
Abstract
Health literacy represents an increasingly important subject in health sciences. This article initially illustrates a domain-specific model of physical activity-related health competence. Movement competence, control competence, and PA-specific self-regulation competence are described as sub-competencies.
This article further aims to develop and validate a questionnaire for certain aspects of physical activity-related health competence, especially to record control competencies, which have yet to be operationalized. The questionnaire was tested after a pilot study in two study groups: In study A, 1028 persons were interviewed in written form at the beginning of a medical rehabilitation program (female: 44.0 %; Mean (M) age = 53.8 years; Standard Deviation (SD) age = 9.2 years). In study B, 1331 participants in fitness- and health-related programs of the university sports were interviewed via an online questionnaire (female: 83.0 %; Mage = 53.8 years; SDage = 9.7 years).
Exploratory and confirmatory factor analyses show that domain-specific facets can be differentiated for physical activity-related health competence. Furthermore, the results of structural equation modeling analyses provide evidence that control competence is associated not only with the amount of physical activity, but also with motor function. These findings support the assumption that physical activity-related health competence contributes to the health benefits of physical activity. The questionnaire developed in this study thus enhances the possibilities of competence-orientated research within sport-scientific applications in the area of exercise therapy and health sports.
Zusammenfassung
Die Gesundheitskompetenz ist zunehmend Gegenstand gesundheitswissenschaftlicher Arbeiten geworden. Dieser Beitrag stellt zunächst ein bereichsspezifisches Modell der bewegungsbezogenen Gesundheitskompetenz vor. Als Teilkompetenzen werden Bewegungskompetenz, Steuerungskompetenz und Selbstregulationskompetenz beschrieben.
Weitergehend zielt der Beitrag auf die Entwicklung und Validierung eines Erhebungsverfahrens insbesondere für die bisher nicht operationalisierten Steuerungskompetenzen. Das Verfahren wurde nach einer Pilotstudie in zwei Untersuchungsgruppen erprobt: In Studie A wurden 1028 Personen zu Beginn einer Reha-Maßnahme (Anteil Frauen: 44.0 %; MAlter = 53.8 Jahre; SDAlter = 9.2 Jahre) schriftlich befragt. In Studie B wurden 1331 Teilnehmende im Fitness- und Gesundheitssport des Hochschulsports (Anteil Frauen: 83.0 %; MAlter = 53.8 Jahre; SDAlter = 9.7 Jahre) anhand eines Online-Fragebogens erfasst.
Explorative und konfirmatorische Faktorenanalysen ergaben, dass bereichsspezifische Teilkompetenzen für die bewegungsbezogene Gesundheitskompetenz differenziert werden können. Mithilfe von Strukturgleichungsmodellen konnte gezeigt werden, dass die Steuerungskompetenz sowohl Assoziationen mit der Sportaktivität als auch mit dem motorischen Funktionszustand aufweist. Diese Ergebnisse bekräftigen die Annahme, dass bewegungsbezogene Gesundheitskompetenz einen zusätzlichen Beitrag zu Gesundheitswirkungen von körperlich-sportlicher Aktivität leistet. Das Erhebungsverfahren erweitert die Möglichkeiten kompetenzorientierter Forschung für die sportwissenschaftlichen Anwendungsfelder der Bewegungstherapie und des Gesundheitssports.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
In recent years, health literacy within the population has become a major focus of health policy activities (e. g., in the US, Australia, the UK, Switzerland, and Austria; Abel et al. 2011). This development has been based on health sciences research dedicated to clarifying the definitions used, utilizing empirical methods to shed light on the interrelationships between health literacy, health behaviors, and health (e. g., Kickbusch et al. 2013; Sorensen et al. 2012).
Despite a large number of ways of approaching this topic, a common core of health literacy can be defined as persons who, based on their individual knowledge, skills, and abilities, are in a position to make decisions that have a positive effect on their health (e. g., Kickbusch 2006; Soellner et al. 2009). Beyond this common core, there are significant differences in the models used (Sorensen et al. 2012): On the one hand, there is a relatively narrow approach already used in early works on health literacy in the context of the medical care system. Using this approach, health literacy is understood as an individual ability to understand health-related information, which includes finding one’s way around the healthcare system as a patient in an informed manner, and being able to act in line with a physician’s or other therapeutic recommendations (e. g., American Medical Association 1999). On the other hand are health promotion approaches that take a broader view. These approaches see health literacy as the abilities, skills, and willingness required for an active approach to dealing with health information. Health literacy also determines decisions relevant to health and the translation of these decisions into behavior relevant to health in lots of different areas of life (e. g., the working environment, the health system, and personal health in everyday life and during leisure time). Health literacy is thus defined broadly as a personal resource that allows the individual to influence his or her own health in a positive way and promotes active participation in designing healthy ways of living (e. g., Abel et al. 2011).
From a European perspective and the perspective of the German-speaking world, two approaches can be highlighted. These have already been clarified conceptually and have met the diagnostic shortcoming as part of more broadly defined concepts of health literacy. The first approach is the Health Literacy Survey in Europe (HLS-EU), which provides comparative surveys on health literacy in eight European countries (HLS-EU Consortium 2012). The questionnaire HLS-EU-Q47 was developed for this purpose, which aims to present health literacy for the three areas of (medical) health care, disease prevention, and health promotion. The second approach stems from research carried out by a working group headed up by Soellner within the framework of the Priority Program for Competence Models of the “Deutsche Forschungsgemeinschaft” (German Research Foundation, DFG; Soellner et al. 2009; Lenartz 2012). Based on an expert survey, the group developed a questionnaire used to empirically derive a structural model for health literacy (Lenartz 2012).
Furthermore, the concept of health literacy was tackled in different applications of sport-scientific health research. These include a broad range of different applications, from individual-based health promotion and prevention (e. g., as part of health education in physical education at school: Demetriou et al. 2015; Döhring and Gissel 2014; Töpfer and Sygusch 2014) to medical rehabilitation (e. g., Pfeifer et al. 2013).
In the field of rehabilitation, for example, the long-term promotion of health literacy as a general objective of exercise therapy was already planned in the 2007 version of the classification of therapeutic services (“Klassifikation therapeutischer Leistungen”, KTL) by the German pension insurance (DRV Bund 2007). The current version, KTL 2015 (DRV Bund 2014), is explicitly geared to the promotion of physical activity (PA)-related health competence. This should favor the initiation and maintenance of a physically active lifestyle and promote a positive approach to dealing with chronic diseases. Accordingly, promoting PA-related health competence is seen as an important educational task of exercise therapy in medical rehabilitation (Pfeifer et al. 2013).
In the field of individual-based health promotion and prevention, health literacy is discussed based on the core objectives of health sports (Brehm et al. 2005) in connection with the promotion of psychosocial resources. For example, the possibilities for improving mood by means of sport activities and the dissemination of knowledge about the possibilities and effects of PA are viewed as viable options for expanding health literacy (Bürklein 2007, p. 16). Reference is also made to the fact that a differentiated and concrete knowledge of actions and effects is regarded as an important basis for the competent self-realization of health sports activities (Pahmeier and Tiemann 2013, p. 680). Although such psychosocial resources are generally primarily named as factors that promote commitment to health-enhancing PA, there is a suggestion that they can also be viewed as a prerequisite for structuring behavior in a health-competent way.
Although the concept of health literacy is already disseminated in the sport-scientific applications of exercise therapy and health sports, a domain-specific conceptual basis is still in its infancy. Accordingly, there are no validated questionnaires for domain-specific health literacy with which to evaluate competence promotion measures. The questionnaires available to record health literacy do not offer any distinct direction for specific behavioral areas. In the questionnaire from the HLS-EU study group, only one of 47 questions addresses physical activities directly (“How easy would you say it is to … join a sports club or exercise class if you want to?”). Soellner’s working group consciously focuses its self-assessment on healthy literacy facets that are as general as possible, and recommends domain-specific adjustments to its conceptual and empirical work (Lenartz 2012).
In view of this conceptual and diagnostic shortcoming from the perspective of sport-scientific health research, Pfeifer and Sudeck initially proposed a conceptual base for PA-related health competence (Pfeifer et al. 2013). Building on the idea of this conceptual base, this article aims to develop a questionnaire for certain aspects of PA-related health competence and to validate it in applications of individual-based health promotion and prevention, as well as in rehabilitation.
Conceptual base of PA-related health competence
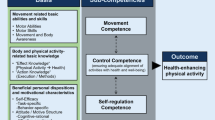
The PA-related health competence model proposed by Pfeifer and Sudeck (Pfeifer et al. 2013), which is modeled after Weinert (2001, p. 72), is based initially on a context- and demand-specific understanding of competence. It places a resource-oriented focus on changeable personal competencies and thus adopts a health promotion strategy proposed by the World Health Organization (WHO 2009). The context- and demand-specific nature stems from the task of integrating PA into everyday life in a health-effective manner. As a result, close attention is paid to those demands that are important for initiating and maintaining PA, and its targeted gearing to health and wellbeing. Based on these premises, three sub-competencies were developed (for a more detailed description, cf. Tab. 1).
1) Movement competence relates to the directly movement-related requirements and comes primarily – but not solely – from the basic motor skills and abilities available. It is understood as a necessary condition for adequately meeting requirements of health sports activities (such as walking, cycling, swimming, gymnastics) and of physical activities on an everyday basis. The model tackles a domain-specific adjustment needed for general health literacy models, as physical and motor aspects play little or no role in such models.
2) Control competence relates to the adequate alignment of physical loads in terms of health and wellbeing. “Adequate” in this context means in line with the basic gearing of training recommendations (e. g., ACSM 2011), generating effective and efficient health gains with minimum risk, and facilitating positive affective reactions to the PA (cf. Ekkekakis et al. 2011). Following Pfeifer (2007), control competence encompasses the extent to which a training-specific knowledge of actions and effects can be applied in a targeted manner that is appropriate to the situation and can be used for structuring activity in a health-effective way. Gearing PA to individual health also requires that body signals can be noticed and used to control and manage the PA load. This relates both to ensuring adequate stimuli (e. g., to avoid excess load, insufficient load, or incorrect load) and to effective mood regulation through PA. Control competence therefore has different facets that, based on Schlicht (1998), range from a functionalistic health concept related to physical fitness (training effects on physical health) to subjectivizing health concepts (subjectively perceived mood-regulating effects).
3) PA-specific self-regulation competence involves the motivational and volitional abilities and willingness required in order to integrate regular health-enhancing PA into everyday life. The description (cf. Tab. 1) here is closely linked to health psychology and action theories of health behavior, which have identified elaborated motivational and volitional behavior determinants (in summary, e. g., Lippke and Wiedemann 2007; Geidl et al. 2014).
To localize these three sub-competencies in a model of PA-related health competence, the basic structure of the health literacy model developed by Soellner’s working group was used (cf. above all Lenartz 2012; Fig. 1). In particular, the method addresses the differentiation of basic elements traditionally found in classic health literacy approaches (e. g., basic abilities and skills, knowledge) from competence facets (in terms of refined abilities). The latter, with their broader focus on the implementation of health-relevant behaviors, are more in line with competence-based approaches of health promotion.

Model of physical activity (PA)-related health competence
One fundamental idea of the model, which was developed based on Lenartz (2012), is that the sub-competencies each comprise specific couplings of the basic elements in terms of refined abilities. How the coupling of basic elements and further-reaching abilities characterize a high level of competency and lead to the specific requirements being adequately met is clarified in Tab. 1. For example, in addition to good physical and motor prerequisites, the competent execution of movements requires that the person is confident about his or her ability to carry out the movement task and is not restricted by, e. g., fears relating to carrying out the movements (cf. Whitehead 2010, who bundles “physical competence” and “confidence” in one common element within her framework of physical literacy). Likewise, control competence cannot be sufficiently described solely by declarative knowledge (e. g., knowledge of the effects of health, “effect knowledge,” cf. Tiemann 2006) or action-related knowledge (e. g., knowledge of the training-effective design and control of physical load, “action knowledge,” cf. Tiemann 2006). Instead, the body- and movement-related knowledge must be applied in a targeted manner that is appropriate to the situation. Furthermore, it is necessary to have good perception and processing of body signals under load, in order to be able to apportion individual load and structure activity so as to achieve positive effects for health and wellbeing. In the area of PA-specific self-regulation competence, individual behavior determinants likewise cannot be seen as sufficient elements of the sub-competence in isolation. It is only through the interaction of the determinants that effective self-regulation can occur and thus the requirements for regular integration of health-enhancing PA in everyday life can be achieved.
Based on the individual sub-competencies, follow-up opportunities for critical and reflective functions of PA-related health competence can be opened up. According to Nutbeam (2000), alongside instrumental and communication elements, these critical and reflective functions constitute the third pillar of health literacy. For example, persons with a high level of control competence combined with high self-regulation competence can take a (more) critical look at recommendations for health-effective PA and assess their significance for their own health and individual wellbeing (Pfeifer 2007). To do this, they can navigate easily through the varied possibilities, incentives, and requirements of physical activities. They know their own motive structure, which is based on motivations that overlap considerably with their own objectives and values and, in a best-case scenario, with their intrinsic motivation for health-enhancing PA. This allows them to make competent decisions regarding the adequacy of exercise activities, to choose activities that feel right, and to carry out these activities on a regular basis (Pfeifer et al. 2013).
Against the backdrop of formulating this PA-related health competence model, steps were taken to provide empirical access to key components of the sub-competencies named above. By analogy to the health literacy research approaches described, this initial operationalization took place on the basis of self-assessments.
Empirical research questions
The aim of developing and validating a questionnaire for sub-facets of PA-related health competence was to extend the possibilities for competence-based research in the applications of exercise therapy and health sports. The initial development and validation work first focused on the areas of control competence, critical reflective decision making, and volitional self-control in the implementation of PA-related intentions (as a sub-aspect of PA-specific self-regulation competence).
The new development placed a special emphasis on control competence in particular, as it is a central factor for structuring one’s own physical activities in a health-promoting way as part of PA-related health competence. Operationalization must be delineated – for example, from motivational and volitional facets – by additionally including aspects of an effective and low-risk increase in physical health or PA-specific mood regulation. For this conceptual core of control competence that incorporates qualitative behavior aspects in terms of positive effects on health and wellbeing, the authors are not aware of any validated German-language questionnaire. The closest comparable approaches can be found in the area of task self-efficacy. McAuley and colleagues (1993) define task self-efficacy as a belief in one’s capabilities to carry out certain exercise tasks and satisfy situational demands. Existing questionnaires focus heavily on the belief in an ability to meet a health-effective situational demand (e. g., to be able to be physically active at moderate intensity for a certain time period three times a week; McAuley et al. 1993) or to be able to be more physically active generally on a regular basis (e. g., Armitage and Arden 2010). The prerequisite for this, namely the concrete belief in an ability to meet the task-specific demand as such, is not dealt with in as much detail. Exceptions include the motor self-efficacy inventory (MOSI; Wilhelm and Büsch 2006) or questionnaires prepared by the working group led by Rodgers (e. g., Rodgers et al. 2008). However, the latter are closer in content to movement competence than control competence, as they are geared to meeting the direct movement-related requirements (cf. Tab. 1).
Therefore, building on the considerations in relation to control competence as an objective of exercise programs for a healthy back (Pfeifer 2007), a questionnaire was developed that presents the (perceived) competence for individually adequate structuring and control of PA. This questionnaire was developed to allow empirical access to such competencies that – in line with the definition of the core of health literacy – ensure optimum positive effects on health and wellbeing in structuring and controlling PA (e. g., effective training of strength and endurance to improve physical health resources; adjusting the activity structure to individual physical and psychological prerequisites; controlling load to avoid excess load or insufficient load based on one’s own body signals; gearing the activity to improving mood).
One aim of the questionnaire is to delineate control competence from the PA-specific self-regulation competencies. As a representative parameter, the questionnaire considers the participant’s assessment with regard to his/her own PA-specific self-control. The selection of this feature and the empirical method were chosen to closely follow Lenartz’s health literacy model (2012). Although comparable tools are already available for this area (e. g., Sniehotta et al. 2005), a short instrument for measuring PA-specific self-control in line with health literacy research was tested in order to examine the discriminant validity.
The questionnaire also aims to allow an assessment of the extent of critical reflective decision making with regard to structuring PA in a health-promoting way. This should also allow for consideration of the critical function of health literacy, which refers to a critical reflective approach to recommendations for health-effective PA on a domain-specific basis.
The processing of the empirical research questions is based on two studies, which were carried out after a pilot study (Tab. 2). In the first study, in the area of exercise therapy, the questionnaire was used in a study group of persons undergoing medical rehabilitation and was examined by factors analysis. Then the final item set was used in a survey of participants in university sports in order to subject the factor structure to cross-validation in the area of health sports and to carry out further validations of the construct.
Developing and testing the item pool
In the pilot study, 21 items were initially generated that were tested in a written survey of an ad hoc sample comprising 65 women and 30 men aged between 30 and 65 years (Mean (M) = 48.6 years; Standard Deviation (SD) = 9.6 years).
To measure the control competence for physical load, two content areas were included. The items formulated (cf. also Tab. 3) were based on previous conceptual work on control competence within the context of an exercise program for healthy backs (Pfeifer 2007). Five items were geared toward assessing the extent to which exercise-specific knowledge can be applied in a targeted manner and used to structure activity in a health-effective way. Another four items involved assessing the extent to which an individual’s own load-related body signals can be noticed and used to control and manage load.
Five items were developed to measure PA-specific mood regulation. Their formulation was based closely on the model used for general health literacy (Lenartz 2012; “self-regulation” sub-scale). For PA-specific self-control, three items from the “self-control” sub-scale in the study conducted by Lenartz (2012) were adapted for specific exercises.
In addition, a further four items were developed that aim to assess critical reflective decision making with respect to adequate physical load. For example, the questionnaire asked respondents to assess the extent to which they themselves can judge whether exercise is doing them good or the extent to which they make sure to understand the meaning and purpose of individual exercises.
In the empirical test, all items had to be answered using a four-stage Likert scale with responses ranging from “disagree completely” (1) to “agree completely” (4). Based on the response behavior (understandability, acceptance) and the initial statistical explorations of the distribution properties of the items and the internal consistencies of the factors considered, 15 items were selected for the further studies. They were allocable to the four areas of control competence for physical load (six items), PA-specific mood regulation (four items), critical reflective decision making (two items), and PA-specific self-control (three items).
Empirical validation of the questionnaire
Methods
Samples and data collection
For study A, participants were interviewed in written form at the beginning of a medical rehabilitation program (Huber and Sudeck 2014).Footnote 1 The interviews took place in ten rehabilitation facilities in Baden-Württemberg, Bavaria, and Rhineland Palatinate. The Ethics Commission of the Faculty of Behavioral and Cultural Studies at Heidelberg University passed a positive vote on the implementation of the study.
The sample comprised n = 463 persons with musculoskeletal disorders, n = 231 with metabolic disorders, n = 199 with cardiovascular diseases, and n = 164 with oncologic diseases. The rate of return for the questionnaires was between approximately 35 % (oncology) and approximately 65 % (cardiology). A total of 29 persons had to be excluded from further data analyses because they had not completed the questionnaire properly (see below). The remaining 1028 persons included 452 women and 576 men. The average age was M = 53.8 years (SD = 9.2 years). Most were aged between 35 and 65 (89.2 %). Only 2 % of the study group were younger than 35 years and 7.5 % were older than 65 years. Furthermore, 40.8 % of respondents had completed basic second-level education, while 31.7 % had obtained advanced second-level education, and 25.4 % had a third-level education.
In study B, 3603 participants of university sports fitness- and health-related programs were alerted by e‑mail to an online questionnaire.Footnote 2 They were given 11 days to log into the questionnaire using a personalized code. Development of the online questionnaire, management for recruiting of the participants, and data backup were carried out using the software package Unipark (www.unipark.com). As an incentive for the subjects taking part, there was a draw for ten free memberships for paid university sports programs in the next semester as well as 15 book vouchers with a value of EUR 20 each. In total, 1741 persons used a link to access the further information on taking part in the study (48.3 %). Of those, 1679 persons provided their informed consent by clicking to place a check mark in a field (cf. Dzeyk 2001) and 1374 persons ultimately completed the questionnaire, i. e., 38.2 % of the persons contacted.
This sample was composed of 1070 students as well as 282 participants in university sports who were allowed to take part as university staff (n = 108) or as guests (n = 174). A further 22 persons did not provide any information on their status. The mean age was M = 26.6 years (SD = 9.7 years). Most people were aged under 30 (82.0 %), 10.5 % were aged between 30 and 40, and 9.5 % were aged over 40 years. Significantly more women took part than men (n = 1141; 83 %). Roughly one in nine participants was male (n = 157; 11.4 %), while 76 did not state their gender.
Measurement method
The data evaluations centered on the items for the sub-competencies of PA-related health competence as described above. In addition, questionnaires for habitual sport activities and for motor function were used to test the validity of the construct.
In study A, the measurement of habitual sport activities was based on the questionnaire to measure PA, exercise, and sport activities (BSA-F, Physical Activity, Exercise, and Sport Questionnaire; Fuchs et al. 2015). The sport and exercise index is relevant for this study report; it was used twice on account of the special situation of some of the persons at the beginning of a medical rehabilitation program (e. g., current limitations due to health problems; cf. Huber and Sudeck 2014). First, the BSA-F variant for sport and exercise activities in the past 4 weeks was completed. If those 4 weeks deviated considerably from the person’s usual activity, e. g., due to health limitations, the respondents were to complete the BSA-F again in the variant for sport and exercise activities normally undertaken. The habitual weekly volume of habitual sport activities (in minutes) was calculated based on the details regarding frequency and duration using the procedure adopted by Fuchs et al. (2015). If the persons at the beginning of a medical rehabilitation program used the second questionnaire, that questionnaire was taken as an indication of habitual sport activities. If the past 4 weeks did not deviate from habitual sport behavior, the first questionnaire was taken as an indication of habitual sport activities. In study A, seven persons (0.1 %) did not provide any information on habitual sport behavior.
In study B, the habitual sport activities were recorded using the Baecke inventory (Wagner and Singer 2003), which uses four indicators to calculate the extent of habitual sport activities. Some information was missing for the sport index indicator that was to be calculated based on the details on the nature, duration, and annual frequency of a maximum of two activities undertaken (cf. also Fig. 3: S1). For example, at least one piece of information was missing for 9.3 % of respondents, which meant that it was not possible to calculate the indicator S1 for those persons. By contrast, relatively few values (maximum 0.5 %) were missing for the other three Likert-scaled items (e. g., S4: “During leisure time I play sports”). Where all four items were answered, there was satisfactory internal consistency for the four indicators (Cronbachs α = 0.75).

Results of the confirmatory factor analyses for the final models in study A (left; N = 1028) and study B (right; N = 1331). (Measurement error variables are not shown explicitly)
The FFB-Mot (Physical Fitness Questionnaire) was used to measure the motor function (Bös et al. 2002). In study A, the short version (12 items) was used, while the long version (20 items) was used for study B. Each of the items can be primarily allocated to one motor skill. In the long version, the creation of total scores provides reliable and valid indicators for status diagnostics in the areas of endurance, strength, coordination, and flexibility (Bös et al. 2002). These total scores were only created if all five items for a motor ability were answered. As only between 3.8 % (flexibility) and 2.6 % (strength) of respondents did not answer all items, there was only a small number of missing values. By contrast, the short version is designed primarily to determine an overall score for motor fitness. In study A, however, there were already good internal consistencies for the motor abilities for the three respective items (endurance: α = 0.75; strength: α = 0.83; flexibility: α = 0.74; coordination: α = 0.74). Total scores were thus also created if all three items were answered.
Statistical data analysis
In study A, the following strategies were used for dealing with missing values (cf. Huber and Sudeck 2014). People who provided less than 75 % of the information requested were excluded from the data analyses in order to minimize possible distortions in subsequent statistical methods for substituting missing values (cf. Wirtz 2004). This meant that 29 persons (2.7 %) were excluded. For the remaining persons, 97 % of the information was available. The values missing here were substituted based on a maximum-likelihood estimation (expectation maximum, EM). For the items of PA-related health competence, the percentage of missing values was between 0.2 % and 1.1 %, with a total 0.6 % of the information for the items in this area substituted.
In study B, the following preparatory data processing steps were necessary. Eleven of the 1374 persons had to be excluded for not completing the questionnaire fully (eight persons did not complete the PA-related health competence section at all; an additional three persons completed fewer than ten of the items). Otherwise the percentage of missing values for the items of PA-related health competence was low: seven persons did not respond to two items and 46 persons did not respond to one item. In addition, persons with extreme response tendencies and/or with an increased probability of “quickly clicking through” as part of the online questionnaire were excluded. To do this, persons were identified who ticked just one possible answer (four throughout: n = 17; three throughout: n = 14) or who only used the extreme answers 1 or 4 when responding (n = 1). The data analyses for study B were thus carried out with 1331 persons. The remaining low percentage of missing values (0.3 % of the data points) was substituted in later evaluations using models (Full information maximum likelihood [FIML] procedure in Mplus).
The exploratory factor analyses were carried out based on study A using principal axis analyses. The purpose of these analyses was to explain the empirical relationship pattern of the 15 manifest indicators using hypothetical parameters. As substantial interrelationships were assumed between the sub-competencies of PA-related health competence, an oblique rotation method (Promax) was used.
The confirmatory analyses based on study A and study B were carried out using the program Mplus 5.21 based on a maximum-likelihood (ML) estimation. The evaluation of the global model fit was based on the guideline values proposed by Schermelleh-Engel et al. (2003). For the convergent validity of the factors, construct validity H and the average variance extracted (AVE) were calculated. The discriminant validity was assessed using the Fornell-Larcker criterion, where the AVE of a factor should be greater than the square of the correlation with other factors in the model. To analyze the indicator reliabilities, the squared multiple correlations (SMC) were used (Bühner 2011).
In addition, for the final set of manifest indicators, descriptive parameters and measures of the reliability of the sub-competencies were determined by means of part-whole correlations as well as internal consistencies (Cronbachs α).
Results
Exploratory factor analyses
The principal axis analysis based on study A showed for the first 15 items used that two (MAP tests) or three factors (eigenvalue criterion, scree plot) could be extracted. For content-related reasons, the three-factor solution was preferred (explained variation: 60.9 %), as it was considerably nearer to the differentiation of factors derived theoretically.
The two items for critical reflective decision making did not result in their own independent factor. They also displayed few clear allocations to one of the three factors. In particular, one item showed low communality (h2 = .26). As a result, the two items for critical reflective decision making were excluded for the following steps.
For a subsequent principal axis analysis with 13 items, as expected three factors had eigenvalues greater than 1, and the screen test also supported an extraction of three factors (explained variation: 64.9 %). The final pattern matrix (Tab. 3) displayed a relatively clear loading structure that did not show any notable external loading (λ < 0.20 in each case). The commonalities of the individual items were medium to high (Bühner 2011), and thus the information available did not indicate a need for any further reduction of the item set.
Descriptive statistics and internal consistency
In both study A and study B, the responses selected to answer the items tended to be in the mid-range of values (Tab. 4). Only the items on PA-related mood regulation were rated as somewhat more positive by the university sports participants in study B. The spread of the response behavior approached normal distribution to the extent that the parameters for the skewness and excess did not indicate any irregularities in the distribution (Miles and Shevlin 2001). The reliability measures were positive on the whole.
Confirmatory factor analyses
To further test the factor validity, confirmatory factor analyses were performed for study A and study B.
Global model fit. To assess the global model fit for the factor structure, two model variants were calculated in each case, as in the first model, a modification index indicated a substantial measurement error covariance in the area of control competence for physical load in both studies (M.I.study A = 22.2; M.I.study B = 54.6). This second model variant was selected for the further considerations, as it was a plausible covariance in terms of content. It indicated a common variance that could not be explained by the latent factor of control competence. For example, the items CC3 and CC5 both relate to aspects of choosing an exercise and structuring activity for muscle training and/or muscle activation (cf. also Tab. 3).
In the overall assessment of the global fit index for the respective final models, an acceptable pattern of findings was arrived at (study A: χ2 = 224.2; χ2/df = 3.68; p < 0.0005; Comparate Fit Index (CFI) = 0.973; Root Mean Square Error of Approximation (RMSEA) = 0.054; Standardized Root Mean Square Residual (SRMR) = 0.028; study B: χ2 = 361.2; χ2/df = 5.92; p < 0.0005; CFI = 0.957; RMSEA = 0.061; SRMR = 0.038).
Convergent and discriminant validity. For all three factors, both study A (CC: H = 0.83; MR: H = 0.89; SC: H = 0.78) and study B (CC: H = 0.79; MR: H = 0.88; SC: H = 0.80) displayed good to very good factor reliabilities, for which values of H > 0.60 are recommended. While the average variance extracted was good (AVE ≥ 0.50) for self-control (study A: AVE = 0.54; study B: AVE = 0.57) and mood regulation (study A: AVE = 0.67; study B: AVE = 0.65), this parameter was below the threshold value for control competence for physical load (study A: AVE = 0.46; study B: AVE = 0.40). The convergent validity for self-control and mood regulation was thus classified as good, while there were mixed findings for control competence for the two criteria H and AVE.
For the discriminant validity, there were likewise no limitations for the factors self-control and mood regulation. These two latent factors had the lowest correlations in both studies (Fig. 2; study A: r = 0.54; study B: r = 0.42). By contrast, in study A the Fornell–Larcker criterion was breached for control competence for physical load. The AVE was lower than the squared factor correlation between control competence and self-control (AVE = 0.46 < (0.76)2 = 0.58; Fig. 2). However, this limitation in the discriminant validity was not confirmed by study B, where factor correlations were lower on the whole. Despite a low AVE for control competence, it was higher than the respective squared factor correlations.

Structural equation modeling to test the validation assumptions (a) in study A (N = 1028) and (b) in study B (N = 1331) based on the features “habitual sport activities” (study A: manifest total index; study B: four indicators: S1–S4) and “motor function” (three indicators: E = total score for endurance; S = total score for strength; C = total score for coordination); Notes: significant covariances between the dependent variables (competence facets, age, gender) were permitted; for more clarity, they are not shown in the diagram, and neither are the measurement models for the competence facets; measurement error variables are only shown if covariances between two measurement error variables were included in the model; * = p < 0.05
Indicator reliabilities. In both studies, the factor loadings were statistically significant for all indicators of the three factors (p < 0.05) and can be rated as satisfactory to good for the most part (Fig. 2). In terms of the SMC, however, study B showed irregularities in the area of control competence for physical load: The two indicators CC3 and CC5, the measurement error variance for which was included in the model, fell short of the recommended value (SMC = 0.28 ≤ 0.40 in each case). This lower indicator reliability must be discussed accordingly in connection with the other parameters for local model fit for the factor of control competence for physical load.
Further construct validation
Two assumptions were central for the further construct validation. Firstly, it was assumed that the three facets of PA-related health competence in terms of behavior determinants can make an independent contribution to explaining the variation in the extent of habitual sport activity. The second assumption relates particularly to the conceptual background of control competence. Because control competence for physical load is geared to the requirement of being able to gear sport activities to health effects, higher control competence for physical load should be linked to a higher level of physical fitness. This association should go beyond the empirically proven interrelationship that the quantitative extent of sport activity has a positive influence on physical fitness. Therefore, it is important to test the empirical expectation that there is a (direct) association between control competence for physical load and motor function that goes beyond the interrelationship between the quantitative extent of habitual sport activity and motor function.
In order to test these two assumptions simultaneously, the measurement model of confirmatory factor analysis was extended to a structural model that made it possible to test the assumptions in connection with the habitual sport activities and motor function (cf. Fig. 3). The habitual sport activities were either supplemented as a manifest indicator (study A: volume of habitual sport activity, BSA-F) or as a latent construct (study B: based on the four indicators of the Baecke sport score). Motor function was taken into account as a latent factor in each case, based on the total scores for motor abilities (study A: three items per total score; study B: five items per total score).Footnote 3 Due to the known age- and gender-dependent distribution of the FFB-Mot (Bös et al. 2002), the two features age and gender were included as covariants for the interrelationships with motor function.
The structural equation model was calculated using the software Mplus 5.21 based on an ML estimation. An acceptable model fit was seen as the prerequisite for interpreting the local path coefficients with a view to the validation assumptions. The significance level for testing the path coefficients was set at α = 0.05. The problem of missing values in study B at the level of the manifest indicators (habitual sport activity) and total scores (motor abilities) described in the methodology was countered with a model-based substitution method (FIML procedure in Mplus). In the final analyses, 1.3 % of the data points were thus substituted in study B.
The findings for the global model fit showed acceptable model fits on the whole. It is true that the χ2 test showed a significant deviation between the theoretical and empirical covariance matrix (study A: χ2 (139) = 458.74; p < 0.001; study B: χ2 (194) = 815.32; p < 0.001) and marginal ratios between the χ2 testing parameters and degrees of freedom in both studies (study A: χ2/df = 3.30; study B: χ2/df = 4.20). However, the other parameters indicated acceptable to good model fits overall (study A: CFI = 0.962; RMSEA = 0.047 [95 % CI: 0.043–0.052]; SRMR = 0.039; study B: CFI = 0.942; RMSEA = 0.049 [95 % CI: 0.046–0.053]; SRMR = 0.040).
The path coefficients between the sub-facets of PA-related health competence and habitual sport activities were statistically significant in both studies with one exception (p < 0.05; Fig. 3). In study A, the path coefficient between control competence for physical load and habitual sport activities missed the statistical significance level. By contrast, as expected, the strongest interrelationship in each case was for self-control. In addition, there were small to medium interrelationships for control competence for physical load (study B) and PA-specific mood regulation (studies A and B), and thus the three competence facets were able to provide an explained variation for sport activities of R 2 = 18.7 % (study A) and R 2 = 53.7 % (study B).
Furthermore, as expected, there was evidence of associations with motor function. However, a strong interrelationship between the habitual sport activities and motor function in study B (β = 0.60; p < 0.05) was countered by a considerably smaller path coefficient in study A (β = 0.07; p < 0.05). In both studies, small to medium interrelationships were determined between control competence for physical load on the one hand and motor function on the other (study A: β = 0.28; p < 0.05; study B: β = 0.19; p < 0.05). The model explained 26.7 % (study A) and 45.9 % (study B) of the variation of motor function.
Discussion
The objective of developing the model of PA-related health competence was to incorporate sport-scientific perspectives on the special aspects of health-effective PA into current health literacy research. A competence-based perspective in the area of health sports and exercise therapy focuses on the demands that a person makes on him/herself to integrate more physical activities, e. g., exercise, in everyday life in a way that is effective for health and wellbeing. From this perspective, sub-competencies were emphasized that can be used to take task-specific requirements into further consideration. A competence-based perspective is considered to add value in this respect, as task-specific or sport-typical elements are often not represented adequately, e. g., in health psychology models of health behavior (e. g., Fuchs 2003). For example, there is often no distinction made between task self-efficacy beliefs and beliefs that relate to carrying out regular health-effective PA, although task self-efficacy is significant for the adoption of regular PA in particular (Higgins et al. 2013).
Control competence is geared to a core idea of health literacy in terms of tasks, namely the ability to make decisions with a positive effect on health and wellbeing. The fit properties of the two scales developed for controlling physical load and for PA-specific mood regulation displayed good internal consistencies. In addition, it was possible to delimit these two facets satisfactorily with respect to both each other and to PA-specific self-control. In the written interview at the beginning of a medical rehabilitation program, it was more difficult to distinguish between control competence for physical load and PA-specific self-control (cf. Fig. 2). In this situation, it is possible that the extent of less actual PA before the rehabilitation due to health limitations with related less well-defined competence features is partially responsible for the relatively high correlations between these features.
In addition, there were indications of conceptual and methodological optimizations for control competence for physical load. The findings on the convergent validity and indicator reliability showed that the indicators are still rather broad and would possibly have to be narrowed down in specific applications. Correspondingly, the confirmatory factor analysis showed a common variation – not explained by the latent factor – of two indicators that relate to specific aspects of choosing an exercise and structuring activity for muscle training and/or muscle activation. Conversely, the core of operationalization for control competence for physical load currently relates more to structuring and controlling endurance loads, as well as to noticing and controlling the load.
Despite the self-assessments recorded here, control competence cannot be equated with task self-efficacy beliefs either conceptually or empirically. Control competence is based on qualitative ways of structuring one’s own behavior with a functional gearing to health and wellbeing. At the operationalization level, this is generally reflected in the functional basic structure of the items for control competence with their relationship to individual applied knowledge (“I know how to do X in order to achieve Y”) and estimates of competence with a functional relationship to the health-effective, risk-minimizing, or mood-improving structuring of physical activities (“I can do X in order to …”). This results in a substantial difference compared with customary operationalizations for task self-efficacy. More specifically, this difference is that, in principle, self-assessments for control competence could be translated into performance-based testing methods with objectifiable criteria for good and bad solutions to tasks. For example, the quality of avoiding excess physical load or insufficient physical load, as well as the quality of noticing one’s own body signals to regulate the load could, in principle, be measured objectively. Furthermore, the subjective assessments of the correct selection of exercises or effective structuring of exercise could be validated using performance-based tests based on expert knowledge. In this way, the items go beyond the subjective beliefs concerning the manageability of movement-related requirements or the confidence in one’s own abilities to achieve quantitative exercise recommendations. However, this argumentation should be qualified by emphasizing that this applies more to control competence for physical load than to PA-specific mood regulation, which always retains an element that cannot be fully objectified.
The empirical studies provide initial indications to support this conceptual understanding of control competence and the corresponding operationalizations. For example, as part of construct validation the expected association between motor function and control competence for physical load was confirmed in both studies to an extent that goes beyond the positive effects of behavior quantity. Based on the cross-sectional data, it can thus be cautiously interpreted that high control competence is associated with positive effects of PA on certain health indicators. Within the framework of PA-related health competence, it is therefore not just about a volume of PA that is as high as possible or that exceeds the minimum recommendations. Instead, control competence also incorporates reflecting on the content and (individual) dosage of PA. Nevertheless, to date, only cross-sectional findings are available, making it impossible to clarify interdependencies definitively. The question regarding the extent to which an association exists between competence assessment for PA-specific mood regulation and selected indicators of psychological health must also be examined.
Self-assessment is a common approach used to record health literacy and has already yielded promising findings in this domain-specific study. As far as control competence is concerned, however, the questions that still need to be answered in the future are the extent to which control competence is actually based on health-relevant knowledge and the extent to which it is expressed in competent behavior that can be observed objectively.
With self-regulation competence, the model of PA-related health competence formulates a relatively complex construct that, in its entirety, promotes the regularity of health-effective PA. The results of construct validation using the structural equation models accordingly affirm that PA-specific self-control has the strongest association with habitual sport activity. The three-item scale, which was developed as a close adaptation of a scale for health literacy with a psychological focus (Lenartz 2012), shows good convergent and divergent validity characteristics in addition to a strong association with habitual sport activities. It therefore constitutes a test-efficient alternative for recording volitional prerequisites in terms of implementing intentions for PA. In addition, further competence-oriented possibilities for recording data would be desirable for the domain of self-regulation that address, for example, motivational competence facets in a domain-specific manner (Rheinberg and Engeser 2007).
Further associations with habitual sport activities were demonstrated for competence assessment for PA-specific mood regulation. This competence assessment can therefore also be of significance for motivational and/or volitional processes. For example, it can promote affective outcome expectancies (e. g., Fuchs 1997) or facilitate overcoming emotional barriers for carrying out regular PA or exercise (e. g., Krämer and Fuchs 2010).
By contrast, there were mixed findings for control competence for physical load in relation to the association with habitual sport activities. While a connection was established for the university sports participants, this was not the case for the persons starting a medical rehabilitation program. In view of the changes in exercise behavior in some cases due to health problems in advance of rehabilitation, it is not possible to clarify here whether this pattern of findings constitutes a generalizable content finding for the domain of rehabilitation or whether it is a consequence of the specific timing of the interview. In addition, the cross-sectional design of both studies must also be taken into account for these interpretations to ensure that empirical support for the function of the sub-competencies that promotes positive behavior is limited. Equally, the reverse situation must also be considered, i. e., that habitual physical activities can have a positive effect on competence assessment.
It has not yet been possible to achieve satisfactory operationalization for the domain of critical reflective decision making. Future studies must further specify the relationship between this domain of health literacy, which was included based on Nutbeam (2000), and the facets of movement competence, control competence, and self-regulation competence. The low level of empirical selectivity is partly plausible, as control competence must be seen as a prerequisite for a critical reflective handling of recommendations for PA behavior. Nevertheless, in view of the low selectivity, it was decided not to extend the breadth of the content of the facets of control competence.
This work did not discuss the methodological possibilities of recording movement competence. Self-assessment can presumably be used here within more narrowly defined limits. Instead, there are indications in some current empirical approaches to recording aspects of physical literacy (e. g., in the summary of Giblin et al. 2014). These testing methods encompass the motor performance level, but the target group has thus far focused on children (e. g., Hermann et al. 2015). In view of the descriptions of movement competence provided here, some measurement approaches could be relevant to the context of rehabilitation. For example, external assessment of self-confident management of exercise tasks (e. g., PLAY, Canadian Sport Institutes 2013) or the fulfillment of minimum requirements for sport participation (e. g., MOBAQ, Kurz et al. 2008), which can be restricted by physical or psychological limitations, could be feasible. For the applications of prevention and rehabilitation for adults, future studies would have to clarify which aspects of movement competence to provide access to and what form of operationalization should be used.
Conclusion
The model of PA-related health competence provides a basis for explicating the interdisciplinary task of assisting people in initiating and maintaining a physically active lifestyle. The focus is on personal competencies that favor the integration of PA into everyday life with positive effects on health and wellbeing. As explained at the outset, this focus is related to important objectives in exercise therapy and health sports concepts. In this respect, the questionnaire developed specifically to record control competencies broadens the possibilities for encouraging competence-based research in the field of individual-based health promotion and prevention, as well as for rehabilitation based on validated methods. In addition to the possibilities of reliable, valid, and test-efficient status diagnostics, which can be assessed positively in adults on the basis of these studies, the questionnaire may also be used to evaluate efforts to promote health competence by means of exercise therapy or health sports offers (Pfeifer et al. 2013). Future research should also focus on answering the question regarding the extent to which this personal competence comes to bear under different social, structural, and economic conditions; as such conditions can promote or hinder PA habits. This also includes the question of the role played by PA-related health competence for health-competent integration of PA into everyday life when an individual’s circumstances change (e. g., new job, change in family circumstances, health limitations). This would close the research gap seen to exist in a failure to link health literacy research geared to individuals and research geared to social structural factors (Abel et al. 2011).
Notes
The survey was part of a research project headed by Prof. Dr. Gerhard Huber (University of Heidelberg) and Prof. Dr. Gorden Sudeck (University of Tübingen). The research project was funded by the German pension insurance (“Deutsche Rentenversicherung Bund”; funding code: 0422-40-64-50-16).
The courses selected were based on the criteria that new participants or returning participants could also be recruited if possible, substantial fluctuation rates were expected, and the courses were not primarily preparatory courses for a competition. As a result, mainly fitness, prevention, and health-related courses as well as beginners’ courses in sports were selected.
Two plausible modifications were needed for the measurement model for motor function: Firstly, in study B in particular, there was a clearly insufficient factor loading for motor function for flexibility (λ = 0.36; SMC = 0.13). This was understandable considering customary dimension approaches to motor skills, which see flexibility as determined primarily by passive structures of the musculoskeletal system and delimit this from the energy and information-processing motor abilities (e. g., Bös et al. 2002). Secondly, the modification index for the covariance of the measurement errors of the total scores for strength and coordination in study B (M.I. = 53.72) indicated that the two indicators still had a common variance that was not represented by the latent construct of motor function. For comparability of the evaluations, flexibility was excluded for both studies and the covariance between the measurement errors of the total scores for strength and coordination was allowed (cf. Fig. 3).
Literatur
Abel, T., Sommerhalder, K., & Bruhin, E. (2011). Health Literacy/Gesundheitskompetenzen. In S. Blümel, P. Franzkowiak, L. Kaba-Schönstein, G. Nöcker, & A. Trojan (Eds.), Leitbegriffe der Gesundheitsförderung und Prävention [Key concepts of health promotion and prevention] (pp. 337–340). Gamburg: Verlag für Gesundheitsförderung.
American Medical Association (1999). Health literacy: report of the council on scientific affairs. ad hoc committee on health literacy for the council on scientific affairs. The Journal American Medical Association, 281, 552–557.
Armitage, C. J., & Arden, M. A. (2010). A volitional help sheet to increase physical activity in people with low socioeconomic status: a randomized exploratory trial. Psychology and Health, 25, 1129–1145.
Brehm, W., Wagner, P., Sygusch, R., Schönung, A., & Hahn, U. (2005). Health promotion by means of health sport – a framework and a controlled intervention study with sedentary adults. Scandinavian Journal of Medicine and Science in Sports, 15, 13–20.
Bös, K., Abel, T., Woll, A., Niemann, S., Schott, N., & Tittlbach, S. (2002). Der Fragebogen zur Erfassung des motorischen Funktionsstatus (FFB-Mot) [The physical fitness questionnaire (FFB-Mot)]. Diagnostica, 2, 101–111.
Bühner, M. (2011). Einführung in die Test- und Fragebogenkonstruktion. [Introduction to designing questionnaires and test forms]. Munich: Pearson.
Bürklein, M. (2007). Gesundheitsverständnis und Gesundheitsmodelle [Health concepts and health models]. In L. Vogt, & A. Neumann (Eds.), Sport in der Prävention [Preventive Sport] (2nd edn., pp. 5–32). Cologne: Deutscher Ärzte Verlag.. revised edition
Canadian Sport Institutes (2013). Physical literacy assessment for youth. www.physicalliteracy.ca/play-tools. Accessed 1 April 2015
Demetriou, Y., Sudeck, G., Thiel, A., & Höner, O. (2015). The effects of school-based physical activity interventions on students’ health related fitness knowledge: A systematic review. Educational Research Review, 16, 19–40.
Deutsche Rentenversicherung Bund (2007). KTL. Klassifikation therapeutischer Leistungen in der medizinischen Rehabilitation. [Classification of therapeutic services in medical rehabilitation]. Berlin: Buck. Version 2007.
Deutsche Rentenversicherung Bund (2014). KTL. Klassifikation therapeutischer Leistungen in der medizinischen Rehabilitation. [Classification of therapeutic services in medical rehabilitation]. Berlin: Buck. Version 2015.
Döhring, V., & Gissel, N. (2014). Sportunterricht planen und auswerten: Ein Praxisbuch für Lehrende und Studierende [Planning and evaluating physical education: A practice book for lecturers and students] (3rd edn.). Hohengehren: Schneider. revised edition.
Dzeyk, W. (2001). Ethische Dimensionen der Online-Forschung. [Ethical dimensions of online-research]. Kölner Psychologische Studien, 6, 1.
Ekkekakis, P., Parfitt, G., & Petruzello, S. J. (2011). The pleasure and displeasure people feel when they exercise at different intensities. Sports Medicine, 41, 641–671.
Fuchs, R. (1997). Psychologie und körperliche Bewegung [Psychology and physical activity]. Göttingen: Hogrefe.
Fuchs, R. (2003). Sport, Gesundheit und Public Health. [Sport, health, and public health]. Göttingen: Hogrefe.
Fuchs, R., Klaperski, S., Gerber, M., & Seelig, H. (2015). Messung der Bewegungs- und Sportaktivität mit dem BSA-Fragebogen: Eine methodische Zwischenbilanz. [Measurement of physical activity and sport activity with the BSA questionnaire]. Zeitschrift für Gesundheitspsychologie, 23, 60–76.
Geidl, W., Semrau, J., & Pfeifer, K. (2014). Health behaviour change theories: Contributions to an ICF-based behavioural exercise therapy for individuals with chronic diseases. Disability and Rehabilitation, 36(24), 2091–2100.
Giblin, S., Collins, D., & Button, C. (2014). Physical literacy: importance, assessment and future directions. Sports Medicine, 44(9), 1177–1184.
Herrmann, C., Gerlach, E., & Seelig, H. (2015). Development and validation of a test instrument for the assessment of basic motor competencies in primary school. Measurement in Physical Education and Exercise Science, 19, 80–90.
Higgins, T. J., Middleton, K. R., Winner, L., & Janelle, C. M. (2013). Physical activity interventions differentially affect exercise task and barrier self-efficacy: a meta-analysis. Health Psychology, 33(8), 891–903.
HLS-EU Consortium (2012). Comparative report of health literacy in eight EU member states. the european health literacy survey HLS-EU First Revised and extended Version, Date July 5th, 2013. www.health-literacy.eu
Huber, G., & Sudeck, G. (2014). Entwicklung einer person-orientierten Bewegungstherapie in der medizinischen Rehabilitation [Development of a person-oriented exercise therapy in medical rehabilitation]. http://forschung.deutsche-rentenversicherung.de/ForschPortalWeb/Final2014_Abschlussbericht_PersonOrientierteBewegungstherapie.pdf
Kickbusch, I. (2006). Die Gesundheitsgesellschaft [The health society]. Hamburg: Verlag für Gesundheitsförderung.
Kickbusch, I., Pelikan, J. M., Apfel, F., & Tsouros, A. D. (2013). Health literacy. The sold facts. Copenhagen: WHO Europe.
Krämer, L., & Fuchs, R. (2010). Barrieren und Barrierenmanagement im Prozess der Sportteilnahme. Zwei neue Messinstrumente. [Barriers and barrier management in physical exercise: Introductio of two new assessment instruments]. Zeitschrift für Gesundheitspsychologie, 18, 170–182.
Kurz, D., Fritz, T., & Tscherpel, R. (2008). Der MOBAQ-Ansatz als Konzept für Mindeststandards für den Sportunterricht? [The MOBAQ approach as a concept for minimum standards for physical education?]. In V. Oesterhelt, J. Hofmann, M. Schimanski, M. Scholz, & H. Altenberger (Eds.), Sportpädagogik im Spannungsfeld gesellschaftlicher Erwartungen, wissenschaftlicher Ansprüche und empirischer Befunde [Sport pedagogy between societal expectations, scientific demands, and empirical evidence] (pp. 97–106). Hamburg: Czwalina.
Lenartz, N. (2012). Gesundheitskompetenz und Selbstregulation. [Health competence and self-regulation]. Göttingen: V & R unipress.
Lippke, S., & Wiedemann, A. U. (2007). Sozial-kognitive Theorien und Modelle zur Beschreibung und Veränderung von Sport und körperlicher Bewegung – ein Überblick. [Prediction and promotion of sport and exercise: An overview of social cognitive theories and models]. Zeitschrift für Sportpsychologie, 14, 139–148.
McAuley, E., Lox, C., & Duncan, T. E. (1993). Long-term maintenance of exercise, self-efficacy, and physiological change in older adults. Journal of Gerontology, 48, 218–224.
Miles, J., & Shevlin, M. (2001). Applying Regression and Correlation: A Guide for Students and Researchers. Thousand Oaks: SAGE Publication.
Nutbeam, D. (2000). Health literacy as a public goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promotion International, 15(3), 259–267.
Pahmeier, I., & Tiemann, M. (2013). Sport und Gesundheit [Sport and health]. In A. Gülich, & M. Krüger (Eds.), Sport: Das Lehrbuch für das Sportstudium [Sport: the coursebook for sport studies] (pp. 655–696). Berlin: Springer.
Pfeifer, K. (2007). Rückengesundheit. [Healthy back]. Cologne: Deutscher Ärzte-Verlag.
Pfeifer, K., Sudeck, G., Brüggemann, S., & Huber, G. (2010). Bewegungstherapie in der medizinischen Rehabilitation – Wirkungen, Qualität und Perspektiven [DGRW-Update: exercise therapy in medical rehabilitation – effects, quality, perspectives]. Rehabilitation, 49, 224–236.
Pfeifer, K., Sudeck, G., Geidl, W., & Tallner, A. (2013). Bewegungsförderung und Sport in der Neurologie – Kompetenzorientierung und Nachhaltigkeit. [Physical activity enhancement and sports in neurology – competence orientation and sustainability]. Neurologie & Rehabilitation, 19(1), 7–19.
Rheinberg, F., & Engeser, S. (2007). Motive training and motivational competence. In O. C. Schultheiss, & J. C. Brunstein (Eds.), Implicit Motive. Oxford: Oxford University Press.
Rodgers, W. M., Wilson, P. M., Hall, C. R., Fraser, S. N., & Murray, T. C. (2008). Evidence for a multidimensional self-efficacy for exercise scale. Research Quarterly for Exercise and Sport, 79(2), 222–234.
Schermelleh-Engel, K., Moosbrugger, H., & Müller, H. (2003). Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. MPR-online, 8(2), 23–74.
Schlicht, W. (1998). Gesundheit [Health]. In O. Grupe, & D. Mieth (Eds.), Lexikon der Ethik im Sport [Dictionary of ethics in sport] (pp. 211–217). Schorndorf: Hoffmann.
Sniehotta, F. F., Scholz, U., & Schwarzer, R. (2005). Bridging the intention-behavior-gap: Planning, self-efficacy, and action control in the adoption and maintenance of physical exercise. Psychology and Health, 20, 143–160.
Soellner, R., Huber, S., Lenartz, N., & Rudinger, G. (2009). Gesundheitskompetenz – ein vielschichtiger Begriff. [Health competence – a complex term]. Zeitschrift für Gesundheitspsychologie, 17(3), 105–113.
Sorensen, K., Van den Broucke, S., Fullam, J., Doyle, G., Pelikan, J., Slonska, Z., & Brand, H. (2012). Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health, 12, 80.
Tiemann, M. (2006). Handlungswissen und Effektwissen [Action knowledge and effect knowledge]. In K. Bös, & W. Brehm (Eds.), Handbuch Gesundheitssport (pp. 357–368). Schorndorf: Hofmann.
Töpfer, C., & Sygusch, R. (2014). Gesundheitskompetenz im Sportunterricht. [Health competence in physical education]. In S. Becker (Ed.), Aktiv und Gesund? [Active and healthy?] (pp. 153–179). Wiesbaden: Springer.
Wagner, P., & Singer, R. (2003). Ein Fragebogen zur Erfassung der habituellen körperlichen Aktivität verschiedener Bevölkerungsgruppen. [A Questionnaire for the evaluation of habitual physical activity in different populations]. Sportwissenschaft, 33(4), 383–397.
Weinert, F. E. (2001). Vergleichende Leistungsmessung in Schulen – eine umstrittene Selbstverständlichkeit. [Comparative assessment of performance in schools – a controversial matter of course]. In F. E. Weinert (Ed.), Leistungsmessungen in Schulen [Assessment of performance in schools] (2nd edn., pp. 17–31). Weinheim: Beltz.
Whitehead, M. (Ed.). (2010). Physical literacy: throughout the Lifecourse. London: Routledge.
WHO (2009). Milestones in health promotion – statements from global conferences. geneva: WHO.. http://www.who.int/healthpromotion/Milestones_Health_Promotion_05022010.pdf. Accessed 1 April 2015.
Wilhelm, A., & Büsch, D. (2006). Das Motorische Selbstwirksamkeits-Inventar (MOSI). [Motor self-efficacy inventory (MOSI). A domain-specific scale of self-efficacy in sport]. Zeitschrift für Sportpsychologie, 13, 89–97.
Wirtz, M. (2004). Über das Problem fehlender Werte: Wie der Einfluss fehlender Informationen auf Analyseergebnisse entdeckt und reduziert werden kann. [On the Problem of Missing Data: How to Identify and Reduce the Impact of Missing Data on Findings of Data Analysis]. Die Rehabilitation, 43, 109–115.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
G. Sudeck and K. Pfeifer state that there are no conflicts of interest.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Caption Electronic Supplementary Material
Rights and permissions
About this article

Cite this article
Sudeck, G., Pfeifer, K. Physical activity-related health competence as an integrative objective in exercise therapy and health sports – conception and validation of a short questionnaire. Sportwiss 46, 74–87 (2016). https://doi.org/10.1007/s12662-016-0405-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12662-016-0405-4