
Abstract
Norovirus (NoV) is responsible for an estimated 90 % of all epidemic nonbacterial outbreaks of gastroenteritis worldwide. Waterborne outbreaks of NoV are commonly reported. A novel GII.17 NoV strain emerged as a major cause of gastroenteritis outbreaks in China during the winter of 2014/2015. During this time, an outbreak of gastroenteritis occurred at a hotel in a ski park in Hebei Province, China. Epidemiological investigations indicated that one water well, which had only recently been in use, was the probable source. GII.17 NoV was detected by real-time reverse-transcription polymerase chain reaction from samples taken from cases, from concentrated water samples from water well, and from the nearby sewage settling tank. Nucleotide sequences of NoV extracted from clinical and water specimens were genetically identical and had 99 % homology with Beijing/CHN/2015. All epidemiological data indicated that GII.17 NoV was responsible for this outbreak. This is the first reported laboratory-confirmed waterborne outbreak caused by GII.17 NoV genotype in China. Strengthening management of well drinking water and systematica monitoring of NoV is essential for preventing future outbreaks.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Norovirus (NoV) has a positive-sense, polyadenylated RNA genome of approximately 7.5 kb. The genome is organized into three open-reading frames (ORFs): ORF1 encodes the nonstructural polyprotein, while ORF2 and ORF3 encode the major (VP1) and minor (VP2) capsid proteins, respectively. Six or seventh NoV genogroups have been recognized (GI to VI or VII) (Vinje 2015). Genogroups GI, GII, and GIV can infect humans. Different genetic clusters can be classified using a web-based genotyping tool (http://www.rivm.nl/mpf/norovirus/typingtool) based on a sequence of ≥100 nucleotides from genogroup I or II NoV capsids or a sequence of ≥100 nucleotides within the 800 nucleotides at the 3′ end of ORF1 (Kroneman et al. 2011). Common symptoms of NoV infection are nausea, vomiting, abdominal pain, and diarrhoea. Rare symptoms include fever, headache, and body aches. Infection occurs predominantly by ingestion of faecally contaminated food or water, or through person-to-person contact (Matthews et al. 2012). NoV infection has an incubation period of 12–48 h, with most cases recovering within 1–3 days (Bull et al. 2006).
NoV is responsible for an estimated 90 % of all epidemic nonbacterial outbreaks of gastroenteritis worldwide (Lindesmith et al. 2003), while waterborne NoV outbreaks accounted for 1.5 % (Kroneman et al. 2008). A number of waterborne NoV outbreaks caused by contaminated drinking water have been reported (Nygard et al. 2003; Maunula et al. 2005), including in China (Li et al. 2013; Zhou et al. 2012, 2015). Outbreaks in closed or semi-closed settings are generally associated with a single GII genotype (Matthews et al. 2012), most commonly GII.4 (Kroneman et al. 2008).
Previous reports have shown that the genotype GII.4/Sydney/2012 has been the major circulating NoV genotype worldwide and has resulted in more than 40 % of all outbreaks (Vega et al. 2014; Emergence of new norovirus strain GII.4 Sydney-United States, 2012 2013). The GII.17 genotype has been circulating for many years and has sporadically been detected throughout the world (de Graaf M et al. 2015). However, a novel GII.P17-GII.17 NoV strain has emerged as the major cause of gastroenteritis outbreaks in China and Japan, including outbreaks in Beijing during the winter of 2014/2015 (Gao et al. 2015; Lu et al. 2015). The frequency of NoV isolation from groundwater has been reported to be approximately 8–21 % worldwide (Lee et al. 2011). Here, we report an outbreak caused by GII.17 NoV-contaminated well water in Hebei Province, China.
Methods
Study Design
We identified a waterborne outbreak of acute gastroenteritis that occurred among guests and staffs at a hotel in China. The hotel was situated in Hebei province, near an international ski resort. The outbreak was investigated immediately after it was reported to Fengtai District Center for Disease Control and Prevention (CDC) of Beijing on 10 December 2014. Two investigators comprehensively recorded the entire investigation and completed all of the relevant documents appropriately. Environmental investigation included microbiological testing of kitchen cleavers, cutting boards, and dishcloths drinking water, and sewage. The water supply system is shown in Fig. 1. The water from wells A, B, C, and D were pumped into the reservoir and disinfected. Drinking wells A, B, and D are 5 m deep. Well C is 20 m deep. The sewage settling tank is 8 m deep and 50 m away from well C. The water from A, B, and D were used everyday, but the water from well C was only used in the dry season. The sewage settling tank was built during summer 2014 and was not constructed with leakage prevention facilities. Wells A and B are located in the north of reservoir. The hotel building, well D and reservoir are at the same altitude. The sewage settling tank and well C are located in the south of reservoir.

Schematic presentation of the water supply system for the hotel. It shows the position relationship among the hotel building, drinking well A, B, C, and D, the reservoir, and the sewage settling tank
No ethical approval was required as this study was carried out as part of a public health response to an acute incident. Each study subject provided verbal informed consent.
Case Definitions
A case was defined as either a guest staying at, or a member of staff working at, the hotel, who had abdominal pain, vomiting, and diarrhoea (defined as two or more loose stools within a 24-h period) on or after 3 December 2014. All cases were at the hotel. We excluded a number of cases that were infected with NoV but did not develop symptoms while at the hotel.
Case–Control Study
All probable cases with onset of symptoms during 3–17 December 2014 at the hotel were enrolled in the case–control study. Controls were selected randomly from asymptomatic staff and guests at a ratio of 1:2. Controls were frequency matched to cases by occupation. A questionnaire survey was conducted by face-to-face interview at the hotel or by telephone interview with cases that had checked out before 10 December 2014. Questionnaires captured details of clinical illness and exposures to suspected food and water.
Sample Collection
Four faecal samples and 11 rectal swabs were collected on or after 7 December 2014 from 15 patients (11 staff and 4 guests) who had ongoing gastrointestinal symptoms and had not received antibiotic treatment. Five-litre samples of water were collected from each well, from the reservoir, and from the sewage settling tank. Thirteen swab samples were collected from kitchen cleavers, cutting boards, and dishcloths. Samples of 12 food items were collected and transported immediately to the laboratory for microbiological testing.
Laboratory Investigation
All samples were screened according to a standard laboratory protocol for the presence of Salmonella spp., Vibrio parahaemolyticus, Shigella spp., Staphylococcus aureus, Proteus spp., and diarrhoea genic Escherichia coli. Suspensions of rectal swabs and swabs of environment surfaces were prepared by adding 1 ml phosphate-buffered saline (PBS; pH 7.2) and briefly vortexing. Suspensions of faecal samples were prepared by vortexing 0.2 g of faeces with 800 µl PBS for 3 min followed by centrifugation at 13,000 rpm for 10 min. Virus was enriched from water samples as described elsewhere (Matsuura et al. 1984, 2000). Briefly, 5000 ml water samples were centrifuged at 10,000×g for 30 min and filtered through paper. Magnesium chloride was added to the filtrate for a final concentration of 0.05 M. The pH was adjusted to 3.0 and then filtered through a cellulose nitrate membrane filter (0.45 μm, Advantec, Japan).Filter membranes were cut into small pieces and immersed in 10 ml 3 % beef extract solution and sonicated for 5 min before centrifugation for 5 min. PEG6000 and sodium chloride were added to the supernatant to make final concentration of 10 % and 0.3 M, respectively. Samples were then incubated (12 h at 4 °C) and centrifuged (10,000×g for 30 min). Pellets were resuspended in 1 ml of RNase-free water (Zhou et al. 2012). RNA was extracted from faecal samples, environmental swabs, rectal swabs, and concentrated water specimens using a QIAamp Viral RNA Mini Kit (Qiagen, Hilden, Germany). Rotavirus and NoV were detected in all the treated samples by real-time reverse-transcription polymerase chain reaction according to the manufacturer’s instructions using detection kits produced by Jiangsu Shuoshi Bio-Tech Co., Ltd. (Jiangsu, China; rotavirus, lot no. JC50101; norovirus, lot no. JC50201). Partial polymerase sequences were obtained from the four faecal samples and two concentrated water specimens as described elsewhere (Jiang et al. 1999) with primers p289 (GATTACTCCAAGTGGGACTCCAC) and p290(TGACAATGTAATCATCACCATA) and sequenced using an ABI 3730 DNA Analyzer (Applied Biosystems) with primer p290. Sequences were genotyped using a web-based genotyping tool (http://www.rivm.nl/mpf/norovirus/typingtool) (Kroneman et al. 2011) and using a BLAST tool (http://blast.ncbi.nlm.nih.gov/).
Statistical and Phylogenetic Analysis
All statistical analyses were performed using SPSS version 15.0 (SPSS Inc., Chicago, IL, USA). Phylogenetic trees were produced using Clustal W and MEGA5.0 with neighbour-joining methods.
Nucleotide Sequence Accession Numbers
Nucleotide sequences obtained from this outbreak have been deposited in the GenBank database with accession numbers: KU310883-KU310888.
Results
Epidemiological Investigation
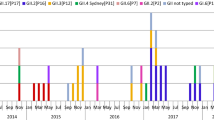
There were 29 cases reported from 3 December to 17 December 2014. Twenty cases were the restaurant staff of the hotel, and nine cases were guests. The earliest case was a receptionist at the hotel. Fourteen cases received clinical treatment but none were hospitalized. Sixty-two percent of cases (18/29) were female, and the median age was 25.2 years (range 18–36 years). Among the 29 cases, 25 (86.2 %) experienced vomiting and other common symptoms, including nausea (60.1 %),diarrhoea (86.2 %), abdominal pain (46.0 %), and fever (17.24 %).The outbreak lasted for 14 days. An epidemic curve showed two peaks, on 6 and 11 December, but new cases were reported nearly every day after the start of the outbreak (Fig. 2).

Epidemiological data for the waterborne gastroenteritis outbreak caused by NoV GII.17. Graph showing the number of cases reported every day and that the outbreak began on 3 December, peaked on 6 and 11 December (after intervention), and ended on 17 December
Seventeen staff cases had a meal while at work and three staff cases had meals from home. The nine guests who were cases had their meals at a cafeteria, fast food eateries, or Chinese hot pot restaurants. Cases and controls ate 16 different foods or set meals from the restaurant or meals prepared by family members and reported drinking three different kinds of water. Three of the 29 (10.3 %) cases and 1/58 (1.72 %) controls had drunk tap water (odds ratio [OR] = 6.0, 95 % confidence interval [CI]:0.60–60.24). Because all the guest cases were athletes from different countries, we investigated and anglicised the information from the athletes and athlete controls. Of the nine cases who were athletes and 18 athlete controls, 3/9 (33.3 %) cases and 1/18 (6 %) controls reported drinking tap water (OR = 6.0, 95 % CI 0.54–66.17) (Table 1).The OR of athlete cases serviced by staff cases to athlete control serviced by healthy staffs was 14.0 (95 % CI 1.49–131.89).
The environmental investigation demonstrated that the tap water at the hotel was sourced from a reservoir whose water was obtained from four wells near the hotel (Fig. 1). The water in the reservoir was disinfected using chlorine but the disinfection effect was not evaluated. A number of food items, such as fruit and vegetables were washed using this water from the reservoir and then were sent to the restaurants. Well C, which is 20 m deep underground, is about 50 m from a sewage settling tank that is 8 m deep underground. The sewage settling tank was built about 5 months before the outbreak and had no anti-osmosis measure to isolate sewage. Drinking well C was a spare well that was used only during periods of drought. This outbreak occurred after drinking well C had been in use for about one week.
Isolation of Bacterial and Viral Pathogens
No bacterial pathogens were detected in any of the samples except those from the sewage settling tank. Salmonella spp. and E. coli. were isolated from the sewage water samples. NoV GII was detected in all faecal samples, rectal swabs, and from two concentrated water specimens from drinking well C and sewage settling tank. No rotavirus was detected in these samples. All other samples were negative for rotavirus and NoV.
Nucleotide Sequence Similarity and Phylogenetic Analysis
The nucleotide sequences from the water samples and the faecal samples were 99.0–100 % homologous to each other. All sequences were genotyped as NoV GII.17 using the web-based genotyping tool (http://www.rivm.nl/mpf/norovirus/typingtool) and a BLAST tool (http://blast.ncbi.nlm.nih.gov/). Phylogenetic analysis indicated that sequences clustered on the same branch and were closely related to the strain GII.17 Beijing/CHN/2015 (GenBank: KP857570) and Zhuhai/CHN/2015 (GenBank: KT253245) (Fig. 3).

Phylogenetic tree of the norovirus detected from the outbreak. Phylogenetic analysis was performed with a 319 base pair sequence of the partial polymerase gene of NoV and the tree constructed using the neighbour-joining algorithm implemented in MEGA version 5.0 software with 1000 bootstrap pseudoreplicates. Norovirus GII.4 strains were used as outgroups
Outbreak Control Measures and End of the Outbreak
The outbreak was reported to Fengtai District CDC of Beijing on 10 December. Epidemiological investigation and sample collection were carried out by Fengtai District CDC of Beijing. Investigation indicated that the outbreak involved the use of drinking well C, but all the factors between the cases and controls did not identify a main risk factor causing the outbreak, and no OR data are statistically significant, including drinking tap water (Table 1). This indicates that exposure to NoV may have been from multiple sources. When the suspected risk factor was identified as drinking water from well C (10 December), the supply of water from drinking well C was stopped. When the pathogen was confirmed on 13 December from the cases and the concentrated water samples, drinking well C was closed and the reservoir and the tap systems well as the hotel rooms and public areas were disinfected according to the National Standard by CDC workers. The water supply system was disinfected with free chlorine at the concentration ≥0.05 mg/l for 30 min. The hotel rooms and public areas were disinfected by cleaning and spraying with 1000 mg/l sodium hypochorite solution of 84 disinfectant solution in accordance with the instructions (Dezhou Gelijie Disinfection Products Co. LTD, Shandong, China). The cases were isolated for 3 days, and health education was carried out to improve the knowledge of staffs for NoV infection. The outbreak was determined to be controlled on 17 December.
Discussion
This study describes the investigation of a gastroenteritis outbreak in a hotel in Hebei province, China. Although no significant risk factor was identified during the investigation, the epidemiological evidence suggests that there was some relationship between the outbreak and using the water from well C. The outbreak occurred one week after well C was put into use. Symptoms of cases were compatible with a clinical diagnosis of NoV infection. NoV GII.17 was detected in all samples from cases and also from well C and sewage water samples. Based on the epidemiological investigation, the laboratory investigation, and the effectiveness of control measures, we can draw the conclusion that NoV GII.17 was responsible for this outbreak.
NoV is present at high levels in wastewater, even after treatment processes (da Silva et al. 2007). NoV particles may be detected in wastewater treatment plant effluents throughout the year (Flannery et al. 2012). GII.17 NoV accounts for 76 % (16/21) of the typed strains from water sources from rural, urban, and refugee settings in Kenya (Kiulia et al. 2014). Viruses dispersed into the aquatic environment can also reach the ground water sources (Locas et al. 2007). We have insufficient evidence to prove conclusively that drinking water from well C was contaminated by the sewage settling tank, but the sewage settling tank was not constructed with anti-leakage devices, and a high nucleotide homology of NoV GII.17 was found between samples detected from well C and the sewage water. It is feasible that the water from the sewage could have seeped into well C and contaminated it. When the contaminated water was not strictly disinfected, the outbreak occurred. The water was subsequently disinfected, but the effect of this intervention was not formally evaluated.
That the OR of one risk factors is 14 (CI 1.49–131.89) (Table 1) indicates that there was statistically significant difference between the exposures of athlete cases serviced by staff cases to athlete control serviced by healthy staffs. It could be inferred that staff cases may have contributed to the development and progression of the outbreak in guests. There were only nine cases among guests, but it is possible that some guests checked out before symptom onset, so the epidemic curve may not reflect the full extent of the outbreak (Fig. 3).
This is the first recorded outbreak caused by NoV GII.17-contaminated drinking water in China. This outbreak was not reported in a timely manner, and effective control measures were not taken immediately; consequently, the outbreak lasted for 15 days. Sensitive monitoring systems are important for timely responses to outbreaks, to confirm the causative agent, to control the spread of NoV, and to monitor the molecular epidemiology of NoV genotypes.
In conclusion, this study described a gastroenteritis outbreak associated with a drinking-water well contaminated with NoV GII.17 in China. This genotype was a novel, predominating genotype in China in the winter of 2014/2015, causing several outbreaks in China. This is the first recorded waterborne outbreak with this NoV genotype. Strengthening water well management is vital for controlling waterborne outbreaks caused by NoV, and systematic monitoring is essential for studying the evolution of NoV and monitoring trends in the geographical spread of GII.17.
References
Bull, R. A., Tu, E. T., McIver, C. J., Rawlinson, W. D., & White, P. A. (2006). Emergence of a new norovirus genotype II.4 variant associated with global outbreaks of gastroenteritis. Journal of Clinical Microbiology, 44, 327–333.
da Silva, A. K., Le Saux, J. C., Parnaudeau, S., Pommepuy, M., Elimelech, M., & Le Guyader, F. S. (2007). Evaluation of removal of noroviruses during wastewater treatment, using real-time reverse transcription-PCR: different behaviors of genogroups I and II. Applied and Environment Microbiology, 73, 7891–7897.
de Graaf, M., van Beek, J., Vennema, H., et al. (2015). Emergence of a novel GII.17 norovirus—End of the GII.4 era? Euro Surveillance 20.
Emergence of new norovirus strain. (2013). GII.4 Sydney-United States, 2012. MMWR. Morbidity and Mortality Weekly Report, 62, 55.
Flannery, J., Keaveney, S., Rajko-Nenow, P., O’Flaherty, V., & Dore, W. (2012). Concentration of norovirus during wastewater treatment and its impact on oyster contamination. Applied and Environment Microbiology, 78, 3400–3406.
Gao, Z., Li, X., Yan, H., et al. (2015). Human calicivirus occurrence among outpatients with diarrhea in Beijing, China, between April 2011 and March 2013. Journal of Medical Virology, 87, 2040–2047.
Jiang, X., Huang, P. W., Zhong, W. M., Farkas, T., Cubitt, D. W., & Matson, D. O. (1999). Design and evaluation of a primer pair that detects both Norwalk- and Sapporo-like caliciviruses by RT-PCR. Journal of Virological Methods, 83, 145–154.
Kiulia, N. M., Mans, J., Mwenda, J. M., & Taylor, M. B. (2014) Norovirus GII.17 predominates in selected surface water sources in Kenya. Food and Environmental Virology.
Kroneman, A., Vennema, H., Deforche, K., et al. (2011). An automated genotyping tool for enteroviruses and noroviruses. Journal of Clinical Virology, 51, 121–125.
Kroneman, A., Verhoef, L., Harris, J., et al. (2008). Analysis of integrated virological and epidemiological reports of norovirus outbreaks collected within the Foodborne Viruses in Europe network from 1 July 2001 to 30 June 2006. Journal of Clinical Microbiology, 46, 2959–2965.
Lee, H., Kim, M., Lee, J. E., et al. (2011). Investigation of norovirus occurrence in groundwater in metropolitan Seoul, Korea. Science of the Total Environment, 409, 2078–2084.
Li, Y., Guo, H., Xu, Z., et al. (2013). An outbreak of norovirus gastroenteritis associated with a secondary water supply system in a factory in south China. BMC Public Health, 13, 283.
Lindesmith, L., Moe, C., Marionneau, S., et al. (2003). Human susceptibility and resistance to Norwalk virus infection. Nature Medicine, 9, 548–553.
Locas, A., Barthe, C., Barbeau, B., Carriere, A., & Payment, P. (2007). Virus occurrence in municipal groundwater sources in Quebec, Canada. Canadian Journal of Microbiology, 53, 688–694.
Lu, J., Sun, L., Fang, L., et al. (2015). Gastroenteritis outbreaks caused by norovirus GII.17, Guangdong Province, China, 2014–2015. Emerging Infectious Diseases, 21, 1240–1242.
Matsuura, K., Hasegawa, S., Nakayama, T., Morita, O., & Uetake, H. (1984). Viral pollution of the rivers in Toyama City. Microbiology and Immunology, 28, 575–588.
Matsuura, K., Ishikura, M., Yoshida, H., et al. (2000). Assessment of poliovirus eradication in Japan: genomic analysis of polioviruses isolated from river water and sewage in toyama prefecture. Applied and Environment Microbiology, 66, 5087–5091.
Matthews, J. E., Dickey, B. W., Miller, R. D., et al. (2012). The epidemiology of published norovirus outbreaks: A review of risk factors associated with attack rate and genogroup. Epidemiology and Infection, 140, 1161–1172.
Maunula, L., Miettinen, I. T., & von Bonsdorff, C. H. (2005). Norovirus outbreaks from drinking water. Emerging Infectious Diseases, 11, 1716–1721.
Nygard, K., Torven, M., Ancker, C., et al. (2003). Emerging genotype (GGIIb) of norovirus in drinking water, Sweden. Emerging Infectious Diseases, 9, 1548–1552.
Vega, E., Barclay, L., Gregoricus, N., Shirley, S. H., Lee, D., & Vinje, J. (2014). Genotypic and epidemiologic trends of norovirus outbreaks in the United States, 2009 to 2013. Journal of Clinical Microbiology, 52, 147–155.
Vinje, J. (2015). Advances in laboratory methods for detection and typing of norovirus. Journal of Clinical Microbiology, 53, 373–381.
Zhou, X., Li, H., Sun, L., et al. (2012). Epidemiological and molecular analysis of a waterborne outbreak of norovirus GII.4. Epidemiology and Infection, 140, 2282–2289.
Zhou, N., Zhang, H., Lin, X., et al. (2015). A waterborne norovirus gastroenteritis outbreak in a school, eastern China. Epidemiology & Infection 1–8.
Acknowledgments
We thank all the staff members of the hotel who helped with this study.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of Interest
The authors declare that they have no competing interests.
Additional information
Meng Qin and Xiao-Gen dong contributed equally to the manuscript.
Rights and permissions
About this article

Cite this article
Qin, M., Dong, XG., Jing, YY. et al. A Waterborne Gastroenteritis Outbreak Caused by Norovirus GII.17 in a Hotel, Hebei, China, December 2014. Food Environ Virol 8, 180–186 (2016). https://doi.org/10.1007/s12560-016-9237-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12560-016-9237-5