
Abstract
We report an extremely rare case of a pancake kidney with a single ureter. During the medicolegal autopsy on the body of a traffic accident victim, the kidneys were not located in the abdomen. The anterior surfaces of both kidneys were completely fused in the pelvic cavity, and the kidney was shaped like a pancake. This pancake kidney had accessory renal arteries around it and one renal vein from each kidney. The left renal vein was much smaller in diameter than the right one. There were two major calyces, one each from each kidney. The major calyces joined to form a single renal pelvis from both the kidneys, which continued as a single ureter. The renal pelvis and ureter lay posterior to the pancake kidney. Urologists and pelvic surgeons should be aware of the variant anatomy of the pancake kidney, particularly concerning its vasculature, to prevent unexpected catastrophic bleeding. If the kidneys are not located in the abdominal cavity, the autopsy surgeon must consider the possibility of its presence in the pelvic cavity. This could be especially important during medicolegal investigations into allegations of missing kidneys and unlawful kidney transplantations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The fetal kidneys appear as buds near the urinary bladder. Later in intrauterine life, the kidneys move superiorly to become lumbar in position and retroperitoneal. On rare occasions, one kidney from either the right or left side fails to ascend and remains in the pelvis as a ‘pelvic kidney.’ Bilateral pelvic kidney is an extremely rare variant; usually both kidneys are found on the same side (Russell et al. 2000). Hence, pelvic kidneys can be uni- or bilateral. The fusion of either the upper or lower pole of the kidney leads to a more common variant known as the ‘horseshoe kidney.’ The ‘pancake kidney’ differs from the ‘horseshoe kidney’ in that it shows fusion of the kidneys at both the upper and lower poles.
The ‘pancake kidney’ is a congenital anomaly that exhibits fused pelvic kidneys. In this rare anomaly, there is extensive fusion of the superior and inferior poles of both kidneys across the entire medial aspect, looking like a pancake or disc (Martínez-Lázaro and Cortés-Blanco 2000). The incidence of ‘pancake kidney’ is not available in the literature. However, the prevalence rate of ‘pelvic kidney’ has been reported to be 0.03–0.05 % cases (Cinman et al. 2007).
The pancake kidney has several other names, such as the cake, disc, doughnut and shield kidney, because it produces a ring- or doughnut-shaped mass. The renal pelvis is tilted anteriorly, and the ureters are not crossed. The collecting parts of the kidneys remain separate, and there is no communication with the contralateral side (Glenn 1958; Tiwari et al. 2014). The pancake kidney still has right and left ureters, which reach the urinary bladder through separate openings (Martínez-Lázaro and Cortés-Blanco 2000). In the present study, we report a rare variant of pancake kidney in which there were two major calyces, one from each kidney, which joined together to form a single common ureter. The renal pelvises and ureter were located posterior to this fused pelvic pancake kidney.
Case report
A 23-year-old male was riding a bike when hit by a bus from behind. He had multiple injuries all over his body and expired on the way to hospital. A medicolegal autopsy was conducted to determine the exact cause of death. The autopsy revealed serious injuries in the thoracic region, including hemothorax, and the pleural cavity contained 100 and 250 ml of blood-mixed fluid on right and left side, respectively. All the ribs on the left side were fractured along the anterior axillary and paravertebral lines. Multiple contusions and lacerations were evident on the lower lobe of the left lung. There were no apparent injuries to the abdominal viscera. Blunt trauma to the chest due to the traffic accident was given as the cause of death.
During the examination of the abdomen, both the right and left kidneys were not found in their usual location. However, during the examination of the pelvic viscera, a pancake-shaped structure (Fig. 1) was observed in the right pelvic cavity. This structure was removed and carefully examined macroscopically, allowing the diagnosis of pelvic fused kidney. Other pelvic organs, such as the urinary bladder, course of the ureter, ureteric orifice and trigone of the urinary bladder, could not be examined in detail. Limitations of the aforementioned observations are attributed to the time limitation since it was an incidental autopsy observation during a medicolegal procedure.

The anterior surface of the pelvic fused kidney, which resembled a pancake (1 accessory renal arteries; 2 renal vein)
The kidney was fixed in 10 % formalin solution and further examined after about a week. Examination revealed a fused kidney with fusion of the kidneys apparent at both the upper and lower poles (Fig. 1). The anterior surfaces of both kidneys were completely fused, and the fusion looked like a pancake (Fig. 1). The fused kidney weighed 150 g. The transverse diameters of the fused kidney at its anterior and posterior surfaces were 116 and 106 mm, respectively. The vertical diameter of the fused kidney measured 72 mm. The transverse diameters of the right and left kidneys were 44 and 49 mm, respectively. The vertical diameters were 70 and 81 mm for the right and left kidneys, respectively.
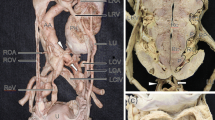
After careful dissection, the posterior surface of the fused kidney was found to exhibit the hilum of the kidneys (Fig. 2). The right kidney was obliquely placed and the left one vertically in that fusion (Fig. 2). There were two major calyces, one each from the right and left kidneys, which joined to form a single renal pelvis, which continued as a common single ureter (Fig. 2). The renal pelvis and ureter were posteriorly related to this pancake kidney. Each kidney had a separate renal vein; the left renal vein had a longer length than the right one. However, the left vein had a much smaller diameter than the right one. The macroscopic examination also revealed multiple renal arteries present around the fused pancake-shaped kidney (Fig. 1). The origin of the renal arteries and drainage of the renal veins could not be established because of the limited time available since this was an incidental autopsy observation during a medicolegal postmortem examination. However, the arteries probably originated from the internal iliac artery, with the veins draining into the internal iliac vein, because the pancake kidney was found inside the pelvic cavity. No congenital anomalies were observed in any of the patient's other organs, including the heart and lungs. The vertebral column and genital organs were also normal.

Posterior surface of the pancake kidney (pelvic fused kidney), exhibiting the hilum of both kidneys. There was fusion at both the superior and inferior poles of the medial border of the kidneys (1 right kidney; 2 left kidney; 3 right major calyx; 4 left major calyx; 5 common renal pelvis from both the kidneys; 6 right renal vein; 7 left renal vein; 8 accessory renal arteries; 9 single ureter of the pancake kidney)
Discussion
Ectopic kidney is a congenital anomaly in which the kidney is located inferiorly, superiorly or on the opposite side from its normal topography. An ectopic kidney is seen in 0.1 % of cases (Bauer 2007). The autopsy examinations reported a slightly higher incidence of ectopic kidneys (0.25 %), and in 85 % of cases, the kidneys were fused (Shoemaker and Braasch 1939). The most common type of ectopic kidney is the horseshoe kidney, with an incidence rate of 0.1 % in autopsy examinations (Eisendrath et al. 1925). Fusion anomalies of the kidney were initially described by Wilmer in 1938. However, in 1957, McDonald and McClellan modified this classification (Bauer 2007). In this modified classification, the kidneys are considered ectopic, and they can be a ‘simple ectopic’ or ‘crossed ectopic’ kidney. The ‘crossed ectopic kidney’ can be with or without fusion and may comprise a single or both kidneys (Tiwari et al. 2014). The ‘crossed fused ectopic kidney’ refers to the fused kidney if it is located on the same side, usually at the midline. The reported incidence rate of crossed ectopic kidney in India is 0.003 % (Tiwari et al. 2014). The crossed fused ectopic kidney may have a pancake type of morphology. The pancake kidney has been reported to be an extremely rare variety of the ectopic fused kidney (Tiwari et al. 2014).
The horseshoe kidney comprises 90 % of all kidney fusions (Türkvatan et al. 2009). This anomaly is characterized by two separate kidneys located with one on either side of the midline, and the fusion is usually seen at the lower poles; the connecting part is called the isthmus. However, it is not uncommon to see the fusion at the upper poles. The horseshoe kidney may be found in either the abdomen or pelvic cavity. The inferior mesenteric artery prevents the horseshoe kidney from moving further higher up. The kidney appears more vertical than normal, and the lower poles become more medial because of their fusion. The arterial supply of the horseshoe kidney is variable, depending upon its location (Türkvatan et al. 2009). The difference between the horseshoe and pancake kidney lies in the extent of fusion. The horseshoe kidney has very minimal fusion only at the pole. The pancake kidney demonstrates complete fusion, including fusion at the upper pole, lower pole and hilum. The isthmus is not seen since there is complete fusion, looking like overlapping of the kidneys. Both kidneys fuse together to form a single mass. The pancake kidney has a much lower prevalence. The horseshoe kidney may be found in either the abdomen or pelvis. However, the pancake kidney is always found in the pelvic cavity, in the greater or lesser pelvis. The arterial supply of the pancake kidney is always constant since it lies in the pelvis. The arteries may branch from the iliac arteries or the distal part of the aorta. The veins drain into the iliac veins or the inferior vena cava. The developmental difference between the horseshoe and pancake kidney has been well understood. In the etiology of the horseshoe type, the kidneys start ascending and make contact with each other during the process of ascent. In the pancake type, the kidneys fail to ascend and fuse with each other.
Although the exact mechanism of renal fusion anomalies is not clearly understood, there are several theories explaining their developmental basis (Babu et al. 2015). The human kidneys develop from the metanephros. The two masses of metanephric blastema lie within the pelvis. During later development, the kidneys start ascending and become lumbar in position. Various movements take place during the migration of the kidneys. These complicated movements include the ascent, lateral migration, axial deflection and internal rotation (Türkvatan et al. 2009). Before starting these movements, the nephrogenic blastema will be pushed between the umbilical arteries. Sometimes the fusion takes place during this pushing in between the umbilical arteries. The fused kidneys fail to ascend and form a disc-shaped mass, commonly called the pancake kidney (Türkvatan et al. 2009). This is considered the mechanical theory. If the fusion takes place after the beginning of the renal ascent, the kidney becomes a horseshoe anomaly. In a case of the horseshoe kidney, the fusion takes place only at the superior or inferior pole. According to the caudal rotation theory, the fusion happens because of the rotation and lateral flexion of the caudal end of the fetus, which alters the correct location of the metanephric blastema (Cook and Stephens 1977). According to the genetic theory, the Sonic hedgehog gene is important for the topography of the kidney, and its disruption results in the renal fusion anomaly (Shapiro et al. 2012). Much research is underway to determine the genetic basis of congenital renal anomalies (Babu et al. 2015).
The pancake kidney was first described by Looney and Dodd (1926). This anomalous kidney is just a renal mass observed in the pelvis caused by the complete fusion of the medial part of the renal parenchyma with no intervening septum between the kidneys. Each kidney contains its own collecting part and anteriorly located ureters, which enter the urinary bladder normally (Tiwari et al. 2014). In the present case, a common renal pelvis arose with the fusion of the major calyces, one from each kidney. The single renal pelvis continued as a single ureter. This type of variation comprising a pancake kidney and single ureter is extremely rare. It can occur because of variation in the development and fusion of the ureteric buds. Only five cases of a pancake kidney with a single ureter have been reported in the literature (Martínez-Lázaro and Cortés-Blanco 2000). The pancake kidney is usually associated with accessory renal arteries located around the fused mass. During development, the internal iliac artery and aorta supply the fetal pelvic kidneys. Once the kidneys have ascended upward, they obtain their arterial supply from the renal artery. The branches from the iliac arteries and aorta degenerate (Sadler 1990; Cocheteux et al. 2001). In the present case, many (accessory) renal arteries were observed around the pancake kidney. Alhough we did not check the origin of these arteries, they probably originated from the internal iliac artery. The embryological basis behind these accessory arteries is that the branches from the iliac arteries, which were initially present during early development, failed to degenerate. This happens because of the failure of the ascent of the kidneys, and there is no shifting of the iliac to the renal arteries. This leads to the formation of polar arteries around the pancake kidney with more than one artery, which are known as accessory renal arteries. Accessory renal arteries have been reported to be associated with systemic hypertension (Gokalp et al. 2010). The renal pelvis and ureter were located posterior to the fused kidney in the present case. This type of variant occurs very rarely and, to the best of our knowledge, is the first reported in the literature. This type of course of the renal pelvis and ureter is more prone to kinking, which may lead to the formation of ureteric calculus and hydronephrosis.
The prevalence of pancake kidneys has been reported to be higher in males than females (Tiwari et al. 2014), as in the reported case. The pancake kidney can lead to recurrent urinary tract infections and pelviureteric junction obstruction, which may result in ureteric calculus formation along with hydronephrosis. The stone formation is caused by the malrotation of the collecting part of the kidney and very short ureters, which cause urine stasis and subsequent obstruction (Tiwari et al. 2014). Patients with pelvic kidneys present to the hospital with histories of fever, burning micturition and lower abdominal pain due to urinary tract infections. This morphologically variant kidney is prone to malignant transformation and is more likely to be injured in case of pelvic trauma. However, it is not uncommon to see patients with fused pelvic kidneys having normal kidney function and absolutely no symptoms (Cinman et al. 2007). This type of kidney can be identified in any age group, from infants to the elderly. In females, the pancake kidney may be associated with gynecological problems such as amenorrhea and infertility. At times this type of kidney may be associated with iliac artery or iliac vein aneurysms.
The pancake kidney is often associated with other congenital genitourinary and vertebral anomalies (Tiwari et al. 2014). However, in the present case, we did not observe any other gross variation in the organs of the genital system and vertebral column. The diagnosis of pancake kidney in clinics is always incidental. Formerly, it used to be detected by intravenous urograms, which have now been replaced by investigations such as ultrasounds, computed tomogram scans, nuclear magnetic resonance imaging and radionucleotide scanning. If a pancake kidney is detected and there are no symptoms, the patient can be managed conservatively, and surgical intervention is not required. However, the patient needs long-term follow-up of renal function. In symptomatic cases, conservative management can be given in the form of analgesics and antibiotics. The patient only requires surgical intervention if there are signs and symptoms suggestive of renal failure. Surgery is usually performed in case of abnormal renal function test values or signs of urinary outflow obstruction or obstructive uropathy (Tiwari et al. 2014).
The pancake kidney can be injured during pelvic surgery because of its variant anatomy. It can cause difficulty in vascular surgeries of the iliac vessels and abdominal aorta. Division of the parenchyma of the pelvic kidney may lead to renal vascular damage, renal necrosis, renal infarction and postoperative renal failure. In this context, urologists and pelvic surgeons should be aware of the variant anatomy of the pancake kidney, particularly its vasculature, to prevent unexpected catastrophic bleeding. Because of the variant accessory renal arteries, preoperative vascular studies may be indicated to avoid such complications (Hernández Toriz et al. 2006).
We believe that the present case report gives additional details about the pancake kidney and its variant anatomy. A pancake kidney with a single ureter is extremely rare. Operating surgeons, particularly urologists, gynecologists and pelvic surgeons, should have adequate knowledge about this anomalous type of pancake kidney. This report is also useful for radiologists and pathologists. Clinical anatomists and embryologists may find this report interesting.
Autopsy surgeons should know about the possibility of pelvic and pancake kidneys. If the kidneys are not found in their usual location, the pelvic cavity must be explored because of the possibility of pelvic kidneys. This could be especially important during medicolegal investigations concerning allegations of missing kidneys and unlawful kidney transplantations.
References
Babu CSR, Sharma V, Gupta OP (2015) Renal fusion anomalies: a review of surgical anatomy. Anat Physiol 5:S5001
Bauer SB (2007) Anomalies of the upper urinary tract. In: Wein A (ed) Campbell-Walsh Urology, 9th edn. Saunders Elsevier, Philadelphia, pp 3269–3304
Cinman NM, Okeke Z, Smith AD (2007) Pelvic kidney: associated diseases and treatment. J Endourol 21:836–842
Cocheteux B, Mounier-Vehier C, Gaxotte V, McFadden EP, Francke JP, Beregi JP (2001) Rare variations in renal anatomy and blood supply: CT appearances and embryological background. A pictorial essay. Eur Radiol 11:779–786
Cook WA, Stephens FD (1977) Fused kidneys: morphologic study and theory of embryogenesis. Birth Defects Orig Artic Ser 13:327–340
Eisendrath DN, Phifer FM, Culver HB (1925) Horseshoe kidney. Ann Surg 82:735–764
Glenn JF (1958) Fused pelvic kidney. J Urol 80:7–9
Gokalp G, Hakyemez B, Erdogan C (2010) Vascular anomaly in bilateral ectopic kidney: a case report. Cases J 3:5
Hernández Toriz N, Flores Ojeda R, Ixquiac Pineda G (2006) Renal tumor in a pelvic kidney. Case report. Arch Esp Urol 59:826–829
Looney WW, Dodd DL (1926) An ectopic (pelvic) completely fused (cake) kidney associated with various anomalies of the abdominal viscera. Ann Surg 84:522–524
Martínez-Lázaro R, Cortés-Blanco A (2000) Cake kidney drained by single ureter: MAG3 renogram for diagnosis and function follow-up. Nephrol Dial Transplant 15:1700–1701
Russell RCG, Williams NS, Bulstrode CJK (eds) (2000) Bailey and Love’s short practice of surgery, 23rd edn. Arnold, London, p 1174
Sadler TW (1990) Langman’s medical embryology, 6th edn. William and Wilkins, Baltimore, pp 266–281
Shapiro E, Bauer SB, Chow JS (2012) Anomalies of the upper urinary tract. In: Wein AJ (ed) Campbell-Walsh Urology, vol 4, 10th edn. Saunders Elsevier, Philadelphia, pp 3145
Shoemaker R, Braasch WF (1939) Fused kidneys. J Urol 41:1–7
Tiwari AK, Choudhary AK, Khowal H, Chaudhary P, Arora MP (2014) Pancake kidney: a rare developmental anomaly. Can Urol Assoc J 8:E451–E452
Türkvatan A, Ölçer T, Cumhur T (2009) Multidetector CT urography of renal fusion anomalies. Diagn Interv Radiol 15:127–134
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors of this manuscript declare no conflicts of interest.
Rights and permissions
About this article

Cite this article
Kanchan, T., Murlimanju, B.V. & Saralaya, V.V. Pancake kidney with a single ureter: a rare incidental observation at autopsy. Anat Sci Int 92, 142–146 (2017). https://doi.org/10.1007/s12565-016-0329-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12565-016-0329-y