
Abstract
Objective
We examined the associations of handgrip strength, upper arm circumference, and waist circumference with dementia among Singapore older adults.
Design
Cross-sectional epidemiological study.
Setting
Residential homes, day care centres, nursing homes and institutions.
Participants
2,565 men and women aged 60 years and above who participated in the Well-being of the Singapore Elderly (WiSE) study in 2013.
Measurements
Socio-demographic correlates, dietary habits, health behaviours, grip strength, upper arm circumference, and waist circumference were collected. Grip strength was measured using a hand dynamometer with the dominant hand. Upper arm circumference was measured using a measuring tape around the thickest part of the upper arm while waist circumference measured in centimetres was measured at the narrowest part of the body between the chest and hips for women, and measured at the level of the umbilicus for men. Dementia was diagnosed using the 10/66 dementia diagnostic criteria.
Results
Mean grip strength was 13.07 kg (SE=0.60) for people with dementia and 21.98 kg (SE=0.26) for people without dementia. After adjusting for all factors, grip strength remained significantly associated with dementia (p <0.0001). Upper arm circumference was associated with dementia (p <0.0001) but this association was only significant in the univariate analysis. Waist circumference was not significantly associated with dementia.
Conclusions
Lower grip strength was independently associated with dementia in the older adult population in Singapore. Further research needs to be done to ascertain whether this association exists for specific types of dementia and look into the relationship of other anthropometric measurements with dementia in Singapore.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Aging population is a concern and challenge for many countries in the world. Between 2000 and 2050, the world’s population of those aged 60 years and above will increase from 11% to 22% (1). Singapore is a country located in Southeast Asia with a multi-ethnic population (74.3% are Chinese, 13.3% are Malays, 9.1% are Indians, and 3.3% belong to Other ethnic groups) (2). It has one of the world’s fastest aging populations with an increasing median age of the resident population from 37.4 years in 2010 to 39.3 years in 2014. With the post-war baby boomers turning 65 years old from 2012 onwards, the oldage support ratio is expected to drop from 6.3 in 2011 to 2.1 by 2030 (3).
The advancement of medical technologies has led to an increase in life expectancy. Individuals are more likely to live longer and thus are vulnerable to neurodegenerative illnesses such as dementia (1). A recent meta-analysis suggested that in most regions of the world, the age-standardized prevalence of dementia falls within 5% to 7%. Latin America had the highest prevalence (8.5%) whereas sub-Saharan Africa regions had the lowest prevalence (2% to 4%). The prevalence of dementia in East Asia was 5% and South East Asia was 6.4% (4).
Cognitive decline and loss of memory are common symptoms of dementia. However, other studies have found that dementia is also associated with changes in body composition and muscular strength (5-7). Furthermore, Rogers (2008) suggested that cognitive status is related to strength and reduced strength in people with dementia is the key factor to functional disability.
To assess changes in body composition and muscular strength, anthropometric measurements are useful. Anthropometry concerns the measurement of physical traits of human body and it is an important tool in nutritional assessment and acts as a clinical indicator for elderly (9, 10). Handgrip strength as an anthropometric measurement has been used as a determinant of an individual’s hand motor abilities. It plays an essential role in daily activities and some studies have looked at grip strength as a proxy for motor functions among older people (11, 12). Reduced grip strength was correlated with physical functioning and disability (13-15), poor cognitive performance (16-18), and morbidity and mortality (19, 20). Literature on arm circumference and waist circumference has found that both measurements decreased with age (21, 22). Arm circumference is also associated with nutritional status and dementia. A cross-sectional survey found that elderly Africans with dementia were more likely to have a smaller arm circumference and suffered from under-nutrition than healthy people (23). Similarly, a study by Taylor (2012) across seven low and middle income countries found support for an inverse relationship between arm and waist circumference with dementia and its severity.
This study aimed to examine the association of grip strength, upper arm circumference, and waist circumference with dementia among Singapore older adults by comparing the differences of these anthropometric measurements between those with and without dementia. The study also investigated whether the association was affected by other factors such as body mass index and dietary habits. We hypothesized that lower grip strength, smaller upper arm circumference, and smaller waist circumference would be associated with dementia.
Methods
Study Population
A cross-sectional epidemiological survey was conducted with 2,565 participants who were randomly selected from a national database of Singapore residents aged 60 years and above. The database consisted of administrative data (i.e. name, ethnicity, gender, and address) of all citizens and permanent residents in Singapore, which was updated on a regular basis. Disproportionate stratified sampling design was used where residents in the older age group and those from Malay and Indian ethnic groups were over-sampled. Older adults who resided in day care centres, nursing homes, and institutions were included as well. Individuals who were not living in Singapore and who could not be contacted due to invalid addresses were excluded from the study. An informant of each participant- someone who knew the participant best, was also invited to take part in the survey. The study was approved by the relevant ethics committees -National Healthcare Group Domain Specific Review Board and the SingHealth Centralised Institutional Review Board, and written informed consent was obtained from the participants. In the case where participants were unable to provide consent, consent was taken from their legally acceptable representative or next-of-kin. A detailed description of the methodology can be found in an earlier paper (25).
Measurements and Assessments
Data collection was conducted through an extensive face-toface interview which lasted for two to three hours. Dementia was coded as a binary variable and diagnosis was made following the 10/66 diagnostic criteria where participants scoring above a cut-point of predicted probability of DSMIV diagnosis of dementia (26), were given the diagnosis. The predicted probability was derived from the logistic regression developed in the 10/66 international pilot study (25, 27).
The NEUROEX (28), a brief fully structured physical and neurological assessment with objectified measures of anthropometric measurements, was administered. Anthropometric measures were obtained by trained interviewers and among these measurements were grip strength, upper arm circumference, and waist circumference. Participant’s grip strength was measured in kilograms using a JAMAR® Plus+ Hydraulic hand dynamometer with the dominant hand and by taking the average of the two attempts measured. Upper arm circumference was measured in centimetres using a measuring tape around the thickest part of the upper arm while waist circumference measured in centimetres was measured at the narrowest part of the body between the chest and hips for women, and measured at the level of the umbilicus for men.
Information on socio-demographic characteristics, medical history, dietary habits, and health behaviours were collected. Socio-demographic information on age, gender, ethnicity, marital status, education, and employment status was collected from participants and verified with informants. Height and weight were measured, and body mass index (BMI) was calculated using the weight in kilograms divided by the height in metres squared (kg/m2). Medical history of hypertension, heart problems, stroke, diabetes, and transient ischemic attack (TIA) were recorded. Dietary habits were assessed based on frequency of meat and fish intake and the number of servings of fruit and vegetables consumed over the last three days from the date of interview. Health behaviours such as smoking, alcohol consumption, and physical activity were assessed. Smoking behaviour was coded as yes or no. For alcohol consumption, participants were asked regarding their maximum regular consumption in units per week. Finally, self-reported physical activity was coded as physically active for those who reported that they were “very physically active” and “fairly physically active”, and not physically active for those reporting “not very physically active” and “not at all physically active” (24). Previous studies have found that age, gender, ethnicity, body mass index, nutritional status, and physical activities were associated with the three anthropometric measurements and thus these variables were controlled for to account for any potential confounders (29-35).
Statistical Analysis
Data analysis was carried out using Statistical Analysis Software (SAS) system version (9.3). Mean and standard error were calculated for continuous variables, and frequencies and percentages were calculated for categorical variables. A univariate test using simple linear regression was conducted to compare the means of the three anthropometric measurements of older adults with dementia to those without dementia. To test for any independent associations between dementia and grip strength, upper arm circumference, and waist circumference, five series of multiple linear regression models were used to estimate modifying effects of socio-demographic variables, body mass index, medical history, dietary habits, and health behaviours. Multivariate analyses were run using linear regression models where dementia was treated as a main predictor and each anthropometric measurement as an outcome variable (24). First regression model was run separately for each of the anthropometric measurements adjusted for sociodemographic variables. The subsequent models were analysed by adding additional factors into each model. The final model was adjusted for socio-demographic variables; body mass index; medical history: hypertension, heart problems, stroke, diabetes, and TIAs; dietary habits: frequency of eating fish, meat, fruit, and vegetables; and health behaviours: smoking, alcohol, and exercise (Table 3, model 5). All statistical significant differences were set at p < 0.05.
Results
Characteristics of Study Participants
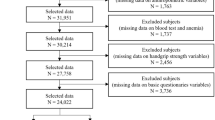
Of the 2,565 participants, 2,421 cases with completed informants’ interview which were required for the 10/66 dementia diagnosis algorithm were included in our sample. The response rate was 65.6%. Table 1 shows the majority were of aged 60-74 (58.0%), women (57.1%) and Chinese (38.5%). Most participants were married/ cohabiting (58.7%), had completed primary education (24.8%), and were retired (39.6%). The distributions of socio-demographic correlates (i.e. age, and ethnicity) were adjusted to match Singapore residents’ population for those aged 60 years and above (Table 1; weighted %).
Comparing Group Means
Table 2 shows the mean grip strength, mean upper arm circumference, and mean waist circumference by dementia diagnosis. 2,170 cases with all three measurements were included for the analysis. Missing data from each measurement were due to reasons such as the older adult being bedridden, suffering from stroke or paralysis. Some subjects also opted out as they were uncomfortable with the measurements. The estimated average grip strength for elderly with dementia was 13.07 kg and 21.98 kg for elderly without dementia. An association was found between grip strength and dementia. Participants with dementia had significantly lower grip strength (M= 13.07, SE= 0.60) compared to participants without dementia (M= 21.98, SE= 0.26; p <0.0001). The average upper arm circumference for elderly with dementia was 25.74 cm and 27.51 cm for elderly without dementia. A significant difference was also found for upper arm circumference where participants with dementia had smaller upper arm circumference (M= 25.74, SE= 0.34) than participants without dementia (M= 27.51, SE= 0.11; p <0.0001). The average waist circumference for elderly with dementia was 87.41 cm and 88.55 cm for elderly without dementia. For waist circumference, no significant differences were found between participants with dementia (M= 87.41, SE= 1.07) and those without dementia (M= 88.55, SE= 0.33, p >0.05).
Multivariate Analysis to Test the Independent Association of Anthropometric Measurements with Dementia
Table 3 shows the unadjusted and adjusted estimates representing difference in grip strength, upper arm circumference, and waist circumference. The multiple linear regreßsion models showed that after sequentially adjusting for socio-demographic variables, BMI, medical history, dietary habits, and health behaviours, the effect of grip strength remained significantly associated with dementia (β =-3.00, 95% CI, -4.67, -1.33, p <0.001). Unadjusted model showed a significant association between upper arm circumference and dementia (p <0.0001) however this association did not reach statistical significance after accounting for other variables (Table 3, model 1 to model 5).
Discussion
From our cross-sectional epidemiological study of older adults in Singapore, we found an association between lower grip strength and dementia. The association between grip strength and dementia remained significant after controlling for other factors such as age, gender, BMI, and dietary habits, which influence grip strength. However, our results are not consistent with other studies that found independent associations between upper arm circumference, and waist circumference with dementia (24, 36), although there were studies that did not find significant associations between waist circumference and risk of dementia (37, 38). An association was found between smaller upper arm circumference and dementia in our univariate analysis. However this association was better accounted for by socio-demographic variables, BMI, medical history, dietary habits, and health behaviours.
Our findings lend support to previous studies that found an association of lower grip strength with dementia. A study on twins in Sweden reported that poorer grip strength was one of the predictors for dementia (39). Furthermore, in a study on a Korean elderly population, older people in Korea with both low grip strength and BMI were more likely to be at risk for dementia (40). Although the findings in this Korean study showed that there was an interaction effect between BMI and grip strength, our study did not show such an effect. A separate analysis using BMI as an outcome variable and dementia as a main predictor showed no significant association between BMI and dementia after controlling for other factors.
Several underlying mechanisms have been proposed for this association between grip strength and dementia. Firstly, three neural pathways- integrated sensory, motor, and sensory systems are interconnected and thus any impairment in one neural pathway may alter the other neural systems (41). Progressive brain cells death in people with dementia would cause impairment to the cognitive system and eventually affect the motor system. Meta-analysis has shown that the primary motor cortex activity exhibits differently in AD patients than in healthy older adults (42). Motor impairments would affect a portion of AD patients at the initial stage of the disease and deteriorate along with cognitive impairment. This could therefore influence the grip strength of the older adults with dementia. Furthermore, a cross-sectional study suggested that the combination of age, gender, and cognitive status was related to grip strength in adults with AD or a related dementia (8). Yet in our results, after controlling for age and gender, the association between grip strength and dementia remained significant. Hence we hypothesize that cognitive status could be more related to the association instead.
Secondly, genetic variants could play a role in affecting the physical functions of people with dementia. Previous research has suggested that the AD risk genes such as presenilin 1 (PS1) and apolipoprotein E (APOE E4) are associated with motor syndromes (43). However, genetic factors were not assessed in the current study and thus future studies could look into this area of research.
Lastly, engaging in physical activity could affect grip strength. Horowitz et al (1997) found significant association between greater grip strength with weekly physical activity in older adults in United States. In model 5 of our multivariate analyses when physical activity variable was included (Table 3), the significance of the finding dropped slightly suggesting that engaging in physical activities might affect the association between grip strength and dementia.
The cross-sectional design of our study does not enable us to make conclusions on the temporal relationship between grip strength and dementia. In addition, this study only looked at dementia as the main predictor. Previous studies have indicated that the association between dementia subtypes with other anthropometric measurements (i.e. skull circumference and leg length) differs (44). Thus it is possible that upper arm circumference and waist circumference are associated with specific types of dementia instead of dementia in general. Lastly, there is also the possibility that the participants, particularly those with dementia, may not have understood the instructions for measuring grip strength and that could affect the validity of the measurements taken (40). To reduce the likelihood of such occurrence, all interviewers received standardized instructions and training from senior researchers to ensure proper use of the equipment and demonstrations of using the dynamometer were also conducted for all subjects.
Notwithstanding the limitations stated above, results from this study have important implications on the healthcare of the elderly. Our findings add to the growing literature that highlights the potential use of physical measurements such as grip strength as markers for cognitive functioning in elderly (45, 46). Home-based self-monitoring of grip strength using reliable instrument such as a grip-ball (47) could be promoted as a non-invasive efficient method to detect elderly who are at risk of having dementia. Furthermore, a number of studies showed that improving grip strength has various other benefits including reduction of risk of mortality and chronic diseases (48, 49). Lastly, given the strength of the association coupled with other studies that found the reliability of grip strength tests in non-severe dementia patients (50, 51), this anthropometric measurement has potential value as a measure in interventions for those with dementia.
In conclusion, lower grip strength was found to be independently associated with dementia in the older adult population in Singapore. This finding adds on to the existing literature that looks at anthropometric measurements and their associations with dementia and showed that dementia was associated with lower grip strength after controlling for other confounding variables. Important implications of our findings have been discussed in this paper and future studies could look into assessing these suggestions.
Funding Sources: The study was funded by the Ministry of Health of Singapore and the Singapore Millennium Foundation of the Temasek Trust.
Conflict of Interest: All authors report grants from Ministry of Health, Singapore, and Singapore Millennium Foundation, during the conduct of the study.
Ethical Standards: The authors declare that the study procedures comply with the current ethical standards for investigation involving human participants in Singapore.
References
World Health Organization [WHO]. Facts about ageing. 2014 30 September 2014 [cited 2015; Available from: http://www.who.int/ageing/about/facts/en/.
Statistics, S.D.o. Statistics Singapore Population Trends. 2015 02 Sept 2015]; Available from: http://www.singstat.gov.sg/docs/default-source/default-documentlibrary/publications/publications_and_papers/reference/monthly_digest/mdsjul15. pdf.
Singapore Department of Statistics. Population Trends 2014. 2014 September 2014 [cited 2015; Available from: http://www.singstat.gov.sg/docs/default-source/defaultdocument-library/publications/publications_and_papers/population_and_population_ structure/population2014.pdf.
Prince, M., R. Bryce, E. Albanese, A. Wimo, W. Ribeiro, and C.P. Ferri, The global prevalence of dementia: a systematic review and metaanalysis. Alzheimers Dement, 2013. 9(1): p. 63–75e2.
Buchman, A.S., R.S. Wilson, P.A. Boyle, J.L. Bienias, and D.A. Bennett, Grip strength and the risk of incident Alzheimer’s disease. Neuroepidemiology, 2007. 29(1-2): p. 66–73.
Camina Martín, M.A., B. de Mateo Silleras, L. Nescolarde Selva, S. Barrera Ortega, L. Domínguez Rodríguez, and M.P. Redondo Del Río, Bioimpedance vector analysis and conventional bioimpedance to assess body composition in older adults with dementia. Nutrition (Burbank, Los Angeles County, Calif.), 2015. 31(1): p. 155–159.
Thomas, V.S. and P.A. Hageman, Can neuromuscular strength and function in people with dementia be rehabilitated using resistance-exercise training? Results from a preliminary intervention study. The journals of gerontology.Series A, Biological sciences and medical sciences, 2003. 58(8): p. 746–M751.
Rogers, S.D. and S.E. Jarrot, Cognitive impairment and effects on upper body strength of adults with dementia. J Aging Phys Act, 2008. 16(1): p. 61–8.
Roriz, A.K., L.C. Passos, C.C. de Oliveira, M. Eickemberg, A. Moreira Pde, and L.R. Sampaio, Evaluation of the accuracy of anthropometric clinical indicators of visceral fat in adults and elderly. PLoS One, 2014. 9(7): p. e103499.
Hanisah, R., S. Shahar, and F.S. Lee, Validation of screening tools to assess appetite among geriatric patients. The journal of nutrition, health & aging, 2013. 16(7): p. 660–665.
Kerr, A., H.E. Syddall, C. Cooper, G.F. Turner, R.S. Briggs, and A.A. Sayer, Does admission grip strength predict length of stay in hospitalised older patients? Age and Ageing, 2006. 35(1): p. 82–84.
Sallinen, J., Hand-grip strength cut points to screen older persons at risk for mobility limitation. J Am Geriatr Soc, 2010. 58(9): p. 1721–1726.
Dong, H.-J., J. Marcusson, E. Wressle, and M. Unosson, Obese very old women have low relative handgrip strength, poor physical function, and difficulties in daily living. The journal of nutrition, health & aging, 2015. 19(1): p. 20–25.
Rantanen, T., J.M. Guralnik, and D. Foley, Midlife hand grip strength as a predictor of old age disability. JAMA [H.W.Wilson -GS], 1999. 281(6): p.558.
Ramlagan, S., K. Peltzer, and N. Phaswana-Mafuya, Hand grip strength and associated factors in non-institutionalised men and women 50 years and older in South Africa. BMC Research Notes, 2014. 7(1): p. 8-8.
Taekema, D.G., J. Gussekloo, A.B. Maier, R.G. Westendorp, and A.J. de Craen, Handgrip strength as a predictor of functional, psychological and social health. A prospective population-based study among the oldest old. Age Ageing, 2010. 39(3): p. 331–7.
Alfaro-Acha, A., S. Al Snih, M.A. Raji, Y.F. Kuo, K.S. Markides, and K.J. Ottenbacher, Handgrip strength and cognitive decline in older Mexican Americans. J Gerontol A Biol Sci Med Sci, 2006. 61(8): p. 859–65.
Taekema, D.G., et al., Temporal relationship between handgrip strength and cognitive performance in oldest old people. Age and Ageing, 2012. 41(4): p. 506–512.
Sultan, P., M.A. Hamilton, and G.L. Ackland, Preoperative muscle weakness as defined by handgrip strength and postoperative outcomes: a systematic review. BMC anesthesiology, 2012. 12(1): p. 1-1.
Metter, E.J., L.A. Talbot, M. Schrager, and R. Conwit, Skeletal muscle strength as a predictor of all-cause mortality in healthy men. The journals of gerontology.Series A, Biological sciences and medical sciences, 2002. 57(10): p. B359–B365.
Santos, J.L., et al., Anthropometric measurements in the elderly population of Santiago, Chile. Nutrition, 2004. 20(5): p. 452–457.
Coqueiro Rda, S., A.R. Barbosa, and A.F. Borgatto, Anthropometric measurements in the elderly of Havana, Cuba: age and sex differences. Nutrition, 2009. 25(1): p. 33–9.
De Rouvray, C., et al., The nutritional status of older people with and without dementia living in an urban setting in Central Africa: the EDAC study. J Nutr Health Aging, 2014. 18(10): p. 868–75.
Taylor, C.L., E. Albanese, and R. Stewart, The association of dementia with upper arm and waist circumference in seven low-and middle-income countries: the 10/66 cross-sectional surveys. J Gerontol A Biol Sci Med Sci, 2012. 67(8): p. 897–904.
Subramaniam, M., et al., Prevalence of Dementia in People Aged 60 Years and Above: Results from the WiSE Study. J Alzheimers Dis, 2015. 45(4): p. 1127–38.
American Psychiatric Association. Task Force on, D.-I. and A. American Psychiatric, Diagnostic and statistical manual of mental disorders: DSMIV. Vol. 4th. 1994, Washington, D.C U6 -ctx_ver=Z39.88-2004&ctx_enc=info%3Aofi%2Fenc%3AUTF-8&rfr_id=info:sid/summon.serialssolutions. com&rft_val_fmt=info:ofi/fmt:kev:mtx:book&rft.genre=book&rft. title=Diagnostic+and+statistical+manual+of+mental+disorders&rft.date=1994-01-01&rft.pub=American+Psychiatric+Association&rft.externalDocID=b18486010&par amdict=en-US U7 -Book: American Psychiatric Association.
Prince, M., D. Acosta, H. Chiu, M. Scazufca, M. Varghese, and G. Dementia Research, Dementia diagnosis in developing countries: a cross-cultural validation study. The Lancet, 2003. 361(9361): p. 909–917.
10/66 Dementia Research Group. Population–based epidemiological studies (prevalence phase): methods. 31 May 2015]; Available from: http://www.alz.co.uk/1066/pop_based_ep_studies_prevalence_phase_methods.php.
Norman, K., N. Stobaus, M.C. Gonzalez, J.D. Schulzke, and M. Pirlich, Hand grip strength: outcome predictor and marker of nutritional status. Clin Nutr, 2011. 30(2): p. 135–42.
Horowitz, B.P., R. Tollin, and G. Cassidy, Grip Strength. Physical & Occupational Therapy in Geriatrics, 1997. 15(1): p. 53–64.
MacInnis, R.J., et al., Predictors of increased body weight and waist circumference for middle-aged adults. Public Health Nutr, 2014. 17(5): p. 1087–97.
Ardebili, H.E., F.L. Boloki, A. Jazayeri, M. Ariaei, and M. Minaei, Nutritional status of elderly people. Journal of School of Public Health and Institute of Public Health Research, 2014. 12(2): p. 67–76.
Lim, W., P. Ong, and M. Lee, 2014, How Strong is Our Grip?: Comparison of Singapore Community Dwellers with Consolidated Norms. Paper presented at Singapore Health & Biomedical Congress 2104: Redefining Healthcare for the Future-Educating, Innovating & Leading for Progress, Singapore: Singapore.
Rantanen, T., K. Masaki, D. Foley, G. Izmirlian, L. White, and J.M. Guralnik, Grip strength changes over 27 yr in Japanese-American men. Journal of applied physiology, 1998. 85(6): p. 2047–2053.
Sternäng, O., C.A. Reynolds, D. Finkel, M. Ernsth-Bravell, N.L. Pedersen, and A.K. Dahl Aslan, Factors associated with grip strength decline in older adults. Age and Ageing, 2015. 44(2): p. 269–274.
Chu, L.-W., et al., Late-life body mass index and waist circumference decrease progressively in amnestic mild cognitive impairment and Alzheimer’s disease. Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association, 2009. 5(4): p. P131-P131.
Ghaderpanahi, M., et al., Association Between Late-Life Body Mass Index, Waist Circumference, and Dementia: Kahrizak Elderly Study. Journal of the American Geriatrics Society, 2012. 60(1): p. 173–174.
Power, B.D., H. Alfonso, L. Flicker, G.J. Hankey, B.B. Yeap, and O.P. Almeida, Body adiposity in later life and the incidence of dementia: the health in men study. PloS one U6 -ctx_ver=Z39.88-2004&ctx_enc=info%3Aofi%2Fenc%3AUTF-8&rfr_id=info:sid/summon.serialssolutions.com&rft_val_fmt=info:ofi/fmt:kev:mtx:journal&rft.genre=article&rft.
Gatz, M., C.A. Reynolds, D. Finkel, N.L. Pedersen, and E. Walters, Dementia in Swedish Twins: Predicting Incident Cases. Behavior genetics, 2010. 40(6): p. 768–775.
Shin, H.Y., S.W. Kim, J.M. Kim, I.S. Shin, and J.S. Yoon, Association of grip strength with dementia in a Korean older population. Int J Geriatr Psychiatry, 2012. 27(5): p. 500–5.
Albers, M.W., et al., At the interface of sensory and motor dysfunctions and Alzheimer’s disease. Alzheimers Dement, 2015. 11(1): p. 70–98.
Di Lazzaro, V., et al., Motor cortex hyperexcitability to transcranial magnetic stimulation in Alzheimer’s disease. J Neurol Neurosurg Psychiatry, 2004. 75(4): p. 555–9.
Buchman, A.S., P.A. Boyle, R.S. Wilson, T.L. Beck, J.F. Kelly, and D.A. Bennett, Apolipoprotein E e4 Allele is Associated With More Rapid Motor Decline in Older Persons. Alzheimer Disease & Associated Disorders, 2009. 23(1): p. 63–69.
Kim, J.M., R. Stewart, I.S. Shin, S.W. Kim, S.J. Yang, and J.S. Yoon, Associations between head circumference, leg length and dementia in a Korean population. Int J Geriatr Psychiatry, 2008. 23(1): p. 41–8.
Narazaki, K., E. Matsuo, T. Honda, Y. Nofuji, K. Yonemoto, and S. Kumagai, Physical Fitness Measures as Potential Markers of Low Cognitive Function in Japanese Community-Dwelling Older Adults without Apparent Cognitive Problems. Journal of sports science & medicine, 2014. 13(3): p. 590–596.
Mielke, M.M., et al., Assessing the temporal relationship between cognition and gait: slow gait predicts cognitive decline in the Mayo Clinic Study of Aging. J Gerontol A Biol Sci Med Sci, 2013. 68(8): p. 929–37.
Vermeulen, J., J.C. Neyens, M.D. Spreeuwenberg, E. van Rossum, D.J. Hewson, and L.P. de Witte, Measuring Grip Strength in Older Adults: Comparing the Grip-ball With the Jamar Dynamometer. J Geriatr Phys Ther, 2015. 38(3): p. 148–53.
Cooper, R., B.H. Strand, R. Hardy, K.V. Patel, and D. Kuh, Physical capability in mid-life and survival over 13 years of follow-up: British birth cohort study. BMJ, 2014. 348(apr28 7): p. g2219.
Leong, D.P., et al., Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet, 2015.
Alencar, M.A., J.M. Dias, L.C. Figueiredo, and R.C. Dias, Handgrip strength in elderly with dementia: study of reliability. Rev Bras Fisioter, 2012. 16(6): p. 510–4.
Blankevoort, C.G., M.J. van Heuvelen, and E.J. Scherder, Reliability of six physical performance tests in older people with dementia. Phys Ther, 2013. 93(1): p. 69–78.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ong, H.L., Chang, S.H.S., Abdin, E. et al. Association of grip strength, upper arm circumference, and waist circumference with dementia in older adults of the wise study: A cross-sectional analysis. J Nutr Health Aging 20, 996–1001 (2016). https://doi.org/10.1007/s12603-015-0643-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12603-015-0643-4