
Abstract
Introduction
Central venous catheters are used commonly in critical care. Evidence-based practices to prevent catheter-related bloodstream infections have been widely promoted. One such practice includes assessing the need for central venous catheters on a daily basis and removing those found to be unnecessary. However, little is known about the adherence to this recommendation. Our objective was to examine the prevalence of unnecessary central venous catheters in our intensive care units.
Methods
We performed a prospective observational study during 28 consecutive days in two adult intensive care units at an academic medical centre. The principal investigator screened patients daily for the presence of non-tunnelled central venous catheters and assessed whether there was an indication for continued central catheterization. Patients under the age of 18 were excluded, as were those undergoing palliative care. Standardized indications were abstracted from the patient’s chart, and the patient’s primary nurse was interviewed if there was no indication for central venous catheterization in the chart. If there were multiple catheters or indications, the most appropriate indication was recorded. The end point was to establish whether a patient had an appropriate indication for central catheterization rather than to attribute an indication to each catheter.
Results
Eighty-one patients experienced a total of 614 days with at least one central venous catheter. Forty-one (50.6%; 95% confidence interval [CI], 39.9-61.3%) of these patients had no indication on at least one central venous catheter day. Of all patient days with central venous catheters, 170 (27.7%; 95% CI, 19.5-37.9%) had no apparent indication. The proportion of patient days with central venous catheters without indication was 4.6 (95% CI, 2.6-8.2; P < 0.001) times greater in the level-2 unit than in the level-3 unit.
Discussion
In two academic adult intensive care units, a large proportion of patients with central venous catheters lacked an ongoing indication for their use during a significant period of time. Many patients were exposed to complications from unneeded catheters. Our findings will serve as a baseline for determining the success of quality-improvement interventions to prevent complications such as catheter-related infections in our program.
Résumé
Introduction
Les cathéters veineux centraux sont couramment utilisés en soins critiques. Les pratiques basées sur des données probantes visant à éviter les infections du sang ont fait l’objet d’une importante promotion. L’une de ces pratiques consiste à évaluer le besoin de poser des cathéters veineux centraux quotidiennement et à retirer ceux qui ne sont pas nécessaires. Toutefois, nous ne savons pas si cette recommandation est bien suivie ou non. Notre objectif était d’examiner la prévalence de cathéters veineux centraux non nécessaires dans nos unités de soins intensifs.
Méthode
Nous avons réalisé une étude observationnelle prospective durant 28 jours consécutifs dans deux unités de soins intensifs pour adultes d’une institution médicale universitaire. Le chercheur principal a quotidiennement passé en revue les patients afin d’examiner si des cathéters veineux centraux non tunnellisés étaient posés et a évalué si la continuation du cathétérisme central était indiquée. Les patients âgés de moins de 18 ans étaient exclus de l’étude, tout comme les patients en soins palliatifs. Les indications standardisées ont été extraites des dossiers des patients, et l’infirmière responsable du patient a été interrogée s’il n’y avait pas d’indication pour un cathétérisme veineux central dans le dossier. S’il y avait plusieurs cathéters ou indications, l’indication la plus adaptée a été enregistrée. Le critère de recherche principal était d’établir si un patient avait une indication justifiant un cathétérisme central plutôt que d’attribuer une indication pour chaque cathéter.
Résultats
Quatre-vingt-un patients ont passé un total de 614 jours avec au moins un cathéter veineux central. Quarante-et-un (50,6 %; intervalle de confiance [IC] 95 %, 39,9-61,3 %) de ces patients n’avaient pas d’indication pour au moins un jour de cathétérisme veineux central. Pour tous les jours-patient avec cathéters veineux centraux, 170 (27,7 %; IC 95 %, 19,5-37,9 %) patients ne présentaient pas d’indication apparente. La proportion de jours-patient avec des cathéters veineux centraux sans indication était 4,6 (IC 95 %, 2,6-8,2; P < 0,001) fois plus importante dans l’unité de niveau 2 que dans l’unité de niveau 3.
Discussion
Dans deux unités de soins intensifs pour adultes, une importante proportion de patients ayant des cathéters veineux centraux n’avaient pas d’indication continue pour leur utilisation pendant une période de temps significative. De nombreux patients ont été exposés à des complications en raison de cathéters non nécessaires. Nos résultats serviront de base pour déterminer la réussite des interventions d’amélioration de la qualité afin d’éviter des complications telles que les infections liées aux cathéters dans notre programme.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Central venous catheters are invaluable in the intensive care unit (ICU). Standard indications include venous access (including need for frequent blood draws), monitoring, cardiac pacing, hemodialysis, and intravenous therapies (for example, inotropes, vasopressors, total parenteral nutrition, chemotherapy, and long term antibiotics).1
Central venous catheters are associated with mechanical, thrombotic, and infectious complications.1 A systematic review by Maki et al. in 2005 estimated short-term non-cuffed non-tunnelled non-medicated catheters to have 4.4 catheter-related bloodstream infections per 100 catheters and 2.7 catheter-related bloodstream infections per 1,000 intravascular device days.2 In particular, this systematic review supports the patient safety practice of reporting catheter-related bloodstream infections per intravascular device days rather than solely per catheter placement.2 The impact of catheter-related bloodstream infections is substantial; not only are there increased associated costs, but there is also an estimated attributable mortality of 35%.3
Several practices have been proposed to reduce the incidence of catheter-related infections.4 , 5 Some practices are applicable to the catheter’s insertion, others to its maintenance.6 , 7 A daily review of the catheter’s necessity is basic to maintenance practices. As the incidence of catheter-related infection appears to be associated with the duration of catheterization, maintaining a catheter in situ should lead to an increased rate of infection.2 However, no studies directly connect increased catheter-related bloodstream infections with the prevalence of unnecessary central catheters. Quantifying the proportion of unnecessary central catheters would reinforce the importance of daily assessment of central catheters and provide a baseline for determining the effectiveness of systematic quality improvement interventions. Therefore, we undertook this study to uncover the baseline prevalence of unnecessary central venous catheters in our ICUs.
Methods
The Queen’s University Research Human Ethics Board approved this study.
Study population
We undertook a prospective observational study at a tertiary care teaching centre, a 456-bed hospital with a catchment area of over 500,000 persons. The adult critical care program consists of a 21-bed level-3 unit and an 18-bed level-2 unit. The level-2-unit provides care for patients who require continuous cardiac and vital sign monitoring, low doses of vasoactive medications, and non-invasive positive pressure ventilation. The level-3 unit provides the full range of ICU care, including mechanical ventilation. In addition, the level-3 unit is a “closed” unit with primary comprehensive care provided by designated critical care physicians. The level-2 unit operates as an “open” unit where patient care is provided by various clinical services. Both units have dedicated critical care nursing staff. The usual nurse to patient ratio is 1:1 in the level-3 unit and 1:2 in the level-2 unit. In the level-3 unit, bedside rounds occur three times a day, with formal administrative rounds and a conference with senior physicians and nursing staff each weekday. In the level-2 unit, individual services determine rounding structures. Patients might stay in both units during the same admission; a patient is occasionally transferred between the level-2 and level-3 units. For example, a patient already admitted to the level-2 ICU may deteriorate and require endotracheal intubation, which will automatically lead to a transfer to the level-3 ICU. Alternatively, usual practice in the level-3 ICU is to discharge recovering patients to the level-2 ICU. In addition, the level-3-unit provides overflow capacity for the level-2-unit. During this study, there was no system-based process in either of our ICUs to ensure adherence to maintenance practices, including daily assessment.
Data collection
During 28 consecutive days, the principal investigator screened patients in these units for any temporary non-tunnelled central venous catheter, including peripherally inserted central catheters (PICC). Patients under the age of 18 or undergoing palliative care were excluded. The current indication to maintain ongoing catheterization was abstracted from patient records for the previous 24-hr period, which corresponded to the end of a 12-hr nursing documentation period and shift change. Standard indications for central venous catheterization were recorded in the following categories: 1) therapies, 2) renal replacement therapy, 3) venous access, 4) monitoring, and 5) cardiac pacing.1 These categories reflect not only the literature but also our institutional practices. If there were multiple catheters or indications, the most appropriate indication for having central catheterization was recorded. The end point was to determine whether a patient had an appropriate indication for central catheterization rather than to attribute an indication to each catheter. If there were more than one indication, central catheterization was designated as necessary, and the principal investigator chose an indication that was most appropriate. We did not assign a specific hierarchy for indications, other than considering lack of vascular access (or need for frequent blood draws) only if there was no other clear indication. The outcome was whether an indication for central catheterization existed. Multiple catheters were not adjudicated to assess if minimization of catheterization could be achieved, although the number and site of each catheter was recorded daily for each patient. For example, if a patient receiving vasopressors and long-term antibiotics had both PICC and internal jugular vein catheters, then central catheterization was recorded as necessary with vasopressor as the indication. If the vasopressors were stopped two days later, then central catheterization was still recorded as necessary with long-term antibiotics as the indication, even though two catheters remained in place.
We were liberal in assigning indications. Our focus was not on indications for initial insertion but rather on indications for maintaining in situ catheterization. For example, on the first day post procedure, we recorded “monitoring” as an indication for central venous catheters for patients with recent procedures such as surgery or extubation. If a central venous catheter was inserted in a patient without previous central catheterization and if there was no indication found for the catheterization, monitoring was also recorded as an indication. Similarly, vasoactive medications needed to be discontinued for at least 24 hr before that indication was considered as no longer being present.
If there was no apparent reason for central venous catheters, the primary bedside nurse was interviewed. If the reason for central venous catheters was “lack of peripheral access”, the nurse was asked whether peripheral access was theoretically attainable. If so, “no indication for central catheterization” was recorded for that patient for that day unless the nurse indicated that the central venous catheter was required for frequent blood draws. If there was variance among nurses with regard to attainability of peripheral venous access for the same patient but on different days, then the indication, or lack thereof, was recorded each study day based on input from the patient’s primary nurse. We did not interact with the physician service or interview or examine patients.
Statistical analysis and sample size considerations
Based on our experience with the two ICUs, we estimated that we would observe approximately 600 days with central venous catheters on 80 patients during a four-week study period. Such a sample size would provide estimates at the patient level to within ± 11% at least 19 times out of 20. The precision of estimates at the daily level would depend on the within patient dependence between days, which could range from ± 4% under complete independence to ± 11% if the outcome variable remained constant within patients.
To account for dependencies induced by the repeated daily observations per patient, risk estimates, P values, and relative risks with 95% confidence intervals were estimated by generalized estimating equations with robust standard errors using PROC GENMOD (SAS version 9.1.3, SAS Institute Inc., Cary, NC, USA) with a binomial distribution and logit link for risks or log link for risk ratios.8
Results
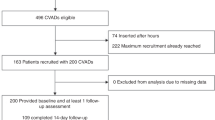
Table 1 details patient demographics. Of 81 patients, 26 patients were admitted to the level-3 unit exclusively, 44 patients were admitted to the level-2 unit exclusively, and 11 patients were admitted to both units at different times. These 11 patients were intermingled between the two units in a relatively short time period.
There were 614 patient days with central venous catheters, 422 (68.7%) patient days in the level-3 unit and 192 (31.3%) patient days in the level-2 unit. Table 2 shows the recorded indications for patient days with central catheterization with no specific hierarchy for indications (other than lack of peripheral catheterization). Forty-one (50.6%; 95% confidence interval [CI], 39.9-61.3%) patients had at least one day with unnecessary central venous catheters, and 31 (38.3%; 95% CI, 28.4-49.3%) patients had at least two consecutive days with unnecessary central venous catheters. Of all patient days with central venous catheters, 170 (27.7%; 95% CI, 19.5-37.8%) had no apparent indication. Fifty-five of these days were recorded in the level-3 unit, and 115 days were recorded in the level-2 unit, representing 13.0% (95% CI, 7.5-21.6%) and 59.9% (95% CI 42.6-75.1%) of all patient days with central venous catheters in these units, respectively. The proportion of patient days with central venous catheters without indication was 4.6 (95% CI, 2.6-8.2; P < 0.001) times greater in the level-2 unit compared with the level-3 unit.
Central catheter sites are presented in Table 3. Only 12.8% (95% CI, 7.9-20.2%) of all catheters – 20.5% of all catheters if PICCs are excluded – were inserted in the subclavian vein.
Discussion
In a single Ontario teaching centre’s critical care program, we found a high prevalence of unnecessary central venous catheters. During the conduct of this study, there were no system-based processes in our critical care program to ensure daily assessment of patient need for central venous catheters. “Usual care”, therefore, may fail to ensure prompt identification of unnecessary catheters.
Why didn’t clinicians remove central lines as soon as an indication was lacking? Physicians may have been balancing the risks of central catheter reinsertion against the risks of maintaining central catheterization in a patient with a high potential for deterioration or difficult catheter insertion. Also, medical teams may have lacked appreciation of the importance of removing unnecessary catheters. Perhaps these catheters provided practitioners with a sense of security while managing critically ill patients. Possibly some catheters were removed shortly after the day they were deemed unnecessary. However, not only were we liberal in accepting indications for central catheterization, but also, we observed that about one-third of patients had at least two consecutive days with unnecessary central venous catheters.
There are several potential explanations for the difference between the level-2 and level-3 units in terms of patient days with unnecessary central venous catheters. With a greater burden of illness and elevated acuteness, level-3 unit patients are more likely to have an indication for central venous catheters compared with level-2 unit patients. Thus, the likelihood of unnecessary central venous catheters is expected to be lower for level-3 patients. Alternatively, better processes of care in the closed-model ICU may have resulted in timely removal of central venous catheters.9 However, even the relatively low prevalence in the level-3 unit (13.0%) may represent lack of reliable processes in identifying unnecessary catheters. Lastly, the comparison between the level-2 and level-3 units may be biased by the intermingling of patients, e.g., when patients were discharged from the level-3-unit to the level-2-unit with catheters in situ but lacking clear indication.
Our study has a number of strengths. First, we included patients admitted to both level-3 and level-2 units. This provides a sample representation of our critical care setting. Second, we collected data prospectively and consecutively for all admitted patients over a four-week period, which minimized the risk of sampling bias. Finally, medical teams were generally unaware of this study. Therefore, we believe our findings reflect the usual practice in our program.
Our study has important limitations. First, to facilitate data collection and to simplify determining a catheter’s necessity, we chose patient days with central venous catheters – rather than individual catheter days – as the main measure. This decision precluded us from discussing potentially important associations between unnecessary catheter days and catheter-specific variables, such as type, site, and indication. In particular, we counted PICCs with other non-tunnelled central venous catheters because they carry risks of complications comparable with other such catheters.2 Peripherally inserted central catheters are easily available in our centre and are often placed by the Interventional Radiology Service as substitutes for other central venous catheters. Perhaps clinicians perceive PICCs as harmless. Also, clinicians may be less inclined to remove an unnecessary PICC, as replacement would require one more procedure by the Interventional Radiology Service. Many patients in our study had multiple concurrent or consecutive catheters, especially PICCs. However, our outcome, being the presence of appropriate central catheterization, precludes a subset analysis to compare patients with PICCs with patients with different central catheters.
Second, we identified unnecessary catheterization based on a daily prospective chart review for predefined standard indications. To minimize bias, such as the Hawthorn Effect, we did not interview the physician teams caring for the patients, and we cannot comment on physician perceptions. We may have failed to capture acceptable indications for central venous catheters outside of those we predefined. Since we did interact with the nursing staff, there was the potential of biasing the nurses towards assessing the need for central venous catheters more frequently and thereby influencing the physician teams indirectly. Moreover, as we were liberal in accepting indications for central venous catheters, we may have underestimated the true prevalence of patient days with unnecessary central catheterization.
Third, the mixed patient populations (level-3 and level-2 ICUs) and care delivery models (closed vs open model) challenge the interpretation of our results. For example, it is possible that the perceptions of health care teams regarding the detrimental effects of central venous catheters on patients varied according to patients’ severity of illness. This may have contributed to increased rates of unnecessary catheters in the level-2 ICU. In addition, the differences between the two units may be attributable to the care delivery model. We chose to present the differences between the two units due to their magnitude. Our data did not allow us to assess the reasons for the differences in the proportions of unnecessary catheters between our ICUs.
We performed this study in a single centre; therefore, our findings cannot be directly generalized to other organizations. For example, extensive use of PICCs may be unique to our centre. In addition, a single observer gathered the data for this study, which may introduce further potential for bias. We minimized this possibility by using a strict list of indications for central catheterization with little occasion for personal adjudication. As we were liberal in accepting indications for central catheterization and as a patient was only deemed to have unnecessary catheterization after interviewing the primary bedside nurse, it is more likely that we underestimated the rate of unnecessary catheterization.
Reliable daily assessments of central catheters and prompt removal of unnecessary catheters may vary among different critical care environments and organizations. Our study was not designed to determine reasons for noncompliance with central catheter maintenance practices but was designed, instead, to describe its extent. Utilization of best practices is influenced by many factors.10 As with other clinical practices, achievement of good performance may require the addition of system-based tools, such as checklists and performance feedback.11 – 13
In conclusion, in a single academic centre, a significant proportion of critically ill patients with central venous catheters had no clear indication for ongoing central venous catheterization. This study will serve as baseline data to inform the success of a planned quality-improvement intervention to identify and remove any unnecessary central venous catheters.
References
Irwin RS, Rippe JM, Lisbon A, Heard SO. Procedures, Techniques and Minimally Invasive Monitoring in Intensive Care Medicine. Fourth edition ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008.
Maki DG, Kluger DM, Crnich CJ. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clin Proc 2006; 81: 1159-71.
Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med 2006; 355: 2725-32.
Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and attributable mortality. JAMA 1994; 271: 1598-601.
Berenholtz S, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med 2009; 32: 2014-20.
O’Grady NP, Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. Centers for Disease Control and Prevention. MMWR Recomm Rep 2002; 51: 1-29.
Canadian ICU Collaborative Faculty. CLI: Getting Started Kit. Prevent Central Line Infections. Central Line Associated – Blood Stream Infections (CLA-BSI). How-to Guide. Available from URL: http://www.saferhealthcarenow.ca/EN/Interventions/CLI/Pages/gsk.aspx. (accessed June 2010).
McNutt LA, Wu C, Xue X, Hafner JP. Estimating the relative risk in cohort studies and clinical trials of common outcomes. Am J Epidemiol 2003; 157: 940-3.
Gutsche JT, Kohl BA. Who should care for intensive care unit patients? Crit Care Med 2007; 35: S18-23.
Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999; 282: 1458-65.
Jones NE, Suurdt J, Ouelette-Kuntz H, Heyland DK. Implementation of the Canadian Clinical Practice Guidelines for Nutrition Support: a multiple case study of barriers and enablers. Nutr Clin Pract 2007; 22: 449-57.
Levy MM, Abraham E, Zilberberg M, MacIntyre NR. A descriptive evaluation of transfusion practices in patients receiving mechanical ventilation. Chest 2005; 127: 928-35.
Sinuff T, Cook D, Giacomini M, Heyland D, Dodek P. Facilitating clinician adherence to guidelines in the intensive care unit: a multicenter, qualitative study. Crit Care Med 2007; 35: 2083-9.
Funding
None.
Competing interests
None declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cload, B., Day, A.G. & Ilan, R. Evaluation of unnecessary central venous catheters in critically ill patients: a prospective observational study. Can J Anesth/J Can Anesth 57, 830–835 (2010). https://doi.org/10.1007/s12630-010-9348-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-010-9348-7