
Abstract
Job strain has been associated with hypertension among younger workers; however, whether this relationship persists among older workers, particularly older racial/ethnic minorities, is unresolved. This study evaluated whether job strain and workplace discrimination are associated with hypertension and poor blood pressure control among older workers and whether these relationships vary by gender and race/ethnicity. Data were drawn from the Health and Retirement Study, and analysis was restricted to employed participants with complete information on job strain and blood pressure (N = 3,794). In adjusted models, high job strain was associated with lower likelihood of hypertension (odds ratio (OR): 0.75, 95% confidence interval (CI): 0.63, 0.89) relative to low job strain. Stratified analyses indicated this association was only significant among white (OR: 0.71, 95% CI: 0.58, 0.86) and male (OR: 0.61, 95% CI: 0.47, 0.79) workers. High job strain was not significantly associated with hypertension among African American (OR: 1.14, 95% CI: 0.63, 2.07) or Hispanic (OR: 0.56, 95% CI: 0.29, 1.09) workers. Workplace discrimination was not associated with hypertension among any group. Neither job strain nor discrimination was associated with poor blood pressure control. These findings suggest that persistence in work characterized by high job strain in later life may signal resilience to the influence of work-related stressors on health. Future research efforts should examine the factors that contribute to gender and racial differences in these relationships.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The “graying” of the United States workforce represents one of the most significant demographic shifts of the early twenty-first century. Over 27 million US adults over the age of 55 currently work at least part-time, and there are indications that the “baby boomer” generation (born 1946–1964) will continue the trend of working well into the sixth decade of life (Gendell 2008; US Bureau of Labor 2009). By 2018, the Department of Labor projects that nearly one out of every four workers will be age 55 or older (United States Bureau of Labor 2009). This transition has implications for the understanding of how work-related stress is related to health in later life. However, the relationship between work-related stress and health among older adults, particularly women and racial/ethnic minorities, has been under explored.
The transition to retirement and work stoppage in later life varies significantly across gender and racial/ethnic groups (Szinovacz and DeViney 1999), and these differences may also be reflected in exposure to and consequences of work-related stress. Compared to whites, African Americans are more likely to experience involuntary job loss in the years immediately preceding (and likely eventuating in) retirement (Flippen and Tienda 2000). Given the instability associated with lower-wage, lower-skill employment that many racial minorities engage in (due in part to lower educational attainment and subsequently truncated employment opportunities), it has been argued that “retirement” as it is commonly conceived (e.g., a period of consumption and leisure after career employment) is not a salient event for these groups (Gibson 1987; Quinn and Kozy 1996). For example, racial/ethnic minorities in the United States tend to rely on social security for retirement benefits more heavily than non-Hispanic whites, with approximately 33% of African Americans and Hispanics using social security for 100% of their retirement income compared to 16% of whites (Hendley and Mushinski 2000).
Although employment is generally associated with better mental health relative to other labor force groups (i.e., disabled, unemployed), occupational stress has been associated with numerous poor health outcomes, including psychological distress, alcohol misuse and abuse, and cardiovascular disease (Karasek 1979; Ohlin et al. 2007; Stansfeld and Candy 2006; Wang et al. 2008; Yang et al. 2001). Several theoretical frameworks of job strain are built on the concept that work-related stress, in and of itself, is not pathogenic, rather, it is the interaction of high levels of stress in the context of low control or reward that drives the association with poor health (Karasek 1979; Theorell and Karasek 1996; Seigrist 1996). For instance, Karasek’s (1979) seminal demand-control model of work is characterized by an imbalance of high cognitive or physical demand accompanied by low decision latitude or control over the type or pace of work. High levels of job strain negatively influence health by fostering learned helplessness and impairing sense of control (Seligman 1975; Wang et al. 2009). However, with few notable exceptions (de Zwart et al. 1999), the majority of these reports have focused on younger adults, and it is not clear how occupational stressors influence older workers (Power et al. 1998).
Hypertension is more prevalent among African Americans relative to any other racial/ethnic group in the United States, affecting approximately one out of every three African American adults over the age of 18 (Hajjar and Kotchen 2003; Egan et al. 2010). Among those with hypertension, African Americans also have disproportionately high levels of poor blood pressure control (Egan et al. 2010). However, the majority of studies that have examined work-related stressors and hypertension have not included substantial numbers of African American workers, and few studies have examined racial/ethnic differences in the relationship between occupational stressors and hypertension. In one of the largest studies of job strain and hypertension among African American workers, Curtis and colleagues (1997) reported that job strain was not significantly associated with blood pressure (Curtis et al. 1997), although the decision latitude component of job strain was related to hypertension among African American men, suggesting that the relationship between work-related stressors such as job strain may vary by gender as well. Additionally, racial discrimination has been linked to hypertension among racial/ethnic minorities (Williams and Neighbors 2001), and the consideration of racial discrimination as a unique work-related stressor and its relationship to hypertension warrants further investigation.
Building on previous literature on the relationship between workplace exposures and hypertension risk among younger adults, we explored the relationship between work-related stressors and blood pressure using data from the 2006 and 2008 waves of the Health and Retirement Study (HRS), a nationally representative sample of adults over the age of 50. We evaluated two main research questions: (1) Are work-related stressors, specifically job strain and workplace discrimination, associated with elevated systolic blood pressure, hypertension, and poor blood pressure control? and (2) Do these relationships vary by gender and race/ethnicity?
Methods
Sample
The Health and Retirement Study (HRS) is a nationally representative prospective cohort of US adults over the age of 50 which has been under study since 1992. Details of the survey design have been discussed elsewhere (Juster and Suzman 1995). This analysis was restricted to employed HRS respondents who completed the Psychosocial Leave-Behind questionnaire. This self-administered questionnaire was given to respondents who completed in-person interviews in 2006 and 2008 (Clarke and Fisher 2007). Approximately 50% of the HRS sample was selected for an in-person interview in 2006, and the other 50% was assigned 2008 (Crimmins et al. 2008). We pooled these two years of data for analysis.
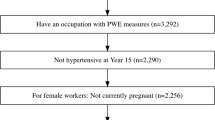
This analysis was restricted to currently employed (full-time, part-time, or partially retired at the time of the in-person interview) participants who completed the items on job strain and workplace discrimination: 2,097 participants in 2006 and 1,697 in 2008. In total, 3,794 respondents employed in either 2006 or 2008 had valid data on the measures of job strain and workplace discrimination and relevant covariates. Respondents missing data on these work-related stressor measures were older (χ2 = 120.1, p < 0.001), less educated (χ2 = 36.8, p = 0.001), less likely to be white (χ2 = 95.4, p < 0.001), less likely to be women (χ2 = 21.7, p < 0.001), and less likely to be working full-time (χ2 = 154.7, p < 0.001) than those with complete data. A post hoc comparison of job strain characteristics of those included in the study versus those excluded for insufficient job strain data (but who still provided at least some data) reveals very few significant differences between these groups. Thus, we feel that the 3,794 participants included in this study are adequately representative of the total eligible pool of participants in terms of job strain.
The Health and Retirement Study was approved by the Institutional Review Board at the University of Michigan and all participants provided informed consent.
Measures
Job Strain
Occupational stress and satisfaction were assessed in the Psychosocial Leave-Behind using a 15-item index derived from Karasek’s job strain scale (Karasek 1998). Participants were asked to rate on a 4-point Likert scale to what degree each statement described their current job (e.g., I receive the recognition I deserve for my work; I have very little freedom to decide how I do my work; I have the opportunity to develop new skills; I am free from conflicting demands that others make). These 15 items describe two factors: job stress (6 items, α = 0.80) and job satisfaction (9 items, α = 0.75) (Clarke and Fisher 2007). The job stress factor included indicators of job effort and degree of control over workflow, while the job satisfaction factor focused more on opportunities for promotion and recognition for achievements. The item scores that describe each factor were averaged to produce an overall score for both job stress and job satisfaction, each having a range of 1–4. In order to examine the combination of job stress and satisfaction, these two scales were dichotomized at the median (indicating high/low job stress and high/low job satisfaction). We developed a categorical measure of “job strain” based on the demand-control and effort-reward imbalance models put forth by Karasek (1979) and Seigrist (1996) in which they outline the conceptual basis for combining positive (e.g., job satisfaction) and negative (e.g., job stress) aspects of work into a single aggregate variable for analysis. Following these models, we created a job strain measure that reflects the confluence of stress and satisfaction in a single, four-level variable (e.g., low stress/high satisfaction (which served as the reference group for all analytic comparisons), low stress/low satisfaction, high stress/high satisfaction, and high stress/low satisfaction). We conducted post hoc sensitivity analyses to assess the influence of this categorization approach by examining job stress and satisfaction as continuous indicators as well and the results were consistent with the findings presented here.
Workplace Discrimination
Experiences of workplace discrimination were measured using a 6-item scale (Cronbach’s alpha = 0.81) developed by Williams et al. (1997). The scale asks about discriminatory experiences at work over the past 12-month period (e.g., how often are you unfairly given the tasks at work that no one else wants to do? How often do you feel that you have to work twice as hard as others? How often do you feel ignored or not taken seriously by your boss?). Items are scored on a 6-point scale ranging from 1 = Never to 6 = Almost every day and averaged to create an overall score (Williams et al. 1997). Because reports of workplace discrimination were extremely uncommon in the sample (average score = 1.65, SD = 0.85, indicating that most people reported experiencing any of these events less than once per year), we collapsed this average score into a four-level indicator variable, workplace discrimination index scoring: never experienced workplace discrimination (average score = 1); infrequently experienced workplace discrimination (average score >1–≤2); occasionally experienced workplace discrimination (average score <2–≤3); and frequently experienced workplace discrimination (average score >3).
Hypertension
During the in-person interviews (conducted with 50% of the sample in 2006 and the remaining 50% in 2008) anthropomorphic and physiologic (e.g., blood pressure, salivary cortisol, and blood spots) measures were collected. The details of the consent and data collection process have been discussed elsewhere (Crimmins et al. 2008). Resting, seated blood pressure was assessed using the Omron HEM-780 N monitor at three points during the interview. In total, 3,561 (93.9%) of the respondents had valid measurements at all three assessments. The repeated measures (up to three) were averaged into single values of diastolic and systolic blood pressure.
In order to evaluate the relationship between work-related stressors and clinically elevated blood pressure, hypertension status was determined by dichotomizing the diastolic and systolic blood pressure measurements. Participants were classified as hypertensive if average systolic blood pressure met or exceeded 140 mmHg and/or if average diastolic blood pressure met or exceeded 90 mmHg (Chobanian et al. 2003). Participants who self-reported that took medication for high blood pressure were considered to have hypertension even if their average blood pressure was less than 140/90 mmHg. Among those who reported taking antihypertensive medication, a dichotomous variable for poorly controlled hypertension was constructed (0 = Taking medication and blood pressure is <140/90 mmHg, 1 = Taking medication and blood pressure is at or above 140/90 mmHg).
Covariates
Several factors that have been identified as potential confounders in the relationship between work-related stressors and hypertension were included in the multivariable models. Demographic characteristics included age (dichotomized as over 65 years vs. 50–65 years to reflect Medicare age-eligibility), sex, race/ethnicity (categorized as non-Hispanic white, non-Hispanic black, and Hispanic), marital status (categorized as married, separated/divorced, widowed, or never married), and educational attainment (dichotomized as high school education less vs. at least some college). Socioeconomic position was indicated by net worth, calculated by subtracting total debt (e.g., mortgage, care payments, loans) from total assets (e.g., home ownership, stocks, income), standardized according to the sample mean; we used net worth to indicate socioeconomic position because it is a more appropriate indicator for older adults that alternative measures such as income (Smith and Kington 1997). Labor force status was categorized according to the RAND criteria (Clair et al. 2009), indicated as full-time, part-time, or partly retired. Occupation was categorized as blue-collar (e.g., farming, machine operators, construction, and similar trade occupations), service-related (e.g., security, cleaning, food preparation, health, and personal service occupations), or white-collar (e.g., management, professional specialists, sales, and administrative occupations). Tenure (in years) at current job was also assessed. Smoking status was assessed by self-report and categorized as never, former, and current. Weekly alcohol use was categorized as a three-level variable: none, 1–7 drinks, and eight drinks or more. Body mass index (BMI) in kg/m2 was calculated from measured weight and height and treated as a continuous variable.
Statistical Analysis
We fit regression models for each of the three outcomes: systolic BP, hypertension, and poor BP control. Initially, the associations between job strain and workplace discrimination with these outcomes were investigated using bivariate (unadjusted) linear (for systolic BP) and logistic (for hypertension and poor BP control) regression models. Next, we conducted a series of nested regression models to assess the relationship between work-related stressors and the three blood pressure outcomes. Each base model was adjusted for age, race, sex, and marital status. Step two additionally adjusted for indicators of socioeconomic position: education, labor force status, type of work, and net worth. Finally, in step three, we adjusted for behavioral factors: smoking status, alcohol intake, and BMI. We assessed whether the relationships between occupational stress and satisfaction varied by race/ethnicity and gender using stratified models and interaction terms.
In order to assess potential bias due to the “Healthy Worker Survivor” effect in which bias can be introduced through the selective attrition of workers in poor health (Arrighi and Hertz-Picciotto 1994; Pearce et al. 2007), we also ran the analysis restricting the sample to those who had worked at their current job for at least 5 years. We also conducted sensitivity analyses examining job stress and satisfaction as continuous indicators (as opposed to the 4-level job strain index). Finally, we conducted post hoc analyses stratifying the sample by job type (white-collar, blue-collar, and service-related) to determine whether the relationship between job strain and hypertension varied by occupation.
Relative model fit was assessed using Akaike Information Criterion (AIC), for which smaller values indicate better fit; the log likelihood, for which smaller values indicate better fit, and rescaled pseudo-R2, for which higher values indicated better fit. We performed all analyses using SAS (version 9.2) and all p-values refer to two-tailed tests.
Results
Overall, workers in the sample reported moderately high job satisfaction (mean = 2.92, SD = 0.50 on a 4-point scale) and moderate job stress (mean = 2.03, SD = 0.54). Approximately 33% of the workers fell into the high job strain (high stress combined with low satisfaction) and 34% fell into the low job strain category (low stress combined with high satisfaction). As shown by Table 1, workers who reported high levels of job strain were younger, had less education, were more likely to be in blue-collar occupation and had lower net worth. Levels of job strain did not vary significantly by race/ethnicity or gender. Approximately 58% of workers met criteria for hypertension, and of those taking antihypertensive medications approximately 35% had poor BP control. Neither systolic nor diastolic BP varied by job strain, but both hypertension and use of antihypertensive medications were more common among those with low job strain. Hispanics reported somewhat more frequent experiences of workplace discrimination (M: 1.76, SD: 0.95) than African Americans (M: 1.68, SD: 0.88) and whites (M: 1.64, SD: 0.85), F = 2.57, p = 0.077. There was no difference in reports of workplace discrimination between men (M: 1.66, SD: 0.86) and women (M: 1.65, SD: 0.86), F = 0.8, p = 0.772.
Job Strain and Blood Pressure
Consistent with the bivariate analyses, job strain was inversely, but not significantly, related to systolic BP in fully adjusted linear regression models (β: −1.02; 95% CI: −2.53, 0.49) in the sample overall. As shown by Table 2, high job strain (high job stress combined with low job satisfaction) was associated with lower likelihood of hypertension, a finding that persisted after adjustment for demographic and occupational characteristics and health behaviors (OR: 0.75; 95% CI: 0.63, 0.89). High job stress combined with high job satisfaction was also significantly associated with lower likelihood of hypertension (OR: 0.66; 95% CI: 0.53, 0.82). Working in a service-related occupation was significantly associated with higher relative odds of hypertension (OR: 1.32; 95% CI: 1.03, 1.68). The analyses treating job stress and satisfaction as individual, continuous predictors produced similar results (ORstress: 0.76; 95% CI: 0.65–0.88; ORsatisfaction: 0.72; 95% CI: 0.79–1.08 in fully adjusted models). In analyses stratified by race/ethnicity and gender (Tables 3, 4), the association between high job strain and lower relative odds of hypertension was only present for non-Hispanic whites and men. However, the interactions between race/ethnicity and gender with job strain from logistic models were not statistically significant (interaction term χ2 = 9.7, p = 0.138 for race/ethnicity; χ2 = 3.4 p = 0.338 for gender).
In post hoc analyses stratifying the sample by occupation type (white-collar, blue-collar, service-related), the inverse relationship between job strain and hypertension was strongest among blue-collar workers (OR for high job strain: 0.58; 95% CI: 0.39–0.88), weaker among white-collar workers (OR for high job strain: 0.76; 95% CI: 0.61–0.94), and not present among service workers (OR for high job strain: 0.97; 95% CI: 0.62–1.52).
Workplace Discrimination and Blood Pressure
Consistent with the analysis of job strain, workplace discrimination was unrelated to systolic blood pressure in either the bivariate or adjusted regression models (B: −0.52; 95% CI; −1.25, 0.21). Workplace discrimination was not significantly associated with relative odds of hypertension in the sample overall (Table 5). Among African Americans, those who reported experiencing discrimination more than few times per year had higher relative odds of hypertension (OR: 1.78; 95% CI: 0.68–4.68), but this association was not statistically significant. Among women, those who reported most frequent experiences of discrimination had higher odds of hypertension relative to those who never experienced discrimination (OR: 1.68; 95% CI: 1.12–2.52). Among men and Hispanics, those who reported occasional, but not frequent, experiences of discrimination had lower odds of hypertension relative to those who reported no experiences.
Job Strain, Workplace Discrimination, and Poor Blood Pressure Control
Similar to the hypertension analysis, factors associated with poor blood pressure control among workers with hypertension (N = 1,455) were being in a service-related job (OR: 1.55; 95% CI: 1.07–2.24), excessive alcohol use (OR: 1.63; 95% CI: 1.13, 2.34), and BMI (OR: 1.02; 1.00–1.04). African American (OR: 1.78; 95% CI: 1.29–2.44) and Hispanic (OR: 1.67; 95% CI: 1.07–2.63) workers were more likely to have poor blood pressure control relative to white workers. Among those with hypertension, high job strain was unrelated to poor blood pressure control (OR: 1.21; 95% CI: 0.91–1.60) in fully adjusted analyses overall or for any racial/ethnic group. Workplace discrimination was not related to poor blood pressure control overall (OR: 1.09, 95% CI: 0.70–1.69) or among any stratified group.
Sensitivity Analysis: Addressing the “Healthy Survivor” Effect
In an effort to determine whether the apparent “protective” association between job strain and hypertension was an artifact of adverse selection of workers with health problems out of high strain jobs (the “healthy survivor” effect) (Arrighi and Hertz-Picciotto 1994; Pearce et al. 2007), we repeated our analyses restricting the sample to those workers who had been at their current job for at least 5 years (N = 2,373). Consistent with the initial analysis, high job strain was associated with lower relative odds of hypertension even in the fully adjusted models (OR: 0.66; 95% CI: 0.53–0.84) relative to low job strain. Similarly, high stress plus high job satisfaction was associated with lower odds of hypertension (OR: 0.53; 95% CI: 0.40–0.70) relative to this reference. The null associations between workplace discrimination with hypertension and poor BP control were substantially unchanged in this restricted sample (data not shown).
Discussion
This is among the first studies of occupational stressors and blood pressure in older adults and one of the only studies to assess variation by race/ethnicity and gender. We found that job strain was inversely associated with hypertension, and this relationship was strongest for white and male workers. There was no overall relationship between job strain and systolic blood pressure or hypertension control, and no association between workplace discrimination and any of the blood pressure outcomes.
The lack of associations between job strain with hypertension or poor blood pressure control among African American and female workers are consistent with previous studies that have examined this relationship among racial/ethnic minorities. Both Curtis and colleagues (1997) and Albright et al. (1992) reported no relationship between job strain and hypertension among African American workers after accounting for confounding characteristics. Alves et al. (2009) also reported no relationship between job strain and hypertension among female Hispanic workers (Alves et al. 2009). The confidence intervals around the predictors of hypertension were wider for African American and Hispanic workers relative to whites, due to both the smaller sample size and potentially more variability in this outcome for these groups. It is important to note that other measures of job stress may be more salient for older minority and women workers, including work-life conflict, work spillover, or financial strain due to low-wage employment (Goldberg 2007; Fisher et al. 2009; Schulz et al. 2010), and future research should examine whether these other sources of stress are differentially associated with hypertension among older workers.
The results suggesting an inverse relationship between job strain and hypertension are somewhat counterintuitive; however, a number of previous studies have reported an inverse association between job strain, and its components, and blood pressure (Winkleby et al. 1988; Pieper et al. 1989; Albright et al. 1992; Greiner et al. 2004). There are two main potential explanations for these counterintuitive findings. The first is that bias, either in measurement of the job strain construct or in the selection of study participants, has influenced the findings. The measure of job strain we report here was derived from previously validated scales, and scores on this measure were associated with other indicators in the study in a predictable manner (e.g., workers in blue-collar and service occupations reported higher job strain than those in white-collar occupations; higher levels of workplace discrimination were associated with higher levels of job strain), suggesting that the measure has construct validity. In addition, in other work using this scale, we have shown that higher job strain is associated with increased odds of depressive symptoms (Mezuk et al. in press), consistent with the notion that higher levels of job strain are associated with worse health outcomes. Together this evidence suggests that the null findings we report here are not a general characteristic of the job strain measure but rather of the specific association between job strain and blood pressure. To account for selection bias (the “healthy survivor” effect), we reran the analyses excluding workers who had been at their present job for less than 5 years and the results did not substantially change. This suggests that premature exit from the labor force of workers from high strain jobs is not a primary explanation for the null results.
A second explanation is that the subjective appraisal and reporting of work-related stressors may be inversely related to blood pressure, such that workers with elevated blood pressure or poor blood pressure control systematically underreport the experience of job strain. This could suggest that job strain is not a valid measure of objective workplace stressors among older hypertensive workers, or it could suggest a direct relationship between suppression of the perceived stress response (e.g., coping through denial or repression of stressful experiences) and higher blood pressure (Winkleby et al. 1988; Albright et al. 1992). For example, there is evidence that underreporting of stressful experiences, including experiences of discrimination, or coping via avoidance or threat minimization is associated with higher blood pressure relative to active means of coping (Theorell and Karasek 1996; Wright and Sweeney 1989; Harrell et al. 2003). Persisting and succeeding in a high strain job may instill a sense of meaning or responsibility for older adults which may translate into better health. However, the relationship between coping styles and blood pressure has not been extensively studied in older adults and thus we can only hypothesize about the mechanisms that may be underlying these findings. Alternatively, the implication of a high strain job for health may vary as a function of the type of occupation. The post hoc analyses examining job strain within each job category (white-collar, blue-collar, service) indicate that the inverse association between job strain and hypertension was most pronounced in blue-collar occupations; as these types of occupations tend to involve more physical labor than white or service-related jobs, persisting in a blue-collar occupation after age 50 may simply be an indicator of better overall physical health. Longitudinal studies are needed to better clarify the links between job strain, workplace discrimination, and blood pressure among older workers.
Contrary to our hypothesis (Williams and Neighbors 2001), there was no association between reports of workplace discrimination and blood pressure, hypertension, or poor blood pressure control. There are several explanations for this discrepancy. First, the majority of the sample did not report experiencing workplace discrimination and thus this measure may not be sensitive enough to detect such experiences among older workers. Also, this measure did not explicitly ask about race-based discrimination but rather unfair treatment in general, which differs from previous studies of this relationship that have found significant positive relationships (Din-Dzietham et al. 2004). There was also no relationship between job strain or workplace discrimination and blood pressure control among those taking antihypertensive medications. Few studies have examined the relationship between work-related stress and blood pressure control, but previous studies have reported an association between discrimination and poor control among African Americans with hypertension (Kressin et al. 2010).
This study has a number of strengths, including the utilization of a nationally representative, ethnically and racially diverse sample of older adults and direct measurement of blood pressure. The vast majority of studies of work-related stressors have focused exclusively on younger age groups, and this study represents one of the largest studies of the influence of workplace stressors and hypertension among older adults. We also examined multiple indicators of work-related stressors, including experiences of workplace discrimination, and multiple cardiovascular indicators, including poor blood pressure control.
These findings should be interpreted in light of study limitations. Foremost, this is a cross-sectional analysis and thus we cannot infer causality of the relationship between job strain and hypertension. Second, job strain and experiences of workplace discrimination were assessed by self-report rather than through objective measures and thus these reports may be subject to recall bias. Those missing complete data on the job strain index were somewhat different than the sample analyzed here which may have influenced our results; however, for the subset of those excluded who had at least some valid data on the job strain index components, we found no evidence that those included in the analysis reported substantially different job strain than those excluded (data not shown). Finally, because the sample is limited to currently employed respondents, it is possible that those in the highest strain jobs had exited the labor force prior to the assessment of occupational stressors. However, our findings persisted when we restricted the sample to respondents who had been at their current job for at least 5 years, suggesting this “healthy survivor effect” did not substantially bias our results.
Significance
The “graying” of the workforce calls attention to the need to examine how occupations and workplace environments are related to health in later life. Increases in the retirement age, due to both cohort trends and financial strain as evidenced by the economic recession, mean that adults are working longer and thus will have more prolonged periods of exposure to work-related stressors. Racial/ethnic minorities often have qualitatively different experiences of the retirement transition than their white counterparts; however, relatively little is known about the ways in which workplace characteristics relate to health in later adulthood among these groups. Considering the paucity of research that has explored the relationship between work-related stressors and health among older workers, particularly racial/ethnic minority workers, the results presented here require replication. Overall, this study suggests that the findings from previous research on job strain and hypertension may not extend to older workers, and research is needed to better understand how workplace stressors are related to social disparities in health in later life.
References
Albright, C. L., Winkleby, M. A., Ragland, D. R., Fisher, J., & Syme, S. L. (1992). Job strain and prevalence of hypertension in a biracial population of urban bus drivers. American Journal of Public Health, 82, 984–989.
Alves, M. G. M., Chor, D., Faerstein, E., Werneck, G. L., & Lopes, C. S. (2009). Job strain and hypertension in women: Pro-Health Study. Revista de Saude Publica, 43, 1–4.
Arrighi, H. M., & Hertz-Picciotto, I. (1994). The evolving concept of the healthy worker survivor effect. Epidemiology, 5, 189–196.
Chobanian, A. V., Bakris, G. L., Black, H. R., et al. (2003). Seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension, 42, 1206–1252.
Clarke, P., & Fisher, G. (2007). Guide to content of the HRS psychosocial leave-behind participant lifestyle questionnaires: 2004 & 2006. Ann Arbor, MI: University of Michigan.
Crimmins,E., Guyer, H., Langa, K., Ofstedal, M.H., Wallace, R., Weir, D. (2008). Documentation of physical measures, anthropometrics and blood pressure in the Health and Retirement Study. February 2008, from http://hrsonline.isr.umich.edu/sitedocs/userg/dr-011.pdf.
Curtis, A. B., James, S. A., Raghunathan, T. E., & Alcser, K. H. (1997). Job strain and blood pressure in African Americans: The Pitt County Study. American Journal of Public Health, 87, 1297–1302.
de Zwart, B. H. C., Frings-Dresen, M. H., & Duivenbooden, J. C. V. (1999). Senior workers in the Dutch construction industry: A search for age-related work and health issues. Experimental Aging Research, 25(4), 385–391.
Din-Dzietham, R., Nembhard, W. N., Collins, R., & Davis, S. K. (2004). Perceived stress following race-based discrimination at work is associated with hypertension in African Americans: The metro Atlanta heart disease study, 1999–2001. Social Science and Medicine, 58, 449–461.
Egan, B. M., Zhao, Y., & Axon, R. N. (2010). US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA, 303, 2043–2050.
Fisher, G. G., Bulger, C. A., & Smith, C. S. (2009). Beyond work and family: A measure of work/nonwork interference and enhancement. Journal of Occupational Health Psychology, 14(4), 441–456.
Flippen, C., & Tienda, M. (2000). Pathways to retirement patters of labor force participation and labor market exit among the pre-retirement population by race, Hispanic origin, and sex. Journal of Gerontology Series B: Psychological Sciences, 55, S14–S17.
Gendell, M. (2008). Older workers: Increasing their labor force participation and hours of work. Monthly Labor Review, January, 41–54.
Gibson, R. (1987). Reconceptualizing retirement for black Americans. Gerontologist, 27, 691–698.
Goldberg, C. (2007). Diversity issues for an aging workforce. In S. Shultz & G. A. Adams (Eds.), Aging and work in the 21st century (pp. 51–72). Mahwah, NJ: LEA.
Greiner, B. A., Krause, N., Ragland, D., & Fisher, J. M. (2004). Occupational stressors and hypertension: A multi-method study using observer-based job analysis and self-reports in urban transit operators. Social Science and Medicine, 59, 1081–1094.
Hajjar, I., & Kotchen, T. A. (2003). Trends in prevalence, awareness, treatment and control of hypertension in the United States, 1988–2000. JAMA, 2003(290), 199–206.
Harrell, J. P., Hall, S., & Taliaferro, J. (2003). Physiologic responses to racism and discrimination: An assessment of the evidence. American Journal of Public Health, 93, 243–248.
Hendley, A. A., & Mushinski, M. (2000). The social security system: Benefit differences among racial/ethnic groups. Statistical Bulletin (Metropolitan Life Insurance Company), 81, 9–16.
Juster, F. T., & Suzman, R. (1995). An overview of the Health and Retirement Study. Journal of Human Resources, 30, S7–S56.
Karasek, R. (1979). Job demands, job decision latitude, and mental strain: Implications for job re-design. Administrative Science Quarterly, 24, 285–306.
Karasek, R. (1998). The job content questionnaire (JCQ): An instrument for internationally comparative assessments of psychosocial job characteristics. Journal of Occupational Health Psychology, 3(4), 322–355.
Kressin, N. R., Orner, M. B., Manze, M., Glickman, M. E., & Berlowitz, D. (2010). Understanding contributors to racial disparities in blood pressure control. Circulatory and Cardiovascular Quality Outcomes, 2, 173–180.
Ohlin, B., Berglund, G., Rosvall, M., & Nilsson, P. (2007). Job strain in men, but not in women, predicts a significant risk in blood pressure after 6.5 years of follow-up. Hypertension, 25, 525–531.
Pearce, N., Checkoway, H., & Kriebel, D. (2007). Bias in occupational epidemiology studies. Occupational and Environmental Medicine, 64, 562–568.
Pieper, C., LaCroix, A. Z., & Karasek, R. A. (1989). The relation of psychosocial dimensions of work with coronary heart disease risk factors: A meta-analysis of five United States databases. American Journal of Epidemiology, 29, 483–494.
Power, C., Matthews, S., & Manor, O. (1998). Inequalities in self-rated health: Explanations from different stages of life. Lancet, 351, 1009–1014.
Quinn, J. F., & Kozy, M. (1996). The role of bridge jobs in the retirement transition: Gender, race, and ethnicity. Gerontologist, 36, 363–372.
Schulz, K. S., Wang, M., Crimmins, E. M., & Fisher, G. G. (2010). Age differences in the demand-control model of work stress: An examination of data from 15 European countries. Journal of Applied Gerontology, 29(1), 21–47.
Seigrist, J. (1996). Adverse health effects of high-effort/low-reward conditions. Journal of Occupational Health Psychology, 1(1), 27–41.
Seligman, M. E. P. (1975). Helplessness: On depression, development, and health. San Francisco, CA: Freeman.
Smith, J. P., & Kington, R. (1997). Demographic and health correlates in old age. Demography, 34(1), 159–170.
St. Clair, P., Blake, D., Bugliari, D., Chien, S., Hayden, O., Hurd, M., et al. (2009). RAND HRS data documentation Version 1. HRS RAND Documentation. Ann Arbor, MI: Health and Retirement Survey.
Stansfeld, S., & Candy, B. (2006). Psychosocial work environment and mental health-—a metaanalytic review. Scandinavian Journal of Work and Environmental Health, 32, 443–462.
Szinovacz, M. E., & DeViney, S. (1999). The retiree identity: Gender and race differences. Journals of Gerontology Series B-Psychological Sciences and Social Sciences, 54, S207–S218.
Theorell, T., & Karasek, R. A. (1996). Current issues related to psychosocial job strain and cardiovascular disease research. Journal of Occupational Health Psychology, 1, 9–26.
United States Bureau of Labor. (2009). Economic and Employment Projections: 2008—2018. US Bureau of Labor. Available at: http://www.bls.gov/news.release/ecopro.t01.htm. Accessed 11 Mar 2010.
Wang, J. L., Lesage, A., Schmitz, N., & Drapeau, A. (2008). The relationship between work stress and mental disorders in men and women: Findings from a population-based study. Journal of Epidemiology and Community Health, 62, 42–47.
Wang, J. L., Schmitz, N., Dewa, C., & Stansfeld, S. (2009). Changes in perceived job strain and the risk of major depression: Results from a population-based longitudinal study. American Journal of Epidemiology, 169, 1085–1091.
Williams, D. R., & Neighbors, H. (2001). Racism, discrimination, and hypertension: Evidence and needed research. Ethnicity and Disease, 11, 800–816.
Williams, D. R., Yu, Y., Jackson, J. S., & Anderson, N. B. (1997). Racial differences in physical and mental health: Socio-economic status, stress and discrimination. Journal of Health Psychology, 2, 335–351.
Winkleby, M. A., Ragland, D. R., & Syme, S. L. (1988). Self-reported stressors and hypertension: Evidence of an inverse association. American Journal of Epidemiology, 127, 124–134.
Wright, T. A., & Sweeney, D. (1989). Coping strategies and diastolic blood pressure. Psychology Reports, 65, 443–449.
Yang, M. J., Yang, M. S., & Kawachi, I. (2001). Work experience and drinking behavior: Alienation, occupational status, workplace drinking subculture and problem drinking. Public Health, 115, 265–271.
Acknowledgments
This work was supported by a pilot study funded by the University of Michigan Center for Integrative Approaches to Health Disparities (P60 MD002249), the University of Michigan Robert Wood Johnson Health and Society Scholars Program, and the Virginia Commonwealth University Building Interdisciplinary Research Careers in Women’s Health Program (K12-HD055881). The Health and Retirement Study is sponsored by the National Institute of Aging (NIA U01AG009740) and is conducted by the University of Michigan. The sponsors had no role in the design, interpretation, or publication of this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mezuk, B., Kershaw, K.N., Hudson, D. et al. Job Strain, Workplace Discrimination, and Hypertension Among Older Workers: The Health and Retirement Study. Race Soc Probl 3, 38–50 (2011). https://doi.org/10.1007/s12552-011-9041-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12552-011-9041-7