stress.
Because research suggests that cultivating mindfulness is important for constructive change, it is important to determine the most effective method(s) of increasing the ability to be mindful. Kabat-Zinn (1982, 1990) designed MBSR as a structured eight-session group intervention with didactic instruction and guided practice in mindfulness meditations, and participants are also assigned homework to engage in daily formal meditations and informal mindfulness practice. Formal meditations are the same as those learned in-session and involve setting aside 45 minutes for daily practice, while informal mindfulness practice involves bringing mindfulness principles into day-to-day activities such as doing the dishes. However, some authors argue that mindfulness can be developed by any method that increases an accepting attitude toward present-moment experiences (Bishop et al. 2004; Hayes and Shenk 2004). For instance, in acceptance and commitment therapy (ACT; Hayes, Strosahl, and Wilson 1999), clients learn mindfulness through metaphors and short experiential exercises, and are encouraged to incorporate mindfulness concepts into their everyday activities. Likewise, individuals engage in brief, 5-minute mindfulness exercises in dialectical behavior therapy (DBT; Linehan 1993), and are then instructed to practice these exercises in addition to bringing mindfulness principles into day-to-day experiences.
Research has shown that formal meditation time, but not informal practice time, was related to increases in trait mindfulness when MBSR was implemented with individuals with stress-related problems, illness, anxiety, and chronic pain (Carmody and Baer 2008), and decreases in rumination have been found in individuals taking part in MBSR or mindfulness-based cognitive therapy (MBCT) (Hawley et al. 2014). In contrast, K. W. Brown and Ryan (2003) found that the extent to which meditation practice was perceived to carry over into day-to-day experiences (informal practice) was related to trait mindfulness levels, while the time spent formally meditating was not. However, their sample consisted of experienced meditators and not participants in MBSR training. As in MBSR, participants in research on the efficacy of ACT and DBT have exhibited significant increases in mindfulness (Fledderus, Bohlmeijer, Pieterse, and Schreurs 2012; Hong 2004). To date, no published research has directly compared a mindfulness-based intervention that teaches mindfulness through formal meditations and informal practice to one that uses brief mindfulness exercises and informal practice. Accordingly, it is not known which method is more successful for cultivating mindfulness.
A program based on brief mindfulness exercises and informal practice without lengthy, daily, and formal meditation may be particularly well-suited for students, who report having stress from an excessive workload (Ross, Niebling, and Heckert 1999), so that they may be unwilling or unable to commit 45 minutes for meditation practice every day. For instance, researchers (Chang et al. 2004; Shapiro, Astin, Bishop, and Cordova 2005) have reported high MBSR attrition rates (e.g., 35 and 44 %, respectively) that participants attribute in part to the extensive time commitment, and participants regularly fail to meditate for the prescribed amount of time (e.g., Carmody and Baer 2008). Additionally, the prescribed 45-minute daily meditation practice and eight-session format may be longer than is necessary for significant change. When a six-session MBSR intervention required participants to formally meditate for 20 minutes daily as opposed to 45 minutes, mindfulness was found to increase significantly in comparison to a wait-list control (Klatt, Buckworth, and Malarkey 2009). An even shorter four-session intervention modeled on MBSR also resulted in significant decreases in distress and increases in positive mood states (Jain et al. 2007), and a meta-analysis concluded that there was no relationship between MBSR in-class hours and reductions in psychological distress. A 2-week online self-guided mindfulness intervention has also been successful at increasing mindfulness and decreasing perceived stress, anxiety, and depression in a student sample (Cavanagh et al. 2013).
The purpose of the present study was thus to compare a mindfulness program for undergraduate and graduate students that incorporated both informal and extended formal mindfulness meditation practice (mindful stress management; MSM) with a training that used brief mindfulness exercises and informal methods (mindful stress management-informal; MSM-I) and with a wait-list control. Both workshops were expected to result in significant increases in mindfulness, mindfulness-related variables, and positive mood states, and decreased stress, anxiety, and depression compared to the control group. Furthermore, change in mindfulness was predicted to mediate reductions in stress. The relation between changes in mindfulness and both formal meditation practice time in MSM and informal mindfulness practice in MSM-I were examined, and practice was expected to be related to the amount of symptom improvement. Finally, the mediating effect of mindfulness-related variables (worry, rumination, psychological inflexibility, self-compassion, and decentering) on changes in stress was examined.
Method
Participants
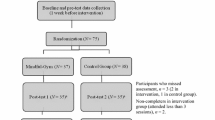
Thirty-four undergraduate and graduate students at a private mid-Atlantic university participated in the study: 13 attended the MSM workshop, 11 attended the MSM-I workshop, and 10 were in the wait-list control group. Women constituted the majority of the sample (88.2 %), and participants’ mean age was 22.35 years (SD = 3.15; range = 18–30). Participants were 70.6 % Caucasian, 8.8 % Asian, 5.9 % Latino, 2.9 % African American, and 11.8 % identified themselves as “other.” Undergraduate students made up 55.9 % of the sample and 44.1 % were graduate students. Prior meditation, yoga, or similar contemplative activity experience was reported by 82.4 % of the sample; mean weekly practice time was 15.38 minutes (SD = 25.85, range = 0–90). The majority with prior experience (53.6 %) reported practicing yoga. (See Table 1 for complete descriptive statistics on the participants.)
Procedure
The study was advertised to students on campus through flyers, announcements in student newsletters, an information table at the student center, and brief announcements at the beginning of undergraduate and graduate psychology classes. Those who were interested in participating were asked to email the first author in order to schedule an appointment to fill out the informed consent form and pretest measures, which were completed the week before the workshops began. The two workshops were randomly assigned to two preselected timeslots, and participants were assigned to the two workshops and wait-list control partly based on their availability. If participants were available during both workshop times, they were randomly assigned to one of the workshops. Each workshop consisted of six weekly 1-hour meetings, with the last meeting occurring 2 weeks after the fifth meeting due to the timing of the university’s spring break. Workshop participants completed the posttest measures at the end of the final meeting, and wait-list control participants completed the posttest measures during that same week.
Interventions
Mindful Stress Management (MSM)
Based on MBSR (Kabat-Zinn 1990), mindfulness-based cognitive therapy (MBCT; Segal, Williams, and Teasdale 2002), and ACT (Hayes et al. 1999), MSM involved psychoeducation about mindfulness and its relationship to stress (especially stress related to being a student), formal mindfulness meditations and informal mindfulness practice, and discussion about the experience of engaging in this practice. The psychoeducational content of each of the six meetings was focused on a different aspect of mindfulness (being on automatic pilot, a focus on the present moment, acceptance, thoughts are not facts, compassion and engaging in positive activities, and reviewing progress and planning for the future). For homework, students were asked to incorporate mindfulness principles into their day-to-day lives (informal mindfulness) and to practice formal mindfulness meditations daily. Informal mindfulness cues and practices (e.g., mindful walking, eating, attending to lectures, listening to music) were suggested by the co-leaders as well as by the participants. The amount of prescribed daily meditation time was set at 10–15 minutes after the first meeting and increased to 30 minutes daily by the fifth week. Handouts on the main points of the psychoeducational content, instructions for formal meditation, and the assigned homework were distributed at the end of each session. Students discussed their experience of home practice and received feedback from the group leaders at the beginning of sessions 2 through 6.
Mindful Stress Management-Informal
Mindful Stress Management-Informal (MSM-I) included the same psychoeducational content that was presented in MSM, but did not include extended formal mindfulness meditation practice during sessions and homework. Instead, students engaged in multiple brief mindfulness and acceptance exercises (lasting for no more than 5 minutes each) designed to demonstrate the same concepts as the extended formal meditations. These mindfulness exercises were drawn primarily from ACT (Hayes et al. 1999) and Metacognitive Therapy (Wells 2009), or were developed by the first author. As examples, participants learned to acknowledge thoughts without getting caught up in or further analyzing them through metacognitive therapy’s “free association task,” which involves allowing the mind to roam freely in response to various words being read aloud. The idea that thoughts are not facts was taught, in part, by ACT’s “bad cup metaphor.” The time spent engaging in and discussing mindfulness exercises was equivalent to that in MSM. After students engaged in the exercises, they were encouraged to discuss their experiences. For homework, participants were asked to incorporate the principles of mindfulness learned during the meetings into their day-to-day lives through informal mindfulness practice. At the end of each session, participants received the same handouts as the MSM group on the main points of the psychoeducational content, along with a handout of the assigned homework. Students discussed their experience of home practice and received feedback from the group leaders at the beginning of sessions 2 through 6.
Therapists
Both MSM and MSM-I programs were co-led by the same two group leaders. One co-leader (the first author) was an advanced doctoral student in clinical psychology with formal training facilitating DBT skills groups, experience attending an MBSR program, and 5 years of experience using mindfulness concepts in working with clients. The other co-leader had 4 years of experience teaching mindfulness meditation at a meditation center and a daily mindfulness meditation practice for 10 years.
Measures
Background Questionnaire
Questions on the Background Questionnaire (BQ) ask for demographic information about gender, age, academic year or program, and race/ethnicity. Additionally, three items inquire about previous experience with meditation, yoga, or similar contemplative activities, including how many minutes per week they currently practice.
Five Facet Mindfulness Questionnaire
The Five Facet Mindfulness Questionnaire (FFMQ) (Baer, Smith, Hopkins, Krietemeyer, and Toney 2006) consists of 39 items and measures mindfulness on 5-point Likert scales from 1 (Never or Very Rarely True) to 5 (Very Often or Always True). In addition to a total mindfulness score, five subscale scores can be calculated: observing, describing, acting with awareness, non-judging of inner experience, and non-reactivity to inner experience. The FFMQ demonstrates acceptable internal consistency as well as acceptable convergent and discriminant validity (Baer et al. 2006).
Mindful Attention Awareness Scale
The Mindful Attention Awareness Scale (MAAS) (K. W. Brown and Ryan 2003) is a 15-item measure of dispositional mindfulness, with items rated on a 6-point scale from 1 (Almost Always) to 6 (Almost Never). This measure reflects a single factor of attention to and awareness of what is occurring in the present moment. Excellent test-retest reliability, good internal consistency, and good convergent and discriminant validity have been found with the MAAS (K. W. Brown and Ryan 2003).
Acceptance and Action Questionnaire-II
The 7-item Acceptance and Action Questionnaire-II (AAQ-II) (Bond et al. 2011) measures psychological inflexibility and experiential avoidance, with items rated on a 7-point Likert scale from 1 (Never true) to 7 (Always true). The AAQ-II demonstrates high test-retest reliability and good predictive, convergent, and discriminant validity (Bond et al. 2011).
Experiences Questionnaire
The Experiences Questionnaire (EQ) (Fresco et al. 2007) is a 20-item self-report measure of decentering. The items are rated on a scale from 1 (Never) to 5 (All the time), and assess the degree to which individuals are able to recognize that thoughts and feelings are transient, objective events, and not necessarily true reflections of the self. Acceptable reliability and convergent and discriminant validity have been demonstrated (Fresco et al. 2007).
Self-Compassion Scale
The 26-item Self-Compassion Scale (SCS) (Neff 2003) assesses six different aspects of self-compassion, with items rated on a 5-point scale from 1 (Almost never) to 5 (Almost always). The total self-compassion score was used in the present study. The SCS has good internal consistency, and the total score exhibits high convergent and discriminant validity (Neff 2003).
Depression, Anxiety, and Stress Scales
The Depression, Anxiety, and Stress Scales (DASS21) (Henry and Crawford 2005) is a 21-item self-report instrument designed to assess the severity of depression, anxiety, and stress over the past week on a 4-point scale from 0 (Did not apply to me at all) to 3 (Applied to me very much, or most of the time). The DASS21 demonstrates high reliability and good convergent validity with other measures of anxiety and depression (Henry and Crawford 2005).
Ruminative Response Scale
The 22-item Ruminative Response Scale (RRS) is a subscale of the Response Styles Questionnaire (RSQ; Nolen-Hoeksema and Morrow 1991), and assesses rumination in response to feelings and symptoms of dysphoria. Items are rated on a scale from 1 (almost never) to 4 (almost always). The RRS is considered a reliable and valid measure of rumination (Luminet 2004).
Penn State Worry Questionnaire
The Penn State Worry Questionnaire (PSWQ) (Meyer, Miller, Metzger, and Borkovec 1990) was designed to measure the trait of pathological worry in both clinical and non-clinical populations. The 16 items assess the generality, excessiveness, and uncontrollability of worry and are rated on a scale from 1 (Not at all typical) to 5 (Very typical). The PSWQ exhibits good internal consistency as well as convergent and discriminant validity (T. A. Brown, Antony, and Barlow 1992; Meyer et al. 1990).
Fordyce Emotions Questionnaire
The Fordyce Emotions Questionnaire (FEQ) (Fordyce 1988) is a 2-item measure of overall mood. The first item, which asks about the person’s general level of happiness ranging from 0 (Extremely unhappy) to 10 (Extremely happy), was used in the present study. Good test-retest reliability and strong convergent and discriminatory validity with well-being and happiness measures are demonstrated by the FEQ (Fordyce 1988).
Satisfaction With Life Scale
The 5-item Satisfaction With Life Scale (SWLS) (Diener, Emmons, Larsen, and Griffin 1985) is a measure of global life satisfaction; items are rated on a 7-point scale from 1 (strongly disagree) to 7 (strongly agree). The SWLS has exhibited good psychometric properties (Pavot, Diener, Colvin, and Sandvik 1991).
Credibility/Expectancy Questionnaire
The Credibility/Expectancy Questionnaire (CEQ) (Devilly and Borkovec 2000) consists of six items and measures perceived treatment credibility and expectancies of improvement after treatment. The CEQ was administered at the end of the first workshop session. The CEQ demonstrates good test-retest reliability, high internal consistency, and stable factors across multiple populations (Devilly and Borkovec 2000).
Daily Formal Mindfulness Log (MSM group only)
Used by Kaufman, Glass, and Arnkoff (2009) and adapted from the Homework Record Form (Segal et al. 2002), this measure asks for a daily record of the number of minutes of formal mindfulness meditation practice, including any comments about this experience that they want to discuss during the next session.
Daily Informal Mindfulness Log (MSM-I group only)
This daily log records the extent to which informal mindfulness meditation is practiced. Specifically, participants record the extent to which they used informal mindfulness skills each day on a 10-point scale from 1 (Not at All) to 10 (To a Great Extent), along with comments for future discussion.
Evaluation of Mindfulness Workshop Form
The Evaluation of Mindfulness Workshop Form (EMWF), adapted from the Evaluation of Therapy Form (Gershefski, Arnkoff, Glass, and Elkin 1996; Levy, Glass, Arnkoff, Gershefski, and Elkin 1996) and the CEQ (Devilly and Borkovec 2000), consists of seven open-ended questions about aspects of the program that were perceived as helpful or problematic, and how it was successful (or unsuccessful) in helping with stress management and learning to be mindful. Additional Likert rating scales ask about the degree of difficulty participants experienced both doing and finding time for the weekly homework assignments and applying the concepts presented in the workshops to their daily lives, how logical the workshop was, the degree of success and percentage of improvement in reducing stress, the level of confidence in recommending the workshop to a friend, and the usefulness of each of the topics that were the main focus of the six workshop meetings. The EMWF was administered at the end of the final session of both the MSM and MSM-I workshops.
Results
Baseline Differences Between Groups
ANOVA and chi-square analyses were used to determine if there were between-group differences in gender, age, degree program, ethnic background, previous experience in contemplative activities, and time spent meditating (see Table 1). There was a significant between-groups difference only for degree program, but not age: the wait-list control consisted of more graduate students (8 graduate, 2 undergraduate), while MSM and MSM-I were comprised of a greater number of undergraduate students (MSM: 11 undergraduate, 2 graduate; MSM-I: 6 undergraduate, 5 graduate). Similarly, ANOVAs to determine if the three groups differed on any pretest measures revealed only one significant difference, on the depression, anxiety, and stress (DASS) anxiety scale, F (2, 31) = 3.87, p = 0.03. Tukey tests showed that the wait-list control group reported less anxiety (M = 4.00, SD = 2.11) than either the MSM (M = 12.46, SD = 9.91) or MSM-I (M = 9.45, SD = 6.46) groups, which did not differ from each other.
Attrition and Attendance
All 34 participants in the MSM, MSM-I, and wait-list control groups completed the posttest measures. The 24 participants in the intervention groups all met criteria for completer status because they attended at least four sessions, with 37.5 % attending all six, 45.8 % five sessions, and 16.7 % four sessions. There was also no significant difference in the average number of sessions attended between MSM (M = 5.46) and MSM-I (M = 4.91), t (22) = 1.99, p = 0.06.
Intervention Credibility and Expectancy
There was no difference between MSM (M = 22.69) and MSM-I (M = 20.64) on intervention credibility on the CEQ, t (22) = 1.34, p = 0.19. Similarly, the MSM group (M = 23.97) did not differ from MSM-I (M = 19.37) on outcome expectations, t (22) = 1.96, p = 0.06.
Were there Within-Group Changes in Outcomes?
Paired-samples t-tests were performed in order to determine if there were significant changes in outcome variables, and pretest and posttest means and within-group effect sizes from the two intervention groups are presented in Tables 2 and 3. Both intervention groups demonstrated significant increases in the FFMQ total score and several FFMQ facets (observing, non-judging of inner experience, non-reactivity to inner experience), decentering (EQ), and self-compassion (SCS total score), and decreases in stress (DASS21), depression (DASS21), rumination (RRS total score), and worry (PSWQ). All effect sizes were large for MSM and medium to large for MSM-I, and the MSM group had larger effect sizes than MSM-I on most measures.
Additionally, MSM participants reported significant increases in mindfulness on additional FFMQ facets (describing, act with awareness) and the MAAS, general level of happiness (FEQ), and satisfaction with life (SWLS), and decreases in psychological inflexibility (AAQ-II) and anxiety (DASS21), and showed medium to large effect sizes. The wait-list control group showed change on only two variables: a significant increase in the FFMQ describing subscale and decrease in rumination (RRS total score).
Did Outcomes Differ Between Groups?
Between-group comparisons of change were accomplished through a series of MANCOVAs, using respective pretest scores as the covariates. Variables from significant MANCOVAs were further analyzed using ANCOVAs and Tukey tests. Between-group effect sizes were calculated by comparing change scores and are presented in Table 3. FFMQ total score was analyzed in a separate ANCOVA, as was the stress subscale of the DASS21, because stress was a main focus of the study.
MANCOVAs were found to be significant for mindfulness (the FFMQ subscales and MAAS: F (12, 42) = 2.00, p = 0.05) and mindfulness-related variables (AAQ-II, EQ, SCS: F (6, 54) = 3.78, p = 0.003), but not significant for anxiety (DASS anxiety, PSWQ), depression (DASS depression, RRS), or positive mood variables (FEQ, SWLS). In comparison to the wait-list control group, both intervention groups demonstrated significantly higher scores on the FFMQ observe facet, and a greater degree of self-compassion (SCS total score), with effect sizes ranging from medium to large and favoring MSM. Additionally, MSM participants showed significantly higher FFMQ total and non-reactivity to inner experience scores, decentering (EQ), and less reported stress than the control group. All effect sizes were large. In comparing the two intervention groups, all significant differences favored MSM, where participants demonstrated less psychological inflexibility (AAQ-II), more self-compassion (SCS total score), and less stress after the workshop than did MSM-I participants. Effect sizes were in the medium range.
Did Mindfulness or other Variables Mediate Changes in Stress?
As in Gaudiano, Herbert, and Hayes (2010), simple mediational analyses were conducted with a non-parametric, bootstrapping approach (Preacher and Hayes 2004) that measured mediation and outcome variables at the same time point. This approach has been recommended as the preferred method for analyzing mediators in small sample sizes (MacKinnon, Lockwood, and Williams 2004; Shrout and Bolger 2002). The bootstrapping approach was bias-corrected and accelerated, and used 5,000 resamples to compute 95 % confidence intervals for the indirect effect of group (MSM vs. control, MSM-I vs. control, MSM and MSM-I combined vs. control) on reductions in stress through change of the potential mediators (mindfulness, worry, rumination, psychological inflexibility, self-compassion, and decentering). The indirect effect is significant when the interval between the lower and upper limits does not include zero. Change scores were derived by subtracting pretest from posttest scores for variables expected to increase, and subtracting posttest from pretest scores on variables hypothesized to decrease for the intervention groups.
For the MSM group, increases in one facet of mindfulness (FFMQ non-reactivity to inner experiences: lower limit = 0.01, upper limit = 9.73) mediated decreases in stress. Additionally, increased self-compassion (SCS total score: lower limit = 0.41, upper limit = 13.05) and decreased worry (PSWQ: lower limit = 1.24, upper limit = 9.55) also mediated decreases in stress. No significant mediators were found to decrease stress for MSM-I. When data from both interventions were combined, decreased worry (lower limit = 0.56, upper limit = 7.60) was the only significant mediator for decreases in stress.
Because multiple variables were significant mediators between MSM and decreases in stress, these significant mediators were analyzed as a multiple mediator model using a bias-corrected and accelerated bootstrapping approach with 5,000 resamples (Preacher and Hayes 2008). FFMQ non-reactivity to inner experiences, worry, and self-compassion together significantly mediated decreases in stress (lower limit = 0.99, upper limit = 15.53). No individual mediator reached significance, which indicates that one mediator alone did not contribute to the indirect effect above and beyond the other mediators. Likewise, there was no significant difference between the strength of any of the mediators.
Was Mindfulness Practice Related to Changes in Mindfulness and Psychological Distress?
An average weekly formal meditation time score for each MSM participant was calculated by summing the number of minutes spent meditating each week and dividing the total meditation time by the number of home practice logs completed. MSM participants formally meditated during the workshop for an average of 69.72 minutes per week (SD = 31.85, range = 25.83−125.00). Pearson correlation coefficients showed no significant relations between time spent formally meditating and changes in any measure of mindfulness (MAAS, FFMQ total score, or FFMQ facets) or psychological distress (stress, anxiety, or depression).
An average weekly informal mindfulness score for each MSM-I participant was calculated by summing the weekly practice ratings and dividing by the number of logs completed. The weekly average for MSM-I participants was 4.86 out of 10 (SD = 1.21, range = 3.05–6.62). No relations were found between informal practice of mindfulness principles and changes in measures of mindfulness (MAAS, FFMQ total score, or FFMQ facets) or psychological distress.
Did Post-Workshop Evaluations Differ Between Groups?
Independent samples t-tests revealed that MSM participants anticipated continued practice of workshop exercises to a greater extent than did MSM-I participants, t (20) = 2.91, p = 0.009, and also rated their workshop as seeming more logical, t (20) = 3.91, p = 0.001. Furthermore, students who attended the MSM workshop reported more success at reducing stress, t (20) = 3.70, p = 0.001, as well as a greater percentage of improvement in stress level, t (20) = 2.32, p = 0.03. When asked to rate the usefulness of the workshops’ main topics in learning to be mindful and reducing stress, MSM participants rated the topics of being on automatic pilot, t (19) = 2.55, p = 0.02, and acceptance, t (19) = 2.63, p = 0.02, as being more useful compared to MSM-I participants’ ratings of these topics.
Discussion
Both interventions were effective in reducing stress for university students, but results demonstrated the superiority of MSM over MSM-I. MSM participants recorded significant within-group changes on all 17 measures, and 6 between-group differences when compared to the wait-list (FFMQ total and observe and non-reactivity to inner experience subscales, EQ, SCS total, DASS21 stress). In contrast, MSM-I participants exhibited within-group changes on 10 measures (FFMQ total, and observe, non-judging of inner experience, and non-reactivity to inner experience subscales, EQ, SCS total, DASS21 stress and depression, RRS total, PSWQ), and on 2 measures in comparison to the wait-list control (SCS total and the observe facet of the FFMQ). Additionally, all significant differences between interventions (AAQ-II, SCS total, DASS21 stress) favored MSM participants.
Because increases in mindfulness have shown to mediate decreases in stress (Shapiro et al. 2008), a main goal of the present research was to determine the most effective method for cultivating mindfulness. This study was the first to directly compare mindfulness-based interventions for stress that teach mindfulness with and without formal mindfulness meditations. MSM participants reported significant increases on both mindfulness measures, while students in MSM-I only demonstrated increases on the FFMQ. On the FFMQ total score and subscales that increased significantly for both interventions, MSM also exhibited larger effect sizes. As the only difference between MSM and MSM-I was the method used to teach mindfulness (with identical didactic psychoeducational content in both workshops), using formal meditations may thus be more effective at cultivating mindfulness. Future studies should be conducted to confirm these results, which might be specific to only the interventions developed for the present study. For instance, other mindfulness-based interventions that include formal mindfulness meditations (e.g., MBSR) could be directly compared to those that do not, such as ACT. It may also be useful to add formal meditations to interventions that do not already include them in order to determine if outcomes can be improved upon.
Kabat-Zinn (1990) states that formal meditation practice is essential for cultivating mindfulness, and meditation may allow individuals the opportunity to experience being mindful at times of low stress so that it becomes easier to be mindful when stress is elevated (Miller et al. 1995). It has also been suggested that formal meditations create a context in which minor distressing stimuli are produced, allowing one to see language from a decentered perspective (i.e., recognizing thoughts and feelings as transient events) and to practice acceptance (Hayes and Shenk 2004; Williams 2008).
MSM participants’ responses on the program evaluation questionnaire confirmed the importance of formal mindfulness meditations, in that 12 of 13 students (92 %) mentioned the meditations as being a helpful aspect of the workshop. When asked what was difficult about home practice, 8 of the 11 MSM-I participants (73 %) mentioned having trouble remembering to practice compared to only 1 MSM participant. Accordingly, daily formal meditative practice may be more effective at cultivating mindfulness because it provides more structure for the use of mindfulness skills. It may be that adding daily reminders for informal mindfulness practice (e.g., by using smartphone technology) would improve outcomes.
In addition to mindfulness, MSM participants exhibited significantly greater increases in all three mindfulness-related variables (psychological inflexibility, decentering, and self-compassion), with the latter two differing significantly from the wait-list. Previous research has also demonstrated the ability of mindfulness-based interventions incorporating formal mindfulness meditations to decrease psychological inflexibility and increase decentering and self-compassion (Bieling et al. 2012; Birnie, Speca, and Carlson 2010; Roemer and Orsillo 2007).
In comparison, MSM-I participants demonstrated significant within-group changes on two of three mindfulness-related variables (decentering and self-compassion), and only self-compassion was significantly different from the wait-list. The present study is the first to measure decentering in a mindfulness-based intervention that does not include formal mindfulness meditation, and future studies of similar interventions, especially ACT, could benefit from including an assessment of decentering. In fact, one goal of ACT is to gain distance from thoughts (cognitive defusion), a construct similar to decentering. While self-compassion significantly increased in MSM-I, perhaps because the workshop contains didactic information and an exercise designed to enhance self-compassion, previous studies of ACT have not found a significant increase (Stafford-Brown and Pakenham 2012). Conversely, although psychological inflexibility (AAQ-II) did not significantly decrease for students in MSM-I, ACT interventions that teach mindfulness through similar methods have produced significant improvement (e.g., Forman, Herbert, Moitra, Yeomans, and Geller 2007; Morton et al. 2012). These ACT interventions consisted of more sessions (12–15) than the 6-session workshop in the present study, suggesting that mindfulness-based treatments without formal mindfulness meditations may need to be longer to produce significant change in psychological inflexibility. Alternatively, although MSM-I is similar to ACT in its use of brief mindfulness exercises and informal practice, they should not be considered comparable, as ACT includes topics (e.g., self as context, willingness) not included in MSM-I.
Similar to research on the efficacy of other mindfulness-based interventions (Mazzucchelli, Rees, and Kane 2009; van Aalderen et al. 2012), MSM participants improved significantly in anxiety, worry, satisfaction with life, and happiness, and both interventions led to significant change in depression and rumination. Anxiety and satisfaction with life have been shown to change in ACT interventions (Forman et al. 2007; Thorsell et al. 2011), so that the small sample size and shorter length of treatment in the MSM-I workshop may have contributed to these non-significant results. Additionally, MSM-I participants reported a lower, although not statistically significant, pretest level of anxiety compared to MSM participants, which may have limited the degree to which it could decrease; in fact, both groups had similar means at posttest.
Both stress reduction workshops resulted in significant within-group reductions in stress, demonstrating the effectiveness of shorter mindfulness-based programs for a student population. Nevertheless, MSM participants exhibited greater reductions in stress compared to both the wait-list control and MSM-I. In order to determine which variables were responsible for decreases in stress, potential mediators were examined. All mediational variables, with the exception of rumination, had larger effect sizes for MSM participants. Mindfulness (non-reactivity to inner experience), self-compassion, and worry together mediated reduction in stress for MSM participants, with no one variable significantly contributing more than another. Studies have similarly found that increases in mindfulness mediated reductions in perceived stress as a result of MBSR (Nyklíček and Kuijpers 2008; Shapiro et al. 2008); however, no other process variables were concurrently examined as mediators. When studying changes in depression, previous mindfulness-based intervention research has also found mindfulness to be a significant mediator, in addition to self-compassion, worry, and rumination (Kuyken et al. 2010; van Aalderen et al. 2012). In contrast to MSM, no variable significantly mediated reductions in stress for MSM-I. The lack of a significant mediator may have been influenced by a combination of smaller pretest-to-posttest changes in stress and mediational variables, as well as low statistical power due to the small sample size. More mindfulness-based intervention research should examine the influence of mediators other than mindfulness. If certain variables consistently mediate reductions in psychological distress, treatments could be tailored to emphasize them.
Measures of mindfulness practice such as minutes spent meditating each day (Daily Formal Mindfulness Log) and ratings of the extent to which informal mindfulness skills were used each day (Daily Informal Mindfulness Log) were not significantly related to increases in mindfulness or decreases in stress, anxiety, or depression. Findings have been inconsistent regarding whether mindfulness practice (formal and informal) is associated with changes in mindfulness and psychological symptoms (Carmody and Baer 2008; Perich, Manicavasagar, Mitchell, and Ball 2013; Shapiro et al. 2008; Vettese, Toneatto, Stea, Nguyen, and Wang 2009). While some studies (e.g., Jha, Stanley, Kiyonaga, Wong, and Gelfand 2010) found a dose-related response to out-of-class time practicing formal mindfulness exercises, other non-significant results have been attributed to factors such as initial low levels of distress and ceiling effects for the amount of practice (Carlson, Speca, Patel, and Goodey 2003), as well as statistical power (Nyklíček and Kuijpers 2008). Power was likely a factor in the present study, where a large correlation between formal practice and FFMQ act with awareness (r = 0.50) did not reach significance. If time spent formally meditating does not influence outcomes, mindfulness interventions could reduce the recommended practice time and thus potentially attract and retain individuals who might not be willing to meditate for 45 minutes daily.
There are several other limitations to the present study. In addition to the small sample size, not all of the participants could be randomly assigned to groups, which increased the likelihood of the conditions not being equivalent at pretest. However, although individuals in the control group reported being less anxious than workshop participants and were more likely to be in graduate school, groups were not significantly different on any other demographic or psychological variable. Another limitation was the restricted demographic range of the sample in that most students were female, Caucasian, and in their 20s, so that results may not be able generalizable to other populations. Future studies should compare MSM and MSM-I with more diverse or clinical samples. It should also be noted that although MSM participants were instructed in informal mindfulness practices, they were not asked to complete the Daily Informal Mindfulness Log, in order for both groups to complete one daily measure. Information is thus not available on how informal practice in the MSM group was related to outcomes. Future studies of interventions including both formal and informal mindfulness instruction may benefit from using logs of both formal and informal mindfulness practice.
Overall, the present study represents an important first step in determining if certain methods used in teaching mindfulness are more effective than others. Results suggest that an intervention with formal mindfulness meditations and informal practice led to better outcomes than one using brief mindfulness exercises and informal practice. Outcomes in both groups were promising, however, adding to evidence that mindfulness-based programs can play an important role in helping students manage stress.
References
American College Health Association. (2004). American College Health Association-National College Health Assessment (ACHA-NCHA) spring 2004 reference group data report (abridged). Journal of American College Health, 54, 201–211.
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13, 27–45.
Bieling, P. J., Hawley, L. L., Bloch, R. T., Corcoran, K. M., Levitan, R. D., Young, L. T., & Segal, Z. V. (2012). Treatment-specific changes in decentering following mindfulness-based cognitive therapy versus antidepressant medication or placebo for prevention of depressive relapse. Journal of Consulting and Clinical Psychology, 80, 365–372.
Birnie, K., Speca, M., & Carlson, L. E. (2010). Exploring self-compassion and empathy in the context of mindfulness-based stress reduction (MBSR). Journal of the International Society for the Investigation of Stress, 26, 359–371.
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., & Devins, G. (2004). Mindfulness: a proposed operational definition. Clinical Psychology: Science and Practice, 11, 230–241.
Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K., & Zettle, R. D. (2011). Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Behavior Therapy, 42, 676–688.
Britz, J., & Pappas, E. (2010). Sources and outlets of stress among university students: Correlations between stress and unhealthy habits. Undergraduate Research Journal for the Human Sciences, 9. Retrieved from http://www.kon.org/urc/v9/britz.html.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: the role of mindfulness in psychological well-being. Journal of Personality and Social Psychology, 84, 822–848.
Brown, T. A., Antony, M. M., & Barlow, D. H. (1992). Psychometric properties of the Penn State Worry Questionnaire in a clinical anxiety disorder sample. Behaviour Research and Therapy, 30, 33–37.
Carlson, L. E., Speca, M., Patel, K. D., & Goodey, E. (2003). Mindfulness-based stress reduction in relation to quality of life, mood, symptoms of stress, and immune parameters in breast and prostate cancer outpatients. Psychosomatic Medicine, 65, 571–581.
Carmody, J., & Baer, R. A. (2008). Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. Journal of Behavioral Medicine, 31, 23–33.
Cavanagh, K., Strauss, C., Cicconi, F., Griffiths, N., Wyper, A., & Jones, F. (2013). A randomised controlled trial of a brief online mindfulness-based intervention. Behaviour Research and Therapy, 51, 573–576.
Chang, V. Y., Palesh, O., Caldwell, R., Glasgow, N., Abramson, M., Luskin, F., & Koopman, C. (2004). The effects of a mindfulness-based stress reduction program on stress, mindfulness self-efficacy, and positive states of mind. Stress and Health, 20, 141–147.
Chiesa, A., & Serretti, A. (2009). Mindfulness-based stress reduction for stress management in healthy people: a review and meta-analysis. The Journal of Alternative and Complementary Medicine, 15, 593–600.
Devilly, G. J., & Borkovec, T. D. (2000). Psychometric properties of the Credibility/Expectancy Questionnaire. Journal of Behavior Therapy and Experimental Psychiatry, 31, 73–86.
Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49, 71–75.
Fledderus, M., Bohlmeijer, E. T., Pieterse, M. E., & Schreurs, K. M. G. (2012). Acceptance and commitment therapy as guided self-help for psychological distress and positive mental health: a randomized controlled trial. Psychological Medicine, 42, 485–495.
Fordyce, M. (1988). A review of research on the happiness measures: a sixty second index of happiness and mental health. Social Indicators Research, 20, 355–381.
Forman, E. M., Herbert, J. D., Moitra, E., Yeomans, P. D., & Geller, P. A. (2007). A randomized controlled effectiveness trial of acceptance and commitment therapy and cognitive therapy for anxiety and depression. Behavior Modification, 31, 772–799.
Fresco, D. M., Moore, M. T., van Dulmen, M. H. M., Segal, Z. V., Ma, S. H., Teasdale, J. D., & Williams, J. M. G. (2007). Initial psychometric properties of the Experiences Questionnaire: validation of a self-report measure of decentering. Behavior Therapy, 38, 234–246.
Gaudiano, B. A., Herbert, J. D., & Hayes, S. C. (2010). Is it the symptom or the relation to it? Investigating potential mediators of change in acceptance and commitment therapy for psychosis. Behavior Therapy, 41, 543–554.
Gershefski, J. J., Arnkoff, D. B., Glass, C. R., & Elkin, I. (1996). Clients’ perceptions of treatment for depression: I. helpful aspects. Psychotherapy Research, 6, 233–247.
Hawley, L. L., Schwartz, D., Bieling, P. J., Irving, J., Corcoran, K., Farb, N. A. S., & Segal, Z. V. (2014). Mindfulness practice, rumination, and clinical outcome in mindfulness-based treatment. Cognitive Therapy and Research, 38, 1–9.
Hayes, S. C., & Shenk, C. (2004). Operationalizing mindfulness without unnecessary attachments. Clinical Psychology: Science and Practice, 11, 249–254.
Hayes, S. C., Strosahl, K., & Wilson, K. G. (1999). Acceptance and commitment therapy: an experiential approach to behavior change. New York: Guilford Press.
Henry, J. D., & Crawford, J. R. (2005). The short form version of the Depression Anxiety Stress Scales (DASS-21): construct validity and normative data in a large non-clinical sample. British Journal of Clinical Psychology, 44, 227–239.
Hofmann, S. G., Sawyer, A. T., Witt, A. A., & Oh, D. (2010). The effect of mindfulness-based therapy on anxiety and depression: a meta-analytic review. Journal of Consulting and Clinical Psychology, 78, 169–183.
Hong, P. Y. (2004). Dialectic behavior therapy for borderline personality disorder: a component analysis of DBT skills training group (Doctoral dissertation, University of Kansas). Dissertation Abstracts International, 64, 4039.
Jain, S., Shapiro, S. L., Swanick, S., Roesch, S. C., Mills, P. J., Bell, I., & Schwartz, G. E. R. (2007). A randomized controlled trial of mindfulness meditation versus relaxation training: effects on distress, positive states of mind, rumination, and distraction. Annals of Behavioral Medicine, 33, 11–21.
Jha, A. P., Stanley, E. A., Kiyonaga, A., Wong, L., & Gelfand, L. (2010). Examining the protective effects of mindfulness training on working memory capacity and affective experience. Emotion, 10, 54–64.
Kabat-Zinn, J. (1982). An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. General Hospital Psychiatry, 4, 33–47.
Kabat-Zinn, J. (1990). Full catastrophe living: using the wisdom of your body and mind to face stress, pain and illness. New York: Dell.
Kaufman, K. A., Glass, C. R., & Arnkoff, D. B. (2009). Evaluation of mindful sport performance enhancement (MSPE): a new approach to promote flow in athletes. Journal of Clinical Sport Psychology, 3, 334–356.
Klatt, M. D., Buckworth, J., & Malarkey, W. B. (2009). Effects of low-dose mindfulness-based stress reduction (MBSR-ld) on working adults. Health Education and Behavior, 36, 601–614.
Kuyken, W., Watkins, E., Holden, E., White, K., Taylor, R. S., Byford, S., & Dalgleish, T. (2010). How does mindfulness-based cognitive therapy work? Behaviour Research and Therapy, 48, 1105–1112.
Levy, J. A., Glass, C. R., Arnkoff, D. B., Gershefski, J. J., & Elkin, I. (1996). Clients’ perceptions of treatment for depression: II. problematic or hindering aspects. Psychotherapy Research, 6, 249–262.
Linehan, M. M. (1993). Skills training manual for treating borderline personality disorder. New York: Guilford Press.
Luminet, O. (2004). Measurement of depressive rumination and associated constructs. In C. Papageorgiou & A. Wells (Eds.), Depressive rumination. Nature, theory, and treatment (pp. 187–215). Chichester: Wiley.
MacKinnon, D. P., Lockwood, C. M., & Williams, J. (2004). Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivariate Behavioral Research, 39, 99–128.
Mazzucchelli, T. G., Rees, C. S., & Kane, R. T. (2009). Group behavioural activation and mindfulness therapy for the well-being of non-clinical adults: a preliminary open trial. The Cognitive Behaviour Therapist, 2, 256–271.
Meyer, T. J., Miller, M. L., Metzger, R. L., & Borkovec, T. D. (1990). Development and validation of the Penn State Worry Questionnaire. Behaviour Research and Therapy, 28, 487–495.
Miller, J. J., Fletcher, K., & Kabat-Zinn, J. (1995). Three-year follow-up and clinical implications of a mindfulness meditation-based stress reduction intervention in the treatment of anxiety disorders. General Hospital Psychiatry, 17, 192–200.
Morton, J., Snowdon, S., Gopold, M., & Guymer, E. (2012). Acceptance and commitment therapy group treatment for symptoms of borderline personality disorder: a public sector pilot study. Cognitive and Behavioral Practice, 19, 527–544.
Neff, K. D. (2003). Development and validation of a scale to measure self-compassion. Self and Identity, 2, 223–250.
Nolen-Hoeksema, S., & Morrow, J. (1991). A prospective study of depression and posttraumatic stress symptoms after a natural disaster: the 1989 Loma Prieta earthquake. Journal of Personality and Social Psychology, 61, 115–121.
Nyklíček, I., & Kuijpers, K. F. (2008). Effects of mindfulness-based stress reduction intervention on psychological well-being and quality of life: is increased mindfulness indeed the mechanism? Annals of Behavioral Medicine, 35, 331–340.
Pavot, W., Diener, E., Colvin, C. R., & Sandvik, E. (1991). Further validation of the Satisfaction with Life Scale: evidence for the cross-method convergence of well-being measures. Journal of Personality Assessment, 57, 149–161.
Perich, T., Manicavasagar, V., Mitchell, P. B., & Ball, J. R. (2013). The association between meditation practice and treatment outcome in mindfulness-based cognitive therapy for bipolar disorder. Behaviour Research and Therapy, 51, 338–343.
Preacher, K. J., & Hayes, A. F. (2004). SPSS and SAS procedures for estimating indirect effects in simple mediational models. Behavior Research Methods, Instruments, & Computers, 36, 717–731.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40, 879–891.
Roemer, L., & Orsillo, S. M. (2007). An open trial of an acceptance-based behavior therapy for generalized anxiety disorder. Behavior Therapy, 38, 72–85.
Ross, S. E., Niebling, B. C., & Heckert, T. M. (1999). Sources of stress among college students. College Student Journal, 33, 312–317.
Schneiderman, N., Ironson, G., & Siegel, S. D. (2005). Stress and health: psychological, behavioral, and biological determinants. Annual Review of Clinical Psychology, 1, 607–628.
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2002). Mindfulness-based cognitive therapy for depression: a new approach to preventing relapse. New York: Guilford Press.
Shapiro, S. L., Schwartz, G. E., & Bonner, G. (1998). Effects of mindfulness-based stress reduction on medical and premedical students. Journal of Behavioral Medicine, 21, 581–599.
Shapiro, S. L., Astin, J. A., Bishop, S. R., & Cordova, M. (2005). Mindfulness-based stress reduction for health care professionals: results from a randomized trial. International Journal of Stress Management, 12, 164–176.
Shapiro, S. L., Oman, D., Thoresen, C. E., Plante, T. G., & Flinders, T. (2008). Cultivating mindfulness: effects on well-being. Journal of Clinical Psychology, 64, 840–862.
Shapiro, S. L., Brown, K. W., Thoresen, C. E., & Plante, T. G. (2011). The moderation of mindfulness-based stress reduction effects by trait mindfulness: results from a randomized controlled trial. Journal of Clinical Psychology, 67, 267–277.
Shrout, P. E., & Bolger, N. (2002). Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychological Methods, 7, 422–445.
Stafford-Brown, J., & Pakenham, K. I. (2012). The effectiveness of an ACT informed intervention for managing stress and improving therapist qualities in clinical psychology trainees. Journal of Clinical Psychology, 68, 592–613.
Thorsell, J., Finnes, A., Dahl, J., Lundgren, T., Gybrant, M., Gordh, T., & Buhrman, M. (2011). A comparative study of 2 manual-based self-help interventions, acceptance and commitment therapy and applied relaxation, for persons with chronic pain. The Clinical Journal of Pain, 27, 716–723.
Toews, J. A., Lockyer, J. M., Dobson, D. J., & Brownell, A. K. (1993). Stress among residents, medical students, and graduate science students. Academic Medicine, 68, S46–S48.
van Aalderen, J. R., Donders, A. R. T., Giommi, F., Spinhoven, P., Barendregt, H. P., & Speckens, A. E. M. (2012). The efficacy of mindfulness-based cognitive therapy in recurrent depression patients with and without a current depressive episode: a randomized controlled trial. Psychological Medicine, 42, 989–1001.
Vettese, L. C., Toneatto, T., Stea, J. N., Nguyen, L., & Wang, J. J. (2009). Do mindfulness meditation participants do their homework? And does it make a difference? A review of empirical evidence. Journal of Cognitive Psychotherapy: An International Quarterly, 23, 198–225.
Vøllestad, J., Sivertsen, B., & Nielsen, G. H. (2011). Mindfulness-based stress reduction for patients with anxiety disorders: evaluation in a randomized controlled trial. Behaviour Research and Therapy, 49, 281–288.
Wells, A. (2009). Metacognitive therapy for anxiety and depression. New York: Guilford Press.
Williams, J. M. G. (2008). Mindfulness, depression, and modes of mind. Cognitive Therapy and Research, 32, 721–733.
Acknowledgments
The authors thank Scott Woodruff for consultation on statistical analyses, Elizabeth Hirschhorn and Megan Wheeler for help with recruiting participants, and Douglas Boyd, Andrea Kulish, Rachel Severino, and Jessica Smith for assistance with data entry.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hindman, R.K., Glass, C.R., Arnkoff, D.B. et al. A Comparison of Formal and Informal Mindfulness Programs for Stress Reduction in University Students. Mindfulness 6, 873–884 (2015). https://doi.org/10.1007/s12671-014-0331-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-014-0331-1