
Abstract
Recent pre-clinical and clinical studies suggest that general anesthesia in infants and children may increase the risk of learning disabilities. Currently, there is no treatment for preventing anesthesia-induced neurotoxicity and potential long-term functional impairment. Animal studies have shown that neonatal exposure to anesthesia can induce acute neurotoxicity and long-term behavioral changes that can be detected a few months later. It is currently unknown whether neonatal exposure, especially repeated exposures, to general anesthesia can induce or increase the risk for cognitive impairment during aging. Here, we report that repeated exposures of neonatal mice (P7–9 days old) to anesthesia with sevoflurane (3 h/day for 3 days) led to cognitive impairment that was detectable at the age of 18–19 months, as assessed by using novel object recognition, Morris water maze, and fear conditioning tests. The repeated neonatal exposures to anesthesia did not result in detectable alterations in neurobehavioral development, in tau phosphorylation, or in the levels of synaptic proteins in the aged mouse brains. Importantly, we found that treatment with intranasal insulin prior to anesthesia exposure can prevent mice from anesthesia-induced cognitive impairment. These results suggest that neonatal exposure to general anesthesia could increase the risk for cognitive impairment during aging. This study also supports pre-treatment with intranasal administration of insulin to be a simple, effective approach to prevent infants and children from the increased risk for age-related cognitive impairment induced by neonatal exposure to general anesthesia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Exposure of young animals, including both rodents and non-human primates, to general anesthesia causes apoptosis (Brambrink et al. 2012; Creeley et al. 2013; Li et al. 2019a; Yon et al. 2005; Zou et al. 2011), impaired synaptic development (Briner et al. 2011; Zou et al. 2011), reduction of neurogenesis (Kang et al. 2017; Zhu et al. 2010), increased reactive oxygen species and mitochondrial dysfunction (Boscolo et al. 2012; Sanchez et al. 2011), and neuroinflammation in the brain (Shen et al. 2013). Anesthesia-induced neurotoxicity in the immature brain could lead to abnormal brain development, which may contribute to cognitive impairment in old age (Jevtovic-Todorovic et al. 2013; Paule et al. 2011). Studies have demonstrated that exposure of animals to anesthesia in the early postnatal period can cause long-term cognitive dysfunction that is detectable at the young adult age in rodents (Fredriksson et al. 2004, 2007; Jevtovic-Todorovic et al. 2003, 2013; Li et al. 2019a; Maloney et al. 2019; Stratmann et al. 2010). It is not known whether neonatal exposure to anesthesia can increase the risk for cognitive impairment during aging.
Pre-clinical studies have raised concerns about whether the neurotoxicity and long-term cognitive impairment induced by early exposure of young animals to general anesthesia also occur in young children when they have surgery. Millions of children prior to the age of 5 years undergo general anesthesia each year in the USA (Sun et al. 2016a). If exposures to general anesthesia cause long-term neurodevelopmental risks in healthy children, it is urgent to develop an approach to prevent the side effects of anesthesia in the children. Recently, several epidemiological studies suggested that multiple exposures to general anesthesia before the age of 4 years could be detrimental to cognitive development and could accelerate cognitive decline in the elderly (Hu et al. 2017; Wilder et al. 2009). To date, there is no effective treatment that can prevent anesthesia-induced neurotoxicity and behavioral deficiencies later in life.
Recent studies have suggested that insulin can regulate neuronal proliferation and differentiation, promote neurite outgrowth, prevent neuronal apoptosis, and protect neurons against oxidative stress (Chen et al. 2014a). Insulin also regulates neural plasticity and plays an important role in memory and cognitive function (Blazquez et al. 2014; Zhao et al. 2004). Human clinical trials have shown that intranasal delivery of insulin, which is safe and bypasses the blood-brain barrier to deliver insulin directly into the brain (Hanson and Frey 2008), improves cognitive function in healthy adults (Benedict et al. 2004, 2007, 2008; Hallschmid et al. 2008; Krug et al. 2010), in memory-impaired older individuals (Claxton et al. 2015; Reger et al. 2006, 2008a), and in individuals in the early stage of Alzheimer’s disease (Claxton et al. 2013, 2015; Craft et al. 2012, 2017; Reger et al. 2008a,b). Intranasal insulin also ameliorates clinically relevant functional improvement in Parkinson disease patients (Novak et al. 2019). In recent studies, we found that intranasal administration of insulin can prevent anesthesia-induced brain changes and cognitive impairment in adult and aged mice (Chen et al. 2014b, 2017; Zhang et al. 2016). We also found that repeated exposures of neonatal mice to sevoflurane led to acute neuronal apoptosis and to a decrease in brain levels of postsynaptic density 95 (PSD95) as well as mild behavioral abnormalities that can be detectable 1–4 months later and that intranasal administration of insulin prior to anesthesia can prevent the anesthesia-induced abnormal biochemical changes and cognitive dysfunction (Li et al. 2019a). The present study was undertaken to investigate whether repeated exposure of neonatal mice to anesthesia with sevoflurane impairs neurobehavioral development and causes any cognitive dysfunction during aging and whether intranasal administration of insulin can protect the mice from anesthesia-induced long-term damages.
Sevoflurane is the most commonly used inhalation anesthetic for pediatric anesthesia. In the present study, we found that exposure of neonatal mice to sevoflurane caused cognitive impairment that was detectable at the age of 18 months and that pre-treatment with a single dose of intranasal insulin prevented the anesthesia-induced cognitive impairment during aging.
Materials and Methods
Antibodies and Reagents
Primary antibodies used in this study are listed in Table 1. Humulin R (U-100) was purchased from Eli Lilly Company (Indianapolis, IN, USA). Chemicals and other reagents were purchased from Sigma-Aldrich (St. Louis, MO, USA) unless otherwise noted.
Mice
C57BL/6 mice were initially obtained from the Jackson Laboratory (New Harbor, ME, USA). The mice were bred in our air-conditioned animal facility and housed with a 12/12-h light/dark cycle and with ad libitum access to food and water. Animal studies were approved by the Institutional Animal Care and Use Committee (IACUC) of the New York State Institute for Basic Research in Developmental and Disabilities (Staten Island, NY, USA) and were conducted according to the US PHS NIH guidelines.
Animal Treatment
Induction of anesthesia was carried out as previously described (Li et al. 2019a). Briefly, neonatal mice at the age of postnatal (P) day 7 were placed in an anesthesia chamber (25 cm × 15 cm × 13 cm) filled with 5% sevoflurane in a mixture of O2 and N2 (50/50%). The sevoflurane concentration was reduced to 3% after a 3-min induction period and maintained for 3 h. The air flow rate was 0.9–1.0 l/min during anesthesia. A small Petri dish of water was placed in the anesthesia chamber to maintain moisture. At the end of anesthesia, the sevoflurane was turned off, and the mouse pups were kept in the same chamber with O2 and N2 to allow their recovery from anesthesia, and then the mouse pups were returned to their parents’ cages. A warm pad was placed in the anesthesia chamber to maintain the body temperature at 35–36 °C during the procedure. Neonatal mice used as controls were placed in the chamber filled with a mixture of O2 and N2 (50/50%), but with no sevoflurane for the same periods of time as the anesthetized group. This procedure of anesthesia was repeated for two more consecutive days.
The neonatal mice received a total of 7.0 μl insulin (0.14 U/mouse) or saline treatment through intranasal delivery 30 min before the beginning of each anesthesia (Fig. 1), as previously reported (Li et al. 2019a). Briefly, the P7–9 mouse pups were held in a supine position in hand, and 1.0 μl insulin or saline was delivered into the left side nare using a 2.5-μl Eppendorf pipette. The pups were given 15–20 s to allow the fluid to be taken into the nose before the administration was repeated six times.

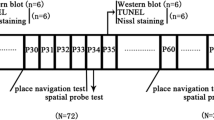
Schematic of animal studies. a P7 neonatal mice were randomly assigned to four groups: (1) control (Con), (2) intranasal administration of saline followed by 3-h anesthesia with 3% sevoflurane starting 30 min after saline administration (Anes), (3) intranasal administration of insulin followed by 3-h anesthesia with 3% sevoflurane starting 30 min after insulin administration (Anes + Ins), and (4) intranasal administration insulin only (Ins). The behavioral tests, including open field (OF), novel object recognition (NOR), Morris water maze (MWM), and fear conditioning (FC), were conducted at the indicated ages. All animals were sacrificed at the age of 564 days. b A separate batch of mice, including Con, Anes, and Anes + Ins groups, was employed for neurodevelopmental milestone assessment from P7 to P24, and the mice were euthanized at P25
Neonatal mice (P7, male) from various litters were randomly assigned into four groups: (1) control (Con) group that received intranasal administration of saline instead of insulin and were not anesthetized, (2) anesthesia (Anes) group that received intranasal saline followed by anesthesia with sevoflurane, (3) anesthesia plus insulin (Anes + Ins) group that received both, and (4) control insulin (Ins) group that received insulin but not sevoflurane. Mouse pups at the age of P7 with body weight less than 2.2 g were excluded from the study. A separate batch of mice randomly grouped into three groups (Con, Anes, and Anes + Ins) were employed to assess neurodevelopmental milestones (Fig. 1b). To eliminate any potential bias caused by litter variations, similar numbers of mouse pups from each litter were assigned to each group, and each group included pups from multiple litters.
Pre-weaning Assessment of Neurobehavioral Development
Newborn mice were weighed daily during P7–9 and then every other two days to P24. Developmental milestones, including eye opening, air righting, ear twitch reflex, and auditory startle, were examined daily from P7, as described previously (Kazim et al. 2017; Tamashiro et al. 2000).
Behavioral Tests
Behavioral tests including open field, novel object recognition test, Morris water maze, and fear conditioning were carried out from less-stress tests to more-stress tests at the indicated ages in Fig. 1a.
Open Field Test
Open field test was used to assess simultaneously locomotion, exploration, and anxiety in rodents (Walsh and Cummins 1976) and was conducted as previously described (Li et al. 2019a). The animals were transferred to the test room for habituation for 1 h before starting the test. Each mouse was placed in the open field arena (made of opaque white plastic material, 50 cm × 50 cm × 40 cm) and allowed to explore in the arena for 15 min. The distance travelled (meters) in the open field arena and the central area (10 cm × 10 cm) and the entries and time spent in the central area were automatically recorded by a video tracking system (Any Maze version 4.5 software, Stoelting Co., Wood Dale, IL, USA).
One-Trial Novel Object Recognition Task
One-trial novel object recognition test was performed as described previously (Dai et al. 2017; Li et al. 2019a). Briefly, testing consisted of a habituation phase, a sample phase, and a test phase. Following initial exposure, four additional 10-min daily habituation sessions were performed for mice to become familiar with the apparatus (50 cm × 50 cm × 40 cm) and the surrounding environment. On the fifth day, each mouse was first submitted to the sample phase, when two identical objects were placed in a symmetric position from the center of the arena. The mouse was allowed to freely explore the objects for 5 min. After a 20-min delay during which the mouse was returned to its home cage, the animal was re-introduced in the arena to perform the test phase. The mouse was then exposed to two objects for another 5 min: a familiar object (previously presented during the sample phase) and a novel object of similar size with a familiar one but of different color and shape. Data were collected using a video tracking system (Any Maze version 4.5 software). Object discrimination index during the test phase was calculated as follows:
Morris Water Maze Task
The Morris water maze (MWM) task was used to evaluate spatial learning and memory of the mice (D’Hooge and De Deyn 2001; Dai et al. 2017; Morris et al. 1982). The test was performed in a white circular pool with a 180-cm-diameter filled with water tinted with non-toxic white dye and maintained at room temperature (20 ± 1 °C). The maze was divided into two virtual principal axes, with each line bisecting the maze perpendicular to the other one to divide the maze into four equal quadrants. The end of each line demarcated four cardinal points: east, south, west, and north. A platform was positioned in the middle of one of the quadrants, submerged 0.5 cm below water surface. Each mouse performed four trials per day for four consecutive days from semi-random start positions (Vorhees and Williams 2006) to find the hidden platform. Each trial was terminated as soon as the mouse climbed onto the hidden platform. If a mouse failed to find the platform within 90 s, it was gently guided to the platform. At the end of each trial, the mouse was left on the platform for 10 s, then removed, dried, and returned to its home cage. A 90-s probe test without platform was performed 24 h after the last trial. The escape latency in initial training, and the latency to the 1st entrance into the target (platform location area), target crossings, swim speed, and time spent in the target quadrant in probe test were recorded through an automated tracking system (Smart video tracking system, version 2.0.14, Panlab; Harvard Apparatus).
Fear Conditioning
Mice were habituated in the testing room for 1 day prior to testing. In a fear-conditioning training session, the mice were habituated to the context for 120 s, and then four tone-shock pairs consisting of a 30-s tone (2000 Hz, 75 dB) co-terminating with a 2-s foot shock at 0.6 mA delivered with a 120-s interval. Afterward, the mice remained in the context for 120 s before being returned to their home cage. In the context session on day 2, the mice were placed into the same testing chamber without tone or electric foot shock for 5 min to measure freezing response to the context. For the cued tone test, the mice were placed in the same chamber with altered context. After a 180-s baseline habituation, a 180-s tone was delivered without the shock pairing, and then the mice remained in the chamber for 90 s before being returned to their home cage. All the data were collected and analyzed with the Freeze Frame and Freeze View system (Coulbourn Instruments, Whitehall, PA, USA).
Western Blot Analysis
After behavioral tests, the mice were sacrificed by cervical dislocation. The mouse brains were immediately dissected, and the cerebrocortical tissue was homogenized in pre-chilled buffer containing 50 mM Tris-HCl, pH 7.4, 150 mM NaCl, 50 mM NaF, 1 mM sodium orthovanadate, 1 mM EGTA, 0.5 mM AEBSF, and 10 μg/ml each of aprotinin, leupeptin, and pepstatin. The homogenates were boiled in 2× Laemmli sample buffer for 10 min. The protein concentrations of the samples were measured by Pierce™ 660-nm protein assay (Thermo Fisher Scientific, Rockford, IL, USA). The samples were resolved by 10% SDS-PAGE and electro-transferred onto Immobilon-P membranes (EMD Millipore, Billerica, MA, USA). The blots were then probed with primary antibodies (Table 1) and developed with the corresponding HRP-conjugated secondary antibody and enhanced chemiluminescence kit (Thermo Fisher Scientific). Densitometric quantification of protein bands in Western blots was analyzed using Multi Gauge version 3.0 software (FUJIFILM North America, Valhalla, NY, USA).
Statistical Analysis
The quantitative data were analyzed by using appropriate statistical tests, including one-way ANOVA for OF data, NOR data, and Western blot data and two-way repeated measures ANOVA plus post hoc test for MWM data and FC data by using GraphPad. All data are presented as means ± SEM, and p < 0.05 was considered statistically significant.
Results
Repeated Exposure of Neonatal Mice to Anesthesia with Sevoflurane Does Not Affect Growth or Neurobehavioral Development in Mice
To investigate whether the exposure of neonatal mice to anesthesia with sevoflurane impacts neurodevelopment of mice, we monitored the neurodevelopmental milestones from P7 to P24. We found that repeated 3-h anesthesia with sevoflurane for three consecutive days did not affect the body weight (Fig. 2a) or the time of first eye opening of the neonatal mice (Fig. 2b). The development of reflexes, as tested by air righting (Fig. 2c), ear twitch reflex (Fig. 2d), and auditory startle (Fig. 2e), was not found to be affected by anesthesia either. These results indicate that repeated 3-h anesthesia of neonatal mice with sevoflurane for three consecutive days does not impair the growth or neurobehavioral development of mice. Similarly, intranasal administration of insulin prior to anesthesia did not show any impact on the growth or neurobehavioral development of mice.

Body weight and days of first appearance of developmental behaviors. a Body weight. b First day of both eyes opened. Days of first performance of air righting (c), ear twitch reflex (d), and auditory startle (e). Con, n = 12; Anes, n = 16; Anes + Ins, n = 15
Repeated Exposure of Neonatal Mice to Anesthesia with Sevoflurane Leads to Cognitive Impairment in Old Age
We previously found that neonatal exposure of mice to anesthesia causes mild cognitive impairment that is detectable at the ages of 1–3 months (Li et al. 2019a). Here, we investigated if repeated neonatal anesthesia could affect cognitive function during aging. Considering that anxiety can impact the assessment of cognitive function, we first conducted open-field test to evaluate the spontaneous activity and anxiety of the mice at the age of 18 months (542 days). We found no significant differences in the distances travelled in the open field between the mice in control and anesthesia groups (Fig. 3a). There were no significant differences in the number of center area entries (Fig. 3b), time in the central area (Fig. 3c), or distance travelled in the central area (Fig. 3d) between the two groups either. These results suggest that neonatal exposure to anesthesia with sevoflurane does not affect spontaneous activity or anxiety in old age.

Open field and novel object recognition tests of aged mice after neonatal exposure to anesthesia and/or intranasal insulin. a–d Open field test performed at the age of 18 months (542 days). The total distance travelled (a), number of central area entries (b), central area time (c), and distance travelled in central area (d) in 15-min session were recorded. e, f One-trial novel object recognition test performed at the age of 18 months (546 days). The percentage of time spent exploring two identical objects during a 5-min sample phase (e) and the discrimination index (time spent exploring novel object over the time spent exploring both novel and familiar objects) in a 5-min test phase (f) are presented. Con, n = 9; Anes, n = 9; Anes + Ins, n = 9; Ins, n = 10. Data are presented as mean ± SEM. *p < 0.05
One-trial novel object recognition test was employed to assess the effect of anesthesia on short-term memory in aged mice. The mice in control and anesthesia groups spent a similar length of time to explore the two identical objects during the 5-min sample phase (Fig. 3e). However, the aged animals with exposure to anesthesia during P7 to P9 spent less time exploring the novel object during the test phase (Fig. 3f). These results indicate that repeated exposure of neonatal mice to sevoflurane can cause long-term cognitive impairment when they become 18 months old.
We also assessed the impact of anesthesia on spatial learning and cognitive function by using Morris water maze test at the age of 18 months (549–553 days). We found that the mice in the control and anesthesia groups spent a similar amount of time to find the hidden platform during the 4-day acquisition phase (Fig. 4a). However, during the probe test, the mice of the anesthesia group crossed the platform location much less often (Fig. 4b) and exhibited a tendency to take more time than the control mice did to reach the platform location (Fig. 4c) and to spend less time in the target quadrant (Fig. 4d). No significant difference was observed in swim speed between these two groups of animals during the probe test (Fig. 4e). These results suggest that repeated exposure of neonatal mice to sevoflurane can cause long-term spatial memory impairment but apparently has no impact on the long-term spatial learning function.

Long-term spatial memory assessment (in Morris water maze) of aged mice after neonatal exposure to anesthesia and/or intranasal insulin. a The escape latency to reach the hidden platform during the four consecutive day acquisition phase. b–e Number of platform location crossings (b), latency to reach the platform location (c), percentage of time in the target quadrant (d), and swim speed (e) during the probe test. Con, n = 9; Anes, n = 9; Anes + Ins, n = 9; Ins, n = 10. Data are presented as mean ± SEM. *p < 0.05
The contextual and cued fear conditioning tests were performed at the age of 18.6 months (559–560 days). The test consisted of a conditioning phase on day 1 and a testing phase on day 2 (Fig. 5a–c). During the conditioning phase, freezing time increased with conditioning in mice with or without neonatal exposure to anesthesia. However, significant reductions in the freezing time were observed in the mice in the anesthesia group as compared to the control group (Fig. 5d), suggesting an impairment in the amygdala/hippocampus-dependent memory of these mice. No significant differences in the freezing time were seen during the context test or cued tone test between mice with or without neonatal exposure to anesthesia (Fig. 5e, f). These results suggest that anesthesia in neonatal mice with sevoflurane at P7–9 can cause learning impairment associated with the amygdala, hippocampus, frontal cortex, and cingulate cortex during aging.

Fear conditioning test of aged mice after neonatal exposure to anesthesia and/or intranasal insulin. Fear conditioning test was carried out at the age of 18.6 months (559–560 days). a–c Fear conditioning test schedule, which was carried out over two consecutive days. d The curve of percentage of frozen time during the conditioning phase on day 1 of the FC test. e Percentage of time the mice froze in the context test. f Percentage of time the mice froze in the cued tone test. Con, n = 9; Anes, n = 9; Anes + Ins, n = 9; Ins, n = 10. Data are presented as mean ± SEM. *p < 0.05; ***p < 0.001
Repeated Exposure of Neonatal Mice to Anesthesia with Sevoflurane Does Not Lead to Detectable Alterations in Levels of Tau Phosphorylation or Synaptic Proteins in the Brain in Aged Mice
Abnormal hyperphosphorylation of microtubule-associated protein tau leads to its accumulation and neurofibrillary degeneration, which underlies cognitive impairment in Alzheimer’s disease (AD) and other tauopathies (Iqbal et al. 2016). To investigate whether neonatal exposure of mice to anesthesia could promote tau hyperphosphorylation later in life, we analyzed the levels of tau phosphorylation at the AD-related sites in the aged mouse brains by using quantitative Western blots developed with tau-specific and phosphorylation-dependent antibodies. However, we did not find any significant differences in the levels of total tau, as determined by antibody R134d or in tau phosphorylation at Ser199, Ser202/Thr205, or Ser396/404 (Fig. 6a and b) between aged mice with and without neonatal exposure to anesthesia.

Western blots of aged mouse brains for tau phosphorylation and synaptic proteins. Cerebral cortices of mice were homogenized and analyzed by Western blots developed with antibodies indicated at the left side of the blots (a and c). Quantification of the blots is shown in b and d. * p < 0.05, **p < 0.01, ***p < 0.001, n = 8 mice per group
To further investigate a possible molecular basis for the cognitive impairment that was detectable in the aged mice after neonatal exposure to anesthesia, we determined the levels of synaptic proteins, including pre-synaptic proteins synapsin 1 and synaptophysin and postsynaptic protein PSD-95, in the aged mouse brains by using Western blots. Again, we found no significant differences in the levels of these synaptic proteins between the aged mice with neonatal exposure to anesthesia and those without the anesthesia exposure (Fig. 6c and d). It is interesting to note higher levels of synapsin 1 and PSD-95 in the aged brains of mice who received intranasal insulin treatment during neonatal age than those who did not receive insulin (Fig. 6c and d).
Intranasal Administration of Insulin Prevents the Neonatal-Anesthesia-Induced Cognitive Impairment in Old Age in Mice
We have previously found that intranasal administration of insulin can prevent anesthesia-induced long-term cognitive impairment examined in 3-month-old mice (Li et al. 2019a). To investigate whether insulin can prevent aged mice from cognitive impairment caused by exposure to anesthesia at the neonatal age, insulin was delivered through intranasal administration to neonatal mice 30 min before each repeated anesthesia with sevoflurane at P7–9 (Fig. 1). We also included an insulin-alone group, for which the neonatal mice received intranasal administration of insulin but not anesthesia, to learn if the neonatal administration of insulin itself affects the neurodevelopment or cognitive function during aging. We found that, like repeated anesthesia with sevoflurane, insulin administration affected neither neurobehavioral development (Fig. 2) nor spontaneous activity or anxiety during aging, as determined by open field test (Fig. 3a–d). During the novel object recognition test, pre-treatment with insulin did not affect the exploration of time during the sample phase (Fig. 3e); however, the mice pre-treated with insulin tended to spend more time exploring the novel object during the test phase (Fig. 3f). The anesthesia-caused significant reduction in the discrimination index was prevented by pre-treatment with intranasal insulin. These results suggest that intranasal administration of insulin can prevent aged mice from the short-term memory impairment caused by neonatal exposure to repeated anesthesia.
As described above, repeated neonatal anesthesia caused spatial memory impairment in aged mice, as evidenced by a significant decrease in the number of target platform location crossings (Fig. 4b) and an increase in the latency to reach the platform location (Fig. 4c) during the probe test in the Morris water maze. A clear tendency, though not statistically significant, to spatial memory impairment was also seen with the time the mice spent in the target quadrant during the probe test (Fig. 4d). Interestingly, these behavioral impairments were completedly prevented with intranasal insulin administrated prior to anesthesia (Fig. 4b–d). Neither intranasal insulin nor anesthesia appeared to have any significant effects on spatial learning, as shown by the similar learning curves during the acquisition phase of the Morris water maze test (Fig. 4a). These results suggest that intranasal administration of insulin can prevent aged mice from the spatial memory impairment caused by repeated neonatal exposure to anesthesia.
Fear conditioning test, which assesses amygdala/hippocampus-associated memory, showed significant learning impairment in the aged mice after repeated neonatal exposure to anesthesia and significant prevention of such impairment with prior treatment with intranasal insulin (Fig. 5d). However, neither anesthesia nor intranasal insulin treatment during the neonatal period showed any significant impact to the memory function assessed in the context test and cued tone test at old age (Fig. 5e, f).
Taken together, our results indicate that intranasal insulin administered 30 min prior to exposure of neonatal mice to sevoflurane can prevent anesthesia-induced cognitive impairment in old age.
Discussion
In 2016, the U.S. Food and Drug Administration (FDA) warned that repeated or prolonged use of general anesthetic and sedation drugs during surgeries or procedures in children younger than 3 years or in pregnant women during their third trimester may affect the development of children’s brains (Ganzberg 2017). However, the long-term effects of neonatal anesthesia remain elusive, and no effective approach that can prevent or reduce anesthesia-induced neurotoxicity and behavioral impairment is currently available. In the present study, we found that P7- to P9-day-old neonatal mice anesthetized with sevoflurane for 3 h per day for three consecutive days can lead to cognitive dysfunction that is detectable in old age (18 months old). Importantly, pre-administration of insulin via intranasal delivery before each exposure to anesthesia prevented long-term anesthesia-induced cognitive impairment.
Insulin in the brain plays important roles in the regulation of food intake and body weight as well as whole-body glucose, energy, and lipid metabolism and in the modulation of learning and memory (Heni et al. 2015). Human studies have demonstrated that intranasal administration of insulin is safe and can improve cognitive function (Hanson and Frey 2008; Schmid et al. 2018). In our previous studies, we found that intranasal administration of insulin at the dose 1.75 IU/mouse decreases anesthesia-induced tau phosphorylation and prevents anesthesia-induced cognitive impairment in adult 3xTg-AD mice (Chen et al. 2014b, 2017) and wild type C57BL/6J mice (Zhang et al. 2016). Importantly, this dose of intranasal insulin has no significant effect on the peripheral blood glucose level (Nedelcovych et al. 2018). Therefore, we administered insulin to neonatal mice via intranasal delivery at the dose of 0.14 IU (approximately equivalent to 1.75 IU/mouse for adult mice). Importantly, we found that intranasal administration of insulin at 0.14 IU/mouse prevented anesthesia-induced abnormal changes in the brain of neonatal mice and prevented anesthesia-induced cognitive impairment as determined at the age of 3 months (Li et al. 2019a). The present study shows that neonatal pre-treatment with intranasal insulin also protected the aged mice (18 months old) from cognitive impairment induced by early exposure to anesthesia during the neonatal period.
Neonatal brain development involves neuronal arborization, synaptogenesis and pruning, gliogenesis, and myelination (van Dyck and Morrow 2017), which is a complex series of dynamic and adaptive processes operating within a highly constrained, genetically organized, but constantly changing context (Stiles and Jernigan 2010). Mouse brain growth spurt reaches the peak at P7, which is approximately equivalent to the first 2 months of life in humans (Dobbing and Sands 1979; Dutta and Sengupta 2016; Semple et al. 2013). Because developing the brain is more vulnerable to insults and injury at this period, most animal studies on developing brain employ P6–8 neonatal animals (Walters and Paule 2017). During this typical neonatal brain development, the glial-vasculature and glial-neuronal interactions are fully defined and play a pivotal role in the functional organization of neural circuits that is crucial to cognitive function later in life. However, exposure of neonatal mice to anesthesia can cause apoptosis (Brambrink et al. 2012; Creeley et al. 2013; Yon et al. 2005; Zou et al. 2011), impaired synaptic development (Briner et al. 2011; Zou et al. 2011), and reduction of neurogenesis (Kang et al. 2017; Zhu et al. 2010), which may lead to abnormal postnatal brain development, which, in turn, may contribute to abnormal neurobehavioral function later in life. Previously, we reported behavioral dysfunction in young adult mice that were anesthetized during the neonatal period (Li et al. 2019a). Here, we further report that abnormalities induced by anesthesia with sevoflurane in neonatal mice can cause cognitive impairment that can be detected in old age (18 months old).
The underlying mechanism of long-term cognitive dysfunction induced by anesthesia at neonatal animals at P7 remains unclear. We previously found that anesthesia can induce abnormal tau phosphorylation (Chen et al. 2014b, 2017; Zhang et al. 2016). Because abnormal hyperphosphorylation of tau in the brain plays a vital role in the pathogenesis of AD (Gong and Iqbal 2008) and can induce cognitive impairment (Di et al. 2016), and intranasal administration of insulin can reduce anesthesia-induced abnormal tau phosphorylation in adult 3xTg-AD mice (Chen et al. 2014b, 2017) and in wild type C57BL/6J mice (Zhang et al. 2016), we first determined the level of phosphorylated tau in mouse brains. We did not find a significant change in the level of tau phosphorylation at several phosphorylation sites. The change in abnormal tau phosphorylation induced by anesthesia is dynamic. Abnormal tau phosphorylation can be detected immediately after anesthesia but not at 24 h or 5 days after anesthesia (Zhang et al. 2016). The level of tau phosphorylation had restored to its baseline level at the examined age.
General anesthesia may impair synaptic remodeling when administered at the peak of synaptogenesis and may cause a significant decrease in synapse volumetric densities (Crosby et al. 2010; Lunardi et al. 2010). We analyzed the presynaptic protein markers synapsin 1 and synaptophysin, and postsynaptic protein PSD95. No significant alterations of these synaptic markers were found in the aged mouse brains after neonatal anesthesia exposure, suggesting that this method cannot detect the structural or molecular basis of the cognitive impairment at this age. Nevertheless, we found that intranasal insulin administered in the neonatal period increased the synapsin 1 and PSD-95 levels of the aged brains. Because the elevation of brain synaptic proteins was previously observed hours to days after intranasal insulin administration to neonatal and adult mice (Li et al. 2019a; Zhang et al. 2016), our results reported here suggest that the effects of intranasal insulin on synapses last a very long time, at least for 18 months in mice.
Several agents have been reported to prevent anesthesia-induced neurotoxicity and long-term cognitive deficiencies in laboratory animals. Melatonin (Yon et al. 2006), EUK-134 (Boscolo et al. 2012), and hydrogen gas (Yonamine et al. 2013) were found to alleviate anesthesia-induced neurotoxicity by improving mitochondrial homeostasis and preventing ROS accumulation. Apocynin, an inhibitor of NADPH oxidase, also suppressed sevoflurane-induce apoptosis and maintained long-term memory in P6 neonatal mice exposed to 3% sevoflurane for 6 h (Sun et al. 2016b). Additionally, non-invasive environmental enrichment may attenuate anesthesia-induced epigenetic inhibition of BDNF signaling and memory loss in rodent models (Wu et al. 2016). However, only very limited animal studies about these agents have been reported, so their efficacies remain to be further investigated. On the other hand, simple intranasal administration of insulin prior to anesthesia has been shown to protect adult mice from anesthesia-induced over-activation of neuronal apoptosis and alterations of synaptic proteins and cognitive impairment (Chen et al. 2014b, 2017; Li et al. 2019b; Zhang et al. 2016). Insulin also prevents neonatal mice from anesthesia-induced over-activation of neuronal apoptosis, reduction of PSD-95, and cognitive impairment later in life up to old age (Li et al. 2019a, and the present study). Thus, pre-treatment with intranasal insulin could be a simple yet effective method to prevent anesthesia-induced neurotoxicity and the consequent cognitive dysfunction.
In conclusion, we found that repeated exposure of neonatal mice to anesthesia with sevoflurane caused cognitive impairment that can be detected at the age of 18 months and that pre-treatment of neonatal mice with intranasal administration of insulin can protect mice from anesthesia-induced long-term cognitive impairment. Given that intranasal administration of insulin has been found to be safe and to be beneficial to cognitive function in clinical trials, our findings provide experimental data to support the use of intranasal insulin to prevent the risk of neonatal anesthesia-induced neurotoxicity and long-term cognitive impairment.
Data Availability
The original data are available upon request to the investigators.
References
Benedict C, Hallschmid M, Hatke A, Schultes B, Fehm HL, Born J, Kern W (2004) Intranasal insulin improves memory in humans. Psychoneuroendocrinology 29:1326–1334
Benedict C, Hallschmid M, Schmitz K, Schultes B, Ratter F, Fehm HL, Born J, Kern W (2007) Intranasal insulin improves memory in humans: superiority of insulin aspart. Neuropsychopharmacology 32:239–243
Benedict C, Kern W, Schultes B, Born J, Hallschmid M (2008) Differential sensitivity of men and women to anorexigenic and memory-improving effects of intranasal insulin. J Clin Endocrinol Metab 93:1339–1344
Blazquez E, Velazquez E, Hurtado-Carneiro V, Ruiz-Albusac JM (2014) Insulin in the brain: its pathophysiological implications for states related with central insulin resistance, type 2 diabetes and Alzheimer’s disease. Front Endocrinol (Lausanne) 5:161
Boscolo A, Starr JA, Sanchez V, Lunardi N, DiGruccio MR, Ori C, Erisir A, Trimmer P, Bennett J, Jevtovic-Todorovic V (2012) The abolishment of anesthesia-induced cognitive impairment by timely protection of mitochondria in the developing rat brain: the importance of free oxygen radicals and mitochondrial integrity. Neurobiol Dis 45:1031–1041
Brambrink AM, Evers AS, Avidan MS, Farber NB, Smith DJ, Martin LD, Dissen GA, Creeley CE, Olney JW (2012) Ketamine-induced neuroapoptosis in the fetal and neonatal rhesus macaque brain. Anesthesiology 116:372–384
Briner A, Nikonenko I, De Roo M, Dayer A, Muller D et al (2011) Developmental stage-dependent persistent impact of propofol anesthesia on dendritic spines in the rat medial prefrontal cortex. Anesthesiology 115:282–293
Chen Y, Deng Y, Zhang B, Gong CX (2014a) Deregulation of brain insulin signaling in Alzheimer’s disease. Neurosci Bull 30:282–294
Chen Y et al (2014b) Intranasal insulin prevents anesthesia-induced hyperphosphorylation of tau in 3xTg-AD mice. Front Aging Neurosci 6:100
Chen Y, Dai CL, Wu Z, Iqbal K, Liu F et al (2017) Intranasal insulin prevents anesthesia-induced cognitive impairment and chronic neurobehavioral changes. Front Aging Neurosci 9:136
Claxton A, Baker LD, Wilkinson CW, Trittschuh EH, Chapman D, Watson GS, Cholerton B, Plymate SR, Arbuckle M, Craft S (2013) Sex and ApoE genotype differences in treatment response to two doses of intranasal insulin in adults with mild cognitive impairment or Alzheimer’s disease. J Alzheimers Dis 35:789–797
Claxton A, Baker LD, Hanson A, Trittschuh EH, Cholerton B, Morgan A, Callaghan M, Arbuckle M, Behl C, Craft S (2015) Long-acting intranasal insulin detemir improves cognition for adults with mild cognitive impairment or early-stage Alzheimer’s disease dementia. J Alzheimers Dis 44:897–906
Craft S, Baker LD, Montine TJ, Minoshima S, Watson GS, Claxton A, Arbuckle M, Callaghan M, Tsai E, Plymate SR, Green PS, Leverenz J, Cross D, Gerton B (2012) Intranasal insulin therapy for Alzheimer disease and amnestic mild cognitive impairment: a pilot clinical trial. Arch Neurol 69:29–38
Craft S, Claxton A, Baker LD, Hanson AJ, Cholerton B, Trittschuh EH, Dahl D, Caulder E, Neth B, Montine TJ, Jung Y, Maldjian J, Whitlow C, Friedman S (2017) Effects of regular and long-acting insulin on cognition and Alzheimer’s disease biomarkers: a pilot clinical trial. J Alzheimers Dis 57:1325–1334
Creeley C, Dikranian K, Dissen G, Martin L, Olney J, Brambrink A (2013) Propofol-induced apoptosis of neurones and oligodendrocytes in fetal and neonatal rhesus macaque brain. Br J Anaesth 110(Suppl 1):i29–i38
Crosby G, Culley DJ, Patel PM (2010) At the sharp end of spines: anesthetic effects on synaptic remodeling in the developing brain. Anesthesiology 112:521–523
D’Hooge R, De Deyn PP (2001) Applications of the Morris water maze in the study of learning and memory. Brain Res Brain Res Rev 36:60–90
Dai CL, Tung YC, Liu F, Gong CX, Iqbal K (2017) Tau passive immunization inhibits not only tau but also Abeta pathology. Alzheimers Res Ther 9:1
Di J, Cohen LS, Corbo CP, Phillips GR, El Idrissi A, Alonso AD (2016) Abnormal tau induces cognitive impairment through two different mechanisms: synaptic dysfunction and neuronal loss. Sci Rep 6:20833
Dobbing J, Sands J (1979) Comparative aspects of the brain growth spurt. Early Hum Dev 3:79–83
Dutta S, Sengupta P (2016) Men and mice: relating their ages. Life Sci 152:244–248
Fredriksson A, Archer T, Alm H, Gordh T, Eriksson P (2004) Neurofunctional deficits and potentiated apoptosis by neonatal NMDA antagonist administration. Behav Brain Res 153:367–376
Fredriksson A, Ponten E, Gordh T, Eriksson P (2007) Neonatal exposure to a combination of N-methyl-D-aspartate and gamma-aminobutyric acid type A receptor anesthetic agents potentiates apoptotic neurodegeneration and persistent behavioral deficits. Anesthesiology 107:427–436
Ganzberg S (2017) The FDA warning on anesthesia drugs. Anesth Prog 64:57–58
Gong CX, Iqbal K (2008) Hyperphosphorylation of microtubule-associated protein tau: a promising therapeutic target for Alzheimer disease. Curr Med Chem 15:2321–2328
Greenberg SG, Davies P, Schein JD, Binder LI (1992) Hydrofluoric acid-treated tau PHF proteins display the same biochemical properties as normal tau. J Biol Chem 267:564–569
Hallschmid M, Benedict C, Schultes B, Born J, Kern W (2008) Obese men respond to cognitive but not to catabolic brain insulin signaling. Int J Obes 32:275–282
Hanson LR, Frey WH 2nd (2008) Intranasal delivery bypasses the blood-brain barrier to target therapeutic agents to the central nervous system and treat neurodegenerative disease. BMC Neurosci 9(Suppl 3):S5
Heni M, Kullmann S, Preissl H, Fritsche A, Haring HU (2015) Impaired insulin action in the human brain: causes and metabolic consequences. Nat Rev Endocrinol 11:701–711
Hu D, Flick RP, Zaccariello MJ, Colligan RC, Katusic SK, Schroeder DR, Hanson AC, Buenvenida SL, Gleich SJ, Wilder RT, Sprung J, Warner DO (2017) Association between exposure of young children to procedures requiring general anesthesia and learning and behavioral outcomes in a population-based birth cohort. Anesthesiology 127:227–240
Iqbal K, Liu F, Gong CX (2016) Tau and neurodegenerative disease: the story so far. Nat Rev Neurol 12:15–27
Jevtovic-Todorovic V, Hartman RE, Izumi Y, Benshoff ND, Dikranian K, Zorumski CF, Olney JW, Wozniak DF (2003) Early exposure to common anesthetic agents causes widespread neurodegeneration in the developing rat brain and persistent learning deficits. J Neurosci 23:876–882
Jevtovic-Todorovic V, Absalom AR, Blomgren K, Brambrink A, Crosby G, Culley DJ, Fiskum G, Giffard RG, Herold KF, Loepke AW, Ma D, Orser BA, Planel E, Slikker W Jr, Soriano SG, Stratmann G, Vutskits L, Xie Z, Hemmings HC Jr (2013) Anaesthetic neurotoxicity and neuroplasticity: an expert group report and statement based on the BJA Salzburg Seminar. Br J Anaesth 111:143–151
Kang E, Berg DA, Furmanski O, Jackson WM, Ryu YK, Gray CD, Mintz CD (2017) Neurogenesis and developmental anesthetic neurotoxicity. Neurotoxicol Teratol 60:33–39
Kazim SF, Blanchard J, Bianchi R, Iqbal K (2017) Early neurotrophic pharmacotherapy rescues developmental delay and Alzheimer’s-like memory deficits in the Ts65Dn mouse model of Down syndrome. Sci Rep 7:45561
Krug R, Benedict C, Born J, Hallschmid M (2010) Comparable sensitivity of postmenopausal and young women to the effects of intranasal insulin on food intake and working memory. J Clin Endocrinol Metab 95:E468–E472
Li H, Dai CL, Gu JH, Peng S, Li J, Yu Q, Iqbal K, Liu F, Gong CX (2019a) Intranasal administration of insulin reduces chronic behavioral abnormality and neuronal apoptosis induced by general anesthesia in neonatal mice. Front Neurosci 13:706
Li X, Run X, Wei Z, Zeng K, Liang Z, Huang F, Ke D, Wang Q, Wang JZ, Liu R, Zhang B, Wang X (2019b) Intranasal insulin prevents anesthesia-induced cognitive impairments in aged mice. Curr Alzheimer Res 16:8–18
Lunardi N, Ori C, Erisir A, Jevtovic-Todorovic V (2010) General anesthesia causes long-lasting disturbances in the ultrastructural properties of developing synapses in young rats. Neurotox Res 17:179–188
Maloney SE, Yuede CM, Creeley CE, Williams SL, Huffman JN, Taylor GT, Noguchi KN, Wozniak DF (2019) Repeated neonatal isoflurane exposures in the mouse induce apoptotic degenerative changes in the brain and relatively mild long-term behavioral deficits. Sci Rep 9:2779
Morris RG, Garrud P, Rawlins JN, O’Keefe J (1982) Place navigation impaired in rats with hippocampal lesions. Nature 297:681–683
Nedelcovych MT, Gadiano AJ, Wu Y, Manning AA, Thomas AG, Khuder SS, Yoo SW, Xu J, McArthur JC, Haughey NJ, Volsky DJ, Rais R, Slusher BS (2018) Pharmacokinetics of intranasal versus subcutaneous insulin in the mouse. ACS Chem Neurosci 9:809–816
Novak P, Pimentel Maldonado DA, Novak V (2019) Safety and preliminary efficacy of intranasal insulin for cognitive impairment in Parkinson disease and multiple system atrophy: a double-blinded placebo-controlled pilot study. PLoS One 14:e0214364
Paule MG, Li M, Allen RR, Liu F, Zou X, Hotchkiss C, Hanig JP, Patterson TA, Slikker W Jr, Wang C (2011) Ketamine anesthesia during the first week of life can cause long-lasting cognitive deficits in rhesus monkeys. Neurotoxicol Teratol 33:220–230
Reger MA, Watson GS, Frey WH II, Baker LD, Cholerton B, Keeling ML, Belongia DA, Fishel MA, Plymate SR, Schellenberg GD, Cherrier MM, Craft S (2006) Effects of intranasal insulin on cognition in memory-impaired older adults: modulation by APOE genotype. Neurobiol Aging 27:451–458
Reger MA, Watson GS, Green PS, Baker LD, Cholerton B, Fishel MA, Plymate SR, Cherrier MM, Schellenberg GD, Frey II WH, Craft S (2008a) Intranasal insulin administration dose-dependently modulates verbal memory and plasma amyloid-beta in memory-impaired older adults. J Alzheimers Dis 13:323–331
Reger MA, Watson GS, Green PS, Wilkinson CW, Baker LD, Cholerton B, Fishel MA, Plymate SR, Breitner JCS, DeGroodt W, Mehta P, Craft S (2008b) Intranasal insulin improves cognition and modulates beta-amyloid in early AD. Neurology 70:440–448
Sanchez V, Feinstein SD, Lunardi N, Joksovic PM, Boscolo A, Todorovic SM, Jevtovic-Todorovic V (2011) General anesthesia causes long-term impairment of mitochondrial morphogenesis and synaptic transmission in developing rat brain. Anesthesiology 115:992–1002
Schmid V, Kullmann S, Gfrörer W, Hund V, Hallschmid M, Lipp HP, Häring HU, Preissl H, Fritsche A, Heni M (2018) Safety of intranasal human insulin: a review diabetes. Obes Metab 20:1563–1577
Semple BD, Blomgren K, Gimlin K, Ferriero DM, Noble-Haeusslein LJ (2013) Brain development in rodents and humans: identifying benchmarks of maturation and vulnerability to injury across species. Prog Neurobiol 106-107:1–16
Shen X, Dong Y, Xu Z, Wang H, Miao C, Soriano SG, Sun D, Baxter MG, Zhang Y, Xie Z (2013) Selective anesthesia-induced neuroinflammation in developing mouse brain and cognitive impairment. Anesthesiology 118:502–515
Stiles J, Jernigan TL (2010) The basics of brain development. Neuropsychol Rev 20:327–348
Stratmann G, Sall JW, May LD, Loepke AW, Lee MT (2010) Beyond anesthetic properties: the effects of isoflurane on brain cell death, neurogenesis, and long-term neurocognitive function. Anesth Analg 110:431–437
Sun LS, Li G, Miller TLK, Salorio C, Byrne MW, Bellinger DC, Ing C, Park R, Radcliffe J, Hays SR, DiMaggio CJ, Cooper TJ, Rauh V, Maxwell LG, Youn A, McGowan FX (2016a) Association between a single general anesthesia exposure before age 36 months and neurocognitive outcomes in later childhood. JAMA 315:2312–2320
Sun Z, Satomoto M, Adachi YU, Kinoshita H, Makita K (2016b) Inhibiting NADPH oxidase protects against long-term memory impairment induced by neonatal sevoflurane exposure in mice. Br J Anaesth 117:80–86
Tamashiro KL, Wakayama T, Blanchard RJ, Blanchard DC, Yanagimachi R (2000) Postnatal growth and behavioral development of mice cloned from adult cumulus cells. Biol Reprod 63:328–334
Tatebayashi Y, Iqbal K, Grundke-Iqbal I (1999) Dynamic regulation of expression and phosphorylation of tau by fibroblast growth factor-2 in neural progenitor cells from adult rat hippocampus. J Neurosci 19:5245–5254
van Dyck LI, Morrow EM (2017) Genetic control of postnatal human brain growth. Curr Opin Neurol 30:114–124
Vorhees CV, Williams MT (2006) Morris water maze: procedures for assessing spatial and related forms of learning and memory. Nat Protoc 1:848–858
Walsh RN, Cummins RA (1976) The Open-Field Test: a critical review. Psychol Bull 83:482–504
Walters JL, Paule MG (2017) Review of preclinical studies on pediatric general anesthesia-induced developmental neurotoxicity. Neurotoxicol Teratol 60:2–23
Wilder RT, Flick RP, Sprung J, Katusic SK, Barbaresi WJ, Mickelson C, Gleich SJ, Schroeder DR, Weaver AL, Warner DO (2009) Early exposure to anesthesia and learning disabilities in a population-based birth cohort. Anesthesiology 110:796–804
Wu J, Bie B, Naguib M (2016) Epigenetic manipulation of brain-derived Neurotrophic factor improves memory deficiency induced by neonatal anesthesia in rats. Anesthesiology 124:624–640
Yon JH, Daniel-Johnson J, Carter LB, Jevtovic-Todorovic V (2005) Anesthesia induces neuronal cell death in the developing rat brain via the intrinsic and extrinsic apoptotic pathways. Neuroscience 135:815–827
Yon JH, Carter LB, Reiter RJ, Jevtovic-Todorovic V (2006) Melatonin reduces the severity of anesthesia-induced apoptotic neurodegeneration in the developing rat brain. Neurobiol Dis 21:522–530
Yonamine R, Satoh Y, Kodama M, Araki Y, Kazama T (2013) Coadministration of hydrogen gas as part of the carrier gas mixture suppresses neuronal apoptosis and subsequent behavioral deficits caused by neonatal exposure to sevoflurane in mice. Anesthesiology 118:105–113
Zhang Y, Dai CL, Chen Y, Iqbal K, Liu F, Gong CX (2016) Intranasal insulin prevents anesthesia-induced spatial learning and memory deficit in mice. Sci Rep 6:21186
Zhao WQ, Chen H, Quon MJ, Alkon DL (2004) Insulin and the insulin receptor in experimental models of learning and memory. Eur J Pharmacol 490:71–81
Zhu C, Gao J, Karlsson N, Li Q, Zhang Y, Huang Z, Li H, Kuhn HG, Blomgren K (2010) Isoflurane anesthesia induced persistent, progressive memory impairment, caused a loss of neural stem cells, and reduced neurogenesis in young, but not adult, rodents. J Cereb Blood Flow Metab 30:1017–1030
Zou X, Liu F, Zhang X, Patterson TA, Callicott R, Liu S, Hanig JP, Paule MG, Slikker W Jr, Wang C (2011) Inhalation anesthetic-induced neuronal damage in the developing rhesus monkey. Neurotoxicol Teratol 33:592–597
Acknowledgments
We thank Jeffrey Goodman, PhD, and Maureen Marlow of the New York State Institute for Basic Research in Developmental Disabilities, Staten Island, New York, USA, for the use of gas anesthesia equipment and for editing of the manuscript, respectively.
Funding
This work was supported in part by the New York State Office for People with Developmental Disabilities, Albany, NY, and a scholarship (to H.L.) from Guangzhou First People’s Hospital, School of Medicine, South China University of Technology, Guangzhou, China.
Author information
Authors and Affiliations
Contributions
C-lD, C-XG, FL, and KI: designed research; C-lD, HL, XH, and JZ: performed research; C-lD, HL, XH, JZ, and C-XG: analyzed data; C-lD and C-XG: wrote the paper.
Corresponding author
Ethics declarations
Conflict of Interest
K.I. serves on the scientific advisory board of AXON Neuroscience, has received research grants from Ever NeuroPharma and Signum Biosciences, and holds several patents on treatment of Alzheimer’s disease and related conditions. C.-X.G. serves on the scientific advisory board of Alectos Therapeutics. K.I., F.L., and C.-X.G hold a patent on intranasal insulin administration for the minimization of anesthesia-induced memory loss.
Ethics Approval
The housing, breeding, and animal experiments were approved by the Institutional Animal Care and Use Committee (IACUC) of the New York State Institute for Basic Research in Developmental Disabilities and were in accordance with the PHS Policy on Human Care and Use of Laboratory animals (revised March 15, 2010).
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Code Availability
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dai, CL., Li, H., Hu, X. et al. Neonatal Exposure to Anesthesia Leads to Cognitive Deficits in Old Age: Prevention with Intranasal Administration of Insulin in Mice. Neurotox Res 38, 299–311 (2020). https://doi.org/10.1007/s12640-020-00223-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12640-020-00223-y