
Abstract
Glucose is a primary energy source for most cells and an important substrate for many biochemical reactions. As glucose is a need of each and every cell of the body, so are the glucose transporters. Consequently, all cells express these important proteins on their surface. In recent years developments in genetics have shed new light on the types and physiology of various glucose transporters, of which there are two main types—sodium–glucose linked transporters (SGLTs) and facilitated diffusion glucose transporters (GLUT)—which can be divided into many more subclasses. Transporters differ in terms of their substrate specificity, distribution and regulatory mechanisms. Glucose transporters have also received much attention as therapeutic targets for various diseases. In this review, we attempt to present a simplified view of this complex topic which may be of interest to researchers involved in biochemical and pharmacological research.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Glucose is a key energy source for most living cells. Due to its polar nature and large size, glucose molecules cannot traverse the lipid membrane of the cell by simple diffusion. Instead, the entry of glucose molecules into the cells is effected by a large family of structurally related transport proteins known as glucose transporters. Two main types of glucose transporters have been identified, namely, sodium–glucose linked transporters (SGLTs) and facilitated diffusion glucose transporters (GLUTs)
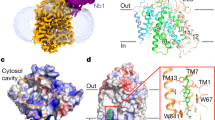
Structure of SGLTs and GLUTs.
Sodium–glucose linked transporter-1 (SGLT1) was the first SGLT to be discovered and extensively studied. It comprises 14 transmembrane helices of which both the COOH and NH2 terminals face the extracellular space. All members of the SGLT family are 60- to 80-kDa proteins containing 580–718 amino acids.
GLUTs are proteins comprising 12 membrane-spanning regions with intracellularly located amino and carboxyl terminals. The amino acid sequence of GLUT proteins has been found to show 28–65 % identity against GLUT 1. Based on this and multiple sequence alignment studies, three subclasses (Class I, II and III) of facilitative transporters have been identified.
Function/physiology of SGLTs and GLUTs
Sodium–glucose linked transporters symport (transport in the same direction) glucose in conjunction with sodium ions. SGLTs do not directly utilize ATP to transport glucose against its concentration gradient; rather, they must rely on the sodium concentration gradient generated by the sodium–potassium ATPase as a source of chemical potential. SGLTs are present on the luminal surfaces of cells lining the small intestine where they absorb glucose from dietary sources. They are also found in renal tubules where they facilitate the re-absorption of glucose from the glomerular filtrate. A summary of the main SGLT types is provided in Table 1.
Facilitative glucose transporters (GLUTs)
The GLUTs transport glucose across the plasma membrane by means of a facilitated diffusion mechanism.
Class I facilitative glucose transporters
Class I facilitative glucose transportors are represented by GLUT1 to GLUT4, among which GLUT2 is expressed mainly in beta cells of the pancreas, liver and kidney. GLUT2 acts as a glucose sensor in beta cells of marine organisms, but human beta cells express mainly GLUT1. The function of glucose sensing has two components: (1) entry of glucose into the cell mediated by GLUTs and (2) metabolism of glucose through phosporylation by glucokinase. In vitro animal and clinical studies have shown that the primary pancreatic beta cell sensor is glucokinase and not GLUT1 or GLUT2 (Efrat et al. 1994). In hepatocytes, GLUT1 is associated with the bi-directional transport of glucose controlled by hormones, such as thyroid hormone. GLUT2 on the hepatocyte membrane regulates the entry and exit of glucose to and from the cell, respectively, and as such controls hepatic glucose metabolism; in contrast GLUT2 in intestinal brush border cells and kidney tubule cells is associated with the absorption and reabsorption of glucose respectively.
GLUT3 is mainly present in the brain. It has high affinity for glucose, a property which is consistent with its function to transfer glucose into cells having a higher requirement of glucose. GLUT4 is an insulin-responsive glucose transporter that is found in the heart, skeletal muscle, adipose tissue, and brain. It is present in the cytoplasm of cells in vesicles from which it is translocated to the plasma membrane under the influence of insulin. Such insulin-directed recruitment of GLUT4 results in a 10- to 20-fold increase in glucose transport (Bryant et al. 2002).
Class II facilitative glucose transporters
This class of glucose transporters has four members, namely, GLUT5, GLUT7, GLUT9 and GLUT11. GLUT5 is primarily a fructose transporter located on cells of the small intestine, testes and kidney where it plays important physiological and pathological roles. GLUT7 has a high affinity for both glucose and fructose and is located in cells of the small intestine, colon, testis and prostate (Li et al. 2004). GLUT9, which has multiple isoforms in humans (Phay et al. 2000), is expressed mainly in the proximal tubule of the kidney and in the liver and placenta. GLUT11 closely resembles fructose transporter GLUT5 (42 % sequence homology). Three isoforms of GLUT11, namely, GLUT11A, -B and -C, have been identified in humans (Sasaki et al. 2001), with GLUT11A present in heart, skeletal muscle and kidney cells, GLUT11B present in placenta, adipose tissue and kidney cells and GLUT11C present in adipose tissue, heart, skeletal muscle and pancreas cells. Unlike GLUT5, GLUT11 facilitates the transport of both glucose and fructose. Of note, the gene for this transporter is absent from the rodent genome (Scheepers et al. 2005).
Class III facilitative transporters
There are five known Class III glucose facilitative transporters, namely, GLUT6, GLUT8, GLUT10, GLUT12 and GLUT13 (HMIT). The glycosylation site in the transporters of this class is located on loop 9, in contrast to Class I and II transporters in which it is located on loop 1 (Asano et al. 1991).
GLUT6 is mainly expressed in brain and spleen cells and in peripheral leukocytes. Godoy et al. (2006) reported that GLU8 is predominantly expressed in testis germinal cells. It is a low-affinity glucose transporter that is located intracellularly. However, its translocation to the membrane is not mediated through insulin (Lisinski et al. 2001).
GLUT8 is a high-affinity transporter of glucose, while fructose and galactose inhibit this transport. Although the translocation of GLUT8 is hormonally regulated, it is not regulated by insulin (Shin et al. 2004). It is mainly distributed brain and testis cells. It is believed to facilitate sugar transport through intracellular membranes, such as the mitochondrial membrane, endoplasmic reticular membrane and lysosomal membrane. This notion is supported by the observation of Schmidt et al. (2009) that Slc2a8 knockout mice were viable and exhibited near normal growth, although mild alterations in cells of the brain, heart and sperm were evident. The sperm cells of these mice had reduced ATP levels and low motility (Schmidt et al. 2009).
GLUT10 is located in cells of tissues—for example, skeletal muscle, heart, lung, brain, placenta, kidney, liver and pancreas. GLU12 is expressed in cells of adipose tissue, small intestine, skeletal muscle and placenta. It exhibits sequence similarity with GLUT10, but in many respects it resembles GLUT4. Similar to GLUT4, insulin is able to induce translocation of GLUT12 to the cell membrane in skeletal muscle (Stuart et al. 2009). However, a recent study using isolated cardiomyocytes of healthy and T1DM rodents showed that GLUT12 expression on the surface of cardiomyocytes is not insulin dependent, indicating a role of basal glucose transporter for GLUT12 (Waller et al. 2013).
HMIT (H+-driven myoinositol transporter) or GLUT13 is expressed in adipose tissue and kidney cells. It is also predominantly expressed in the brain, especially in the hippocampus, hypothalamus, cerebellum and brain stem. It is mainly located intracellularly, and its translocation occurs by depolarization or protein kinase C activation in neuronal cells (Uldry and Thorens 2004). Distinct from other GLUTs, this transporter is associated with the transport of inositol-3-phosphate. In the brain, myo-inositol is the precursor of phosphotidyl inositol, which is an important regulator of various signaling pathways. Deregulation in this pathway has been shown to be associated with various psychiatric disorders (e.g. bipolar disorder).
Diseases associated with SGLTs and GLUTs
Genetic variations in SGLT1 that cause defective SGLT1 protein result in an autosomal recessive disorder called glucose–galactose malabsorption. This disorder is characterized by severe watery diarrhea on oral administration of lactose, glucose or galactose. SGLT2, which is the main glucose transporter in kidney tubules, reabsorbs glucose from glomerular filtrate. In individuals with a genetic defect in the SGLT2 gene this reabsorption of glucose is impaired, leading to he excretion of high concentrations of glucose in urine. Mutation of this gene is associated with altered transforming growth factor beta 1 activity and arterial tortuosity syndrome (ATS) characterized by connective tissue disorders, with elongation and tortuosity of the major arteries (e.g. the aorta), skin and joint abnormalities, micrognathia and elongated face (Lin et al. 2006).
The activity of SGLT is increased threefold in the brush border membrane vesicles of the intestine of diabetic subjects, with the potential for an increased capacity of glucose absorption in diabetic subjects (Dyer et al. 2002). Cardiac sarcolemmal SGLT1 expression, which is mediated through leptin, was found to be increased in Type 2 diabetes mellitus (T2DM) and ischemia and decreased in Type 1 DM (T1DM). These SGLT1 levels were found to be correlated to insulin levels. Insulin stimulates SGLT1 activity mediated through protein kinase C activation, which in turn leads to the recruitment of SGLT1 to the plasma membrane. Increased levels of SGLT1 lead to increased uptake of glucose in cardiomyocytes of T2DM patients (Banerjee et al. 2009).
Glucose present in bile is reabsorbed later in intrahepatic bile ducts by SGLT1 and GLUT1. This reabsorbed glucose provides an osmotic gradient for the movement of water from bile, thus reducing bile volume. Due to their higher blood sugar concentration, diabetic patients also have high bile glucose concentrations. An increase in glucose transport causes a reduction in bile flow and vice versa, which likely explains the low bile secretion observed in diabetic subjects (Lazaridis et al. 1997).
SGLT1 is expressed in epithelial cells of salivary glands and is responsible for reabsorbing ductal water and reducing the amount of water and saliva which is secreted. Increased SGLT1 expression has been observed in the luminal membrane of salivary gland ductal cells of diabetic and hypertensive animals, leading to the proposal that this increase in SGLT1 expression results in reduced salivary flow in diabetic and hypertensive subjects, which in turn increases their proneness for oral complications (Sabino-Silva et al. 2009).
Some studies have indicated an immunological protective role of SGLT1 in gastrointestinal infections. Palazzo et al. (2008) reported that mice given oral glucose demonstrated complete protection against a lethal dose of endotoxin. This protective effect of SGLT1 was observed to be mediated through the anti-inflammatory cytokine interleukin-10.
GLUT2 gene mutations may result in severe Fanconi–Bickel Syndrome characterized by fasting hypoglycemia, postprandial hyperglycemia, elevated cholesterol level, hepatorenal glycogen accumulation leading to hepatomegaly, proximal renal tubular dysfunction and dwarfism (De Vos et al. 1995).
Insulin resistance in T2DM is characterized by decreased ability of the skeletal muscle cells to utilize extracellular glucose. GLUT4 levels were found to be normal in skeletal muscles of such patients, indicating that it their translocation to membrane which is impaired, possibly due to a defect in insulin signaling mechanism or abnormal accumulation of GLUT4 in the membrane compartments (Garvey et al. 1998).
Recent years has seen increasing amounts of fructose being added to many foods, and this trend has resulted in researchers focusing on the role of fructose and its transporters in diseases such as DM, obesity, hypertension and nonalcoholic fatty liver disease. In T2DM, the synthesis of GLUT5 mRNA is stimulated and the abundance of GLUT5 protein is increased in skeletal muscle; the opposite trend occurs in adipose tissue. This effect can be reversed by pioglitazone. Obesity as well as hypoxia stimulates the expression and activity of GLUT5 in adipose cells. Hypertension causes an increase in the expression and activity of GLUT5 in the kidney, but decreases in the small intestine. Gastrointestinal infection and inflammation decrease the expression and activity of GLUT5 in the small intestine (Douard and Ferraris 2008). Three isoforms of GLUT9 were observed to be upregulated in diabetic mice (Keembiyehetty et al. 2006). The gene for GLUT10 is located on chromosome 20 at a known T2DM locus. However, different studies have failed to prove any correlations between T2DM and GLUT10 polymorphism.
Disease treatments that exploit GLUTs and SLGTs
The excessive growth of malignant cells of a tumor requires high energy, which comes in the form of glucose. Isselbacher (1972) showed that there is an overexpression of glucose transporters in several types of tumor cells. One proposal is that the evasion of apoptosis in tumor cells is due to stabilization of SGLT1 on the tumor cell membrane by epidermal growth factor receptor (EGFR). This proposal led to the development of a novel chemotherapeutic strategy in which the cytotoxic drug was linked to D-glucose, resulting in better penetration of the drug into the tumor cell. Another approach is to inhibit glucose transport through glucose transporter into the tumor cell. D-Allose, a rare sugar, has been shown to interfere with D-glucose transport in head and neck carcinomca cells, thus inhibiting their growth (Mitani et al. 2009). Antisense oligonucleotides against GLUT5, which can block expression of GLUT5 in tumor cells, were found to reduce cell proliferation in two breast cancer cell lines MCF-7 and MDAMB-231 (Chan et al. 2004). GLUT11, GLUT4 and GLUT8 have also been found to play important roles in the growth of malignant cells of multiple myeloma and have been proposed as important therapeutic targets (McBrayer et al. 2012).
As SGLT1 plays an important role in secretary diarrhea, this mechanism is used to prevent dehydration by oral rehydration therapy (ORT). It is estimated that one adult patient may require 80 L of intravenous fluid over 5 days to prevent dehydration. This nearly impossible goal can be achieved simply by giving an oral solution of sodium chloride–glucose. The glucose is absorbed along with two sodium ions through the SGLT and water will follow by osmosis. It was this knowledge which led the WHO/UNICEF to recommend a new formulation of oral rehydration salts for use in ORT.
SGLT2 is also a potential target for the treatment of DM. A novel approach in DM treatment is to reduce blood glucose levels by increasing its excretion through the kidney. Glucose in tubules is reabsorbed through SGLT2; thus, inhibiting SGLT2-mediated reabsorption would lead to the excretion of higher levels of glucose in the urine. Phlorizin (an inhibitor of SGLT2) has shown to reduce blood sugar levels in diabetic animals without producing hypoglycemia. The first drug of this class, Dapagliflozin, developed by AstraZeneca Pharmaceuticals, was approved by the U.S. Federal Drug Administration on 8 January 2014 for use in T2DM patients.
Conclusion
The significance of glucose transporters in biology is apparent as they are the gateways to one of the most important molecules of life, namely, glucose. Apart from its role in normal physiology, glucose is the central culprit in diseases such as DM mellitus. Concomittant with advances in DM therapeutics is the continuing search for innovative approaches for blood sugar control. The role(s) of glucose transporters will become more and more prominent as new antidiabetic drugs are approved and become available in the clincal setting. Drugs targeted against glucose transporters are also potential anticancer agents.
References
Asano T, Katagiri H, Takata K, Lin JL, Ishihara H, Inukai K et al (1991) The role of N-glycosylation of GLUT1 for glucose transport activity. J Biol Chem 266:24632–24636
Banerjee SK, McGaffin KR, Pastor-Soler NM, Ahmad F (2009) SGLT1 is a novel cardiac glucose transporter that is perturbed in disease states. Cardiovasc Res 84:111–118
Bryant NJ, Govers R, James DE (2002) Regulated transport of the glucose transporter GLUT4. Nat Rev Mol Cell Biol 3:267–277
Chan KK, Chan JY, Chung KK, Fung KP (2004) Inhibition of cell proliferation in human breast tumor cells by antisense oligonucleotides against facilitative glucose transporter 5. J Cell Biochem 93:1134–1142
De Vos A, Heimberg H, Quartier E, Huypens P, Bouwens L, Pipeleers D et al (1995) Human and rat beta cells differ in glucose transporter but not in glucokinase gene expression. J Clin Invest 96:2489–2495
Douard V, Ferraris RP (2008) Regulation of the fructose transporter GLUT5 in health and disease. Am J Physiol Endocrinol Metab 295:E227–E237
Dyer J, Wood IS, Palejwala A, Ellis A, Shirazi-Beechey SP (2002) Expression of monosaccharide transporters in intestine of diabetic humans. Am J Physiol Gastrointest Liver Physiol 282:G241–G248
Efrat S, Leiser M, Wu YJ, Fusco-DeMane D, Emran OA, Surana M et al (1994) Ribozyme mediated attenuation of pancreatic β-cell glucokinase expression in transgenic mice results in impaired glucose-induced insulin secretion. Proc Natl Acad Sci USA 91:2051–2055
Garvey WT, Maianu L, Zhu JH, Brechtel-Hook G, Wallace P, Baron AD (1998) Evidence for defects in the trafficking and translocation of GLUT4 glucose transporters in skeletal muscle as a cause of human insulin resistance. J Clin Invest 101:2377–2386
Godoy A, Ulloa V, Rodríguez F, Reinicke K, Yañez AJ, García M et al (2006) Differential subcellular distribution of glucose transporters GLUT1–6 and GLUT9 in human cancer: Ultrastructural localization of GLUT1 and GLUT5 in breast tumor tissues. J Cell Physiol 207:614–627
Isselbacher KJ (1972) Sugar and amino acid transport by cells in culture—differences between normal and malignant cells. N Engl J Med 286:929–933
Keembiyehetty C, Augustin R, Carayannopoulos MO, Steer S, Manolescu A, Cheeseman CI et al (2006) Mouse glucose transporter 9 splice variants are expressed in adult liver and kidney and are up-regulated in diabetes. Mol Endocrinol 20:686–697
Lazaridis KN, Pham L, Vroman B, De Groen PC, LaRusso NF (1997) Kinetic and molecular identification of sodium-dependent glucose transporter in normal rat cholangiocytes. Am J Physiol Gastrointest Liver Physiol 272:G1168–G1174
Li Q, Manolescu A, Ritzel M, Yao S, Slugoski M, Young JD et al (2004) Cloning and functional characterization of the human GLUT7 isoform SLC2A7 from the small intestine. Am J Physiol Gastrointest Liver Physiol 287:G236–G242
Lin WH, Chuang LM, Chen CH, Yeh JI, Hsieh PS, Cheng CH et al (2006) Association study of genetic polymorphisms of SLC2A10 gene and type 2 diabetes in the Taiwanese population. Diabetologia 49:1214–1221
Lisinski I, Schurmann A, Joost HG, Cushman SW, Al-Hasani H (2001) Targeting of GLUT6 (formerly GLUT9) and GLUT8 in rat adipose cells. Biochem J 358:517–522
McBrayer SK, Cheng JC, Singhal S, Krett NL, Rosen ST, Shanmugam M (2012) Multiple myeloma exhibits novel dependence on GLUT4, GLUT8, and GLUT11: implications for glucose transporter-directed therapy. Blood 119:4686–4697
Mitani T, Hoshikawa H, Mori T, Hosokawa T, Tsukamoto I, Yamaguchi F et al (2009) Growth inhibition of head and neck carcinomas by D‐allose. Head Neck 31:1049–1055
Palazzo M, Gariboldi S, Zanobbio L, Selleri S, Dusio GF, Mauro V et al (2008) Sodium-dependent glucose transporter-1 as a novel immunological player in the intestinal mucosa. J Immunol 181:3126–3136
Phay JE, Hussain HB, Moley JF (2000) Strategy for identification of novel glucose transporter family members by using internet-based genomic databases. Surgery 128:946–519
Sabino-Silva R, Freitas HS, Lamers ML, Okamoto MM, Santos MF, Machado UF (2009) Na+-glucose cotransporter SGLT1 protein in salivary glands: potential involvement in the diabetes-induced decrease in salivary flow. J Membr Biol 228:63–69
Sasaki T, Minoshima S, Shiohama A, Shintani A, Shimizu A, Asakawa S et al (2001) Molecular cloning of a member of the facilitative glucose transporter gene family GLUT11 (SLC2A11) and identification of transcription variants. Biochem Biophys Res Commun 289:1218–1224
Scheepers A, Schmidt S, Manolescu A, Cheeseman CI, Bell A, Zahn C et al (2005) Characterization of the human SLC2A11 (GLUT11) gene: alternative promoter usage, function, expression, and subcellular distribution of three isoforms, and lack of mouse orthologue. Mol Membr Biol 22:339–351
Schmidt S, Joost HG, Schurmann A (2009) GLUT8, the enigmatic intracellular hexose transporter. Am J Physiol Endocrinol Metab 296:E614–E618
Shin BC, McKnight RA, Devaskar SU (2004) Glucose transporter GLUT8 translocation in neurons is not insulin responsive. J Neurosci Res 75:835–844
Stuart CA, Howell ME, Zhang Y, Yin D (2009) Insulin-stimulated translocation of glucose transporter (GLUT) 12 parallels that of GLUT4 in normal muscle. J Clin Endocrinol Metab 94:3535–3542
Uldry M, Thorens B (2004) The SLC2 family of facilitated hexose and polyol transporters. Pflügers Archiv 447:480–489
Waller AP, George M, Kalyanasundaram A, Kang C, Periasamy M, Hu K et al (2013) GLUT12 functions as a basal and insulin-independent glucose transporter in the heart. BBA-Mol Basis Dis 1832:121–127
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Archana M. Navale declares that she has no conflict of interest.
Archana N. Paranjape declares that she has no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Navale, A.M., Paranjape, A.N. Glucose transporters: physiological and pathological roles. Biophys Rev 8, 5–9 (2016). https://doi.org/10.1007/s12551-015-0186-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12551-015-0186-2