
Abstract
Objectives
To examine the risk of disability in 15 individual ADL, IADL, and mobility in older adults by age; and to assess the association of multimorbidity, gender, and education with disability.
Design & Setting
A prospective cohort study. The sample included 805 community-dwelling older people aged 60+ living in the Netherlands.
Measurements
Disability was assessed using the Katz-15 Index of Independence in Basic Activities of Daily Living (ADL), Instrumental Activities of Daily Living (IADL) and one mobility item. Disability in any of these activities was defined as the inability to perform the activity without assistance. The risk of disability by age for each individual ADL, IADL, and for mobility was assessed using Generalized mixed models.
Results
Disability in activities as household tasks, traveling, shopping, and continence had the highest risk and increased rapidly with age. The risk traveling disability among people aged 65 with two comorbidities increase from 9% to 37% at age 85. Disability in using the telephone, managing medications, finances, transferring, and toileting, had a very low risk and hardly increased with age. Compared to those without chronic conditions, those with ≥ 3 chronic conditions had a 3 to 5 times higher risk of developing disability. Males had a higher risk of disability in managing medication (P=0.005), and preparing meals (P=0.019), whereas females had a higher risk of disability with traveling (P=0.001). No association between education and disability on the individual ADL, IADL, and mobility was observed.
Conclusions
Older adults were mostly disabled in physical related activities, whereas disability in more cognitive related activities was less often experienced. The impact of multimorbidity on disability in each activity was substantial, while education was not.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
For many older people maintaining independence as long as possible is the paramount goal. The ability to perform activities of daily living (ADL), such as bathing or dressing, instrumental activities of daily living (IADL), like shopping and managing finances and mobility – the ability to walk without assistance- are essential to remain independent (1, 2). Each year 10% of the previously not disabled older persons develops disability, i.e. the need for assistance in ADL, and even a higher percentage develops disabilities in IADL (3). Moreover, over 30% of people aged 65 and over lost mobility within a four-year time window (4). Progressive disability seriously affects older peoples’ quality of life, and is associated with institutionalization, increased health care costs and mortality (1, 2, 5-7).
Previous studies have shown that with increasing age more people suffer from ADL and IADL disability (8-11). Older adults with comorbidities, females, and older adults with a low socio-economic status or education are considered to be at higher risk for developing disability (12-15). However, these studies defined disability as the inability to perform any of the ADL or IADL. Very few assessed the development of disability on the individual ADL and IADL activity separately. It is therefore unclear what the risk of disability is on the individual ADL, IADL and mobility activities, and what the impact is of risk factors on these individual activities. Understanding the development of disability on the individual ADL, IADL and mobility is important for health care professionals in order to develop and apply targeted interventions (2). Moreover, this information facilitate the design of successful interventions to preserve daily functioning and independently living among older adults. To the best of our knowledge, no study investigated the risk of disability in six ADL, seven IADL and one mobility item separately in the same population aged 60 years and older.
Therefore, the objective of this study was to examine the risk of disability on 15 individual ADL, IADL, and mobility activities among community-dwelling older adults by age; and to assess the association of chronic conditions, gender and education on disability on the individual activities.
Methods
Participants
A prospective observational study with one-year follow-up using the data of the Utrecht Proactive Frailty Intervention Trial (U-PROFIT). The U-PROFIT trial is a single blind three-armed cluster randomized controlled trial that was conducted in the Netherlands between 2010-2012 (16). This trial evaluated the (cost) effectiveness of a proactive personalized primary care program to preserve daily functioning in older people (n=3092). Details and the results have been described elsewhere (16, 17). Briefly, the first arm consisted of a screening and monitoring intervention based on routine primary care data to identify patients at risk. General practices in this arm we asked to use this instrument and to provide care based on current guidelines. General practices in the second arm received this instrument combined with a nurse-led care program. Registered practices nurses were extensively trained and delivered this evidence-based care program, conducted a comprehensive geriatric assessment at home, developed a care plan in close collaboration with the GP and other health care professionals (17). General practices in the third arm provided care as usual.
In the current study, data was used of participants enrolled in the control group (N=805).
Participants were recruited from 35 general practices located in and around Utrecht, the fourth city in the Netherlands, with over 300.000 citizens. The electronic medical record (EMR data) from the general practitioner (GP) was screened for eligible participants, who had to be aged 60 years and over, and at least one of the following criteria: (1) a frailty index score using the accumulated deficit approach18 with a cut-off of >0.20 19; (2) polypharmacy, defined as five or more different medications in chronic use ; (3) a consultation gap, defined as not having consulted the GP in the past three years, except for the yearly influenza vaccination. The frailty index was constructed according to the Rockwood-approach18 and consisted of a list of 50 items of International Classification of Primary Care (ICPC) and anatomic therapeutic chemical (ATC) codes (18, 19). Exclusion criteria were living in a nursing home or assisted living facility, and terminal illness. Eligible older adults were invited and participated after written informed consent. Data were collected using questionnaires at baseline, six and twelve months after inclusion.
Measures
Outcome - Assessment of disability
Disability was assessed using a modified version of the Katz-15 Index of Independence that measures Basic Activities of Daily Living (ADL), Instrumental Activities of Daily Living (IADL) and mobility (20). This self-reported questionnaire consists of six ADL items equal to the Katz-6 index (21) (i.e. bathing, dressing, eating, toileting, continence, transferring), eight IADL items (i.e. traveling, grooming, preparing a meal, use of telephone, shopping, household tasks, managing medications, and managing finances), and a question on mobility. Participants were asked whether they needed help with performing ADL, IADL or mobility. Each item was scored as zero (no disability) or one (yes, disabled), and summed, leading to a range of 0-15 for the Katz score, with a higher score indicating higher level of dependency. The need for help in any of these 15 activities generally indicates that the person will need assistance from a family member, caregiver or long-term care services (22, 23). In this study, the risk of disability in these 15) individual ADL/IADL and mobility was examined. The modified Katz-15 is demonstrated to be a reliable and valid instrument for the prediction of unfavorable health outcomes in community-dwelling older people (24).
Demographics and other measures
Demographic data such as age, gender, marital status, living situation (e.g. alone or with others), highest completed education (low-average-high), and socioeconomic status (SES) were collected using self-reported questionnaires. Low education was defined as: primary school or less; average education was defined as: secondary school, and high education was defined as: more than secondary school. SES was determined using the Netherlands Institute for Social Research-status scores that are based on the social status of postcode areas. Chronic conditions such as diabetes, heart failure, lung diseases, cancer, stroke, joint damage (osteoarthritis), osteoporosis, and cognitive function were collected at baseline, and the number of self-reported chronic conditions was calculated for each individual. Cognitive functioning was measured with one self-reported question: “Do you experience memory problems”.
Statistical analysis
The characteristics of the participants were summarized using frequency and percentages for categorical and means (SD) for continuous variables. Age was calculated at baseline, at 6 months follow-up (i.e. age at baseline plus a half year), and at 12-months follow-up (i.e. age at baseline plus one year). Thus, each participant contributed up to 3 measurements in one year follow-up: at baseline, 6 months, and 12 months. This allows to incorporate the individual progression of disability in each ADL, IADL and mobility over a one-year life-span, and also, as patients age varied at baseline, over the entire range of available ages. For each participant, risk of disability (mean Katz-15 score) in the individual ADL, IADL, and walking was calculated by age.
Mixed linear regression models (for the Katz-15 score) and mixed logistic regression models (for the individual Katz-items) were fitted on the age-scale, corrected for multiple measurements and clustering within primary care practices. Details of the statistical models are described in a supplementary file (S1). First, models were fitted to estimate the unadjusted and adjusted mean Katz-15 score and the risk of disability in each ADL, IADL, and mobility activity by age. We adjusted for determinants reported to be associated with disability such as gender, education, and the number of chronic conditions. The risk for each activity by age was calculated and reported with 95% confidence intervals (CI).
Second, we determined the association of multimorbidity (0, 1 or 2, or ≥3 chronic conditions), gender, and education (low- average- high) on each ADL, IADL and mobility activity. Unadjusted and adjusted Odds Ratios (OR) were calculated to assess the strength of the association. Similar adjustments were applied as descripted above. Next, for each ADL, IADL, and mobility activity, the interaction with chronic conditions, gender, and education with age was tested to determine whether the association of these factors differed according to age. All analyses were performed using SAS version 9.2 (SAS Institute, Inc., Cary, NC), and IBM SPSS version 21 (IBM).

Baseline Characteristics Participants (N=805)
Results
The mean age of the participants was 75 years (SD 8.8), 56.3% (453 out of 805) were female, and the average number of chronic conditions was 2 (SD 1.4) (Table 1). The mean Katz-15 score at baseline was 1.74 (SD: 2.4). At inclusion, 373 participants (46.3%) were free of disability in all ADL and IADL, 219 (27.2%) had one or two disabilities, 105 (13%) had three or four disabilities, and 108 (13.4%) experienced four or more disabilities (Table 1). At baseline, 110 out of 805 (13.7%) needed help with walking around.

Risk of ADL, IADL, and walking disability by age (60 – 85 years) adjusted for gender, education and number of chronic conditions
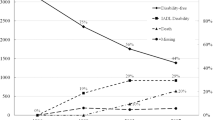
The mean Katz-15 score of participants between 60 and 80 years was around two, and increases more rapidly after age 80 (Appendix Figure 1). Figure 1 presents the risk of disability for each individual ADL, IADL, and mobility by age, adjusted for chronic conditions, gender, and education. Disability in activities with household tasks, traveling, shopping, and continence had the highest risk; disability in these activities increased rapidly with increasing age (Figure 1; Table 2). Disability in activities with eating, toileting using the telephone, managing medication, and managing finances showed the lowest risk, and hardly progressed with increasing age. The risk of disability in ADL, IADL, and walking was approximately 3 to 5 times higher for those with 3 or more chronic conditions compared to those without chronic conditions (Table 2). For example, the risk of traveling disability for 75-year olds without chronic conditions was 9.2% [95%CI 5.5-15.2], and 42.8% [95%CI: 36.7-49.1] for 75 year olds with three or more chronic conditions. For urinary incontinence, the risk was almost 10 times higher for those with three or more chronic conditions compared to those without chronic conditions (2.1% [95%CI: 1.3-3.5] and 18.9% [95%CI 13.8-25.2]) (Table 2).

Risk of ADL, IADL and mobility disability by age, stratified by the number of chronic conditions
Older adults with three or more chronic conditions, females, and those with a low education perceived greater levels of dependence compared to their counterparts (Table 3). A significant interaction between age and number of chronic conditions was observed for disability in walking (p=<0.001). The risk for 75 year old increased from 2.5% [95%CI1.3-4.7] to 19.6% [95% CI: 12.2-30.6] (Table 4). Significant interactions between age and gender on disabilities with traveling (P= 0.001), managing medications (P=0.005), and preparing meals (P=0.019) were observed. The risk of disability in managing medications was greater for men with advancing age, while for women, the risk was low and relatively flat across age groups (Table 5). No significant interaction between age and education on disability in the individual ADL, IADL, or mobility disability was observed.
Discussion
Older adults were mostly disabled in physical related activities such as household, traveling, shopping, and continence, and the risk of disability in these activities rapidly increases with age. Disability in more cognitive related activities such as using the telephone, managing medications, and managing finances, and activities such as toileting and transferring were less often experienced, and the risk of disability in these activities hardly increased with age in this population. Older adults with multimorbidity had a substantial higher risk of developing disability in all individual ADL, IADL, and mobility activities compared to those without chronic conditions. For example, a 75-year-old person with three or more chronic conditions in our study, the odds ratio for disability with traveling, e.g. an important factor to maintain independence was 7.2 higher compared to those without chronic conditions. Compared with females, males had a higher risk of developing disability with managing medications and preparing a meal whereas females had a higher risk for developing disability with traveling. No significant association between education and disability on the individual ADL, IADL, and mobility was observed.
Maintaining independence is one of the most important goals of the majority of older people (25). The onset of disability in activities of daily living is one of the greatest threats to the ability of older people to live independently (26, 27). Previous studies showed that IADL precedes ADL disability.15,28 IADL are considered as more complex activities compared to ADL since it requires cognitive functioning i.e. planning, organizing, and making decisions, as well as physical functioning (15, 28, 29). Our results demonstrate a more subtle distinction: IADL that require adequate physical functioning such as traveling, decline earlier than ADL, whereas disability in cognitiverelated IADL, such as using the telephone, managing medications and finances, developed later than disability in ADL such as bathing, dressing, and transferring.
Several studies showed an independent association between education and disability in older adults, suggesting that low education may be regarded as a risk factor for accelerating decline (12, 30). In contrast, we observed no significant interaction between age and education on disability in the individual ADL, IADL, and mobility. One possible explanation might be that previous studies investigated the association between education and multiple ADL or IADL activities, whereas in the current study the association on the individual activities was examined. Longitudinal studies are needed to determine how education influences the progression of disability in specific subgroups of older people on the individual activities. Although some studies examined the relationship between chronic conditions and disability, (31, 32) this is the first study that assessed the association between the number of chronic conditions on disability in 15 individual ADL, IADL and mobility activities. We observed some differences between males and females on managing medications, traveling and preparing meals. Females had a higher risk for developing disability with preparing meal that might my attributable to the fact that older males do not experience difficulty because they rarely perform this activity. Gender differences in disability have been confirmed in previous studies (33). Females do not only live longer than males, they also experience greater disability, and suffer from a greater burden than males (33) that should be taken into account when designing interventions.

Association between gender, education, chronic diseases, and disability, Odds Ratios (OR 95%CI)
The current study has important implications for patients, clinical practice and policy. Due the rapidly increasing aging population, early detection and prevention or preservation of daily functioning should be the highest priority both for physicians, as well as for society in order to meet the needs of older adults. The results of the current study shows that a one-size-fits-all approach for preventive interventions focusing on disability (ADL, IADL and mobility together) is clearly not successful because the risk of disability on the individual ADL, IADL and mobility varies among older adults. For example, a 75-year old female who report disability on four cognitive-related items on the Katz-15 index, may suffer from disability in different activities compared to another 75-year old female who had a similar Katz-15 score, but was disabled on four physical-related activities. Despite the similar Katz score, both females have different health needs that require different type of interventions in clinical practice. Moreover, this example shows the benefit of understanding the development of disability in the individual activities; reporting whether someone is disabled or not may therefore not always sufficient. The last decade, various intervention programs have been developed aimed to prevent (the onset of) disability among community-dwelling older adults however, they have shown inconsistent results (34, 35). Furthermore, trajectories of disability in older adults have been examined showing that certain subgroups develop unfavorable trajectories (8, 33). The results of the current study provides, combined with previous evidence, valuable starting point towards the design and evaluation of tailored interventions. Evidence-based tools need to be developed to help physicians, nurses and other health care professionals adequately identify those at high risk of disability. Moreover, effective interventions are urgently needed to prevent or delay the onset of disability in older adults in, especially for those with multimorbidity.

Risk of walking disability stratified by age and the number of chronic conditions
Some limitations need to be considered when interpreting the results. First, this study used data of participants enrolled in the control group of the U-PROFIT trial. Although the number of exclusion criteria of the trial were very few, i.e. only older adults living in a nursing home and those who were terminally ill were excluded, the included population of older adults may not be fully representative to all community-dwelling older adults that may have resulted in an underestimation of the observed probabilities. Second, self-reported bias might have played a role for some items such as managing medications. The low risk might be an underestimate since many older adults in the Netherlands receive their medication in little prepared bags per dose from their pharmacist, and older adults are then able to manage their own medication. However, a large sample of community-dwelling older people was included and clearly shows that with increasing age the majority of the population developed functional decline. Finally, chronic conditions were based on self-report. This may have contributed in underestimated results. A major strength of this study is that the risk of disability was assessed on a large number of activities: six ADL, eight IADL, and one mobility item. We were therefore able to capture a broad range of functioning compared to other studies. We examined for 15 individual activities the association between multimorbidity, gender and education, stratified by age which is, to our knowledge unique. The results clearly shows at which age disability in certain activities develop and confirms that most community-dwelling older adults develop ADL and IADL dependency (27, 36). We examined the development of disability on each individual ADL, IADL, and mobility by age, allowing us to use the follow-up data of each participant instead of using cross sectional data only.

Risk of managing medications, preparing a meal and traveling, stratified by gender and age
In conclusion, in community-dwelling older adults aged 60 years and over, the risk of disability in activities of household tasks, traveling, and shopping showed was high, and increased rapidly with age, whereas the risk of disability in using the telephone, managing medications and finances was very low, and hardly increased with age. The association of multimorbidity on all ADL, IADL disability was substantial. Differences in ADL, IADL, and mobility disability were observed for gender, but not education. These results indicate that preventive interventions should focus on the heterogeneous group of older adults, particularly those with multimorbidity.
Conflict of Interest: The authors declare no conflict of interest.
Author Contributions: NB contributed to the data analysis plan, undertook the data analysis and interpretation. NZ was involved in the data analysis and interpretation. NW and MJ collaborated in formulating the aims and interpretation of the data. AS was involved in the interpretation of the data and writing the manuscript. All authors read the final draft of the manuscript and approve its submission for publication.
Sponsor’s Role: This study was funded by a grant from The Netherlands Organization for Health Research and Development (reference 311040201) as part of the National Care for the Elderly Program. The sponsor had no role in the design, methods, recruitment, data collections, analysis and preparation of manuscript.
Funding: Data was used of the Utrecht Proactive Frailty Intervention Trial (U-PROFIT) and was supported by a grant from The Netherlands Organization for Health Research and Development (reference 311040201) as part of the National Care for the Elderly Program.
Ethical standard: Informed consent was obtained from all participants.

Adjusted mean Katz-15, adjusted for sex, education and number of chronic conditions
References
Covinsky KE, Palmer RM, Fortinsky RH, et al. Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: Increased vulnerability with age. J Am Geriatr Soc. 2003;51(4):451–458.
Fried LP, Guralnik JM. Disability in older adults: Evidence regarding significance, etiology, and risk. J Am Geriatr Soc. 1997;45(1):92–100.
Gill TM, Hardy SE, Williams CS. Underestimation of disability in Community-Living older persons. J Am Geriatr Soc. 2002;50(9):1492–1497.
Guralnik JM, LaCroix AZ, Abbott RD, et al. Maintaining mobility in late life. I. demographic characteristics and chronic conditions. Am J Epidemiol. 1993;137(8):845–857.
Ferrucci L, Guralnik JM, Pahor M, Corti MC, Havlik RJ. Hospital diagnoses, medicare charges, and nursing home admissions in the year when older persons become severely disabled. JAMA. 1997;277(9):728–734.
Stineman MG, Xie D, Pan Q, Kurichi JE, Saliba D, Streim J. Activity of daily living staging, chronic health conditions, and perceived lack of home accessibility features for elderly people living in the community. J Am Geriatr Soc. 2011;59(3):454–462.
Kim K, Kim S, Kim K, Jang H, Kim C, Chin HJ. Low hemoglobin A1C increases the risk of disability in community-dwelling older non-diabetics adults. J Nutr Health Aging.:1–6.
Han L, Allore H, Murphy T, Gill T, Peduzzi P, Lin H. Dynamics of functional aging based on latent-class trajectories of activities of daily living. Ann Epidemiol. 2013;23(2):87–92.
Lin S, Beck AN, Finch BK, Hummer RA, Master RK. Trends in US older adult disability: Exploring age, period, and cohort effects. Am J Public Health. 2012;102(11):2157–2163.
Sjölund B, Wimo A, Qiu C, Engström M, von Strauss E. Time trends in prevalence of activities of daily living (ADL) disability and survival: Comparing two populations (aged 78 years) living in a rural area in sweden. Arch Gerontol Geriatr. 2014;58(3):370–375.
Avila-Funes JA, Medina-Campos RH, Tamez-Rivera O, Navarrete-Reyes AP, Amieva H, Aguilar-Navarro S. Frailty is associated with disability and recent hospitalization in community-dwelling elderly: The coyoacan cohort. J Frailty Aging. 2014;3(4):206–210. doi: 10.14283/jfa.2014.25 [doi].
Deeg DJ, Huisman M, Terwee CB, Comijs HC, Thomese GF, Visser M. Changes in functional ability with ageing and over time. In: Aging in european societies. Springer; 2013:117–132.
Gjonca E, Tabassum F, Breeze E. Socioeconomic differences in physical disability at older age. J Epidemiol Community Health. 2009;63(11):928–935. doi: 10.1136/ jech.2008.082776 [doi].
Hoogendijk EO, van der Horst, Henriëtte E, Deeg DJ, et al. The identification of frail older adults in primary care: Comparing the accuracy of five simple instruments. Age Ageing. 2013;42(2):262–265.
Millán-Calenti JC, Tubío J, Pita-Fernández S, et al. Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Arch Gerontol Geriatr. 2010;50(3):306–310.
Bleijenberg N, Drubbel I, ten Dam VH, Numans ME, Schuurmans MJ, de Wit NJ. Proactive and integrated primary care for frail older people: Design and methodological challenges of the utrecht primary care PROactive frailty intervention trial (U-PROFIT). BMC geriatrics. 2012;12(1):16.
Bleijenberg, N., Drubbel, I., Schuurmans, M. J., Dam, H. T., Zuithoff, N., Numans, M. E., & Wit, N. J. Effectiveness of a Proactive Primary Care Program on Preserving Daily Functioning of Older People: A Cluster Randomized Controlled Trial. Journal of the American Geriatrics Society, 2016;64(9), 1779–1788.
Rockwood K, Andrew M, Mitnitski A. A comparison of two approaches to measuring frailty in elderly people. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2007;62(7):738–743.
Drubbel I, de Wit NJ, Bleijenberg N, Eijkemans RJC, Schuurmans MJ, Numans ME. Prediction of adverse health outcomes in older people using a frailty index based on routine primary care data. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2012.
Weinberger M, Samsa GP, Schmader K, Greenberg SM, Carr DB, Wildman DS. Comparing proxy and patients’ perceptions of patients’ functional status: Results from an outpatient geriatric clinic. J Am Geriatr Soc. 1992;40(6):585–588.
Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. JAMA: the journal of the American Medical Association. 1963;185(12):914.
Verbrugge LM, Jette AM. The disablement process. Soc Sci Med. 1994;38(1):1–14.
Covinsky KE, Pierluissi E, Johnston CB. Hospitalization-associated disability:“She was probably able to ambulate, but i’m not sure”. JAMA. 2011;306(16):1782–1793.
Laan W, Bleijenberg N, Drubbel I, Numans ME, de Wit NJ, Schuurmans MJ. Factors associated with increasing functional decline in multimorbid independently living older people. Maturitas. 2013.
Beswick A, Gooberman-Hill R, Smith A, Wylde V, Ebrahim S. Maintaining independence in older people. Reviews in Clinical Gerontology. 2010;20(02):128–153.
Covinsky KE, Wu AW, Landefeld CS, et al. Health status versus quality of life in older patients: Does the distinction matter? Am J Med. 1999;106(4):435–440.
den Ouden ME, Schuurmans MJ, Mueller-Schotte S, van der Schouw Y. Identification of high-risk individuals for the development of disability in activities of daily living. A ten-year follow-up study. Exp Gerontol. 2013.
Judge JO, Schechtman K, Cress E, Group F. The relationship between physical performance measures and independence in instrumental activities of daily living. J Am Geriatr Soc. 1996;44(11):1332–1341.
Finlayson M, Mallinson T, Barbosa VM. Activities of daily living (ADL) and instrumental activities of daily living (IADL) items were stable over time in a longitudinal study on aging. J Clin Epidemiol. 2005;58(4):338–349.
Hoogendijk E, van Groenou MB, van Tilburg T, Deeg D. Educational differences in functional limitations: Comparisons of 55–65-year-olds in the netherlands in 1992 and 2002. International journal of public health. 2008;53(6):281–289.
Klijs B, Nusselder WJ, Looman CW, Mackenbach JP. Contribution of chronic disease to the burden of disability. PLoS One. 2011;6(9):e25325.
Hoeymans N, Wong A, van Gool CH, et al. The disabling effect of diseases: A study on trends in diseases, activity limitations, and their interrelationships. Am J Public Health. 2012;102(1):163–170.
Gill TM, Gahbauer EA, Lin H, Han L, Allore HG. Comparisons between older men and women in the trajectory and burden of disability over the course of nearly 14 years. Journal of the American Medical Directors Association. 2013;14(4):280–286.
Beswick AD, Rees K, Dieppe P, et al. Complex interventions to improve physical function and maintain independent living in elderly people: A systematic review and meta-analysis. The Lancet. 2008;371(9614):725–735.
Lin JS, Whitlock EP, Eckstrom E, et al. Challenges in synthesizing and interpreting the evidence from a systematic review of multifactorial interventions to prevent functional decline in older adults. J Am Geriatr Soc. 2012;60(11):2157–2166.
Smith AK, Walter LC, Miao Y, Boscardin WJ, Covinsky KE. Disability during the last two years of life. JAMA internal medicine. 2013;173(16):1506–1513.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bleijenberg, N., Zuithoff, N.P.A., Smith, A.K. et al. Disability in the individual ADL, IADL, and mobility among older adults: A prospective cohort study. J Nutr Health Aging 21, 897–903 (2017). https://doi.org/10.1007/s12603-017-0891-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12603-017-0891-6