
Abstract
This study is aimed at the isolation, identification, and characterization of potential probiotic strains capable of inhibiting Clostridium difficile in vitro and in vivo. Twenty isolates were isolated from infant fecal samples and screened against C. difficile using their cell-free supernatant. Only three isolates showed maximum inhibition from 56.05 to 60.60%, thus they were characterized for probiotic properties and safety. The results obtained approved their tolerance to the gastrointestinal tract conditions and safety profile. They were identified by sequencing 16S rRNA as Enterococcus faecalis NM815, E. faecalis NM915, and Enterococcus faecium NM1015. For in vivo evaluation, a viable mixture of these three strains (109 CFU/mL) was administrated to a group of mice (treated group) in daily dose for 14 days, then followed by challenge with viable C. difficile (105 CFU/mL) in daily dose for 7 days, then a second administration of a viable mixture of the three strains was done daily for 7 days. In addition, the control group was administered PBS buffer only and the untreated group received PBS buffer instead of the probiotic mixture before and after the challenge with C. difficile. The results obtained from histological analysis confirmed the effectiveness of our three potential probiotic strains which expressed inhibition of C. difficile and maintained the structural integrity of the liver and intestinal cells.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Clostridium difficile is known for its public heath complications, and the Centre for Disease Control (CDC) listed it as one of the top three “urgent threat” pathogenic microorganisms that needs immediate and urgent attention [1]. C. difficile infections (CDI) pose a high health risk that can lead to death especially in older adults [2]. Previous studies showed that 25–30% of patients with an episode of CDI had experienced recurrence [3,4,5]. The most common treatment for CDI involves oral antibiotic therapy using vancomycin, metronidazole, or fidaxomicin [6] with success range from 64 to 82% [7]. However, oral antibiotic therapy is very expensive [8, 9] and carries the risk of promoting antibiotic-resistant organisms then disrupting the beneficial microbiota [10]. Probiotics represent an alternative approach for CDI by enhancing gut-associated immunity and improving the gut microbiota imbalance [11].
Probiotics are defined as live microorganisms that, when administered in adequate amounts, confer a health benefit for the host [12]. It has been proposed by researchers that the routine use of probiotics in hospitalized patients receiving antibiotics may prevent CDI. Probiotics capable of producing substances such as bacteriocins, hydrogen peroxide, and short-chain fatty acids can cause inhibition of C. difficile spore germination [13, 14]. In addition, they can enhance the antibody-secreting cells in the intestinal mucosa and boost immune responses against C. difficile and its toxins [15]. Furthermore, probiotics can compete with clostridia via competitive exclusion and avoid their pathogenic action [16]. In this study, we isolated and characterized new probiotic strains capable of inhibiting C. difficile in vitro and in vivo as an effective and safe strategy for controlling CDI.
Materials and Methods
Collection of Fecal Samples and Isolation of Lactic Acid Bacteria (LAB)
The breast-fed infants were chosen in this study as a reliable source of probiotic bacteria. Fecal samples were collected from 20 infants aged from 1 to 12 months and resuspended into sterile saline and kept at −40 °C. For isolation, each fecal sample was inoculated into de Man, Rogosa, and Sharpe (MRS) broth (Oxoid, Basingstoke, UK) supplemented with 0.05% w/v l-cysteine (Sigma-Aldrich, St. Louis, MO, USA) and incubated anaerobically using anaerobic jars and AnaeroGen kits (Oxoid) at 37 °C for 48 h. The cultures were then plated on MRS plus 0.05% w/v l-cysteine agar plates and incubated anaerobically at 37 °C for 48 h. Five colonies were picked randomly from each plate and preliminarily evaluated for Gram stain reaction, microscopic examination, and catalase production.
Microorganisms and Growth Conditions
C. difficile ATCC 43255, a ribotype 087 strain with high levels of the two toxins A and B which was isolated from an abdominal wound, was used in this study and obtained from the American Type Culture Collection (ATCC). C. difficile was grown on clostridial reinforced medium or brain heart infusion (BHI) broth (Oxoid) supplemented with 10% l-cysteine (w/v) under anaerobic conditions using the anaerobic jar and the AnaeroGen sachet (Oxoid) at 37 °C for 48 h.
Screening of Fecal Isolates for C. difficile Inhibition Using Their Cell-Free Supernatants
Twenty isolates were grown in MRS broth overnight and cells were collected and resuspended in phosphate buffered saline (PBS) to obtain an O.D600 nm of 0.22, and 1 mL of this suspension was added to 9 mL MRS broth and incubated at 37 °C for 48 h followed by centrifugation at 4000 rpm for 10 min and filtered using 0.22-μm membrane filters. The filtered supernatants from the selected isolates were neutralized to pH 7.0.
An overnight BHI (Oxoid) culture of C. difficile was centrifuged and resuspended in PBS buffer to obtain an O.D600 nm of 0.22, and 400 μL of this suspension was added to 10 mL BHI broth with 2 mL of each isolate supernatant individually or 2 mL MRS broth at pH 6.8 and pH 3.9 for controls with and without pH neutralization, respectively. These were incubated at 37 °C for 0 and 48 h, and the growth was measured at 600 nm on each time interval against a blank (5.5 mL BHI/1 mL MRS). The difference in O.D600 measurements in the control samples between 0 and 48 h of incubation was defined as 100% growth. Differences in O.D600 measurements at 0 and 48 h of incubation of the test samples were calculated as percentages of the value obtained from the control. The isolates which exhibited growth reduction inhibition percentage as 50% or more were picked. Each test was performed in triplicate.
Agar Well Diffusion Assay
The abilities of the selected isolates to inhibit the C. difficile were further tested by agar well diffusion assay. Cell-free supernatants from overnight cultures were collected by centrifugation and their pH were neutralized followed by filter sterilization. Overnight culture of C. difficile was diluted 1:50 (v/v) in reinforced clostridial agar and dispensed in petri dishes, and wells were made at the solidified agar. The wells were filled with 50 μL neutralized supernatant or non-neutralized supernatant; in addition, a well was filled with 50 μL broth and was used as a control in each plate. The plates were kept anaerobically at 37 °C for 24 h and were examined for inhibition zones >1 mm. Each test was performed in duplicate.
Auto- and Coaggregation Assays
The abilities of the isolates to autoaggregate in addition to coaggregate with C. difficile were assessed as described previously [17] in triplicate. Briefly, stationary-phase cells from isolated cultures were centrifuged, washed, and resuspended in PBS to O.D600 = 0.25. In addition, a heat inactivated cell suspension was prepared by incubation at 95 °C for 10 min. The assays were done for viable and heat inactivated cell suspension.
To determine percentage autoaggregation, the cell suspensions were incubated in aliquots at 37 °C and were monitored at various times (0, 2, 5, and 24 h). The autoaggregation percentage was calculated according to the equation 1 – (A t/A 0) × 100, where A t represents the absorbance at time t = 2, 5, and 24 h and A 0 is the absorbance at t = 0.
To determine the selected isolates’ binding ability with the pathogen C. difficile, coaggregation assay was conducted by mixing an equal volume (4 mL) of cell suspension of the tested isolates and C. difficile followed by incubation at 37 °C for 0, 2, 5, and 24 h. Individual cultures of all the selected isolates and C. difficile were also maintained separately. Absorbance (A 600 nm) of the mixed and individual cultures was recorded at 0, 2, 5, and 24 h and the percentage coaggregation was calculated as Coaggregation % = ((AX + AY) − (AM)/(AX + AY)) × 100, where AX and AY represent the absorbance of the individual suspension of C. difficile and tested isolates, respectively, and AM represents the absorbance of the mixed suspensions.
DNA Extraction and PCR
DNA was extracted from bacterial cultures using the AxyPrep bacterial genomic DNA miniprep kit (Axygen Biosciences, Union City, CA, USA) according to the manufacturer’s instructions. PCR was carried out on a thermal cycler system Mj Mini (Bio Rad, Hercules, CA, USA) using PCR Master Mix (Fermentas Life Sciences, Vilnius, Lithuania), and primers (Table 1) were obtained from Sigma Scientific Services (Cairo, Egypt). For purification, a QIAquick PCR purification kit (Qiagen, Hilden, Germany) was used according to the manufacturer’s instructions.
Molecular Identification of Selected Isolates
Isolates were identified by amplification and sequencing of their 16S rRNA genes using universal primers FD1 and RD1 [1]. Sequencing was conducted using the dideoxy chain termination method [19], and sequence similarity was determined by the BLAST search tool within the National Centre of Biotechnology Information [20].
Co-Culture of Selected Isolates with C. difficile
The co-culture protocol was carried out as described previously [21]; in brief, overnight cultures from each selected isolate were diluted 10-fold in fresh MRS broth and 600 μL from each were placed altogether in a sterile tube and combined with 200 μL of a fresh C. difficile culture (diluted 1:100). For controls, co-culture of the isolates without C. difficile and culture of individual C. difficile were used. These co-cultures were incubated anaerobically at 37 °C for 48 h. Serial dilutions were spread on two different agar plates, MRS and C. difficile selective agar medium (Oxoid, UK), to determine the total count on each medium.
Characterization of the Probiotic Features of the Selected Isolates
Acid and Bile Tolerance
As the stomach is considered the first transit point in the digestive tract for the isolates, therefore the acid and bile tolerance were the initial assessment for the selected isolates as probiotic. For acid tolerance, the cells of overnight cultures were collected by centrifugation and resuspended in four tubes of PBS adjusted to four different pH values, 1.5, 3, 5, and 7, then incubated at 37 °C for 0, 2, 4, and 6 h where the cells at each time interval were collected by centrifugation and resuspended in PBS pH 7, and then serial dilutions were incubated on MRS agar plates at 37 °C for 48 h for viable count. The experiment was performed in triplicate, and the survival percentage was calculated compared to the control.
For bile tolerance, test cultures were supplemented with oxgall bile (0.3 and 0.7% w/v) (Sigma-Aldrich, St. Louis, MO, USA) then incubated for 3 h at 37 °C. Survival of control (no bile) and test cultures (with oxgall) was determined by plating on MRS agar plates and incubation for 48 h at 37 °C followed by calculating the colony-forming unit (CFU) compared to the control. The experiment was performed in triplicate.
Tolerance to Pancreatin
Tolerance to pancreatic enzyme was performed in triplicates as described previously [22]. After incubation at 37 °C for 24 h, 30 μL of MRS broth strain cultures was transferred in microtiter plates containing 270 μL of the test medium [150 mM NaHCO3 and 1.9 mg/mL pancreatin (Sigma-Aldrich); pH 8] and incubated at 37 °C with shaking. The CFU was determined by plating onto MRS agar after 0, 3, and 6 h, and the survival percentage was calculated and compared to the control. The test was performed in triplicate.
Hydrophobicity
Determination of cell surface hydrophobicity was assessed based on the ability of the bacteria to adhere to hydrocarbon as described previously [23]. The n-hexadecane was used as a hydrocarbon example. Decrease in the absorbance of the aqueous phase at A 560 nm was used as a measure of the cell surface hydrophobicity (H%), which was calculated with the formula H% = ((A 0 − A)/A 0) × 100, where A 0 and A are the absorbance before and after extraction with n-hexadecane, respectively.
Adhesion to Human Colon Carcinoma Cell Line (Caco-2 Cells)
The adhesion of the bacterial isolates to Caco-2 cells was carried out at Vacsera (the holding company of biological products and vaccines, Cairo, Egypt) as described previously [24]. The number of bacteria adhering to the Caco-2 cells (B2) was determined by subtracting the number of non-adherent bacteria (B1) from the initial number of bacteria (B0) added to the well. The test was performed in triplicate. The adhesion percentage was then calculated as:
Safety Profile of the Selected Isolates
Susceptibility to Antibiotics
Antibiotic susceptibilities against the following eight antibiotics, ampicillin, chloramphenicol, kanamycin, tetracycline, ciprofloxacin, vancomycin, oxytetracycline, and erythromycin, were determined as described previously [25]. The antibiotic susceptibility discs were obtained from bioMerieux (Lyon, France). Diameters of inhibition zones were measured and the results expressed as resistant, intermediate, and susceptible, according to the guidelines of the Clinical and Laboratory Standards Institute (CLSI).
Determination of Enterococcal Virulence Factors
PCR with primers (Table 1) were used to screen for the common enterococcal virulence genes, cylA, which is involved in the expression of cytolysin, the aggregation substance gene (agg), two cell wall adhesins (efaAfs and efaAfm), and two sex pheromones (cob and ccf) [26].
Hemolytic Activity
Hemolysin activity was assessed on Columbia blood agar (Oxoid) containing 5% v/v human blood after 48 h of incubation at 37 °C.
In Vivo Evaluation of Potential Probiotic Strains in Prevention of CDI
Mice
For in vivo experiment, 48 Swiss albino female mice aged 6 weeks were obtained from the National Research Centre—Egypt (NRC) and kept at the animal facilities of NRC. All mice received the standard care according to the standard guidelines during all the stages of the experiment to avoid any discomfort. The animal experiments were conducted according to the guidelines of the ethical committee of the NRC (Egypt) and under its approval.
Administration of the Selected Probiotic Strains to Mice
The intragastric method was used for administration of the selected strains to the experimental mice which were divided into three groups. Each group contained eight mice: control group which received 200 μL of PBS, untreated group which received 200 μL of PBS before challenge with C. difficile, and the treated group which received a mix of the three probiotic strains containing 109 CFU in volume 200 μL of PBS. The administration was done in daily dose for 14 days then followed by the challenge experiment.
Challenge with C. difficile
Cells were collected from fresh culture of C. difficile by centrifugation and resuspended in PBS buffer to OD600 1.0. Two hundred microliters from the C. difficile cell suspension was administered intragastrically to the treated and untreated mice groups in daily dose for 7 days, after which the treated and untreated groups received a daily dose for 7 days more with a mixture suspension of the three strains and PBS, respectively. The mice were then sacrificed and histological examination for the intestine and liver was done.
Statistical Analysis
Results were evaluated statistically by Student’s t test using GraphPad Prism 5.00, and a p value <0.05 was considered significant.
Results
Isolation of LAB from Fecal Samples
Infant fecal samples were used to isolate LAB for further screening as potential probiotics to control the enteropathogen C. difficile. Initially, 20 Gram-positive, catalase-negative isolates were picked and examined for inhibition of C. difficile.
Screening the Inhibition Abilities of the Isolates Against C. difficile
The ability of the isolates’ supernatant to control the growth of C. difficile was determined in broth cultures as described in the “Materials and Methods” section. The results indicated that the growth reduction percentage of C. difficile varied according to the isolates’ supernatant from a minimum value of 16.0% to a maximum of 60.6% (Fig. 1). The isolates 5, 17, and 18 showed the highest growth reduction percentage of C. difficile as 59.44, 56.05, and 60.60%, respectively, thus, they were chosen for further investigation. When the neutralized supernatants of these three isolates were used in the assay, the growth of C. difficile was reduced to 39.00, 31.98, and 36.11%, respectively (Fig. 2). It has previously been shown that non-neutralized supernatants induced higher inhibition abilities than neutralized supernatants [27, 28].

Inhibition percentage of the cell-free supernatant of fecal isolates against C. difficile in broth assays. Data are presented as the mean ± SD of three experiments

Inhibition percentage of the cell-free neutralized and non-neutralized supernatant of fecal isolates 5, 17, and 18 against C. difficile in broth assays
Antimicrobial Activity
The three isolates 5, 17, and 18 were screened for their antimicrobial activity toward C. difficile as individual and mix using the agar well diffusion method. Zones of inhibition were measured; the neutralized supernatant showed inhibition zones as 20 mm for isolate 18, followed by 18 and 15 mm for isolate 5 then isolate 17, respectively. At the same time, the non-neutralized supernatant showed slightly higher inhibition zones as 27, 21, and 20 mm for isolates 18, 5, and 17, respectively. Furthermore, the inhibition zones of the neutralized and non-neutralized supernatants of their mix cultures were 27 and 35 mm, respectively, whereas no inhibition zone was detected for MRS broth as a control.
Aggregation Ability
It was proposed that probiotic bacteria have the ability to compete with pathogens by several mechanisms, among them the coaggregation with certain pathogenic bacteria, adherence to epithelial cells, and biofilm formation based on autoaggregation and surface hydrophobicity [29]. Hence, the autoaggregation of probiotic bacteria is important to inhibit pathogens and the coaggregation may inhibit colonization by pathogens [30]. The results of autoaggregation of isolates 5, 17, and 18 ranged from 48 to 76% at 37 °C for 24 h (Fig. 3). The three isolates also demonstrated noticeable coaggregation abilities with C. difficile and varied based on the incubation period (Table 2); it ranged from 44.14 to 71.83% for 24 h and isolate 5 exhibited the highest coaggregation percentage (71.83%) suggesting its potential ability to prevent C. difficile from colonizing epithelial cells and mucosal surfaces. In addition, the heat-inactivated cell suspensions showed good coaggregation with isolates 5 and 17 after 24 h as 84.71 and 57.34%, respectively. It has previously been proposed that autoaggregation can facilitate probiotic bacteria to adhere to the human gut and promotes colonization, and coaggregation with a pathogen can promote the displacement of pathogens [17].

Autoaggregation ability of the three isolates 5, 17, and 18 were cultivated in MRS broth for 24 h. The results are expressed as percentage of aggregated bacteria (a) and microscopic examination of autoaggregation ability of the isolates (b) where preparations were stained by Gram (magnification ×1000)
Co-Culture of the Selected Three Isolates and C. difficile
The growth of C. difficile was inhibited by each of the isolates 5, 17, and 18. Therefore, a mix of the three isolates (5, 17, and 18) in co-culture with C. difficile was evaluated. The counting of CFU after the incubation of the co-culture on C. difficile selective agar and MRS agar plates for 48 h at 37 °C revealed obvious reduction in C. difficile growth. A total of 102 CFU/mL of C. difficile was detected from co-cultures compared to its positive control expressing 107 CFU/mL. The CFU of the co-cultures of the three isolates with C. difficile and without C. difficile were calculated from the MRS agar plates as 1.8 × 109/mL and 2 × 109/mL, respectively.
Molecular Identification of the Selected Isolates Using 16S rRNA Sequencing
The 16S rRNA genes from isolates 5, 17, and 18 were amplified by PCR and sequenced, and the resulting sequences were analyzed by the BLAST search tool by comparison to the bacterial 16S rRNA genes available in the database at NCBI. The results indicated that isolate 5 and 17 showed 99% homology to Enterococcus faecalis while isolate 18 showed 98% homology to Enterococcus faecium. The isolates 5, 17, and 18 were designated as E. faecalis NM815, E. faecalis NM915, and E. faecium NM1015, and their partial 16S rRNA nucleotide sequence were deposited in GenBank under accession numbers KU365166, KU365167, and KU365168, respectively.
Characterization of the Probiotic Features
Viability and survival are important features for probiotic bacteria to be able to afford their health beneficial and therapeutic purposes. Thus, their ability to tolerate acid, bile salts, and pancreatic enzymes is necessary to enable their colonization in the human gut.
Low pH Tolerance
The stomach has the highest acidity in the human body and the pH can drop to 1.5, thus the survival of E. faecalis NM815, E. faecalis NM915, and E. faecium NM1015 were examined under acidic conditions (pH 1.5, 3.0, and 5.0). The results shown in Table 3 (A) revealed that all three strains have good survival in all the tested pH conditions during 2 h of incubation, where the survival percentage decreased with extended incubation period up to 6 h, particularly at pH 1.5 as the survival percentage was reduced to 38.87 and 23.64% after 4 and 6 h of incubation, respectively. E. faecium NM1015 showed the highest survival percentage (55.88%) for 4 h at pH 1.5 followed by E. faecalis NM915 (40.05%) and E. faecalis NM815 (38.87%).
Bile Tolerance
The bile concentration in the duodenum varies according to the food ingested as well as the time of digestion, and it has been reported that the bile concentration can range between 0.5 and 2.0% [31]. The three Enterococcus strains were examined for their tolerance to different concentrations of bile salts (0.3, 0.7, and 2.0% w/v). As shown in Table 3 (B), all three strains showed good survival at 0.3 and 0.7% w/v bile salts up to 6 h and even 24 h of incubation while their survival in 2% w/v bile salts decreased after 6 h of incubation. Strain E. faecalis NM915 exhibited the highest survival percentage (61.63%) after 24 h of incubation followed by E. faecalis NM815 (48.4%) and E. faecium NM1015 (34.67%).
Pancreatin Tolerance
The tolerance of the three Enterococcus strains (NM815, NM915, and NM1015) to pancreatic enzyme was evaluated, and the results are listed in Table 3 (C). All strains showed good survival (70.82–86.12%) in the presence of pancreatic enzyme for 6 h. E. faecalis NM915 (86.12%) showed the highest survival (95.6%), followed by E. faecium NM1015 (84.69%) and E. faecalis NM815 (70.82%).
Hydrophobicity
The hydrophobic properties of the bacterial surface are involved in the adhesion of bacteria to host tissue. The assessment of microbial adhesion to hexadecane is a valid protocol to evaluate the ability of a strain to adhere to epithelial cells [32] that commonly retain good communication with epithelial cells.
The three Enterococcus strains NM815, NM915, and NM1015 exhibited moderate hydrophobicity percentages of 36.5, 33.5, and 23.5%, respectively, to n-hexadecane after 30 min, while after 5 h the percentages increased to 40, 45.6, and 39.5%, respectively. These results substantiate their ability to adhere to the epithelial cells.
Adhesion to Caco-2 Cells
The adhesion ability to the intestinal epithelial cells is necessary for probiotic cultures for colonization [33], and several factors have been suggested for the adhesion of probiotic bacteria to epithelial cells such as surface proteins, cell-bound exopolysaccharides, and cell-wall-associated proteins. The adhesion ability of the three strains to Caco-2 cells was evaluated. Strain NM1015 showed the highest adhesion ability (58%), followed by NM815 (49%) and NM915 (44%) by giving CFU 3.44E+06, 2.48E+06, and 2.48E+06, respectively.
Safety Assessment of the Enterococcus Strains
Antibiotic Sensitivity
The antibiotic sensitivities of the three Enterococcus strains (NM815, NM915, and NM1015) were tested using eight antibiotics, and the results are shown in Table 4. According to CLSI guidelines [25], all the three strains were resistant to erythromycin, kanamycin, and ciprofloxacin, which could be considered as intrinsic resistance. However, all of them were susceptible to four of the tested antibiotics (chloramphenicol, oxytetracycline, tetracycline, and vancomycin). In addition, strain NM815 was susceptible to ampicillin while strains NM915 and NM1015 were resistant.
Antibiotic resistance in the genus Enterococcus can be a concern as acquired resistance has been found to be encoded in plasmids and transposons [34, 35], from which vancomycin resistance is the most significant concern for Enterococcus safety. However, all three Enterococcus strains NM815, NM915, and NM1015 were sensitive to vancomycin. It has been reported that intrinsic resistance to some antibiotics is a common feature for some Enterococcus strains [34]. Furthermore, enterococci have been a part of food production for centuries [36] due to their favorable metabolic activities (lipolysis, esterolysis, citrate utilization, etc.) that contribute to the typical taste and flavor of fermented foods [37, 38].
Hemolytic Activity
All three strains NM815, NM915, and NM1015 did not show any hemolytic activity on blood agar plates.
Detection of Enterococcal Virulence Genes
The three strains were tested for the presence of common enterococcal virulence genes by PCR, and the results are shown in Table 5 revealing different profiles, with strain E. faecalis NM815 being positive for agg, ccf, and efaAfs genes and strain E. faecalis NM915 positive for the agg, ccf, efaAfs, and cob genes, while strain E. faecium NM1015 was positive for agg, ccf, and efaAfm genes. All three strains were negative for the cylA gene, which is considered the main pathogenic factor involved in hemolysin/cytolysin production [39, 40]. All the three strains carried the agg gene encoding for an aggregation protein that is involved in adherence to eukaryotic cells as well as cell aggregation [41, 42], and this may have a role in disrupting the colonization of pathogens. Genes efaAfs and efaAfm are involved in the adhesion process and agg is desired in the absence of the major pathogenic traits hemolysin and cytolysin. The cob and ccf genes encode sex pheromones and are not considered a pathogenic characteristic by themselves, as they may have the potential to acquire the respective sex pheromone plasmids related to transfer of the antibiotic-resistant genes [43] which are particularly significant to the problems associated with acquired glycopeptide resistance as vancomycin and hence all three strains are susceptible to vancomycin confirming they are free from the vancomycin-resistant genes and indicating that the presence of the cob and ccf genes within their genome has no concern. Taken together, the results of hemolytic activity, antibiotic susceptibility, and presence of pathogenic genes, the three tested isolates would be considered as potentially safe and promising as probiotics.
In Vivo Evaluation of the Potential Probiotic Strains in Controlling C. difficile in Mice
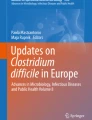
In regard that our strains showed controlling the growth of C. difficile in vitro, an in vivo experiment was conducted as described in the “Materials and Methods” section to evaluate their ability in mice. The histological analyses were performed for intestinal and liver tissues from the mice groups used in this study. Figure 4 shows that administrating the mix of the three enterococcal strains for 2 weeks before the challenge with C. difficile and 7 days after the challenge protects tissues from damage compared to the untreated group. Dense inflammation and mucin depletion for epithelial injury were evident in the untreated group. In contrast, the treated group indicated that intestinal tissues and epithelial cells within the treated group showed minimal inflammatory infiltrate and normal-looking crypts and retained structural integrity. Furthermore, the histological analysis of liver showed mild inflammation of liver in the untreated group while the treated and control groups represent normal liver (Fig. 4).

Representative histology pictures of the intestine (a) and liver (b) about the protection effects of enterococcal strains (NM815, NM915, NM1015) from C. difficile infection (CDI) after challenge in the treated mice group compared to control and untreated mice group
The C. difficile was investigated within fecal samples collected from the mice by count. The C. difficile count on selective agar plates showed a significant difference between the treated and untreated groups, 109 ± 0.06 CFU/mL and 5 × 109 ± 0.05 CFU/mL, respectively, with p value = 0.0003.
Discussion
This study aimed at the isolation, identification, characterization, and evaluation of three potential probiotic strains E. faecalis NM815, E. faecalis NM915, and E. faecium NM1015 for their ability to control C. difficile in vivo in animal experiments.
The infant feces were used as a source of isolation for probiotics targeting the LAB group as it is known since many centuries in the food and dairy fermentations and generally recognized as safe (GRAS) for human consumption. Probiotic bacteria received great attention in recent years to control the CDI which cause a serious health problem especially in older patients. The initial screening revealed 3 isolates out of 20 that showed more than 50% inhibition against the C. difficile when their supernatant was used in inhibition broth test, and this inhibition action would be due to antibacterial substances in addition to organic acids where this inhibition was slightly reduced when neutralized supernatants were used. Further in vitro evaluation using the agar well diffusion assay confirmed the antibacterial effect of these three isolates by giving inhibition zones.
The three isolates 5, 17, and 18 also showed antimicrobial activity toward C. difficile using the agar well diffusion method. When the mixture of these isolates was used in co-culture with C. difficile, an inhibition in the growth of this pathogen was observed. These results are in agreement with the results obtained from other LAB where Yun et al. [44] showed the ability of Lactobacillus acidophilus GP1B cell extract to control C. difficile-associated disease. Our three enterococci isolates have been identified by molecular method to the species level and named as E. faecalis NM815, E. faecalis NM915, and E. faecium NM1015.
Enterococcus faecalis and faecium strains are frequently isolated from food products, and certain strains have been used as cheese starter and food products in the market worldwide [45]. Moreover, they are used as probiotics in many applications for human and animals [46]. Nevertheless, some E. faecalis strains are also considered as nosocomial pathogens and impact on some contagions such as endocarditis and urinary tract infections [47]. Thus, the selection of food-grade enterococcal strain is a very crucial step as probiotic; therefore, we assessed the safety of these strains in addition to their ability to survive through the conditions resembling the GI tract. The three strains showed good survival for 3 h at low pH (1.5), 2.0% bile salts, and pancreatic enzyme. Furthermore, they exhibited good ability for adhesion to hydrocarbons and Caco-2 human cell line which confirm their abilities to colonize the GI tract to secrete their beneficial effects and support their function for competitive exclusion of enteropathogens. The conclusion of their safety and probiotic features assessment approved them as potential probiotic strains, thus we evaluate their ability to control the CDI in vivo in a mice experiment in which a mixture from the three strains have been administered to the treated group before and after the challenge with C. difficile and was compared to the control group which received PBS only without challenge and untreated group which received PBS before and after the challenge with C. difficile. The mice were assessed by histological examination and monitoring the C. difficile. The histology analysis of the intestine and liver revealed the protection effect of the three Enterococcus strains NM815, NM915, and NM1015 from damage and their ability to maintain the structural integrity of the cells. These results are in agreement with others; Kotowska et al. [48] showed that co-administration of probiotic Saccharomyces boulardii decreased the CDI in children. Gao et al. [49] indicate that daily intake of probiotic formula of L. acidophilus CL1285 and Lactobacillus casei LBC80R was able to decrease the CDI in adult patients [49].
As a conclusion, this study would provide novel candidates to control the CDI for medical and pharmaceutical preparations. However, further investigations and evaluations are in progress.
ATCC, American Type Culture Collection; BHI, brain heart infusion; C, Clostridium; Caco-2 cells, human colon carcinoma cell line; CDC, Centers for Disease Control; CDI, C. difficile infections; CFU, colony-forming unit; CLSI, Clinical and Laboratory Standards Institute; E, Enterococcus; GRAS, generally recognized as safe; H%, hydrophobicity percentage; L, Lactobacillus; LAB, lactic acid bacteria; NRC, National Research Centre—Egypt; PBS, phosphate buffered saline.
References
Control C.f.D and Prevention (2013) Antibiotic resistance threats in the United States, 2013: Centers for Disease Control and Prevention, US Department of Health and Human Services
Control C.f.D and Prevention (2012) Vital signs: preventing Clostridium difficile infections. MMWR Morb Mortal Wkly Rep 61:157
Norén T, Åkerlund T, Bäck E, Sjöberg L, Persson I, Alriksson I, Burman L (2004) Molecular epidemiology of hospital-associated and community-acquired Clostridium difficile infection in a Swedish county. J Clin Microbiol 42:3635–3643
Musher DM, Aslam S, Logan N, Nallacheru S, Bhaila I, Borchert F, Hamill RJ (2005) Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole. Clin Infect Dis 40:1586–1590
Pépin J, Alary ME, Valiquette L, Raiche E, Ruel J, Fulop K, Godin D, Bourassa C (2005) Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada. Clin Infect Dis 40:1591–1597
Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG, McDonald LC, Pepin J, Wilcox MH (2010) Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol 31:431–455
Aslam S, Hamill RJ, Musher DM (2005) Treatment of Clostridium difficile-associated disease: old therapies and new strategies. Lancet Infect Dis 5:549–557
Wilcox M, Cunniffe J, Trundle C, Redpath C (1996) Financial burden of hospital-acquired Clostridium difficile infection. J Hosp Infect 34:23–30
Louie TJ, Miller MA, Mullane KM, Weiss K, Lentnek A, Golan Y, Gorbach S, Sears P, Shue YK (2011) Fidaxomicin versus vancomycin for Clostridium difficile infection. N Engl J Med 364:422–431
Rodríguez-Julbe MC, Ramírez-Ronda CH, Arroyo E, Maldonado G, Saavedra S, Meléndez B, González G, Figueroa J (2004) Antibiotics in older adults. P R Health Sci J 23(1):25–33
Doron S, Gorbach SL (2006) Probiotics: their role in the treatment and prevention of disease. Expert Rev Anti-Infect Ther 4:261–275
FAO/WHO (2001) Evaluation of health and nutritional properties of probiotics in food, including powder milk with live lactic acid bacteria. Food and Agricultural Organization of United Nations and World Health Organization Expert Consultation Report
Karpa KD (2007) Probiotics for Clostridium difficile diarrhea: putting it into perspective. Ann Pharmacother 41:1284–1287
McFarland LV, Beneda HW, Clarridge JE, Raugi GJ (2007) Implications of the changing face of Clostridium difficile disease for health care practitioners. Am J Infect Control 35:237–253
Gorbach SL (2000) Probiotics and gastrointestinal health. Am J Gastroenterol 95:S2–S4
Seal D, Borriello S, Barclay F, Welch A, Piper M, Bonnycastle M (1987) Treatment of relapsing Clostridium difficile diarrhoea by administration of a non-toxigenic strain. Eur J Clin Microbiol 6:51–53
Collado MC, Meriluoto J, Salminen S (2008) Adhesion and aggregation properties of probiotic and pathogen strains. Eur Food Res Technol 226:1065–1073
Weisburg WG, Barns SM, Pelletier DA, Lane DJ (1991) 16S ribosomal DNA amplification for phylogenetic study. J Bacteriol 173:697–703
Sanger F, Nicklen S, Coulson AR (1977) DNA sequencing with chain-terminating inhibitors. Proc Natl Acad Sci U S A 74:5463–5467
Altschul SF, Madden TL, Schäffer AA, Zhang J, Zhang Z, Miller W, Lipman DJ (1997) Gapped BLAST and PSI-BLAST: a new generation of protein database search programs. Nucleic Acids Res 25:3389–3402
Folkers BL, Schuring C, Essmann M, Larsen B (2010) Quantitative real time PCR detection of Clostridium difficile growth inhibition by probiotic organisms. North Am J Med Sci 2:5–10
Rönkä E, Malinen E, Saarela M, Rinta-Koski M, Aarnikunnas J, Palva A (2003) Probiotic and milk technological properties of Lactobacillus brevis. Int J Food Microbiol 83:63–74
Vinderola C, Reinheimer J (2003) Lactic acid starter and probiotic bacteria: a comparative “in vitro” study of probiotic characteristics and biological barrier resistance. Food Res Int 36:895–904
Deepika G, Green RJ, Frazier RA, Charalampopoulos D (2009) Effect of growth time on the surface and adhesion properties of Lactobacillus rhamnosus GG. J Appl Microbiol 107:1230–1240
Wayne P (2007) Clinical and laboratory standards institute. Performance standards for antimicrobial susceptibility testing
Eaton TJ, Gasson MJ (2001) Molecular screening of Enterococcus virulence determinants and potential for genetic exchange between food and medical isolates. Appl Environ Microbiol 67:1628–1635
Schoster A, Kokotovic B, Permin A, Pedersen P, Dal Bello F, Guardabassi L (2013) In vitro inhibition of Clostridium difficile and Clostridium perfringens by commercial probiotic strains. Anaerobe 20:36–41
Ratsep M (2014) Effect of Lactobacillus plantarum strains on clinical isolates of Clostridium difficile in vitro. J Prob Health 2:119. doi:10.4172/2329-8901.1000119
Süßmuth SD, Muscholl-Silberhorn A, Wirth R, Susa M, Marre R, Rozdzinski E (2000) Aggregation substance promotes adherence, phagocytosis, and intracellular survival of Enterococcus faecalis within human macrophages and suppresses respiratory burst. Infect Immun 68:4900–4906
Boris S, Suárez JE, Vázquez F, Barbés C (1998) Adherence of human vaginal lactobacilli to vaginal epithelial cells and interaction with uropathogens. Infect Immun 66:1985–1989
Davenport HW (1982) Physiology of the digestive tract: Year Book Medical Publishers
Kiely LJ, Olson NF (2000) The physicochemical surface characteristics of Lactobacillus casei. Food Microbiol 17:277–291
Dunne C, O’Mahony L, Murphy L, Thornton G, Morrissey D, O’Halloran S, Feeney M, Flynn S, Fitzgerald G, Daly C (2001) In vitro selection criteria for probiotic bacteria of human origin: correlation with in vivo findings. Am J Clin Nutr 73:386s–392s
Giraffa G (2002) Enterococci from foods. FEMS Microbiol Rev 26:163–171
Hollenbeck BL, Rice LB (2012) Intrinsic and acquired resistance mechanisms in Enterococcus. Virulence 3:421–569
Franz CM, Hummel A, Holzapfel WH (2005) Problems related to the safety assessment of lactic acid bacteria starter cultures and probiotics. Mitt Lebensmittelunters Hyg 96:39–65
Centeno J, Menéndez S, Rodriguez-Otero J (1996) Main microbial flora present as natural starters in Cebreiro raw cow’s-milk cheese (Northwest Spain). Int J Food Microbiol 33:307–313
Schillinger U, Geisen R, Holzapfel W (1996) Potential of antagonistic microorganisms and bacteriocins for the biological preservation of foods. Trends Food Sci Technol 7:158–164
Manolopoulou E, Sarantinopoulos P, Zoidou E, Aktypis A, Moschopoulou E, Kandarakis IG, Anifantakis EM (2003) Evolution of microbial populations during traditional feta cheese manufacture and ripening. Int J Food Microbiol 82:153–161
Kotzamanidis C, Kourelis A, Litopoulou-Tzanetaki E, Tzanetakis N, Yiangou M (2010) Evaluation of adhesion capacity, cell surface traits and immunomodulatory activity of presumptive probiotic Lactobacillus strains. Int J Food Microbiol 140:154–163
Huycke M, Spiegel C, Gilmore M (1991) Bacteremia caused by hemolytic, high-level gentamicin-resistant Enterococcus faecalis. Antimicrob Agents Chemother 35:1626–1634
Muscholl-Silberhorn A, Rozdzinski E, Wirth R (2002) Aggregation substance of Enterococcus faecalis: a multifunctional adhesin. Genes and proteins underlying microbial urinary tract virulence. Springer
Jett BD, Huycke MM, Gilmore MS (1994) Virulence of enterococci. Clin Microbiol Rev 7:462–478
Yun B, Oh S, Griffiths M (2014) Lactobacillus acidophilus modulates the virulence of Clostridium difficile. J Dairy Sci 97:4745–4758
Moreno MF, Sarantinopoulos P, Tsakalidou E, De Vuyst L (2006) The role and application of enterococci in food and health. Int J Food Microbiol 106:1–24
Franz CM, Huch M, Abriouel H, Holzapfel W, Gálvez A (2011) Enterococci as probiotics and their implications in food safety. Int J Food Microbiol 151:125–140
Guzman C, Pruzzo C, LiPira G, Calegari L (1989) Role of adherence in pathogenesis of Enterococcus faecalis urinary tract infection and endocarditis. Infect Immun 57:1834–1838
Kotowska M, Albrecht P, Szajewska H (2005) Saccharomyces boulardii in the prevention of antibiotic-associated diarrhoea in children: a randomized double-blind placebo-controlled trial. Aliment Pharmacol Ther 21:583–590
Gao XW, Mubasher M, Fang CY, Reifer C, Miller LE (2010) Dose–response efficacy of proprietary probiotic formula of Lactobacillus acidophilus CL1285 and Lactobacillus casei LBC80R for antibiotic-associated diarrhea and Clostridium difficile-associated diarrhea prophylaxis in adult patients. Am J Gastroenterol 105:1636–1634
Acknowledgements
This work has been funded by the National Research Centre, Cairo, Egypt.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
None of the authors have any conflicts of interest to disclose.
Rights and permissions
About this article

Cite this article
Mansour, N.M., Elkhatib, W.F., Aboshanab, K.M. et al. Inhibition of Clostridium difficile in Mice Using a Mixture of Potential Probiotic Strains Enterococcus faecalis NM815, E. faecalis NM915, and E. faecium NM1015: Novel Candidates to Control C. difficile Infection (CDI). Probiotics & Antimicro. Prot. 10, 511–522 (2018). https://doi.org/10.1007/s12602-017-9285-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12602-017-9285-7