
Abstract
Background
The aim of this study was to determine the frequency and etiology of maxillary sinus retention cysts (RCs) in a Turkish patient population in the Middle Black Sea region by using panoramic radiography.
Material and methods
We retrospectively reviewed 9,659 panoramic radiographs that were taken from March 2012 to January 2014. The number, location, and the size of the RCs as well as the age, gender, dental status, and radiographic dental findings of the patients were recorded.
Results
Of the 9,659 patients, 158 had RCs with a frequency of 1.6 %. Male patients had significantly more RCs than female patients did (p < 0.001). RCs were mostly seen in patients aged between 30 and 39 years and no significant difference was found between age groups. We detected 169 RCs in the 158 patients. Of these patients, 147 were dentate and 11 were edentulous. Moreover, 39 % of the patients had dental findings in the adjacent teeth to the maxillary sinus. The size of the RCs measured on panoramic radiographs ranged from 0.8 to 9.5 cm2 with a mean of 3.7 cm2.
Conclusion
This study shows that the prevalence of RCs is low (1.6 %) and the frequency of RCs diminishes slightly with age. Most of the patients that had RCs were dentate, and dental findings were observed in around 50 % of the patients. Therefore, dental pathology may be considered to be a contributing factor for RCs. According to the findings of our study, the size and prevalence of RCs are not age dependent.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Retention cysts (RCs) are common incidental and asymptomatic findings of the paranasal sinuses and occur mostly in the maxillary sinus [1–3]. The reported incidence of RCs in the maxillary sinus is 1.4–9.6 % in the general population [4–7]. These cysts originate from the obstruction of a duct of a seromucinous gland of the sinus mucosa, resulting in cystic dilatation of the gland by the accumulated mucus [5]. On radiographs, cysts usually have the appearance of a round, ovoid, or dome-shaped shadow [8–11] of uniform density within the maxillary sinus in continuity with the floor or the wall of the sinus [11]. The reported size of the cysts varies from the size of a grass seed to the size of a walnut [12]. The etiology of these cysts is still not clear [3, 7, 13], but they have been strongly associated with allergic, inflammatory, and infectious processes [14, 15]. In some cases, barotrauma has been considered to be a factor contributing to the development of RCs [2, 15]. There have also been studies reporting that high humidity and air pollution might be associated with their occurrence [14].
RCs in the maxillary sinus are generally asymptomatic and do not need treatment [16]. They usually rupture and clear up spontaneously [6, 13, 17, 18] at the rate of 16–41 % [13]. However, occasionally they might be related to a variety of symptoms such as headache or facial pain in the frontal, orbital, or nasal area, nasal discharge, nasal obstruction, and sinusitis [19]. In the presence of such symptoms, management of RCs is surgical. Punction and aspiration through the inferior meatus or natural ostium or removal via the Caldwell–Luc approach are the procedures used for treatment. Endoscopic intranasal sinus surgery is another procedure of choice for the treatment of RCs of the maxillary sinus [5].
The aim of this retrospective study was to determine the frequency and characteristics of maxillary sinus RCs in a Turkish patient population in the Middle Black Sea region.
Material and methods
The present study was carried out in a retrospective manner using 9,659 panoramic radiographs of patients who presented to our Oral and Maxillofacial Surgery Services of the Dentistry Faculty, Ordu University, between March 2012 and January 2014. Regardless of gender, patients aged between 10 and 90 years were included in the study. Radiographs of poor quality, which hinder accurate diagnosis, and radiographs of patients under 10 year of age,in whom the formation of the sinuses is still incomplete, were excluded from the study. The number, location, and size of the RCs as well as the age, gender, dental status, and dental findings of the patients were recorded.
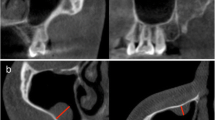
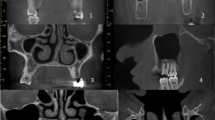
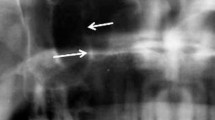
The panoramic radiographs were obtained using the Kodak 8000C Digital Panoramic and Cephalometric Extraoral Imaging System (Kodak Dental Systems, Rochester, NY) and images were stored in a digital database. The criterion for radiographic detection of RCs on panoramic radiographs was a radiopaque dome-shaped or hemispherical image seen on the wall or floor of the maxillary sinus (Fig. 1). All radiographic images were reviewed and discussed by one group of researchers to determine the presence and localization of the RCs as well as the dental findings of the patients. The size of RCs was measured by using a digital archiving system (Turcasoft Dent, Samsun, Turkey; Fig. 2). Acquired data were recorded and classified for statistical analysis.

A panoramic radiograph showing the typical appearance of a retention cyst in the right maxillary sinus (arrows)

Measurement of a retention cyst on a panoramic radiograph
All descriptive and comparative statistical analyses were performed using the SPSS software package (Statistical Package for Social Sciences, version 11.0, SPSS Inc., Chicago, Ill.). Normally distributed continuous data (cyst size) are expressed as sample size and mean values with standard deviation, and were analyzed by using one-way ANOVA for the age groups. Categorical data are expressed as sample size and proportions. Cross-tabulated data were analyzed with the chi-square test. The Z test was used to determine any further differences between the ratios for the different age groups. A probability value of p < 0.05 was considered as significant.
Results
RCs were observed in 158 patients (94 male and 64 female patients) with a frequency of 1.6 %. Patients ranged in age from 10 to 78 years with a mean of 33 years. Male patients showed significantly more RCs than female patients (Table 1). The highest number of RCs was found for the group aged between 30 and 39 years, but no statistically significant differences were found between the various age groups (Fig. 3). Regarding the location, 80 (47 %) of the RCs were found in the right sinus and 67 (39 %) in the left sinus The prevalence of RCs according to location showed no significant difference across the study population but the prevalence of RCs regarding side of location showed a significant difference in the age groups of 30–39 and 40–49 years, with a slight predominance in the right side. In 11 (6.5 %) patients, RCs were found bilaterally. The majority of RCs were located on the floor of the maxillary sinus. Of the 158 patients, 147 were dentate and 11 were edentulous. Dental findings below the RCs were noted in 39 % of patients. The size of the RCs measured on panoramic radiographs ranged from 0.8 to 9.5 cm2 with a mean of 3.7 cm2. No significant correlation was found between the size of the RCs and age (Fig. 4; p = 0.011). According to the results of the present study, the prevalence of RCs diminishes slightly with age while the mean size of RCs increases with age. Demographic and radiographic data are shown in Table 2.

Distribution of retention cysts according to age group

Relationship between cyst size and age group
Discussion
RCs are incidental findings that are commonly encountered in the maxillary sinus on routine radiographs [1–3]. It is well established that a majority of RCs are detected on the floor of the maxillary sinus [5, 11, 19]. However, these lesions may also be detected on the lateral, posterior, medial, or superior walls of the maxillary sinus [5]. Bhattacharyya [3] detected 13.3 % of RCs on the medial wall in his study. The correlation between RCs and the floor of the maxillary sinus was associated with gravity and good visualization of this region with panoramic radiography [7, 20]. Moreover, the proximity between roots with periapical lesions and the floor of the sinuses is considered to elevate the risk of RC occurrence [20, 21]. Similarly, in our study RCs were mostly detected on the floor of the maxillary sinus. According to Donizeth-Rodrigues et al. [13], panoramic radiography is still used as a routine screening tool for the evaluation of the sinuses, despite its limitations. However, Balaji et al. [22] reported that a well-suited imaging modality for the craniofacial area is cone beam computed tomography (CBCT).
RCs are usually present in the second or third decade of life [13, 23, 24] and are fairly rare in childhood [19]. Rodrigues et al. [14] detected 201 RCs in 6,293 radiographs and most of the subjects were in the second and third decade of life. Similarly, in another study reported by Halstead [25], a higher prevalence of RCs was seen in the third decade of life among a dental school clinic population. The presence of RCs in children was associated with the development stage of the paranasal sinuses [13, 19]. For this reason, RCs are rarely seen in childhood because of the incomplete development of the paranasal sinuses [19]. RCs were found more frequently in male patients, and the reported male-to-female ratio is approximately 2:1 [4, 5, 13, 26]. We found the male-to-female ratio to be 1.5:1 (94 male and 64 female patients). According to Vallo et al. [20], the reason for RCs being detected more frequently in men was that the men under investigation were exposed to respiratory infections more often than women were, especially during their national service. We believe that the claim by Vallo et al. might be valid, as there was also a male predominance in the present study of a Turkish population in the Middle Black Sea region.
The prevalence of RCs differs widely in published studies and the reported incidence decreases gradually with age [5, 23]. Although the reported prevalence of RCs varies from 1.4 to 9.6 % on panoramic radiographs and occipitomental views in most of the documented studies [27], MacDonald-Jankowski [28] reported that the prevalence of RCs was 14 % in his study using panoramic radiographs. Bhattacharyya [3] also reported a prevalence of RCs of 12.4 % using CT scans in another study. This variation among findings in various studies may be associated with the differences in the geographic origin of the study groups or the sensitivity of the imaging methods used in the studies. Our results are consistent with most of the previous studies in the literature. However, it is one of the lowest documented ratios, similar to the one reported by Casamassimo and Lilly [24]:1.6 % [3, 11, 12, 20].
A predominance for both the right [13, 28] and the left side of the maxillary sinus [25, 29] has been shown. Casamassimo and Lilly [24] reported that allergic or rhinogenic factors frequently lead to a bilateral occurrence of the cysts. And according to Bjorn et al. [30], usually odontogenic factors cause unilateral sinus involvement and unilateral occurrence of RCs. In most of the patients, we observed radiographic dental findings on the same side as the RCs. Hence, according to our findings we believe that dental pathologies may contribute to the unilateral development of RCs.
The reported size of RCs is in the range of 1.0–15 cm2 [28]. In our study, the size of the cysts ranged from 0.8 to 9.5 cm2 with the mean of 3.7 cm2 on panoramic radiographs. Wang et al. [5] found the mean size of RCs to be 3.0 cm2 on occipitomental views. Albu [2] hypothesized that the greater the size of a cyst, the more pronounced the symptoms, but he found no correlation. Generally, RCs are symptomless and remain unchanged but occasionally they may resolve completely [14]. Approximately 60 % of RCs have been reported to remain about the same size, whereas fewer than 25 % either decrease in size or completely disappear [5]. Wang et al. [5] stated that if the RC has increased significantly in size after 48 months, it is likely to increase further and should be kept under observation. In addition, Casamassimo and Lilly [24] reported that there was no association between the age of the patients and the cyst size, as found in our study group.
RCs are generally asymptomatic but they occasionally give rise to different types of discomfort, such as headache and facial pain [7, 31], postnasal drip and nasal discharge [17, 29], toothache [32], and ocular complaints [28, 33, 34]. However, in most cases RCs remain untreated. The patient should be informed about the presence of the lesion and advised to seek care if any symptoms develop [6].
In conclusion, this study provides information about the prevalence of RCs in a Turkish patient population. According to the findings of our study, dental pathology may be considered a contributing factor for RCs, and the size/prevalence of RCs is not age dependent.
Conflict of interest
M.M. Omezli, D. Torul, and S. Cankaya state that there are no conflicts of interests.
References
Hoang JK, Smith EC, Barboriak DP. Ruptured maxillary retention cyst: cause of unilateral rhinorrhea after trauma. AJNR Am J Neuroradiol. 2009;30:1121–2.
Albu S. Symptomatic maxillary sinus retention cysts: should they be removed? Laryngoscope. 2010;120:1904–9.
Bhattacharyya N. Do maxillary sinus retention cysts reflect obstructive sinus phenomena? Arch Otolaryngol Head Neck Surg. 2000;126:1369–71.
Ruprecht A, Batniji S, el-Neweihi E. Mucous retention cyst of the maxillary sinus. Oral Surg Oral Med Oral Pathol. 1986;62:728–31.
Wang JH, Jang YJ, Lee BJ. Natural course of retention cysts of the maxillary sinus: long-term follow-up results. Laryngoscope. 2007;117:341–4.
MacDonald A, Newton CW. Pseudocyst of the maxillary sinus. J Endod. 1993;19:618–21.
Allard RH, van der Kwast WA, van der Waal I. Mucosal antral cysts. Review of the literature and report of a radiographic survey. Oral Surg Oral Med Oral Pathol. 1981;51:2–9.
Kım YS, An YK, Lee SK. Pathological findings for mucous retention cyst in maxillary sinus. Kor J Oral Maxillofac Pathol. 2010;34:9–18.
Ramesh A, Pabla T. Mucous retention cyst of maxillary sinuses. Oral Maxillofacial Radiol. 2008;57:14–5.
Whyte A, Chapeikin G. Opaque maxillary antrum: a pictorial review. Australas Radiol. 2005;49:203–13.
Ohba T. Value and limitation of panoramic radiography in the diagnosis of maxillary sinus pathosis. Int J Oral Surg. 1977;6:211–4.
Bosio JA, Tanaka O, Rovigatti E, de Gruner SK. The incidence of maxillary sinus retention cysts in orthodontic patients. World J Orthod. 2009;10:e7–8.
Donizeth-Rodrigues C, Fonseca-Da Silveira M, Goncalves-De Alencar AH, Garcia-Santos-Silva MA, Francisco-De-Mendonca E, Estrela C. Three-dimensional images contribute to the diagnosis of mucous retention cyst in maxillary sinus. Med Oral Patol Oral Cir Bucal. 2013;18:e151–7.
Rodrigues CD, Freire GF, Silva LB, Fonseca da Silveira MM, Estrela C. Prevalence and risk factors of mucous retention cysts in a Brazilian population. Dentomaxillofac Radiol. 2009;38:480–3.
Harar RP, Chadha NK, Rogers G. Are maxillary mucosal cysts a manifestation of inflammatory sinus disease? J Laryngol Otol. 2007;121:751–4.
Chan HL, Wang HL. Sinus pathology and anatomy in relation to complications in lateral window sinus augmentation. Implant Dent. 2011;20:406–12.
Hadar T, Shvero J, Nageris BI, Yaniv E. Mucus retention cyst of the maxillary sinus: the endoscopic approach. Br J Oral Maxillofac Surg. 2000;38:227–9.
Soikkonen K, Ainamo A. Radiographic maxillary sinus findings in the elderly. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;80:487–91.
Rahnama M, Czupkallo L, Czajkowski L, Czajkowska W, Kozıcka-Czupkallo M. Mucous retention cyst of the maxillary sinus—minimally invasive treatment with use of piezosurgery. Case report. Curr Issues Pharm Med Sci. 2012;25:49–52.
Vallo J, Suominen-Taipale L, Huumonen S, Soikkonen K, Norblad A. Prevalence of mucosal abnormalities of the maxillary sinus and their relationship to dental disease in panoramic radiography: results from the Health 2000 Health Examination Survey. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:e80–7.
Schalek P, Otruba L, Hornackova Z, Hahn A. Mucosal maxillary cysts: long-term subjective outcomes after surgical treatment. Eur Arch Otorhinolaryngol. 2013;270:2263–6.
Balaji SM, Krishnaswamy NR, Kumar MS, Rooban T. Inferior alveolar nerve canal position among South Indians: a cone beam computed tomographic pilot study. Ann Maxillofac Surg. 2012;2:51–5.
Fukuta Y, Satoh H, Totsuka M. Dome-shaped radiopacities in the maxillary sinus on panoramic radiographs: a clinical and radiological study. Asian J Oral Maxillofac Surg. 2002;14:139–43.
Casamassimo PS, Lilly GE. Mucosal cysts of the maxillary sinus: a clinical and radiographic study. Oral Surg Oral Med Oral Pathol. 1980;50:282–6.
Halstead CL. Mucosal cysts of the maxillary sinus: report of 75 cases. J Am Dent Assoc. 1973;87:141–3.
Myall RW, Eastep PB, Silver JG. Mucous retention cysts of the maxillary antrum. J Am Dent Assoc. 1974;89:1338–42.
Mardinger O, Manor I, Mijiritsky E, Hirshberg A. Maxillary sinus augmentation in the presence of antral pseudocyst: a clinical approach. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:180–4.
MacDonald-Jankowski DS. Mucosal antral cysts observed within a London inner-city population. Clin Radiol. 1994;49:195–8.
Lilly GE, Cutcher, JL, Steiner M. Spherical shadows within the maxillary antrum. J oral Med. 1968;23:19–21.
Bjorn H, Holmberg K, Nylander G. Maxillary sinus in periodontal disease—a clinical and radiographic investigetion. Odontol Revy. 1967;18:83–110.
Paparella MM. Mucosal cyst of the maxillary sinus: diagnosis and management. Arch Otolaryngol. 1963;77:650–70.
Alberti PW. Applied surgical anatomy of the maxillary sinus. Otolaryngol Clin North Am. 1976;9:3–20.
Ence BK, Parsons DS. Mucous retention cyst causing pain of the infraorbital nerve. Otolaryngol Head Neck Surg. 1990;103:1031–4.
Bret-Day RC. Secretory cyst of the maxillary antrum presenting with oral symptoms. Br Dent J. 1960;109:269–70.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Omezli, M., Torul, D. & Cankaya, S. Frequency and characteristics of retention cysts in the maxillary sinus in a Turkish patient population. J. Stomat. Occ. Med. 8, 17–21 (2015). https://doi.org/10.1007/s12548-015-0120-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12548-015-0120-z