
Abstract
Anthracyclines and taxanes are cytotoxic agents commonly used for treatment of breast cancer, including in adjuvant, neoadjuvant, and metastatic settings. Each drug class is associated with cumulative and potentially irreversible toxicity, including cardiomyopathy (anthracyclines) and neuropathy (taxanes). This may either limit the duration of therapy for advanced disease, or prevent retreatment for recurrence if previously used as component of adjuvant or neoadjuvant therapy. Several classes of cytotoxic agent have been evaluated in patients with anthracycline and taxane-pretreated metastatic breast cancer (MBC), including other antitubulins (vinorelbine, ixabepilone, eribulin), antimetabolites (capecitabine, gemcitabine), topoisomerase I inhibitors (irinotecan), platinum analogues (cisplatin, carboplatin), and liposomal doxorubicin preparations. No trials have shown an overall survival advantage for combination chemotherapy in this setting, indicating that single cytotoxic agents should usually be used, expect perhaps for patients with rapidly progressive disease and/or high tumor burden.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Anthracyclines and taxanes are the two most active classes of cytotoxic agent for early and advanced stage breast cancer, and are thus commonly used as a component of either adjuvant or neoadjuvant therapy [1], and/or for patients with metastatic breast cancer (MBC) [2]. Anthracyclines are not usually used for metastatic disease if previously used for adjuvant therapy, because of the potential for cumulative cardiac toxicity, although liposomal anthracyclines may be safely used for patients with a history of exposure to anthracyclines [3•]. Anthracyclines are also often not considered even if there has been no previous adjuvant exposure, because they are generally less effective than taxanes as first-line therapy [4, 5] and because there are often other alternatives for second-line therapy or beyond. The purpose of this review is to summarize available information about cytotoxic agents that have been evaluated specifically for patients with anthracycline and taxane-pretreated metastatic breast cancer (MBC), with a focus on pivotal phase II or III trials which contributed to drug approval or provided important information for use of commonly used cytotoxic agents in this setting.
Objectives of Systemic Cytotoxic Therapy
Cytotoxic therapy is usually reserved for patients with “triple negative” cancers, estrogen-receptor (ER)-positive cancers that have become resistant to endocrine therapy, or cancers that are rapidly progressive and/or associated with high visceral tumor burden. Cytotoxic therapy is commonly used in combination with anti-HER2 directed therapy in patients with HER2/neu overexpressing disease, because it has been shown to improve survival compared with chemotherapy alone [6••]. For patients with hormone receptor-positive disease, however, concurrent use of chemotherapy plus endocrine therapy is not more effective than chemotherapy alone [7]. Virtually all patients with MBC will receive chemotherapy at some point during their course, expect perhaps the very elderly, frail, or infirm.
Although patients with distant metastatic disease are usually regarded as incurable, systemic cytotoxic therapy improves survival, delays progression of the disease, and may result in symptom palliation [8–10] Moreover, up to 10 % of patients with MBC may survive beyond 10 years or longer, particularly if there has been an objective response to cytotoxic therapy [11]. Of the hundreds of phase III trials in MBC that have been performed over the past three decades, survival in the experimental group was significantly improved for a handful only [6••, 12, 13••, 14]. Despite difficulty in demonstrating improved survival in individual trials, population-based studies suggest that patients with MBC are now surviving modestly longer than in the past [15–17]. The improvement observed in population-based studies may be because of the increased availability of drugs which when used individually have no or minimal effect in prolonging life, but when used sequentially can result in modest increases in survival. Other studies, however, suggest that improved survival in recent years for patients who relapse after adjuvant chemotherapy may solely be for patients with short relapse-free interval, suggesting that this effect may be attributable to the availability of anti-HER2 directed therapy in recent years rather than the availability of new cytotoxic agents [18].
Resistance to Cytotoxic Therapy
Although an objective response or a period of disease stabilization is observed for most patients after cytotoxic therapy for metastatic disease, resistance invariably develops. Although there is no accepted standardized definition of resistance, some very large phase III trials have provided very specific definitions used to select patients for inclusion in the trials [19, 20••]. Resistance is not synonymous with pretreatment. For the purpose of this review, “pretreatment” is defined as previous exposure to an agent as a component of therapy in the adjuvant, neoadjuvant, or metastatic setting. “Resistance” is defined as disease progression during therapy for metastatic disease, or relapse 6–12 months after completing adjuvant therapy, a definition that has correlated with lower response and shorter time to disease progression when cytotoxic therapy is used for second-line treatment or beyond [21•]. For patients who relapse 12 months or more after completing adjuvant chemotherapy, the clinical benefit of retreatment with the same regimen is comparable with that observed when they are not pretreated [22, 23].
Mechanisms of Drug Resistance
Several mechanisms of drug resistance have been identified, including P-glycoprotein mediated drug resistance (MDR-1 or MRP), which may affect sensitivity to multiple agents, or mechanisms associated with resistance to specific agents or drug classes, for example topoisomerase II gene amplification (anthracyclines) or alterations in glutathione levels (alkylating agents) or beta-tubulin isoform expression (antitubulins). Use of cytotoxic agents in combination is a strategy that has been used to overcome resistance to therapy [24]. Use of agents, for example P-glycoprotein-modifying agents, to reverse drug resistance have been ineffective [25]. There are no clinically validated assays that define drug-resistant tumors.
Approach for Patients with Anthracycline and Taxane-Pretreated Metastatic Breast Cancer
For these patients, five questions should be considered when formulating a treatment plan (Fig. 1):
-
First, what is the patient’s previous cytotoxic drug history? This will affect the selection of agents for defining a list of potentially suitable agents.
-
Second, are there comorbidity or residual toxicity from previous cytotoxic therapy? This may limit the list of potentially suitable agents that were initially defined in reviewing the treatment history.
-
Third, is there evidence of resistance in addition to pretreatment?
-
Fourth, should the cytotoxic agent chosen be used alone, or in combination with biological therapy? Patients with HER2/neu-overexpressing disease should almost always receive anti-HER2 directed therapy in combination with cytotoxic therapy because of evidence that concurrent therapy improves clinical outcomes compared with cytotoxic therapy alone [6••, 26].
-
Fifth, if cytotoxic therapy alone is used, should it be used as a single agent, or in combination with other cytotoxic agents? Single cytotoxic agents should be suitable in most cases, although combination therapy may be considered for patients with rapidly progressive disease, high visceral tumor burden, or impaired performance status, which is often associated with the former.

Algorithm for selecting chemotherapy regimen
Cytotoxic Agents Commonly Used for Anthracycline and Taxane-Pretreated Metastatic Breast Cancer
Three cytotoxic drugs, capecitabine, ixabepilone and eribulin, are currently approved for anthracycline and taxane-pretreated MBC. One (eribulin) is approved as monotherapy only whereas others are approved either as monotherapy or in combination. Other agents not specifically approved for this indication but are commonly used in clinical practice either alone or in combination with other cytotoxic agents and/or biological treatments include antimetabolites (gemcitabine), platinum analogues (cisplatin, carboplatin), antitubulins (vinorelbine, docetaxel), topoisomerase I inhibitors (irinotecan), liposomal anthracyclines (pegylated liposomal anthracyclines), and other agents that are rarely used because of their toxicity profile (mitomycin-C). Their mechanisms of action are listed in Table 1.
Capecitabine
Capecitabine is an orally available prodrug that is enzymatically converted to the antimetabolite 5-fluorouracil (5-FU). It was approved by the United States Food and Drug Administration (FDA) on the basis of activity observed in phase II trials for patients with anthracycline and taxane pretreated MBC [27••]. For a capecitabine dose and schedule of 1250 mg m−2 PO BID for 14 days of every 21 days for 163 patients with MBC and 2 or 3 previous chemotherapy regimens for MBC, objective response was 20 %, median response duration was 8.1 months, and median overall survival was 12.8 months. The most common grade 3 or 4 side effects included diarrhea (14 %) and hand–foot syndrome (10 %), and dose reductions for toxicity were common. Clinicians typically use lower doses (1000 mg m−2 PO BID) and different schedules (1 week on then 1 week off), which seem to improve tolerability without compromising efficacy [28, 29]. Although the drug is available as 500-mg and 150-mg tablets, most clinicians round the dose to the nearest 500 mg for greater patient convenience. Capecitabine monotherapy is also commonly used as first-line therapy for MBC because it does not cause alopecia or myelosuppression.
Capecitabine has also been evaluated in combination with biological agents. In HER2/neu overexpressing disease, combination with the HER2 tyrosine kinase inhibitor lapatinib was shown to be more effective than capecitabine alone for patients with disease resistant to trastuzumab plus taxane therapy, and is an approved combination. In predominantly HER2 non-expressing disease, a phase III trial found that although addition of bevacizumab to capecitabine improved response (19.8 % vs. 9.1 %; P = 0.001) for patients with anthracycline and taxane-pretreated MBC, there was no improvement in progression-free survival (the primary study endpoint) or overall survival [30].
Ixabepilone Alone or in Combination with Capecitabine
The epothilones, similar to the taxanes, bind to tubulin and stabilize microtubules but are active in taxane-resistant cell lines [31, 32]. Ixabepilone is a semisynthetic analogue of epothilone B, a natural product derived from the myxobacterium Sorangium cellulosum. It is approved as a single agent for patients with anthracycline, taxane, and capecitabine-resistant disease, and in combination with capecitabine for patients with anthracycline and taxane-resistant disease. Patients were required to meet strict pretreatment and resistance definitions for inclusion in the trials. In addition, patients with grade 2 or higher neuropathy were not eligible.
The first trial that supported regulatory approval of ixabepilone evaluated it as monotherapy (40 mg m−2 IV over three hours every three weeks) for 126 women with anthracycline, taxane, and capecitabine-resistant disease [33]. Resistance was defined as disease progression during therapy, or within eight weeks of the last dose, for metastatic disease, recurrence within six months of the last dose of adjuvant or neoadjuvant anthracyclines and/or taxanes therapy, or recurrence after previous trastuzumab (for the 7 % of patients who had HER2-overexpressing disease). The response, by central radiographic review, for 113 evaluable patients was 12.4 % (95 % confidence interval (CI) 6.9, 19.9 %); investigator-assessed response for 126 evaluable patients was 18.3 % (95 % CI 11.0, 26.1 %). The most common grade 3 or 4 treatment-related adverse events occurring in at least 10 % of patients included neutropenia (54 %), sensory peripheral neuropathy (14 %), and fatigue/asthenia (13 %).
The second trial which supported regulatory approval of ixabepilone was a phase III trial of ixabepilone (40 mg m−2 IV over three hours every three weeks) plus capecitabine (1000 mg m−2 BID days 1–14) compared with capecitabine alone (1250 mg m−2 BID on days 1–14) for 752 patients with MBC resistant to anthracyclines and taxanes (Table 2) [19, 20••]. Anthracycline and taxane resistance was defined as tumor progression during treatment or within four months of last dose in the metastatic setting, or recurrence within 12 months in the neoadjuvant or adjuvant setting. All patients were required to have measurable disease. Median progression-free survival (PFS) based on central radiology review was significantly prolonged by the combination compared with capecitabine monotherapy (5.8 vs. 4.2 months, P < 0.0001), the primary study endpoint. The combination was also associated with significantly improved response (35 % vs. 14 %; P < 0.0001) but not overall survival (OS). Grade 3 or 4 adverse events, including neutropenia (68 % vs. 11 %), sensory neuropathy (21 % vs. 0 %), and fatigue (16 % vs. 4 %), occurring in at least 10 % of patients, were more common in the combination group. In addition, the incidence of toxic death was higher in the combination group (3 % vs. 1 %). All deaths within 30 days of last dose in the combination group were related to neutropenia, and the risk was greatest for those with baseline grade 2 or higher elevation in liver chemistry; 5 of 16 such patients (31 %) died, compared with 7 of 353 patients (2 %) with no or grade 1 liver dysfunction; this led to amendment of the study protocol excluding those with grade 2 or higher liver dysfunction at baseline.
A second phase III study randomized 1221 patients with MBC to a combination of ixabepilone and capecitabine or capecitabine alone using the same doses, schedules, and dose modification criteria as in the previous trial (Table 2) [19, 20••]. In contrast with the previous trial, the primary endpoint was OS (rather than PFS). Patients with non-measurable or measurable disease (rather than measurable disease only) were eligible. In addition, although anthracycline and taxane pretreatment were also required, patients were not required to have resistant disease. The study was powered to detect a 20 % reduction in the hazard ratio for death, but failed to show a significant OS benefit in the primary unadjusted analysis (median 16.4 vs. 15.6 months; hazard ratio (HR) 0.9; 95 % CI 078–1.03; P = 0.12). Benefit from the combination was observed in the pre-specified analysis after adjustment for baseline covariates (HR = 0.85; 95 % CI: 0.75, 0.98; P = 0.023). Similar to the previous trial, significantly improved median PFS (6.2 vs. 4.2 months; HR 0.79; P = 0.0005) and objective response (43 % vs. 29 %, P = 0.0001) were observed in the combination group for patients with measurable disease. The toxicity patterns in this trial were similar to those in the previous phase III trial, although fewer patients (3 % vs. 7 %) treated with the combination died during therapy in this study. In addition, the number of treatment-associated deaths was similar in the two groups (0.7 % vs. 0.3 %); this was attributed to the exclusion from this trial of patients with hepatic dysfunction. Combined analysis of both trials indicated that patients with impaired performance status (Karnofsky performance status 70–80) derived greater clinical benefit from the combination and that excessive toxicity was not observed [34•].
Eribulin
Eribulin mesylate is a non-taxane microtubule dynamic inhibitor. It is a structurally simplified synthetic derivative of halichondrin B, a natural product derived from the marine sponge Halichonria okidai. It has a novel mode of action, causing tubulin sequestration into nonfunctional aggregates. This suppresses microtubule polymerization and causes irreversible mitotic block, cell cycle arrest, and apoptosis, and is active against paclitaxel-resistant cell lines [35]. The principal dose limiting toxicity in phase I trials was neutropenia.
After several phase II trials identified clinical activity of single-agent eribulin for patients with anthracycline and taxane-pretreated disease [36–38], a phase III trial compared eribulin (1.4 mg m−2 IV over 3–5 minutes on days 1–8 every 21 days) with physicians’ choice of therapy for 762 patients with locally recurrent or MBC who had received between two and five previous regimens that included an anthracycline and a taxane (Table 2) . Patients were also required to have received at least two agents for advanced disease and have disease progression within six months of their last chemotherapy regimen. In contrast with previous trials with ixabepilone, patients with grade 2 neuropathy were eligible [13••]. Patients were randomly assigned 2:1 to eribulin or treatment of physician’s choice, a discretionary selection of any monotherapy, which included vinorelbine (25 %), gemcitabine (19 %), capecitabine (18 %), taxanes (15 %), anthracyclines (24 %), or other cytotoxic agent (9 %) or endocrine therapy (4 %). The primary endpoint was achieved, with significantly improved median OS in the eribulin group (13.1 vs. 10.7 months; HR 0.81; 95 % CI, 0.66, 0.99, P = 0.041) [13••]. For patients with measurable disease, overall response by independent review was also significantly higher for eribulin (12 % vs. 5 %, P = 0.005), although median PFS was not significantly improved (3.7 vs. 2.2 months; HR 0.87; 95 % CI, 0.71, 1.05; P = 0.14). Sensitivity analysis for predefined exploratory subgroups revealed consistent results for improved OS favoring eribulin by disease subtype (estrogen and/or progesterone receptor positive, HER2-positive, and triple-negative), number of organs involved, sites of disease, and previous capecitabine. Overall frequencies of adverse events and serious adverse events were similar in the two groups. In the eribulin group, neutropenia was the most frequently reported grade 3 or 4 adverse event (45 %), but febrile neutropenia occurred in only 5 %, and hematologic toxicity resulted in discontinuation for fewer than 1 %. Peripheral neuropathy was the most common adverse event leading to discontinuation from eribulin (5 %). For those who developed grade 3 or 4 sensory neuropathy but continued treatment because of clinical benefit, it improved to grade 2 or better in later cycles after delays and dose reductions. A recently completed phase III trial comparing eribulin with capecitabine failed to show prolongation of median PFS or OS, the primary trial endpoints [39].
Gemcitabine
Gemcitabine is a pyrimidine nucleoside analogue that inhibits DNA polymerization and RNA synthesis [40]. There has been only one phase III trial evaluating gemcitabine for patients with anthracycline and taxane-pretreated disease (Table 2). The study included 252 women with locally recurrent or MBC pretreated with anthracyclines and taxanes; they were randomly assigned to vinorelbine (30 mg m−2 IV on days 1 and 8 every 3 weeks) alone or in combination with gemcitabine (1200 mg m−2 IV on days 1 and 8 every 3 weeks) [41]. Median PFS was significantly better for the combination (6.0 vs. 4.0 months; HR 0.66; 95 % CI 0.50–0.88; P = 0.003). Response for the combination group was numerically higher (36 % vs. 26 %, P = 0.093), but no difference in OS was observed (15.9 vs. 16.4 months). There was more grade 3 or 4 neutropenia (61 % vs. 44 %) and febrile neutropenia (11 % vs. 6 %) for the combination group, but comparable non-hematologic toxicity.
Platinum Analogues Plus Gemcitabine
Cisplatin and carboplatin are platinum complexes that bind predominantly to the N-7 position of guanine and adenine and produce DNA interstrand cross links. Carboplatin has a similar mechanism of action, although a higher drug concentration and longer incubation time in vitro are required to produce a comparable effect. Both drugs undergo renal elimination. Compared with cisplatin, carboplatin causes less nausea and vomiting, nephrotoxicity, and neuropathy, but more thrombocytopenia and neutropenia [42]. Both drugs are effective for patients with MBC associated with germline BCRA mutations [43]. For unselected patients who mostly have sporadic breast cancer, the platinum agents are also active when used as first-line therapy, but are relatively ineffective when used as second-line therapy [44, 45]. Two randomized trials evaluating the poly(ADP ribose) polymerase (PARP) inhibitor iniparib provide some information about the efficacy of the carboplatin–gemcitabine combination for patients with anthracycline and taxane-pretreated metastatic triple-negative breast cancer (TNBC). The first was a randomized phase II trial including 116 patients receiving first or second-third line therapy which included carboplatin (AUC 2 IV) plus gemcitabine (1000 mg m−2 IV on days 1 and 8 every 3 weeks) alone or in combination with iniparib [46]. The iniparib group was associated with significantly higher response, median PFS, and overall survival, and thereby provided information about the effectiveness of the carboplatin–gemcitabine combination for this population. A confirmatory phase III trial failed to show a benefit of addition of iniparib to the same carboplatin–gemcitabine regimen for 519 patients with metastatic TNBC, most of whom were anthracycline and taxane-pretreated, and of whom 222 (43 %) received it as second or third-line therapy [47]. The trial failed to meet its co-primary endpoints of improving PFS (median 5.1 vs. 4.1 months) and OS (11.8 vs. 11.1 months); response was similar in the two groups (34 % vs. 30 %) (Table 2). In addition, although the primary mechanism of action of iniparib was initially thought be inhibition of PARP, it was subsequently found to be a relatively weak PARP inhibitor, and induced its antitumor effects by inducing cell cycle arrest in the G2-M phase, promoting double strand DNA damage, and potentiating cell cycle arrest induced by carboplatin and gemcitabine [47].
Irinotecan
Irinotecan and its active metabolite, SN-38, interact with cellular topoisomerase I–DNA complexes and has S-phase-specific cytotoxicity by preventing re-ligation of the DNA strand, resulting in double-strand DNA breakage and cell death [48]. A randomized phase II study of 103 patients with MBC who had progressive disease after one to three lines of chemotherapy compared irinotecan given IV in a three-weekly (240 mg m−2 IV every 3 weeks) or weekly (100 mg m−2 IV for 4 of 6 weeks) schedule. The weekly regimen was associated with more favorable response (23 % vs. 14 %) and median PFS (2.8 vs. 1.9 months) [49•]. Activity against MBC has been demonstrated for a polymer-containing formulation of SN-38 (etirinotecan pegol) which results in sustained SN-38 blood levels [50]. A phase III trial has been initiated comparing etirinotecan pegol (145 mg m−2 IV every 3 weeks) with physician’s choice of therapy for patients with MBC who have previously been treated with an anthracycline, taxane, and capecitabine (ClinicalTrials.Gov identifier NCT0149210).
Pegylated Liposomal Doxorubicin
Liposomes are closed vesicular structures, initially described in the 1960s, that are capable of enveloping water-soluble molecules and may serve as a vehicle for more specific delivery of cytotoxic agents to tumors, thus limiting exposure of normal tissues [51]. Current liposome preparations are divided into two broad classes on the basis of their recognition by the mononuclear phagocyte system (MPS). One class of liposome is readily recognized and phagocytised by the MPS, because of binding of plasma proteins to the liposome surface; this induces uptake by macrophages in the liver, spleen, lungs, and bone marrow, minimizing exposure of normal tissues and thus diminishing some acute and chronic toxicity [52, 53]. A second class of agents includes liposomes that are designed to avoid detection by the MPS system. One example is pegylated liposomal doxorubicin (PLD), which circulates in the plasma for a relatively long period compared with conventional doxorubicin and non-pegylated liposomal formulations [54]. The rationale for their development and use in breast cancer has been extensively reviewed [55].
Of three phase III trials evaluating PLD for MBC, two have included patients with anthracycline and/or taxane-pretreated disease (Table 2). The first study included 301 patients who had disease progression after a first or second-line taxane-containing regimen for metastatic disease. Patients were randomized to either PLD (50 mg m−2 every 4 weeks) or a comparator of physician’s choice—vinorelbine (30 mg m−2 weekly) for 85 % of patients and mitomycin C (10 mg m−2 day 1 and every 4 weeks) plus vinblastine (5 mg m−2 day 1, day 14, day 28, and day 42) every 6 to 8 weeks for the remainder [56]. FS (median 2.9 vs. 2.5 months) and OS (median 11.0 vs. 9.0 months) were similar for PLD and the comparator. The most frequently reported adverse events were nausea (23 % vs. 31 %), vomiting (17 % vs. 20 %), and fatigue (9 % vs. 20 %), and were similar among treatment groups. PLD-treated patients experienced more HFS (37 %; 18 % grade 3, 1 patient grade 4) and stomatitis (22 %; 5 % grades 3 or 4). Neuropathy (11 %), constipation (16 %), and neutropenia (14 %) were more common with vinorelbine. Alopecia was low in both the PLD and vinorelbine groups (3 % and 5 %).
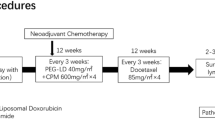
The second study compared docetaxel (75 mg m−2 IV every 3 weeks) alone or in combination with PLD (30 mg m−2 IV) for 751 patients with MBC who had relapsed at least one year after previous adjuvant doxorubicin-containing therapy [3•]. The combination group was associated with significantly improved median TTP (median 9.8 vs. 7.0 months; HR = 0.65; 95 % CI 0.55-0.77; P = 0.0001), which was the primary study endpoint. The combination was also associated with improved response (35 % vs. 26 %, P = 0.009) but similar OS. Importantly, there was no excess cardiac toxicity in the PLD group, providing proof of principle that PLD may be safety used after previous adjuvant anthracycline therapy. As in previous studies with PLD, the most common toxicity included HFS, stomatitis, and rash.
Conclusions
Anthracyclines and taxanes are effective cytotoxic agents that improve the potential for cure when used as adjuvant therapy, and prolong survival and palliate symptoms when used for the treatment of metastatic disease. Resistance invariably develops when used to treat metastatic disease, however, and contributes to recurrence in early stage disease. Several classes of cytotoxic agent produce response or disease stabilization in a modest proportion of patients who have progressive disease after previous anthracycline and taxane therapy, and have differing toxicity profiles. There are no predictive factors that are useful in guiding which agents to select for an individual patient. A systematic approach may be helpful in identifying which agents may be potentially used, and includes:
-
1.
reviewing the patients’ previous antineoplastic drug history;
-
2.
identifying comorbidity or residual toxicity from previous cytotoxic therapy that may limit the list of potentially suitable agents;
-
3.
identify agents for a history of resistance to the drug or class of agents;
-
4.
determine whether there is an indication for concurrent administration with biological therapy (e.g., HER2-positive disease) or combination cytotoxic therapy (e.g., rapidly progressive visceral disease); and
-
5.
if cytotoxic therapy alone is used, should it be used as a single agent, or in combination with other cytotoxic agents? Single cytotoxic agents should be suitable in most cases, although combination therapy may be considered for patients with rapidly progressive disease or high visceral tumor burden.
The choice of treatment regimen must be individualized on the basis of careful consideration of all of these factors.
References
Papers of particular interest have been highlighted as: • Of importance •• Of major importance
Sparano JA, Wang M, Martino S, et al. Weekly paclitaxel in the adjuvant treatment of breast cancer. The New England journal of medicine. 2008;358:1663–71.
Carrick S, Parker S, Thornton CE, Ghersi D, Simes J, Wilcken N. Single agent versus combination chemotherapy for metastatic breast cancer. Cochrane Database Syst Rev. 2009;CD003372
• Sparano JA, Makhson AN, Semiglazov VF. Pegylated liposomal doxorubicin plus docetaxel significantly improves time to progression without additive cardiotoxicity compared with docetaxel monotherapy in patients with advanced breast cancer previously treated with neoadjuvant-adjuvant anthracycline therapy: results from a randomized phase III study. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2009;27:4522–9. Demonstrated cardiac safety for pegylated liposomal doxorubicin after previous exposure to adjuvant anthracycline therapy.
Chan S, Friedrichs K, Noel D, et al. Prospective randomized trial of docetaxel versus doxorubicin in patients with metastatic breast cancer. J Clin Oncol. 1999;17:2341–54.
Sledge GW, Neuberg D, Bernardo P, et al. Phase III trial of doxorubicin, paclitaxel, and the combination of doxorubicin and paclitaxel as front-line chemotherapy for metastatic breast cancer: an intergroup trial (E1193). J Clin Oncol. 2003;21:588–92.
•• Slamon DJ, Leyland-Jones B, Shak S. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. The New England journal of medicine. 2001;344:783–92. Demonstrated that trastuzumab improves survival when added to chemotherapy as first-line therapy for HER2/neu overexpression metastatic breast cancer.
Kardinal CG, Perry MC, Weinberg V, Wood W, Ginsberg S, Raju RN. Chemoendocrine therapy vs chemotherapy alone for advanced breast cancer in postmenopausal women: preliminary report of a randomized study. Breast Cancer Res Treat. 1983;3:365–71.
Siegel R, DeSantis C, Virgo K, et al. Cancer treatment and survivorship statistics, 2012. CA Cancer J Clin. 2012;62:220–41.
Cardoso F, Di LA, Lohrisch C, Bernard C, Ferreira F, Piccart MJ. Second and subsequent lines of chemotherapy for metastatic breast cancer: what did we learn in the last two decades? Ann Oncol. 2002;13:197–207.
O'Shaughnessy J. Extending survival with chemotherapy in metastatic breast cancer. Oncologist. 2005;10 Suppl 3:20–9.
Greenberg PA, Hortobagyi GN, Smith TL, Ziegler LD, Frye DK, Buzdar AU. Long-term follow-up of patients with complete remission following combination chemotherapy for metastatic breast cancer. J Clin Oncol. 1996;14:2197–205.
Nabholtz JM, Senn HJ, Bezwoda WR, et al. Prospective randomized trial of docetaxel versus mitomycin plus vinblastine in patients with metastatic breast cancer progressing despite previous anthracycline-containing chemotherapy. 304 Study Group. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 1999;17:1413–24.
•• Cortes J, O'Shaughnessy J, Loesch D, et al. Eribulin monotherapy versus treatment of physician's choice in patients with metastatic breast cancer (EMBRACE): a phase 3 open-label randomised study. Lancet. 2011;377:914–23. Demonstrated that eribulin improved survival compared with physician's choice of another monotherapy regimen for patients with extensively pretreated metastatic breast cancer.
O'Shaughnessy J, Miles D, Vukelja S, et al. Superior survival with capecitabine plus docetaxel combination therapy in anthracycline-pretreated patients with advanced breast cancer: phase III trial results. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2002;20:2812–23.
Giordano SH, Buzdar AU, Smith TL, Kau SW, Yang Y, Hortobagyi GN. Is breast cancer survival improving? Cancer. 2004;100:44–52.
Chia SK, Speers CH, D'Yachkova Y, et al. The impact of new chemotherapeutic and hormone agents on survival in a population-based cohort of women with metastatic breast cancer. Cancer. 2007;110:973–9.
Dawood S, Broglio K, Gonzalez-Angulo AM, Buzdar AU, Hortobagyi GN, Giordano SH. Trends in survival over the past two decades among white and black patients with newly diagnosed stage IV breast cancer. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2008;26:4891–8.
Tevaarwerk AJ, Gray RJ, Schneider BP, et al. Survival in patients with metastatic recurrent breast cancer after adjuvant chemotherapy: Little evidence of improvement over the past 30 years. Cancer 2012
Thomas ES, Gomez HL, Li RK, et al. Ixabepilone plus capecitabine for metastatic breast cancer progressing after anthracycline and taxane treatment. J Clin Oncol. 2007;25:5210–7.
•• Sparano JA, Vrdoljak E, Rixe O, et al. Randomized phase III trial of ixabepilone plus capecitabine versus capecitabine in patients with metastatic breast cancer previously treated with an anthracycline and a taxane. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2010;28:3256–63. Phase III trial which showed that the ixabepilone–capecitabine combination improved response and progression-free survival compared with capecitabine alone for anthracycline and taxane-pretreated breast cancer; the combination did not improve survival.
• Pivot X, Asmar L, Buzdar AU, Valero V, Hortobagyi G. A unified definition of clinical anthracycline resistance breast cancer. Br J Cancer. 2000;82:529–34. Proposed definitions for anthracycine and taxane pretreatment versus resistance.
Castiglione-Gertsch M, Tattersall M, Hacking A, et al. Retreating recurrent breast cancer with the same CMF-containing regimen used as adjuvant therapy. The international breast cancer study group. Eur J Cancer. 1997;33:2321–5.
Guo X, Loibl S, Untch M, et al. Re-Challenging Taxanes in Recurrent Breast Cancer in Patients Treated with (Neo-)Adjuvant Taxane-Based Therapy. Breast Care (Basel). 2011;6:279–83.
Longley DB, Johnston PG. Molecular mechanisms of drug resistance. The Journal of pathology. 2005;205:275–92.
Fojo T, Coley HM. The role of efflux pumps in drug-resistant metastatic breast cancer: new insights and treatment strategies. Clin Breast Cancer. 2007;7:749–56.
Geyer CE, Forster J, Lindquist D, et al. Lapatinib plus capecitabine for HER2-positive advanced breast cancer. N Engl J Med. 2006;355:2733–43.
•• Blum JL, Dieras V, Lo Russo PM, et al. Multicenter, Phase II study of capecitabine in taxane-pretreated metastatic breast carcinoma patients. Cancer. 2001;92:1759–68. Demonstrated efficacy of capecitabine monotherapy for anthracycline and taxane-pretreated metastatic breast cancer.
Bajetta E, Procopio G, Celio L, et al. Safety and efficacy of two different doses of capecitabine in the treatment of advanced breast cancer in older women. J Clin Oncol. 2005;23:2155–61.
Traina TA, Theodoulou M, Feigin K, et al. Phase I study of a novel capecitabine schedule based on the Norton–Simon mathematical model in patients with metastatic breast cancer. J Clin Oncol. 2008;26:1797–802.
Miller KD, Chap LI, Holmes FA, et al. Randomized phase III trial of capecitabine compared with bevacizumab plus capecitabine in patients with previously treated metastatic breast cancer. J Clin Oncol. 2005;23:792–9.
Lee FY, Borzilleri R, Fairchild CR, et al. BMS-247550: a novel epothilone analog with a mode of action similar to paclitaxel but possessing superior antitumor efficacy. Clin Cancer Res. 2001;7:1429–37.
Goodin S, Kane MP, Rubin EH. Epothilones: mechanism of action and biologic activity. J Clin Oncol. 2004;22:2015–25.
Perez EA, Lerzo G, Pivot X, et al. Efficacy and Safety of Ixabepilone (BMS-247550) in a Phase II Study of Patients With Advanced Breast Cancer Resistant to an Anthracycline, a Taxane, and Capecitabine. J Clin Oncol. 2007;25:3407–14.
• Roche H, Conte P, Perez EA, et al. Ixabepilone plus capecitabine in metastatic breast cancer patients with reduced performance status previously treated with anthracyclines and taxanes: A pooled analysis by performance status of efficacy and safety data from 2 phase III studies. Breast cancer research and treatment. 2011;125:755–65. Pooled analysis of 2 phase III trials indicating a survival benefit of the ixabepilone–capecitabine combination compared with capecitabine alone for patients with a Karnofsky performance status of 70–80, but not 90–100.
Towle MJ, Salvato KA, Wels BF, et al. Eribulin induces irreversible mitotic blockade: Implications of cell-based pharmacodynamics for in vivo efficacy under intermittent dosing conditions. Cancer Res. 2011;71:496–505.
Vahdat LT, Pruitt B, Fabian CJ, et al. Phase II study of eribulin mesylate, a halichondrin B analog, in patients with metastatic breast cancer previously treated with an anthracycline and a taxane. J Clin Oncol. 2009;27:2954–61.
Cortes J, Vahdat L, Blum JL, et al. Phase II study of the halichondrin B analog eribulin mesylate in patients with locally advanced or metastatic breast cancer previously treated with an anthracycline, a taxane, and capecitabine. J Clin Oncol. 2010;28:3922–8.
Aogi K, Iwata H, Masuda N, et al. A phase II study of eribulin in Japanese patients with heavily pretreated metastatic breast cancer. Ann Oncol. 2012;23:1441–8.
Eribulin301. http://www.eisai.com/news/enews201244pdf.pdf. 2012
Plunkett W, Huang P, Xu YZ, Heinemann V, Grunewald R, Gandhi V. Gemcitabine: Metabolism, mechanisms of action, and self-potentiation. Semin Oncol. 1995;22:3–10.
Martin M, Ruiz A, Munoz M, et al. Gemcitabine plus vinorelbine versus vinorelbine monotherapy in patients with metastatic breast cancer previously treated with anthracyclines and taxanes: final results of the phase III Spanish Breast Cancer Research Group (GEICAM) trial. Lancet Oncol. 2007;8:219–25.
Go RS, Adjei AA. Review of the comparative pharmacology and clinical activity of cisplatin and carboplatin. J Clin Oncol. 1999;17:409–22.
Narod SA. BRCA mutations in the management of breast cancer: The state of the art. Nat Rev Clin Oncol. 2010;7:702–7.
Decatris MP, Sundar S, O'Byrne KJ. Platinum-based chemotherapy in metastatic breast cancer: Current status. Cancer Treat Rev. 2004;30:53–81.
Carrick S, Ghersi D, Wilcken N, Simes J. Platinum containing regimens for metastatic breast cancer. Cochrane Database Syst Rev. 2004;CD003374
O'Shaughnessy J, Osborne C, Pippen JE, et al. Iniparib plus chemotherapy in metastatic triple-negative breast cancer. N Engl J Med. 2011;364:205–14.
Ledford H. Drug candidates derailed in case of mistaken identity. Nature. 2012;483:519.
Liu LF, Desai SD, Li TK, Mao Y, Sun M, Sim SP. Mechanism of action of camptothecin. Ann N Y Acad Sci. 2000;922:1–10.
• Perez EA, Hillman DW, Mailliard JA, et al. Randomized phase II study of two irinotecan schedules for patients with metastatic breast cancer refractory to an anthracycline, a taxane, or both. J Clin Oncol. 2004;22:2849–55. Demonstrated efficacy of irinotecan for patients with extensively pretreated metastatic breast cancer.
Gale S, Croasdell G. 28th Annual JPMorgan Healthcare Conference—Exelixis and Nektar Therapeutics. IDrugs. 2010;13:139–41.
Bangham AD, Horne RW. Negative Staining of Phospholipids and Their Structural Modification by Surface-Active Agents as Observed in the Electron Microscope. J Mol Biol. 1964;8:660–8.
Kanter PM, Bullard GA, Pilkiewicz FG, Mayer LD, Cullis PR, Pavelic ZP. Preclinical toxicology study of liposome encapsulated doxorubicin (TLC D-99): comparison with doxorubicin and empty liposomes in mice and dogs. In Vivo. 1993;7:85–95.
Kanter PM, Bullard GA, Ginsberg RA, et al. Comparison of the cardiotoxic effects of liposomal doxorubicin (TLC D-99) versus free doxorubicin in beagle dogs. In Vivo. 1993;7:17–26.
Gabizon A, Shmeeda H, Barenholz Y. Pharmacokinetics of pegylated liposomal Doxorubicin: review of animal and human studies. Clin Pharmacokinet. 2003;42:419–36.
Robert NJ, Vogel CL, Henderson IC, et al. The role of the liposomal anthracyclines and other systemic therapies in the management of advanced breast cancer. Semin Oncol. 2004;31:106–46.
Keller AM, Mennel RG, Georgoulias VA, et al. Randomized phase III trial of pegylated liposomal doxorubicin versus vinorelbine or mitomycin C plus vinblastine in women with taxane-refractory advanced breast cancer. J Clin Oncol. 2004;22:3893–901.
Disclosures
E. Andreopoulou: none; J.A. Sparano: consultant to Johnson and Johnson and Eisai; member of a speakers bureau for Bristol-Myers Squibb; and member of the data monitoring committee for Genenetech/Roche.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Andreopoulou, E., Sparano, J.A. Chemotherapy in Patients with Anthracycline and Taxane-Pretreated Metastatic Breast Cancer: An Overview. Curr Breast Cancer Rep 5, 42–50 (2013). https://doi.org/10.1007/s12609-012-0097-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12609-012-0097-1