
Abstract
Poor dietary quality is an underlying contributor to the high rates of maternal and child undernutrition in Timor-Leste. The majority of households own livestock: however, the consumption of domestic animal-source food (ASF) is low, and there are few reports of the utilisation of non-domesticated species. This mixed-methods study was conducted in three villages from mid-2015 to mid-2017. Two hundred and three households with children under 24 months were enrolled in the quantitative study of maternal and child dietary diversity. To explore factors affecting household ASF consumption, 12 key informants were recruited for in-depth interviews and 312 participants, mostly mothers and fathers of young children, for focus group discussions. Participants expressed a desire to consume more ASF. Barriers to ASF consumption include having low income or limited income streams, high levels of small livestock morbidity and mortality leading to small or unstable flock or herd sizes, reserving livestock for sale and ceremonies, and living far from forested areas or where hunting is not allowed. Factors that enable greater ASF consumption include villages being located near forested areas with wild animal populations, those that observe a large number of ceremonies of long duration, households with a greater number of small livestock, and where women are able to make autonomous decisions about livestock assets. Findings suggest that policies and programs designed to achieve sustainable improvements in household nutrition would include a focus on women and improving the health and production of small livestock species frequently utilised by households.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Undernutrition is a major challenge in Timor-Leste, with one-quarter of non-pregnant mothers (aged 14–60 years) being underweight (BMI < 18.5 kg/m2), and one-eighth having short stature (height < 145 cm) (MoH 2015). Poor maternal nutrition pre- and post-conception leads to increased chances of preterm birth, low birthweight at term (birthweight <2500 g), neonatal mortality, child wasting (when children are more than two standard deviations below the World Health Organisation (WHO) Child Growth Standards median for weight for length/height, WHZ), and stunting, (when children are more than two standard deviations below the WHO Child Growth Standards median for length/height for age, HAZ) (ACC/SCN 2000; NSD et al. 2010; WHO 2008). In Timor-Leste, a nationally-representative nutrition survey in 2013 reported that wasting from acute undernutrition affects 11% of children aged 0–59 months, while stunting from chronic undernutrition affects 50% of children aged 0–59 months (Table 1), with 10% of infants already stunted by 5 months (MoH 2015). Child stunting is significantly associated with thinness of the mother if she is the primary carer (MOH 2015). Although the prevalence of stunting has decreased from 58% since the Demographic and Health Survey (DHS) in 2009–2010 (NSD et al. 2010), it remains unacceptably high given the long-term outcomes including decreased cognitive ability, limited capacity for physical labour, lower earning capacity, and increased risk of communicable and non-communicable diseases later in life (DeBoer et al. 2012; WHO 2010a).
Micronutrient deficiencies are also common, with almost 40% of non-pregnant mothers (aged 14–60 years) anaemic (Hb < 120 g/L) - about 40% of which are due to iron deficiency, and 13.5% vitamin A deficient (serum retinol <1.05 μmol/L) (MoH 2015). In children (aged 6–59 months), 63% are anaemic (haemoglobin <110 g/L) – of which 30% are due to iron deficiency, 34% are zinc deficient (<8.7 μmol/L), and 8% are vitamin A deficient (serum retinol <0.7 μmol/L) (MoH 2015). The prevalence of anaemia is reported to have almost doubled since 2009–2010, when 38.2% of children (aged 6–59 months) and 21% of non-pregnant mothers (aged 15–49 years) were reported to be anaemic (NSD et al. 2010). Factors associated with this rise are unknown, and other anaemias due to deficiencies in folate, vitamin B2, vitamin B12 and copper, or parasitic, infectious, and genetic causes are yet to be explored. Currently, there is no published data on the nutritional status of adult men.
Inadequate dietary intake is an immediate cause of undernutrition. In 2013, the Timor-Leste Food and Nutrition Survey (MoH 2015) found that 61% of households had an acceptable food consumption score (FCS) (>42 unique foods consumed within the household over the previous seven days). However, individual dietary data was not collected for adults. Data collection for this 2013 survey spanned the less-rainy to dry post-harvest season, when food is more abundant. The 2009–2010 DHS (NSD et al. 2010) collected information on maternal food consumption during the dry and rainy season and found that the most common food groups consumed in the previous 24 h were grains (92% of mothers) and vitamin A-rich fruits and vegetables (88%). Fifty-three percent of mothers ate animal-source foods (ASF). No analyses were published of associations between maternal nutritional status and food group consumption, but in 2013, increased consumption of vitamin A-rich fruits, eggs, and bread, biscuits or cake were significantly associated with lower prevalence of thinness. There was no association between household FCS and maternal thinness (MoH 2015).
In 2013, it was found that only 18% of children (aged 6–23 months) achieved the minimum acceptable diet (MoH 2015; WHO 2010b), with 79% of children consuming an adequate number of meals but only 28% of children achieving adequate dietary diversity, a measure of individual dietary quality (MoH 2015). Higher household FCS was significantly associated with higher quality diet in children (MoH 2015), though animal-source foods (ASFs) are one of the least-consumed food groups: about a quarter of children (aged 6–23 months) consumed eggs, dairy, meat or fish, and in older children (aged 24–59 months) ASF consumption ranged between 11 and 31% (MoH 2015). A significant statistical association between ASF consumption and decreased levels of stunting was found amongst children aged 24–59 months, (MoH 2015), indicating the importance of ASF in children’s diets.
Animal-source foods are a significant contributor to the nutrient content of plant-based diets as they are rich in proteins and micronutrients that are highly bioavailable and readily absorbed and utilised, particularly haem iron and pre-formed vitamin A, and contain vitamin B12 which is rarely found in foods of plant origin (de Bruyn et al. 2015; Demment et al. 2003; Ianotti et al. 2017; Murphy and Allen 2003; Neumann et al. 2002; Schönfeldt et al. 2013; Wong et al. 2017). They are nutrient-dense, which is especially important for growing infants and young children (IYC) as they have small stomach capacities (Brown 1991; WHO 2009). In other regions, inclusion of ASF in the diets of IYC has been shown to decrease stunting rates, increase cognitive ability and educational attainment rates (Calloway et al. 1992; Darapheak et al. 2013; Ianotti et al. 2017). Increasing consumption of ASF in Timor-Leste is a key component of current government strategies tackling undernutrition (RDTL 2016a).
Possible sources of ASF for home consumption include imported meats (usually frozen broiler chicken carcasses), local produce sold at market, meat, milk and eggs from the household’s own livestock, and undomesticated ASF sourced from fishing or hunting, which is legal in rural areas of Timor-Leste. Although consumption of buffalo milk from own livestock was reported in Timor-Leste in the past, this practice stopped during the struggle for independence when large numbers of livestock were lost (Bettencourt et al. 2015). In 2002, a dairy was established at an agricultural high school in Lautem, Don Bosco Fuiloro, but the harsh climatic conditions caused rapid deterioration of the equipment (Land O’Lakes 2010). This facility is now disused and there are no other facilities for producing pasteurised fresh milk in Timor-Leste. For unpasteurised fresh milk, there may be several reasons why this is not consumed by households: 1) cattle, buffalo and goats in Timor-Leste largely graze on native pastures – the nutritional quality of which may be low and vary greatly by season – and drink from natural water sources. A low plane of nutrition and inadequate water supply would limit reproduction and milk production, making milk more likely to be reserved for feeding calves and kids (Waldron et al. 2016); 2) The cattle reared by households is an Indonesian beef cattle breed, rather than a dual-purpose or milking breed (Waldron et al. 2016), and may have inherently low rates of milk production; 3) The presence of Brucella abortus, a bacterium that is transmissible to humans via unpasteurised milk (Davies and Casey 1973), in buffalo and cattle may mean that the consumption of unpasteurised milk is not recommended or actively discouraged (Conceição 2012; OIE 2016); and 4) milk and dairy product consumption my not be the cultural norm in Timor-Leste. All in all, dairy consumption outside of Dili is low (Bettencourt et al. 2015; MoH 2015), and no published data are available on consumer attitudes. There has also been little published to date about consumer attitudes to imported poultry meat in Timor-Leste. However, literature from Africa and other parts of Asia show a strong preference for locally-sourced chickens (Alders and Pym 2009; Guèye 2000; Melesse 2014; Mtileni et al. 2009; Sankhyan et al. 2013).
In 2011, AMSAT International found that in five municipalities, meats were infrequently consumed, and mostly saved for special events such as parties and ceremonies. Nationally, studies have shown that most ASF consumed by households are purchased (MoH 2015), despite high levels of livestock ownership (RDTL 2016b). While very few studies have explored the reason for low ASF consumption at the sub-national level, Bettencourt et al. (2015) found that in Bobonaro, consumption of own livestock occurs at ceremonies only, when there are no vegetables, and when guests visit, with households reserving livestock as an important form of savings. Small animals – chickens, pigs and goats - are more commonly consumed, while buffalo and cattle are kept for prestige.
Fresh fish is most commonly purchased for consumption at coastal markets with limited availability inland due to lack of transport facilities, while some households purchase imported canned fish (AMSAT International 2011; MoH 2015). Inland sources of undomesticated ASF are rarely mentioned and have not been reported in any of the national surveys to date.
While food proscriptions and prescriptions are common and varied, their impact on nutritional status is probably negligible: Castro (2013) reported that although food proscriptions and prescriptions exist, they affected very small and specific portions of the population and were unlikely to influence nutritional status. Qualitative data on intra-household distribution of foods including ASF report mixed results. AMSAT International (2011) reported that there was no specific pattern in intra-household allocation of ASF within the household in Baucau, Bobonaro, Covalima, Dili, and Oecusse, and Castro (2013) noted similar patterns in Ermera and Liquica. Despite similar findings, the MoH (2015) suggested that this may not truly be the case given the patriarchal societal structure in Timor-Leste.
This article reports on several gaps that exist in the current knowledge, including factors preventing households from consuming their own livestock, the nutritional importance of ceremonies where ASF is consumed and the use of undomesticated ASF in inland areas, and further investigates intra-household food distribution and the role of gender in food and resource access. It focuses on male and female adults within rural households in three municipalities in Timor-Leste: although the authors support that infant and young child (IYC) consumption of ASF is extremely important for growth, an in-depth discussion of factors influencing IYC feeding is out of the scope of this article. However, improved household ASF consumption may also benefit IYC. While all sources of ASF are considered, there is an emphasis on village chickens and eggs, as chicken meat is preferentially consumed in Timor-Leste (AMSAT International 2011), chickens are the most numerous livestock in Timor-Leste (RDTL 2016b), and because this research project was linked to a village chicken vaccination program. By understanding the limitations on households’ utilisation of their livestock assets, policies, programs and findings can be directed toward addressing these issues.
1.1 Study setting
Timor-Leste is a small, half-island nation nestled amongst the Indonesia archipelago just north of Australia. A Portuguese colony for 450 years, and then under Indonesian occupation for 24 years, Timor-Leste had a long struggle towards independence in 2002. The Catholic church played a significant role during this difficult period, and the majority of Timor-Leste’s population identify as Roman Catholic, though most practice their Christian beliefs in parallel with the animistic cultures passed on from their ancestors (Bagnol 2014). Many households have both Christian altars within their homes and also construct traditional houses in which their ancestors are venerated (Bagnol 2014; Traube 1980). In parallel with national government laws and the health system, people often observe local laws (tara bandu) governing the use of water, wild forests and animals, and sacred areas, and consult with traditional healers when sick (Bagnol 2014; Cardinoza 2005; McWilliam 2001).
Timor-Leste is a young nation, with 39% of the population under 15 years old, and 8% over 60 years (RDTL 2016c). The majority (84%) of households are male-headed, and average rural household size is 5.5 (RDTL 2016d). The fertility rate of rural women is 6.0 (NSD et al. 2010). In 2009–2010, almost half of all rural households are in the lowest two wealth quintiles, and 72% of women and 78% of men are engaged in agriculture (NSD et al. 2010). Maize, rice and cassava are the main staple foods of Timor-Leste, with 83% of farming households growing maize as a major crop (Andersen et al. 2013). Timor-Leste experiences a hot tropical climate with distinct periods of rainfall (NSD et al. 2010). Most farmers produce one staple crop per year, as well as small crops of fruits and vegetables (Andersen et al. 2013). In 2015, 87% of all households in Timor-Leste owned livestock, with 82% of these households owning chickens (average 6.4 per household), 82% owning pigs (average 2.9 per household), 30% owning cattle (average 4.25 per household), and 26% owning goats (average 3.4 per household) (RDTL 2016b).
This study is situated in three municipalities of Timor-Leste: Aileu, Bobonaro, and Lautem. Data disaggregated by municipality from 2013 (MoH 2015) show high levels of house (range 86–87% of households) and land ownership (86–99%) across all three municipalities, and among these three municipalities, a similar percentage range of households using unimproved sources of drinking water (28–35%) and having unimproved sanitation (47–55%). There are differences among the municipalities in primary carer education and literacy levels, with highest levels of primary carers with no education (40%) and illiteracy (44%) in Bobonaro, and the lowest levels of primary carers with no education (23%) and illiteracy (24%) in Lautem (MoH 2015).
Disaggregated nutrition data (Table 1) shows that the percentage of households achieving acceptable food consumption scores are similar across the municipalities, ranging from 65 to 73% of households. Lautem has lower rates of underweight in non-pregnant women and stunting in children (aged 24–59 months). However children in Aileu are reported to be more likely to achieve adequate dietary diversity (MoH 2015).
2 Materials and methods
2.1 Intervention, overall study design and objectives
The Village Poultry Health and Biosecurity Programme (VPHB) was an Australian Government-funded programme implemented in 2014–2017 by the Australian Department of Agriculture and Water Resources, the Timor-Leste Ministry of Agriculture and Fisheries, with technical support provided by The University of Sydney and Berrimah Veterinary Laboratory in the Northern Territory of Australia. Its primary aims were to improve village chicken production, largely through community-based control of virulent Newcastle disease (ND) (Alders and Spradbrow 2001) in rural areas of Timor-Leste; to ensure a functional cold chain from vaccine suppliers to rural villages; and to enhance biosecurity measures from a whole island perspective through to that of small-scale rural farmers (Jong 2016).
The VPHB ND vaccination programme was piloted in three villages, selected on the basis of criteria outlined in Table 2. The villages are located in rural locations in the east (Pairara Village, Municipality of Lautem), central (Hautoho Village, Municipality of Aileu), and west (Saburai Village Municipality of Bobonaro) of Timor-Leste (Fig. 1).

Map of Timor-Leste with study sites and villages highlighted and enlarged in black rectangles. Figure adapted from UNMIT GIS Unit (2007)
Associated with the VPHB, a research project titled “Discovering the links between village poultry and maternal and child diets and nutrition” aimed to investigate possible associations between improving village chicken health and maternal and child diets and nutrition. This research project collected data between 2015 and 2017, with analysis currently ongoing. The research was implemented in collaboration with the Timor-Leste Ministry of Agriculture and Fisheries, and the Ministry of Health and was designed as a two-year longitudinal mixed-methods study across (i) three pilot villages where the ND vaccination program was being implemented, and (ii) three matched control villages that were not vaccinating. Objectives of this research include: describing local understanding, concepts and knowledge of food and nutrition; studying the factors that affect maternal and child consumption of nutritious cultivated and non-cultivated foods over the seasonal calendar; and assessing the contributions of village chickens to the diets and nutritional status of children under 24 months at the time of enrolment and their mothers. For this paper, aspects of this research that are relevant to ASF consumption in adults is presented with an overview of the methodological tools employed provided in Table 3.
2.2 Quantitative methods
2.2.1 Maternal dietary diversity
Baseline child and adult carer (mostly maternal) dietary diversity data were collected in April–June 2015 during the less-rainy season. A multiple-pass method was used (Blanton et al. 2006), where participants were firstly asked to freely recall foods consumed in the previous 24-h, secondly to confirm the number of meals and snacks. Lastly, food groups not mentioned, and foods commonly consumed or forgotten were then checked from an extensive food list. Individual foods consumed by participants were entered into Microsoft Excel spreadsheets, and foods grouped according to the Minimum Dietary Diversity for Women (MDD-W) (FAO and FHI 360 2016), and the Infant and Young Child Feeding Minimum Dietary Diversity (IYCF-MDD) (WHO 2010b) indicators, respectively. Maternal dietary diversity data was collected initially in April–June 2015, then once per season thereafter for 1 year. For this paper, summary statistics for adult and child food group consumption as well as individual types of ASF at baseline in the pilot villages were generated using Microsoft Excel, and further analysis of subsequent seasonal data is ongoing.
2.2.2 Participant selection
A target of the VPHB’s Newcastle disease vaccination program is for the percentage of children 6–59 months living in the pilot villages eating four or more food groups per day to increase from 28% (MoH 2015) to 51%. To detect a difference of 23% change in child dietary adequacy with 80% power at the 2-sided 5% level, a sample size of 65 households should be selected from each pilot and control village. Allowing 10% withdrawal or loss to follow up, household enrolment for the study was aimed at 65–72 households from each village. For each village, a list of all households with children under the age of 24 months was created from census data compiled by the lead author and field teams. Where there were fewer than 72 households, all households were invited to participate in the study. Where there were more than 72 households, a blinded hat draw was used to randomly select households to invite to the study. Within each household, the youngest child and his/her mother or primary carer were enrolled into the study. At baseline, 203 households were enrolled in pilot villages.
2.2.3 Data collection and summary
The Minimum Dietary Diversity for Women indicator (MDD-W) (FAO and FHI 360 2016) was translated into Tetun using the key word list where appropriate, the translation verified, and pre-tested with national staff at the Ministry of Agriculture and Health and the field teams. Field teams in each village were trained in the multiple-pass data collection, starting with free listing of foods eaten in meals and snacks, then confirming consumption using a food list. Data collected was entered into Microsoft Excel, and the incidence of mother and carer ASF consumption compared across villages.
2.3 Qualitative methods
Semi-structured key informant interviews and focus group discussions were conducted in pilot villages annually in April–June from 2015 to 2017. Although ideal, interviews and discussion groups were not conducted in control village or during all seasons due to financial and temporal limitations. For the study, topics for these interviews and discussion groups included: determining the number and timing of seasons recognised by communities in the three project locations, assessing community response to the ND vaccination program, identifying issues with food availability, and any issues of food access including proscriptions, prescriptions, or intra-household distribution that would limit the efficacy of programs aiming to increase availability of ASF, and understanding infant and young child feeding (IYCF) practices within the different communities. For this paper, all information pertaining to ASF consumption in adults from any of these topics were included in the analysis.
2.3.1 Individual interviews
Key informant interviews were conducted initially with village leaders, doctors and elders, and municipal agriculture and nutrition staff. Participants for the key informant interviews were predominantly male as these positions were predominantly occupied by men rather than women. During the data collection period from 2015 to 2017, a total of 12 key informant interviews were conducted.
2.3.2 Focus groups (FG)
Participants for FG discussions in 2015 were mostly mothers and fathers selected from households enrolled for the quantitative study, with at least one child under 24 months of age, then snowball sampling was used for subsequent discussion groups based on characteristics such as being mothers, fathers, households that vaccinated their chickens against ND, and households where chickens were not vaccinated (Table 4). When this was not possible (e.g. during periods of agricultural activity), a convenience sample was used. Each FG discussion recruited participants from a single sub-village in order to capture differences within villages and to minimise travel time for participants. They were also disaggregated by gender, as the roles of men and women differ in society, and this may affect the willingness of one gender to speak of their experiences and views in the presence of the other. A total of 47 FG discussions (29 female groups) with a total of 312 participants (197 female) were conducted with different research themes explored in different discussions.
2.3.3 Data collection
A key word list in English and Tetun was constructed in advance, and the interpreter received training on conducting discussion groups. Research topics and questions were pre-tested with the interpreter and with the field teams to ensure the questions were understood and discussion groups functioned effectively, and all interviews and FG discussions were recorded. In a small number of discussion groups, participants preferred to speak their local language rather than Tetun, and an enumerator from the quantitative field team acted as a second interpreter.
Due to the difficulty in verifying translations remotely, the key informant interviews and FG discussions were transcribed under field conditions. English translations of the discussion were transcribed verbatim until the lead author had a good grasp of Tetun. At this point, discussion notes were written in English, with quotes recorded in Tetun, and the notes were checked with the interpreter using the audio recordings to ensure translations and meanings were accurate.
Data collection was facilitated by the lead author and field assistant living amongst the community during all qualitative and quantitative data collection periods. Three seasons (i.e. dry, rainy and less-rainy seasons) were defined at the start of the project in consultation with the community (Wong et al. 2016) and the timing of data collection set to coincide with these three seasons. A total of 244 days were spent in the field over 2 years. This enabled participant-observation as well as participation in village activities including cooking, sharing meals, going to the market, observing people working in their fields, and informal conversations between the researcher, research team, participants, and families. The lead author and field assistant were also able to observe re-enactments of, or participate in sociocultural events happening in the villages during the data collection period. Field notes detailing observations, experiences and thoughts were recorded throughout the data collection periods.
2.3.4 Analysis
The interview and FG data along with field notes were transcribed into Microsoft Word and analysed by the lead author using the Framework Method (Gale et al. 2013). As described by this method, the researcher familiarised herself with all collected data, and a combination of deductive and inductive line-by-line coding was used. Codes were then grouped into categories and charted using a Microsoft Excel spreadsheet, where data on specific categories were compared within and across villages, genders and years and assessed for common themes.
2.4 Integration of qualitative and quantitative methods
The research approach was discussed by a number of co-authors of this paper and was intended to be an evolving process. Initially, the study started with a relatively small set of qualitative research topics, including the experience of seasons and agricultural production, as well as attitudes to chicken rearing and vaccination, and chicken and egg consumption. As data collection progressed, participant-observation and preliminary quantitative results showed strong differences between villages in food group consumption, particularly ASF. As findings emerged from the quantitative study, topics of interest were included in the qualitative question guides to be able to explore and understand these issues more clearly.
2.5 Research teams
The research activities were conducted by the first author (the researcher), a postgraduate research student from Australia, and a field assistant who also acted as a facilitator and interpreter for all questionnaires, interviews, and FG discussions. The field assistant/interpreter is a male Ministry of Agriculture and Fisheries staff member, working at the sub-district level local to Hautoho village, and living in a rural village similar to the research villages. He was selected as the field assistant due to his interest in agriculture and animal health, previous experience living near Pairara village and willingness to travel, familiarity with rural lifestyles, and ability to communicate and develop rapport with study participants.
In each village, the research team was comprised of the researcher, a field assistant/interpreter who works for the Ministry of Agriculture and Fisheries, a staff member from the national or regional Ministry of Health office, and 3–6 male or female (with balanced genders where possible) community members as nominated by the Chief of Village or Sub-village for their good standing within the village. Discrete teams for each village were required due to differences in language groups and cultures between villages.
3 Results
Initial key informant interviews identified three seasons: the less-rainy season from April to July, the dry season from August to October, and the rainy season from November to March. Initial adult and child dietary diversity data were collected in April to June 2015. A total of 203 pilot village households were enrolled, comprised of 64 households from Hautoho, 70 households from Saburai, and 69 households from Pairara. Ninety-seven percent of survey participants were mothers, 2 % grandmothers, and 1 % fathers. As the majority of participants were women of reproductive age (15–49 years), all adult dietary diversity data were analysed using the MDD-W (FAO and FHI 360 2016).
In all three villages, both adults (Fig. 2) and children (Fig. 3) had high rates of consumption of grains and starchy staples, and moderate to high consumption of dark green leafy vegetables and other vitamin A-rich fruits and vegetables. In the MDD-W, sugar-sweetened beverages such as diluted sweetened condensed milk and chocolate- or cereal-flavoured milk were not counted as dairy products due to the minimal dairy content. Amongst participating adults, there was no consumption of fresh or powdered milk, yoghurt or cheese. Using the IYCF-MDD, infant formulas were not included in the calculation of food groups, however other liquids with the main ingredient as fresh milk or milk powder were counted as part of the dairy food group. Among study participants, the only foods consumed containing milk powder were infant formulas, and as this was counted as ASF consumption and has been included in this representation of foods consumed (Fig. 3).

Food group consumption of participating mothers and carers aged between 17 and-58 years, based on a 24-h recall period. Data collected at baseline (April–June 2015, less-rainy season) using the Minimum Dietary Diversity for Women indicator (FAO and FHI 360 2016). Created using Microsoft Excel Version 1802

Food group consumption of children aged 6–24 months, based on a 24-h recall period. Data collected at baseline (April–June 2015, less-rainy season), using the Infants and Young Child Feeding Practices Minimum Dietary Diversity indicator (WHO 2010b). Created using Microsoft Excel Version 1802
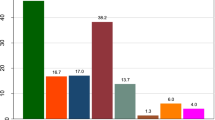
Quantitative baseline data from the dietary diversity dataset found stark differences in animal-source food consumption between villages, with 48% of mothers and carers in Pairara consuming ASF in the previous 24 h, compared to 6% in Hautoho (Fig. 4). More detailed exploration of ASF consumption (Fig. 5) shows that eggs are the most commonly consumed ASF amongst both adults and children. Fish is more commonly consumed in Pairara, and non-domesticated animal species were consumed in Pairara only.

Percentage of participating mothers and carers aged 17–58 years, and children aged 6–24 months consuming any animal-source food (ASF) at baseline (April – June 2015, less-rainy season). Data from dietary diversity study using a 24-h recall period. Child ASF consumption includes infant formulas containing milk powder. Created using Microsoft Excel Version 1802

Types of animal-source foods consumed by adults aged 17–58 years and children aged 6–24 months at baseline (April – June 2015, less-rainy season). Data from dietary diversity study using a 24-h recall period (n = 47–70). Data from each village are a similar colour; adults are represented in darker shades, while data from children are represented in lighter shades. Created using Microsoft Excel Version 1802
In examining the food consumption data from the 2013 Food and Nutrition Survey (MoH 2015) and the 2009–2010 DHS (NSD et al. 2010), the differences between the municipalities of Aileu, Bobonaro and Lautem were not as pronounced as the respective differences between Hautoho, Saburai and Pairara villages, sparking a focus in qualitative interviews and FG discussions to explore ASF consumption. Prominent themes that emerged from the qualitative study in the analysis of factors influencing the consumption of ASF were availability, access, sociocultural practices, and women’s decision-making power, as detailed below.
3.1 Availability of ASF
Of the key informant interviews and FG discussion participants asked about ASF consumption preferences, most stated that they like to eat all types of ASF and would consume more if they were available. One male participant from Saburai who stated that he does not eat meat because it makes him feel nauseous, indicated that he would eat fish. Chickens are the most abundant livestock species in Timor-Leste, and chicken meat the most commonly consumed ASF, therefore problems with the availability of their own chickens and eggs were discussed in depth.
For chickens, all discussion groups cited disease and predation as the major limiting factors for consumption. Due to ongoing losses, remaining chickens and eggs were reserved to allow the flock to perpetuate. When participants have few chickens, they are reserved for emergency use only, and regular consumption within the household does not occur - I want to eat my own chickens, but there are not enough chickens, (Hautoho, male FG, 2017). However, when there were more chickens, male and female participants mentioned that they give the eggs to the children to eat. In the dry season when chicks are more likely to be lost due to predation, or when there are a lot of eggs, adults also eat the eggs. If participants had a lot of chickens, they would eat chickens and eggs with much greater frequency - If the [wild] cat does not eat them, and the chickens are not dying, why not eat them? (Saburai, male FG, 2015) and If we have a lot of chickens, we can eat chicken and eggs whenever we feel like it, (Saburai, male FG, 2017). As chickens are valued household assets, participants prioritised sale over consumption, but explained that if they had enough chickens, they would sell some, eat some, and reserve some for ceremonies.
Fish was observed to be one of the most commonly consumed ASF in Pairara village, which is both closest to the coast and has the easiest terrain to traverse. In Pairara, fishermen or traders regularly come by motorbike to sell fresh fish in the village, or villagers can travel to coastal markets where fish is available. In Saburai village, fresh fish is sometimes available in the regional market about 1 hour away, and villagers require transport to be able to purchase, and in Hautoho, fresh fish is purchased from Dili, almost 2 hours away. Dried, salted fish is sometimes available in regional markets, while canned fish (mostly tuna and sardines) is usually available from kiosks within the villages. Fish ponds, where households raise their own fish in stand-alone or mixed farming systems, are not common in any of these three villages.
Undomesticated species are also an important source of ASF. Hunting was mentioned by both male and female participants, but is an activity undertaken by boys and men only. Participation in hunting was dependant on whether the activity was allowed in their village, whether the village was close to forested areas, and the motivation and skill of hunters. In Hautoho, local law (tara bandu) prohibits hunting, and most participants asked about hunting in this village stated that people there do not hunt. In contrast, hunting is permitted in Saburai and Pairara villages, and men were frequently observed on their way to or from the forest in both villages. In both villages, almost all participants who discussed hunting confirmed that people within the village hunt. In Pairara village, it was common for boys and men to hunt, and for children to walk through the streets of the village selling the carcasses.
For participants who said that people in their village hunt, or that people came to sell animals sourced from hunting in their village, the species of animal was determined (Table 5). Not only is hunting more common in Pairara, but a greater variety of undomesticated animals inhabiting the forested areas near this village were reported by participants.
3.2 Value of livestock and economic access to ASF
Livestock are often not functionally accessible to households for general consumption as they are reserved for sale or ceremonies – All of the community here keep many animals, but they cannot eat them because they get money from these animals, said one male FG participant in Saburai (2015). Another man summarised it as eating meat is like eating money, (Saburai, male FG, 2015). Because livestock are of high monetary value, participants would often prefer to reserve their own animals and purchase meat when they want to eat it: We just buy [frozen imported chicken] to eat. We will kill our own chickens during good times, like for cultural ceremonies - then we will kill and eat our own chickens. But normally, if we want to eat chicken meat, we buy [frozen imported chicken] from the market. We don’t just eat our own chickens any time (Saburai, male FG, 2017). It should be noted that the value of a local chicken (USD 5–12, June 2017) is much higher than the cost of frozen imported chicken (USD 3–3.50, June 2017), so it is possible for households to sell their own chicken and use some of the money for household needs and some to purchase frozen chicken for home consumption. Households would sell their chickens within their villages to households that required a chicken for a ceremony, or wealthier households that could afford to purchase the chicken for consumption. Chickens are also sold on the roadside or at regional markets to travellers passing through, or traders who transport the chickens to a larger town for sale.
Participants expressed that ASF is highly valued as food, but many people could not afford to consume it. The quotes below illustrate that participants feel that they would consume more ASF, including milk from ruminants, if they had more money or a higher status:
Rich people have a lot of money and they can buy good food like meat, fruit and whatever else they want to eat. They can buy meat like beef, wild boar, venison, pork and chicken. People who are poor eat bad food, only corn, yam and cassava. Sometimes people sell meat but it is very expensive and [poor people] cannot buy it because they do not have money. They want to eat this, but because they are poor, they do not have the money to buy it, (Pairara, female FG, 2015).
We only buy milk when we have a lot of money, or when we are sick. We do not have a lot of money to spend because our income is very small. However, when we are sick, we need good foods to improve our health, like meat, milk and fruit. We know that these foods are good for health, (Saburai, male FG, 2016).
Participants explained that they know these foods are good for their health because this is the information they get from doctors and nurses at the health posts and clinics.
Livestock are usually sold for a specific reason, such as to cover educational expenses, pay for ceremonies, or to purchase food items, with smaller species sold first: When there is less food, people sell chickens, goats, pigs, and buffalo to buy food to eat. First, they sell the chickens and buy food. When they do not have food again and have no more chickens, they also sell large animals, (Pairara, female FG, 2015). Staple foods are prioritised – when asked what foods people buy with the money after selling livestock, male and female participants most commonly listed rice, oil, sugar, salt and seasoning. After this, if money was left over, women said that they would buy other foods including ASF. If there were no money remaining, participants stated that they could just eat plain rice, plain rice with chili, or rice with the vegetables grown by the household. A common sentiment was that people like to eat ASF, and if they had money, they would purchase it more often, however, they are able to go to the market to buy ASF only if they had something to sell: We like meat, eggs and fish, but it depends on money. If we bring vegetables or something to sell in Dili, then we can buy meat, eggs and fish. In the rainy season, we can grow more vegetables, sell more, and buy more food. In the dry season, it depends on the production of mustard greens and Chinese cabbage and if we are hardworking, (Hautoho, female FG, 2017). Even to improve the diet of their children, households cannot always buy the recommended food. For food, we hear information from the doctor and health staff about what foods are good for children. But we don’t always follow this advice if we have no money, (Hautoho, female FG, 2017).
There is a difference between ASF from livestock slaughtered and consumed and that which is purchased, in that micronutrient-rich organ meats are always consumed when livestock are slaughtered at home, but rarely purchased. Through observations at market places, organ meats were sometimes available for purchase, however they were chopped, mixed and partially cooked to prevent malodour, and sold as small plated portions. Most participants stated that they like to eat organ meat and that it is tasty, but when discussing preferred parts of the animal to buy, participants invariably said that they only purchased meat, not the organs. Normally organs were not available to purchase, because the household who slaughtered the animal normally kept them for their own consumption, or they bought frozen imported chickens that only contained meat and bone. Participants explained that organs are available for purchase and are cheap, but they would buy them only if they had money left over after buying meat, and that they only purchased meat, because they do not have refrigeration to store organ meat.
Lastly, it is common for households to consume ASF when livestock become ill or die from unknown causes. In relation to the broader research question, this topic was discussed with respect to chickens that were ill or had died, but participants did mention that other animal species would be consumed if they died. What participants would do with sick or dead chickens was discussed in 18 FGs (including 10 female FGs). Of the 103 participants, most said that they would slaughter sick chickens for consumption or if a dead chicken still looked fresh and did not smell, it was consumed. Chickens that had died did not have the same flavour and were not as pleasant to eat as healthy chickens. However, it was seen as wasteful to throw the carcass away: We ate the dead chickens, but they were not tasty. We had kept the chickens until they were big already, so it didn’t feel good to throw them away, (Hautoho, male FG, 2017). When discussing the impact of the Newcastle disease vaccination program, one man stated that some people wait until the chicken has died and then they eat it; others kill and eat the chicken when it looks very sick. Now that the chickens are not dying, we don’t have to do this as much, (Saburai, male FG, 2016). One man (Saburai) stated that if one or two chickens die, they can just be thrown away, but if many chickens die, it is a waste if they do not eat them. Another man in the same group said that he never eats chickens that have died because disease can infect humans too. Participants who stated that they did not like to consume dead chickens said that they sometimes gave them to children to eat or to neighbours who like to eat chicken.
3.3 Sociocultural practices
In Timor-Leste, social custom, ceremonies, and rituals commonly intertwine with everyday life, although they vary by region and language group. They may be performed within households, or involve the wider community.
Ceremonies were the most commonly cited occasion for the consumption of ASF: they were mentioned in every discussion where ASF consumption was specifically asked about, and in three FGs in Saburai, participants noted that ceremonies were the only occasion when people consumed ASF. Social events and Christian ceremonies were celebrated in all three villages. Social occasions involving the consumption of ASF include birthday celebrations for children and adults, graduation from university, parties, New Year celebrations, or family members visiting from afar. Christian ceremonies include the Sacrament of Baptism (Sarani), Sacrament of Confirmation (Krizma), All Soul’s Day (Finadu), Christmas, and weddings. Funerals are always accompanied by ASF consumption, and ceremonies are a combination of Christian and animist rituals. Participants report there are no restrictions on the consumption of ASF for these events either generally or by age, gender, or socioeconomic status – depending on the purpose of the occasion, all members of the household or community are welcome to participate. In the ceremonies involving the whole community that were observed by the lead author, the food was placed on a communal table, and each person lines up to take a plate and to serve themselves the quantity of food they wished to eat. It is possible that ceremonies taking place within households may have a different method of food distribution.
While social and Christian ceremonies were common across the three villages, there was great variation between the villages as to the number of animistic ceremonies observed (Table 6), and the duration of these ceremonies. Participants from Hautoho, the village with the lowest level of ASF consumption, also listed the lowest number of ceremonies, and one informant and one FG stated that animistic ceremonies were not performed at all in their village.
Not all animistic ceremonies require animal sacrifices of chickens, pigs, goats or cattle; other offerings included eggs, maize, tobacco, and betel nut. Ceremonies involving the wider community involve killing and eating multiple animal species, while ceremonies within households more commonly use smaller livestock including chickens and their eggs. The traditional elder or cultural leader (lia nain) is the keeper of knowledge for these rituals, including advising on the appropriate location, time, words, process and roles of individuals. Where animal sacrifices are involved, the blood may not be available for consumption because of specific slaughter techniques or it may be used as part of the ritual, though the remainder of the carcass is available for consumption. Where chickens or eggs are used, they must only be from local breeds. Ceremonies using eggs may require the eggs to be left in sacred places such as under a revered tree or rock, placed in a symbolic location such as on a road, or opened onto a plate and examined.
When animistic ceremonies were cited as an opportunity for villagers to consume ASF, participants were asked what ceremonies were performed in their village that required an animal sacrifice. A number of different ceremonies were described, though ceremonies for members of the household who were ill was the most common in all three villages. Following these, rituals surrounding construction, especially that of sacred buildings such as traditional houses (uma lulik) or clan houses (uma lisan) were cited as the next most common. Table 6 shows the number of different ceremonies listed by participants from each village. A greater number of ceremonies are practised in Pairara, the village with the highest level of maternal ASF consumption, and based on observation, it was noted that there was a marked difference in the duration of ceremonies between villages. As an example, when there is a death in the village, animals are always sacrificed in honour of the person’s spirit – We always eat meat when people die – whether you like meat or not! (Pairara village, female FG, 2016). The traditional elder advises family members on the number of days the ceremony will take place, how many animals would be required, and which species should be brought by which family members. In Hautoho and Saburai villages, these ceremonies generally took place over 1–3 days, however in Pairara village, ceremonies were observed to last for a week or more. In the dry season, when there were more ceremonies, the periods of time in which households can consumed ASF may start to overlap or run consecutively, resulting in almost daily consumption.
Consumption of ASF at ceremonies may also be prescribed by rules. In Hautoho village, when a person dies, family members from the wife’s side can only consume ASF from cattle and goats, while family members from the husband’s side can consume ASF from pigs only. Guests at the ceremony who are not family members are able to consume any ASF. This differs from the cultural norm in Saburai, where any participants, family members or not, can consume any ASF at the ceremony.
Aside from social events and ceremonies, another common practice that enables community members to consume ASF is sharing amongst the local community. It is not uncommon for villagers to eat ASF because they have received it as a gift from extended family, friends, or neighbours.
3.4 Gender and ASF consumption
3.4.1 Food distribution
Women, generally the mother of children in the household, are responsible for meal planning and food preparation, with workload shared between the mother and teenage daughters: It is always the mothers who cook. Mothers decide what to eat each day. It is always the mothers that distribute food to the rest of the family, although the eldest daughter can also help if she is not at school (mother from Hautoho).
Most of the time, participants reported that the mother of the children in the household apportions food, so that everyone gets a fair share and there is enough food for everyone. One-third of participants said that all food is placed on the table and everyone in the household eats together, and a few participants said that the mother will plate food for the children but then food is placed on the table to eat together for adults. In general, men and women consider that food, including ASF, is distributed evenly within the household. One key informant from Pairara stated Now, here, there is no difference between males and females in how people eat food in the family compared to past times during colonialism, indicating a change in intra-household food allocation from times past. One mother from Hautoho said: It is the mother [of the children in the household] who decides how much food to put on each plate, but for all family members that are already adults, the amount of food must be equal. If one plate has more or less food, the person will shout that it is not equal. All adults should be equal. Another mother in Pairara explained: The mother always distributes food for each person in the household, people do not choose themselves. We do this because if they choose food for themselves, they may not finish all the food and they will waste it, or some people will eat more. We need to make sure everyone has enough to eat. Very few participants stated that it depends on the situation – if there are guests, they eat first with the men, then the women and children eat. Through repeated observation, this is the norm. However, it is not the case that women and children eat the food that is left over – before serving, the mother has already apportioned the food, ensuring that the dishes are equitably shared. Where there is a lot of food, each dish is placed on the table and each person serves themselves the amounts of staple food and side dishes as they would like. Where particular dishes are limited, portion sizes of similar appearance are distributed to each adult, and similar portions of side dishes are distributed to each child, although adults are apportioned more food than children. The amount of staple food given to each person may differ according to the size of the person. When asked if there were any ASFs that particular people could not eat, all participants stated that for general consumption, there were no restrictions on any particular ASF for any particular groups of people.
On occasion, it was observed that the staple served with the dishes was different. In these cases, rice was served to the men and guests, and women and children ate maize and beans instead. When asked why this was the case, mothers explained that guests preferred to eat rice, and that it was considered a higher status food. Although the rice was abundant, the women and children said that they preferred to eat maize sometimes if they have been eating rice a lot recently, because it is tasty, filling, and is their traditional food. Sometimes after the guests leave, men will also eat a bowl of maize.
Although the distribution of food within households is considered by participants to be equal, outside of the household there may be more opportunities for men to consume ASF than women. One FG in Pairara mentioned that only men ate meat during some ceremonies, and another mentioned that ceremonies for inaugurating clan houses (uma lisan) were solely for men – women and children were not allowed: For this ceremony, the women do not eat the meat, the men eat it. Female and male children also do not eat. Even an 80-year-old woman cannot eat the meat, because this is tradition. If a woman eats the meat, she can become sick or go crazy, (Pairara, female FG, 2016). This discussion group stated that this is the only ceremony observed in which women are not allowed to consume any ASF. There are no ceremonies in which only women can consume ASF. All ceremonies observed by the researcher involved both men and women, and there was no restriction on women’s consumption of ASF.
In Hautoho, men mentioned that about once a month, they will sit together, chat, drink alcohol and consume ASF. It is common for food to be consumed while drinking alcohol and ASF is preferred. However it is only accessible if the men have enough money to purchase it. The act of sitting together, drinking alcohol and consuming ASF was also only practised by men; women in Hautoho stated that women never sit together to eat ASF in the same way men do. Through observation, women’s social time sometimes involved tasks such as fetching water or weaving, and often accompanied by sharing of areca nut and betel leaf, but never alcohol and ASF.
3.4.2 Decision-making ability
Chickens are a small livestock species that can be owned by anyone in the household. For adults, the owner must play a role in decision-making, but for children, ownership is often nominal, given by parents to encourage children to take care of the chickens. From the focus groups, most participants asked about chicken care said that all members of the family look after the chickens, depending on who is available, and one-third said that only women look after the chickens. Through observation, women and children play a bigger role in caring for chickens, while men play a bigger role in caring for larger livestock species.
In deciding when to use these assets, it is rare for women in these three villages to be able to make autonomous decisions. Most male and female participants stated that the husband and wife must decide together whether chickens are sold or not. In Saburai, men and women stated that men can make the decision to sell chickens independently, but none stated that women can make the decision on their own. In Pairara, some men stated that women take care of the chickens, but men make the decision to sell. In both Hautoho and Pairara, men and women said that women can decide to sell chickens on their own if there is a need within the household. However Pairara was the only village where women said they can decide to sell chickens on their own for their own needs. One female participant in Pairara stated that we can sell piglets, goats and chickens – small animals. We decide to sell them ourselves and buy what we like with the money. More commonly, when husbands and wives decide together to sell livestock, they decide together what the money will be spent on. Furthermore, Pairara was the only village where women said that they are able to make the decision to slaughter a chicken for household consumption. These observations about the difference in women’s autonomy and agency between villages fits with some other observations: at the commencement of fieldwork, Pairara was the only village with a female in a prominent leadership position, until late in the course of fieldwork, when one woman was elected to a leadership position in Hautoho also. In the selection of field team members, the chief of village in Pairara was strongly supportive of gender balance, and two males and two females were recruited for the team, while in Saburai, initially, no females were deemed suitable for the role. One female (out of three) was later recruited when an original team member became ill.
In the discussions focusing on the reasons for chicken ownership, women seem to place greater importance on keeping chickens for consumption and for purchasing foods that increase dietary variety, while men emphasised the keeping of chickens for income generation or other purposes. Both men and women stated that they would use the money from selling chickens to buy household staples, such as rice, oil, salt, sugar and seasoning. Females more commonly stated that they would use the money to purchase different vegetables, ASF, and children’s school needs, while a larger proportion of men listed expenses such as ceremonies, alcohol, tobacco, cigarettes and business needs. In Saburai, men from one discussion group listed the following items they would purchase with money earned from selling chickens: We always buy tobacco, betel leaf and areca nut. Then we buy cigarettes. Then books, pens, shirts and pants. Then rice and oil. Then coffee and sugar. Lastly, we also use some for cultural ceremonies. In the same village, females stated that when they sell chickens, they would buy things for school like books, pens and clothes. Foods like rice, food from other people’s fields. Occasionally we buy fish or meat. We buy moisturiser and deodorant. We also buy betel leaf and areca nut, oil, salt, sugar and coffee. The sentiment that chicken ownership was only important for income generation was expressed most strongly by one man, who stated: If you have a chicken program, you need to work with people to buy chickens, otherwise you raise chickens just to die, or to eat! What’s the point - only eating the chicken, or to be able to sell it? (Pairara, male FG, 2017). In his opinion, a program to improve chicken production would only be successful if you could sell the chickens; raising chickens for consumption was not a valued end-point.
4 Discussion
This study finds a number of interacting and competing factors affecting household consumption of ASF. The most important constraints are low numbers of small livestock species, limited household income, and low decision-making ability of women, leading to decreased prioritisation of household nutrition.
For these rural villages, no food proscriptions or prescriptions specific to everyday consumption of ASF were identified, and participants in this study indicated that they would like to consume more ASF. Thus, increasing the numbers of healthy livestock may be a way to provide a stable source of ASF to households, but livestock ownership does not necessarily increase ASF intake. Consistent with the findings of AMSAT International (2011), large livestock species are kept more for status, savings and ceremonies, while small livestock species are more likely to be sold for households needs including food or consumed at home. This is a similar finding to Azzarri et al. (2015), who reported that in Uganda, poultry ownership increased household chicken consumption, however, goat and sheep ownership did not increase goat and sheep meat consumption, and that cattle ownership did not increase beef consumption but was associated with increased milk consumption. In Timor-Leste, fresh milk is not often consumed, so although the occasional sale of large livestock (cattle and buffalo) is an important income source for some households, ownership of large livestock species cannot be considered to contribute regularly to household nutrition. In small livestock, including poultry and goats, disease and predation are major limitations to production, and small flock or herd sizes decrease the likelihood that households would utilise their own livestock. These are important considerations for nutrition-sensitive agricultural programs, which should be aimed at improving health and husbandry, and targeted more towards preferred smaller livestock species such as chickens and pigs.
The species of livestock supported is also important from a gender perspective. From these results, it is possible for women in Timor-Leste to own and make autonomous decisions about small livestock species. However, this is not common. When women are able to decide what to buy, their income is more likely to be spent on improving dietary diversity, and livestock under the control of women are more likely to be used for household consumption than sale. These findings are similar in other parts of the world - in Kenya, Jin and Ianotti (2014) found that when livestock are owned by women, there are positive impacts on nutrition and child growth; the same impacts are not found when livestock are owned by men, as a greater percentage of resources under the control of women are used to improve household nutrition and health compared to resources controlled by men. Although in demographic and health surveys, women are considered empowered if they participate in any decision-making, joint or autonomous, a mixed-methods report from Mercy Corps (Scantlan and Previdelli 2013) suggests that women may take a more subservient role during joint decision-making, increasing the importance of autonomous decision-making for women in Timor-Leste.
There is a large body of evidence showing the importance of women’s empowerment in agriculture to achieve better dietary outcomes for households (Malapit and Quisumbing 2014; Ruel et al. 2013; van den Bold et al. 2013), although studies examining the relationships between women’s empowerment and child nutritional status have produced mixed results (Cunningham et al. 2015a). Smith et al. (2002) found that women’s relative household decision-making power had a strongly positive effect on child WHZ and HAZ in South Asia and Sub-Saharan Africa, but a positive effect on child WHZ only in Latin America and the Caribbean. In South Asia, financial autonomy has both been positively (Shroff et al. 2009) and not significantly (Shroff et al. 2011) associated with stunting in Andhra Pradesh, India, while in Nepal, a positive association was found between maternal decision-making power in daily household purchases and child WHZ, but the association was negative with large household purchasing decisions. Using the Women’s Empowerment in Agriculture Index (WEAI)’s Five Domains of Empowerment (5DE), Cunningham et al. (2015b) found that child HAZ was significantly associated with overall women’s empowerment. However they found no significant associations between child HAZ and major household asset ownership, or the ability to purchase, sell or transfer productive assets. These findings contrast with that in South-East Asia, where asset ownership by mothers was found to be significantly and positively associated with child HAZ and WHZ in Papua New Guina (van der Meulen Rodgers and Kassens 2018). These mixed results suggest that the relationship between women’s empowerment and child nutrition outcomes are complex, with environmental and cultural influences likely affecting the significance of different domains of women’s empowerment.
These findings still strongly support national policies and programs that address women’s empowerment. In agriculture, as women are more likely to utilise their livestock for household consumption or mobilise their assets to support household nutrition, they should be given the same access to programs, extension services, information, and technologies as men, enabling them to produce livestock more efficiently (Tesfaye et al. 2015). Programs promoting the production of livestock under the control of women, particularly when extensive and semi-intensive production systems are employed, have the potential to make great contributions to household nutrition and improve women’s status without considerably increasing their workload. In Mozambique, participation in a Newcastle disease vaccination program allowed women to sell 4–5 chickens and buy a goat, with the ultimate aim of selling some goats to buy cattle, increasing their economic autonomy as well as self-esteem and confidence (Bagnol 2001). These programs should be integrated with nutrition behaviour change for greater impact on child nutrition (Olney et al. 2015).
Economic constraints were raised by participants as a major barrier to ASF consumption. It is well known that as household income increases, utilisation of livestock as ASF increases (Delgado 2003), and this is demonstrated in this study. Poorer households value ASF and produce livestock, but need to sell the livestock for income, while wealthier households, including households that do not produce livestock, value ASF and can afford to consume or purchase it. Programs or policies aimed at improving economic opportunities would benefit any households living at or below the poverty line. For policies and programs specifically aiming to improve household nutrition through enhanced income generation, it is important for the policy environment to be supportive, and for nutrition behaviour change and communication to be incorporated (Lamstein et al. 2014), as nutrient-dense foods including ASF are more expensive, while fat- and sugar-rich processed foods are cheap, tasty, and readily available at many small kiosks in rural villages in Timor-Leste.
Although increased ASF consumption is nutritionally beneficial, the risks of poor food safety, emerging infectious diseases and loss of biodiversity also need to be considered (Golden et al. 2011; Jones et al. 2008). Carcasses of animals that have died from undiagnosed illnesses are consumed out of necessity when people have scarce resources. This increases the risk of zoonoses such as highly pathogenic avian influenza (Alders et al. 2013). Non-domesticated animals can contribute significantly to diets, but the encroachment of human activity into wild areas increases the risk of emerging infectious diseases and puts pressure on wild populations. When loss through hunting exceeds a critical point, wild animal populations are no longer sustainable, resulting in threatened local food security and loss of global biodiversity (Golden et al. 2011). In Madagascar, non-domesticated animals were found to be important contributors to nutrition. However, there is current support for the production of indigenous chickens to decrease the reliance on wild food sources (Borgenson et al. 2017). Supporting household livestock production may decrease these risks to human health and biodiversity.
Much of the literature from Timor-Leste and these results indicate that ceremonies and social events are the most common time for people to consume ASF. The findings from the present study in Aileu, Bobonaro and Lautem municipalities is comparable to the findings of a larger study by AMSAT International (2011), which found that 89% of their study participants (adult females, lay people, or from poor families) from Baucau, Bobonaro and Covalima municipalities ate ASF at traditional ceremonies, compared to 29% of participants consuming ASF every day. In addition to fulfilling social and cultural duties, animal sacrifice at community-level events may be a way for households to display socioeconomic status, and to reduce inequality by distributing wealth in the form of ASF (Castro 2013). Additionally, the sharing of ASF among households, whether associated with a ceremony or not, may be due to limited storage options for ASF in villages, but is also a way for households to reinforce social networks and build social capital (Hastorf 2017). However, there are vast differences among different municipalities within Timor-Leste in the frequency and length of ceremonies. This study finds that in villages where there are many observed ceremonies of long duration, the overlapping of ceremonies increases the frequency of ASF consumption to the level where it may be significant enough to contribute to improved nutritional status, although this effect may be seasonal. In other villages, ceremonies and social events occur too sporadically to contribute to nutrition, and in the face of low livestock numbers, may inhibit everyday consumption as livestock are reserved rather than utilised.
In regard to ASF distribution, this study finds that men may participate in a greater number of social or ceremonial events involving ASF consumption outside the household compared to women, but within the household, no evidence of “channelling” ASF to male household members was found. There are a few limitations in the interpretation of this finding: firstly, this study did not quantitatively measure ASF consumption in either men or women; secondly, the distribution of ASF was only observed by the lead author in households during times of sufficient food – intra-household food allocation patterns may change at times of food shortage; and thirdly, participants may not feel comfortable reporting preferential treatment given to any specific household members or biases in food distribution may occur without a conscious decision-making process. Despite these limitations, these findings are similar to that of AMSAT International (2011) on household fish consumption, where only a small proportion of participants stated that older members (4%) or household heads (3%) receive a larger portion of fish, or that women get a smaller portion (2%). These findings are in contrast to findings in Nepal: Gittelsohn (1991) found that high status foods were channelled to men and children, placing women at a nutritional disadvantage, and Harris-Fry et al. (2018) found that 43% of household heads consumed flesh foods compared to 33% of pregnant women and mothers-in-law, while common foods including starchy foods, pulses and vegetables were more equitably shared. In other parts of South Asia, a number of determinants were found to influence intra-household food allocation, including household wealth, where higher socioeconomic households may channel preferred foods including ASF to high status household members (Harris-Fry et al. 2017). This review also found that women are likely to be at higher risk of unfavourable intra-household food distribution at times of food insecurity.
In summary, this study found a number of factors influencing the consumption of ASF in rural villages in Timor-Leste. Factors with a positive influence on ASF consumption included: observing a large number of ceremonies - particularly those of longer duration - where consuming ASF is part of the ritual; having available income to enable the purchase of ASF; having greater numbers of livestock, in particular smaller livestock species that are more likely to be slaughtered and consumed; living close to forested areas with wild animal populations, and women having greater control over resources and a greater role in household decision-making. Barriers to ASF consumption include having low income or limited income streams, high levels of small livestock morbidity and mortality leading to small or unstable flock or herd sizes, reserving livestock for sale and ceremonies, living far from forested areas or where hunting is not allowed. The extent of these contributing factors varied between the three study villages, helping to explain why the level of ASF consumption is higher in Pairara than Hautoho.
The benefits of ASF consumption particularly for undernourished women and children are clear – the question is, how do we sustainably improve availability, access and utilisation of ASF? From these findings, policies and programs aimed at improving the health and production of small livestock species that are more likely to be utilised by the household and more likely to be under the control of women, are more likely to be effective and sustainable in improving the nutritional status of households.
References
Administrative Committee on Coordination (ACC)/Sub-Committee on Nutrition (SCN). (2000). Fourth report on the world nutrition situation. Geneva: ACC/SCN in collaboration with International Food Policy Research Institute.
Alders, R. G., & Pym, R. A. E. (2009). Village poultry: still important to millions, eight thousand years after domestication. World's Poultry Science Journal, 65(2), 181–190.
Alders, R., & Spradbrow, P. (2001). Controlling Newcastle disease in village chickens: A field manual. Canberra: Australian Centre for International Agricultural Research.
Alders, R., Awuni, J., Bagnol, B., Farrell, P., & de Haan, N. (2013). Impact of avian influenza on village poultry production globally. Eco Health. https://doi.org/10.1007/s10393-013-0867-x.
AMSAT International. (2011) Fish and animal protein consumption and availability in Timor-Leste. Regional Fisheries Livelihoods Programme for South and Southeast Asia (GCP/RAS/237/SPA). Field Project Document 2011/TIM/02.
Andersen, A.B., Pant, J., Thilsted, S.H. (2013). Food and nutrition security in Timor-Leste. CGIAR Research Program on Aquatic Agricultural Systems. Penang, Malaysia. Project Report: AAS-2013-29.
Azzarri, C., Zezza, A., Haile, B., & Cross, E. (2015). Does livestock ownership affect animal source foods consumption and child nutritional status? The Journal of Development Studies, 51(8), 1034–1059.
Bagnol, B. (2001). The social impact of Newcastle disease control. ACIAR Newsletter, March, 69–75. http://aciar.gov.au/files/node/2131/pr103chapter16.pdf. Accessed 11 March 2018.
Bagnol, B. (2014). Timor-Leste Village poultry health and biosecurity program, the University of Sydney technical support, mission from 7 to 29 august 2014. Dili: The Village Poultry Health and Biosecurity Programme (VPHB).
Bettencourt, E. M. V., Tilman, M., Narciso, V., da Silva Carvalho, M. L., & de Sousa Henriques, P. D. (2015). The livestock roles in the wellbeing of rural communities of Timor-Leste. Revista de Economia e Sociologia Rural, 53, 63–80. https://doi.org/10.1590/1234-56781806-94790053s01005.
Blanton, C. A., Moshfegh, A. J., Baer, D. J., & Kretsch, M. J. (2006). The USDA automated multiple-pass method accurately estimates group total energy and nutrient intake. The Journal of Nutrition, 136(10), 2594–2599.
Borgenson, C., Rajaona, D., Razafindrapaoly, B. N., Rasolofoniaina, B. J. R., Kremen, C., & Golden, C. (2017). Links between food insecurity and the unsustainable hunting of wildlife in a UNESCO world heritage site in Madagascar [abstract]. The Lancet, 389(S3), 3.
Brown, K. H. (1991). The importance of dietary quality versus quantity for weanlings in less developed countries: a framework for discussion. Food and Nutrition Bulletin, 13(2).
Calloway, D. H., Murphy, S., Balderston, J., Receveur, O., Lein, D., & Hudes, M. (1992). Village nutrition in Egypt, Kenya and Mexico: Looking across the CRSP projects. Berkeley: University of California.
Cardinoza, M. (2005). Reviving traditional NRM regulations (Tara Bundu) as a community-based approach of protecting carbon stocks and securing livelihoods. In D. Murdiyarso & H. Herwati (Eds.), Proceedings of work-shop on carbon sequestration and sustainable livelihoods (pp. 197–210). Bogor: CIFOR.
Castro, A. (2013). An approach to the food habits of three communities in Timor-Leste. Final report. Dili: CARE International Timor-Leste.
Conceição, F. (2012) Major Findings of Active Diseases Surveillance on Priority Animal Diseases of Timor-Leste. Communication presented at the final project workshop. Dili: Timor-Leste: Ministry of Agriculture and Fisheries.
Cunningham, K., Ruel, M., Ferguson, E., & Uauy, R. (2015a). Women's empowerment and child nutritional status in South Asia: a synthesis of the literature. Maternal & Child Nutrition, 11, 1–19.
Cunningham, K., Ploubidis, G. B., Menon, P., Ruel, M., Kadiyala, S., Uauy, R., & Ferguson, E. (2015b). Women’s empowerment in agriculture and child nutritional status in rural Nepal. Public Health Nutrition, 18, 3134–3145.
Darapheak, C., Takano, T., Kizuki, M., Nakamura, K., & Seino, K. (2013). Consumption of animal source foods and dietary diversity reduce stunting in children in Cambodia. International Archives of Medicine, 6, 29. https://doi.org/10.1186/1755-7682-6-29.
Davies, G., & Casey, A. (1973). The survival of Brucella Abortus in milk and milk products. British Veterinary Journal, 129(4), 345–353.
de Bruyn, J., Wong, J., Bagnol, B., Pengelly, B., & Alders, R. (2015). Family poultry production and food and nutrition security. CAB Reviews, 10(13), 1–9.
DeBoer, M., Lima, A., Oría, R., Scharf, R., Moore, S., Luna, M., & Guerrant, R. (2012). Early childhood growth failure and the developmental origins of adult disease: do enteric infections and malnutrition increase risk for the metabolic syndrome? Nutrition Reviews, 70(11), 642–653.
Delgado, C. (2003). Rising consumption of meat and milk in developing countries has created a new food revolution. Journal of Nutrition, 133(11), 3907S–3910S.
Demment, M. W., Young, M. M., & Sensenig, R. L. (2003). Providing micronutrients through food-based solutions: a key to human and national development. Journal of Nutrition, 133(11), 3879S–3885S.
FAO and FHI 360. (2016). Minimum dietary diversity for women: A guide for measurement. Rome: Food and Agricultural Organization.
Gale, N. K., Heath, G., Cameron, E., Rashid, S., & Redwood, S. (2013). Using the framework method for the analysis of the qualitative data in multi-disciplinary health research. BMC Medical Research Methodology, 13, 117.
Gittelsohn, J. (1991). Opening the box: intrahousehold food allocation in rural Nepal. Social Science and Medicine, 33(10), 1141–1154.
Golden, C. D., Fernald, L. C. H., Brashares, J. S., Rasolofoniaina, B. J. R., & Kremen, C. (2011). Benefits of wildlife consumption to child nutrition in a biodiversity hotspot. Proceedings of the National Academy of Sciences, 108, 19653–19656. https://doi.org/10.1073/pnas.1112586108.
Guèye, E. (2000). The role of family poultry in poverty alleviation, food security and the promotion of gender equality in rural Africa. Outlook on Agriculture, 29(2), 129–136.
Harris-Fry, H., Shrestha, N., Costello, A., & Saville, N. M. (2017). Determinants of intra-household food allocation between adults in South Asia – a systematic review. International Journal for Equity in Health, 16, 107. https://doi.org/10.1186/s12939-017-0603-1.
Harris-Fry, H., Paudel, P., Shrestha, N., Harrison, T., Beard, J., Jha, S., Shrestha, B., … Saville, N. M. (2018). Status and determinants of intra-household food allocation in rural Nepal. European Journal of Clinical Nutrition. https://doi.org/10.1038/s41430-017-0063-0.
Hastorf, C. A. (2017). The gift of food. In: The social archaeology of food: thinking about eating from prehistory to the present (pp. 27–29). New York: Cambridge University Press.
Ianotti, L., Lutter, C., Stewart, C., Riofío, C., Malo, C., Reinhart, G., et al. (2017). Eggs in early complementary feeding and child growth: a randomized controlled trial. Pediatrics, 140, e20163459. https://doi.org/10.1542/peds.2016-3459.
Jin, M., & Ianotti, L. (2014). Livestock production, animal source food intake, and young child growth: the role of gender for ensuring nutrition impacts. Social Science & Medicine, 105, 16–21. https://doi.org/10.1016/j.socscimed.2014.01.001.
Jones, K., Patel, N., Levy, M., Storeygard, A., Balk, D., Gittleman, J., & Daszak, P. (2008). Global trends in emerging infectious diseases. Nature, 451, 990–993. https://doi.org/10.1038/nature06536.
Jong, J. (2016). Scavenging for protein and micronutrients: village poultry in Timor-Leste. Proceedings of the Crawford Fund 2016 Annual Conference. https://www.crawfordfund.org/wp-content/uploads/2017/04/CF-2016-Conference-Proceedings-Jong.pdf. Accessed 29 January 2018.
Lamstein, S., Stillman, T., Koniz-Booher, P., Aakesson, A., Collaiezzi, B., Williams, T., et al. (2014). Evidence of effective approaches to social and behavior change communication for preventing and reducing stunting and anemia: Report from a systematic literature review. Arlington: USAID/Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) Project.
Land O’Lakes. (2010). Building agribusiness capacity in East Timor. Quarterly report April–June 2010. USAID. https://pdf.usaid.gov/pdf_docs/Pdact222.pdf. Accessed 24 March 2018.
Malapit, H. J. L., & Quisumbing, A. R. (2014). What dimensions of women’s empowerment in agriculture matter for nutrition in Ghana? Food Policy, 52, 54–63. https://doi.org/10.1016/j.foodpol.2015.02.003.
McWilliam, A. (2001). Prospects for sacred groves: Valuing lulic forests on Timor. The Asia Pacific Journal of Anthropology, 2, 89–113.
Melesse, A. (2014). Significance of scavenging chicken production in the rural community of Africa for enhanced food security. World's Poultry Science Journal, 70(3), 593–606.
Ministry of Health (MoH). (2015) Timor-Leste Food and Nutrition Survey 2013. Final report 2015. Southeast Asian Ministers of Education Organization Regional Centre for Food and Nutrition. Dili: Timor-Leste Ministry of Health.
Mtileni, B. J., Muchadeyi, F. C., Maiwashe, A., Phitsane, P. M., Halimani, T. E., Chimonyo, M., & Dzama, K. (2009). Characterisation of production systems for indigenous chicken genetic resources of South Africa. Applied Animal Husbandry & Rural Development, 2, 18–22.
Murphy, S. P., & Allen, L. H. (2003). Nutritional importance of animal source foods. Journal of Nutrition, 133(11 Suppl 2), 3932S–3935S.
National Statistics Directorate (NSD), Ministry of Finance, ICF Macro. (2010). Timor-Leste demographic and health survey 2009–10. Dili: NSD and ICF Macro.
Neumann, C. G., Harris, D. M., & Rogers, L. M. (2002). Contribution of animal source foods in improving diet quality and function in children in the developing world. Nutrition Research, 22, 193–220.
OIE. (2016). Timor-Leste country information. World Animal Health Information Database (WAHIS Interface). http://www.oie.int/wahis_2/public/wahid.php/Countryinformation/Animalsituation. Accessed 22 March 2018.
Olney, D. K., Pedehombga, A., Ruel, M. T., & Dillon, A. (2015). A 2-year integrated agriculture and nutrition and health behaviour change communication program targeted to women in Burkina Faso reduces anemia, wasting, and diarrhea in children 3-12.9 months of age at baseline: a cluster-randomized controlled trial. The Journal of Nutrition, 145, 1317–1324. https://doi.org/10.3945/jn.114.203539.
República Democrática de Timor-Leste (RDTL). (2016a). National food and nutrition security policy. Dili: Government of Timor-Leste.
República Democrática de Timor-Leste (RDTL). (2016b) Timor-Leste population and housing census 2015. Suco tables – Volume 4 (agriculture: Type of livestock reared). Dili: Government of Timor-Leste.
República Democrática de Timor-Leste (RDTL). (2016c) Timor-Leste Population and housing census 2015. Suco tables – Volume 2 (Population by age and sex). Dili: Government of Timor-Leste.
República Democrática de Timor-Leste (RDTL). (2016d) Timor-Leste Population and housing census 2015. Suco tables – Volume 2 (Population and household distribution). Dili: Government of Timor-Leste.
Ruel, M. T., Alderman, H., & the Maternal and Child Nutrition Study Group. (2013). Nutrition-sensitive interventions and programmes: how can they help to accelerate progress in improving maternal and child nutrition? The Lancet, 382, 536–551. https://doi.org/10.1016/S0140-6736(13)60843-0.
Sankhyan, V., Katoch, S., Thakur, Y. P., Dinesh, K., Patial, S., & Bardwaj, N. (2013). Analysis of characteristics and improvement strategies of rural poultry farming in north western Himalayan state of Himachal Pradesh, India. Livestock Research for Rural Development, 25(12).
Scantlan, J., & Previdelli, A. (2013). Women’s empowerment and childhood malnutrition in Timor-Leste: a mixed-methods study. Portland: Mercy Corps.
Schönfeldt, H. C., Pretorius, B., & Hall, N. (2013). The impact of animal source food products on human nutrition and health. South African Journal of Animal Science, 41(3), 394–412.
Shroff, M., Griffiths, P., Adair, L., Suchindran, C., & Bentley, M. (2009). Maternal autonomy is inversely related to child stunting in Andhra Pradesh, India. Maternal & Child Nutrition, 5(1), 64–74.
Shroff, M. R., Griffiths, P. L., Suchindran, C., Nagalla, B., Vazir, S., & Bentley, M. E. (2011). Does maternal autonomy influence feeding practices and infant growth in rural India? Social Science and Medicine, 73(3), 447–455.
Smith, L. C., Ramakrishnan, U., Ndiaye, A., Haddad, L., Martorell, R. (2002). The importance of women’s status for child nutrition in developing countries. Research report 131. Washington, DC: International food policy research institute and Department of International Health, Emory University.
Tesfaye, A., Zelalem, A. Y., Alebachew, M., Shiferaw, W., Leweye, A., Tsegaye, M., & Mebratu, M. (2015). Access of rural women to agricultural extension services, opportunities and challenges in Ethiopia. Addis Ababa: Women and Youth Affairs Directorate of Ministry of Agriculture and Agricultural Transformation Agency.
Traube, E. (1980). Mambai rituals of black and white. In J. Fox (Ed.), The flow of life: Essays on eastern Indonesia (pp. 290–315). MA: Harvard University Press.
United Nations Mission in Timor-Leste (UNMIT) Geographical Information Systems (GIS) Unit. (2007). Timor-Leste administrative boundaries [map]. 1:300,000. Dili: UNMIT GIS Unit, 16 May 2007.
van den Bold, M., Quisumbing, A. R., Gillespie, S. (2013). Women’s empowerment and nutrition. An evidence review. IFPRI Discussion Paper 01294. Washington, DC: International Food Policy Research Institute.
van der Meulen Rodgers, Y., & Kassens, A. L. (2018). Women's asset ownership and children's nutritional status: evidence from Papua New Guinea. Social Science & Medicine, 204, 100–107. https://doi.org/10.1016/j.socscimed.2018.03.026.
Waldron, S., de Paulo Correia, V., Mulik, M., de Rego, A., da Costa Varela, C., Fordyce, G., ... & van de Fliert, E. (2016). Sub-sector analysis of the Timor Leste beef industry, report for ACIAR project LPS-2009-036 enhancing smallholder beef production in Timor Leste. Canberra, ACT: Australian Centre for International Agricultural Research.
WHO. (2008). Indicators for assessing infant and young child feeding practices: Conclusion of a consensus meeting held 6–8 November 2007 in Washington D.C., USA. Part 1: Definitions. Geneva: World Health Organization.
WHO. (2009). Session 3: Complementary feeding. Infant and young child feeding: Model chapter for textbooks for medical students and allied health professionals. Geneva: World Health Organization. https://www.ncbi.nlm.nih.gov/books/NBK148957/ Accessed 24 March 2018.
WHO. (2010a). Nutrition landscape information system (NLIS) country profile indicators: Interpretation guide. Geneva: World Health Organization.
WHO. (2010b). Indicators for assessing infant and young child feeding practices. Part 2: Measurement. Geneva: World Health Organization.
Wong, J.T., Bagnol, B., Grieve, H., Li, M. and Alders, R. 2016. Drivers behind seasonal changes in household animal-source food consumption in Timor-Leste. Poster presented at the Conference on Agri-Health Research at ANH Academy Week, Addis Ababa, 20–24 June 2016.
Wong, J. T., de Bruyn, J., Bagnol, B., Grieved, H., Li, M., Pym, R., & Alders, R. G. (2017). Small-scale poultry and food security in resource-poor settings: A review. Global Food Security, 15, 43–52. https://doi.org/10.1016/j.gfs.2017.04.003.
Acknowledgements
This research would not have been possible without Mario Moreira dos Reis from the Nutrition Department in the Timor-Leste Ministry of Health, field assistant and interpreter Ananias Frederico Benevides from the Livestock and Veterinary Directorate in the Ministry of Agriculture and Fisheries, the communities in Timor-Leste that accommodated us, and the respondents who kindly offered much of their time and knowledge by participating in research activities. The authors would like to acknowledge the Government of Australia and The University of Sydney for their financial support of this research, as well as the Government of Timor-Leste for their technical and practical support.
Funding
This research was funded by The University of Sydney and the Government of Australia.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This research project was approved by the Timor-Leste Ministries of Agriculture and Fisheries, and Health, and received ethical approval through The University of Sydney for both Human Ethics (Project number 2014/815) and Animal Ethics (Project number 2014/705). The research was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments.
Statement of informed consent
Informed consent was obtained from all individual participants included in the study. Study aims, activities, and the voluntary nature of participation were explained to each potential participant prior to enrolment into the study at baseline. Each participant then gave their signature or a thumb-print if illiterate to indicate consent prior to each round of data collection.
Rights and permissions
About this article

Cite this article
Wong, J.T., Bagnol, B., Grieve, H. et al. Factors influencing animal-source food consumption in Timor-Leste. Food Sec. 10, 741–762 (2018). https://doi.org/10.1007/s12571-018-0804-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12571-018-0804-5