
Abstract
Purpose
This study drew upon the ecological system theory to demonstrate rural-urban differences in the relationships between the availability of recreational facilities, physical activity (PA), functional health status, and depressive symptoms in middle-aged and older Chinese adults.
Methods
Nationally representative data (n = 5949) from the Chinese Health and Retirement Longitudinal Study (CHARLS, 2011–2013) were examined using the multigroup structural equation modeling approach.
Results
The results suggest that higher availability of recreational facilities in the urban communities was associated with higher levels of leisure time physical activity (LTPA), better functional capacity, and less occurrence of depressive symptoms among urban participants. In contrast, LTPA engagement among rural participants was low and had negligible mitigating effects on functional decline and depressive symptoms. The findings also show that functional health status mediated the association between total PA and depressive symptoms in both rural and urban participants. However, high levels of total PA were directly associated with elevated depressive symptoms, suggesting that the context of PA and related socioeconomic factors might explain this association after the non-LTPA components were included.
Conclusions
The findings highlight how complex patterns of intrapersonal, behavioral, and environmental correlates influence depressive symptoms in middle-aged and older Chinese adults. The context of PA should be considered when creating targeted strategies to prevent depressive symptoms. As an inactive lifestyle evolves with China’s rapid urbanization, joint efforts from public health and urban planning should be made to promote LTPA and develop active living communities for achieving optimal health in later life.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Depression is a serious public health problem and one of the leading causes of disease burden worldwide [1]. As the aging population grows in China, the socioeconomic costs of depression in later life are vast, given that depressive symptoms are common and often neglected among Chinese elderly [2]. Depressive symptoms are associated with physical and cognitive functioning declines that accompany aging [3], and functional decline may be more common in depressed older Chinese adults than those that are non-depressed [4]. Although functional health has substantially improved among older adults in some regions [5], functional disability is still a formidable challenge in China, especially in underdeveloped rural areas. Thus, understanding the mitigating mechanism of depressive symptoms is critical for promoting healthy aging.
Physical activity (PA) offers numerous physiological and psychological benefits including reduced depressive symptoms [6] and better functional health [7], which may improve the quality of retirement life. A systematic review highlighted that regular PA reduced the risk of functional limitations and delayed the onset of limitation in instrumental activities of daily living (IADLs) among older adults [8]. While many studies focused on walking and leisure time physical activity (LTPA), the influences of PA within different contexts (LTPA and non-LTPA) on health have seldom been reported, and thus warrant careful scrutiny.
The built environment may exert both direct and indirect impacts on PA behavior and health outcomes [9]. Convenient access to recreational facilities has been shown to promote LTPA engagement and was positively associated with other forms of PA such as walking to and from the facilities [10]. A recent review summarized that non-park PA facilities were among the most significant environmental correlates of PA among adults in major cities of China [11]. However, non-uniform socioeconomic developments between rural and urban communities in China may result in barriers to access recreational facilities in residents of underdeveloped communities. Unfortunately, there is a paucity of research examining the potential rural-urban heterogeneity with respect to the environmental impacts on PA behavior and health outcomes among older adults residing in rural and urban communities.
To address the research gaps, this study drew upon the ecological system theory [12] to elucidate the interrelationships between the availability of recreational facilities, PA, functional health status, and depressive symptoms among middle-aged and older Chinese adults. According to the ecological system theory [12], an individual is surrounded by different personal, social, and environmental factors within the overlapping layers of the ecological system, known as the microsystem, mesosystem, exosystem, macrosystem, and chronosystem. The microsystem includes personal behaviors, interpersonal relations, and interaction patterns with immediate surroundings. The outer-layer mesosystem indicates linkages between two or more settings containing the outcome variables. While the exosystem does not contain the outcomes directly, it does affect them indirectly. The macrosystem further describes the broader systems of culture and beliefs, and the chronosystem displays longitudinal markers and systems of time [12, 13].
In this study, the availability of recreational facilities and PA behaviors (LTPA and total PA) were microsystem variables, which had a direct influence on intrapersonal variables (functional health status and depressive symptoms). The interrelationships of theses microsystem variables were formed the mesosystem (Fig. 1). This theoretical structure was subsequently fitted into rural and urban macrosystems. The multigroup structural equation modeling approach was used to examine the rural-urban moderating effect on the interrelationships between the variables of interest. We hypothesized that high availability of recreational facilities promoted participation in LTPA and total PA, which in turn prevented functional decline, and alleviated depressive symptoms in middle-aged and older Chinese adults. In addition, we expected to find rural and urban differences in the examined interrelationship patterns.

Hypothesized model within rural and urban macrosettings. PA physical activity, LTPA leisure time physical activity. Rectangles represent single item variables; ellipses represent latent variables
Methods
Sample
The China Health and Retirement Longitudinal Study (CHARLS) is an ongoing longitudinal study assessing the social, economic, and health status of nationally representative samples of Chinese residents age 45 or older and their spouses [14]. After two waves of pilot studies, the national baseline study of CHARLS was conducted between June 2011 and March 2012 using a face-to-face, computer-aided personal interview (CAPI), and the Wave II follow-up data were collected in 2013. A total of 17,708 participants from 150 urban districts and rural counties that fell within 28 provinces were chosen using a multistage probability sampling strategy. As the availability of local infrastructure and services as well as policy parameters may vary at the community level, the community questionnaire was developed to investigate the social, economic, and policy environments of each community. Detailed sampling procedures and the cohort profile are published elsewhere [14].
The national baseline community level data and household interview data from the second wave were used in this study. The community level variable of interest was the availability of recreational facilities, whereas the individual level variables included depressive symptoms, PA (LTPA and total PA), and functional health status. Given that only main respondents and their spouses in the random subsample of households reported lifestyle and health behavior parts of the questionnaire during the interview, we kept the subsample of 6085 participants who responded to the PA questionnaire. After removing 136 participants younger than 45, a total of 5949 participants were retained for further analysis.
Measurements
Depressive Symptoms
Depressive symptoms were measured using the 10-item version of the Center for Epidemiologic Studies Depression Scale (CES-D) [15]. The questions asked how often each of following was true during the past week: (1) I was bothered by things that don’t usually bother me; (2) I have trouble keeping my mind on what I was doing; (3) I felt depressed; (4) I felt everything I did was an effort; (5) I felt hopeful about the future; (6) I felt fearful; (7) my sleep was restless; (8) I was happy; (9) I felt lonely; (10) I could not get “going.” Answers consisted of rarely or none of the time (< 1 day), some or a little of the time (1–2 days), occasionally or a moderate amount of the time (3–4 days), and most or all of the time (5–7 days), which were coded from 1 to 4 respectively. The 8-item latent variable of depressive symptoms was constructed to measure depressed affect and somatic symptoms, after excluding two positively formulated items (i.e., item 5 and 8). Previous literature suggested that positively and negatively worded items measure independent constructs, and using only negatively worded items to measure depressive symptoms as a factor is appropriate [16, 17]. Cronbach’s α in this sample was 0.80.
Functional Health Status
Functional health status was assessed using the Instrumental Activities of Daily Living (IADLs) [18], which evaluates the functional limitations in engagement of higher ordered skills that are essential for independent living. The participants responded to how difficult it was to perform five functional activities: doing household chores, preparing hot meals, shopping for groceries, managing money, and taking medications. The response set for each item includes the following: “(1) no, I don’t have any difficulty, (2) I have difficulty but can still do it, (3) yes, I have difficulty and need help, and (4) I cannot do it.” Cronbach’s α was 0.84.
The Availability of Recreational Facilities
The number of available types of recreational facilities in the community was measured by the 2011 community survey completed by officers at the lowest level of government organizations. The availability score was calculated by summing the following available facilities: basketball court, swimming pool, outside exercising facilities, other outdoor sports facilities (such as Ping-Pong tables), room for card games and chess games, room for Ping-Pong, activity centers for the elderly, elderly associations, and other entertainment facilities.
Physical Activity
Two variables of PA were formed to represent LTPA (activities for the purposes of exercise and entertainment only) and total PA (activities for exercise, entertainment, job demand, and other purposes). The survey asked participants how much time they spent performing vigorous activities, moderate activities, and walking for at least 10 min continuously during a usual week. Vigorous activities included activities such as heavy lifting, digging, plowing, aerobics, fast bicycling, and cycling with a heavy load. Moderate activities included carrying light loads, bicycling at a regular pace, or mopping the floor. Walking at work and home, walking to travel from place to place, and walking for recreation, sport, exercise, or leisure were also reported. The responses on the amount of PA in 1 day were indexed as 1 = < 0.5 h; 2 = 0.5–2 h; 3 = 2–4 h; and 4 = > 4 h. The weekly PA duration score was calculated by multiplying the number of days and the daily PA duration index for each activity. Subsequently, the LTPA and total PA score were calculated using metabolic equivalent (MET) multipliers as follows: (1) LTPA score = 8.0 × leisure vigorous activity weekly duration score + 4.0 × leisure moderate activity weekly duration score + 3.3 × leisure walking weekly duration score and (2) total PA score = 8.0 × total vigorous activity weekly duration score + 4.0 × total moderate activity weekly duration score + 3.3 × total walking weekly duration score [19].
Statistical Analyses
Means and standard deviations were calculated for the examined variables in a preliminary data analysis. Group independences of sociodemographic characteristics of the respondents were measured using Pearson’s χ2 test. Cohen’s d was chosen as an estimate of effect size to quantify the difference between the rural and urban groups [20]. A small effect size would have a Cohen’s d value of 0.2, while medium and large effect sizes correspond to value of 0.5 and 0.8, respectively. Approximately 1.5% of the total values were missing in the dataset, and the number of missing values ranges from 0 to 266 for each variable. All missing values were imputed using the predictive mean matching method, which is appropriate when the assumption of normality is untenable [21]. The imputation was performed in R version 3.3.1 using the package “mice” [22]. The structural equation modeling with a two-step modeling approach (measurement model and structural model) was adopted in this study [23]. In order to assess the multigroup measurement model, a series of hierarchical invariance tests with gradual model constraints were conducted to gauge measurement equivalence between rural and urban groups [24]. First, the configural model was examined by allowing free estimation of all parameters across groups. Sequentially, the metric invariant model was established by constraining the factor loadings to be equal across groups. Lastly, the scalar invariant model sets equal intercepts (i.e., means) across groups. The multigroup structural model was established based on the conceptual model presented in Fig. 1. The invariant paths between groups were constrained to be equal in the interest of parsimony. Modification indices were evaluated to assist in model selection. Given that the data did not meet the assumption of multivariate normality, bias-corrected bootstrap techniques with 20,000 resampling iterations were performed to obtain parameter estimates with 95% confidence intervals [25, 26]. The SEM analyses were performed using Mplus 8 [27].
The overall goodness of fit was assessed with multiple indices, including the chi-square statistic (χ2), comparative fit index (CFI), standardized root mean square residual (SRMR), and root mean square error of approximation (RMSEA) with its 90% confidence interval. CFI, SRMR, and RMSEA with respective values of greater than 0.90, less than 0.08, and less than 0.06 suggest a good model fit [28]. The difference in CFI value (ΔCFI) was used as the criterion of model invariance. When ΔCFI is less than 0.01, the constrained model is preferred over non-constrained model. The merit of using ΔCFI rather than Δχ2 is that the CFI value is independent from model complexity and sample size [29].
Results
Sample Characteristics
Table 1 shows the sociodemographic characteristics of the participants. Of the 5949 total participants, 54% were female and 62% resided in rural areas. Rural community residents reported an average LTPA score of 23.24 with standard deviation (SD) of 46.9 and an average total PA score of 141.16 with SD of 122.01, respectively (Table 2). The corresponding scores for urban counterparts were 42.58 with SD of 53.97 and 102.29 with SD of 92.23. The mean and standard deviation of the community physical areas were 11 and 20 km2 in rural areas and 3.5 and 6.4 km2 in urban areas. The average availability of recreational facilities in rural communities was lower than that of urban communities. According to Cohen’s d, the difference in the availability of recreational facilities between rural and urban communities was large, while the differences for the other variables were small or negligible (Table 2).
Multigroup Measurement Models
Measurement models examine measurement invariances of multigroup models. The availability of recreational facilities and PA variables as single-item variables were not tested in the measurement model. The configural invariant model initially yielded an acceptable fit (Table 3). Based on the modification indices, there were apparent content overlaps outside the latent variable existing between two indicators; doing household chores and preparing hot meals. Correlation between their residual terms was allowed to improve model fit [30]. Subsequently, the metric invariant model and scalar invariant model showed good model fit (Table 3). Compared with the configural model, the ΔCFIs were 0.009 in favor of the scalar invariant model. Table 4 shows the correlation matrices of the examined variables. The standardized factor loadings of the indicators are shown in Table 2. In summary, the multigroup measurement models revealed that the measurements of depressive symptoms and functional health status are invariant between rural and urban groups.
Multigroup Structural Models
Heterogeneous patterns in structural paths due to a rural-urban moderating effect were captured in the multigroup analyses (Figs. 2 and 3). The final LTPA multigroup model accounted for 12 and 10% of explained variance (R2) in depressive symptoms in the rural group and urban group, respectively, and yielded good fit (Table 3). The paths from the availability of recreational facilities and functional health status to depressive symptoms were fixed to be equal across groups. In urban communities, high availability of recreational facilities predicted increased LTPA among participants (the standardized path coefficient β = 0.080), which then mediated through functional health status to mitigate depressive symptoms. Because the availability of recreational facilities merely provided one aspect of facility usage and LTPA only represented a small portion of daily PA engagement, the indirect effect from the availability of recreational facilities to depressive symptoms through LTPA and functional health status were small in urban responders (β = − 0.002) (Table 5). On the other hand, LTPA had a negligible influence on depressive symptoms in rural dwellers, as all paths through the LTPA latent variable were not significant.

Multigroup structural model using the LTPA variable (China, 2011–2013). Dash arrows represent non-significant paths (0 was included in the 95% bootstrap confidence interval); solid arrows represent significant paths; bold arrows represent equally constrained paths across groups; rectangles represent single item variables; ellipses represent latent variables. All path coefficient estimates were standardized

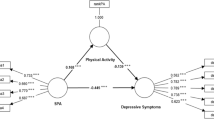
Multigroup structural model using the total PA variable (China, 2011–2013). Solid arrows represent significant paths (0 is not included in the 95% bootstrap confidence interval); dash arrows represent non-significant paths; bold arrows represent equally constrained paths across groups; rectangles represent single item variables; ellipses represent latent variables. All path coefficient estimates were standardized
In contrast with the LTPA model, the total PA multigroup model had two freely estimated paths from the availability of recreational facilities to total PA and functional health status across groups and yielded a good model fit (Table 3). The R2 for the rural group and urban group were 0.13 and 0.12, respectively. The model suggested that functional declines were significantly associated with increased depressive symptoms (rural: β = 0.349, and urban: β = 0.332). The negative associations between total PA and depressive symptoms were partially mediated through the functional health status in both groups (rural: indirect effect = − 0.068, and urban: indirect effect = − 0.057), whereas the direct paths between total PA and depressive symptoms were positive. Furthermore, the availability of recreational facilities played different roles in rural and urban communities. In rural settings, more available recreational facilities were associated with lower levels of total PA (β = − 0.077), better functional health (β = − 0.096), and decreased depressive symptoms (β = − 0.053). In urban communities, the availability of recreational facilities was negatively associated with functional health status (β = − 0.040) and depressive symptoms (β = − 0.079). Table 5 shows the direct, indirect, and total effects along with the corresponding bias-corrected bootstrap confidence intervals.
Discussion
This study examined rural-urban differences in the relationships between the availability of recreational facilities, PA, functional health status, and depressive symptoms in middle-aged and older Chinese adults. Overall, the models suggested that depressive symptoms were associated with the interplay of intrapersonal, behavioral, and environmental factors.
Our findings indicated that difficulties performing functional health tasks were associated with high occurrence of depressive symptoms among Chinese middle-aged and older adults, which is consistent with previous research [31]. Functional decline in later life often imposes physical pain and psychological stress on older people, disrupting their sense of control over life and perception of self-worth, and leading to the elevated depressive symptoms [32]. It is worth noting from our findings that functional difficulties and depressive symptoms were comorbid syndromes in both rural and urban residents. Similarly, functional disability has been shown to predict depression in Chinese adults aged 55 and above [33], adding support to the relationships between functional health status and depressive symptoms. Future investigations that track longitudinal changes in this relationship may offer intriguing insights into possible reciprocal effects between functional health and depression.
Our results showed that functional health status mediated the relationship between PA engagement and depressive symptoms, which is consistent with previous literature [34]. This lends support to the idea that PA plays a critical role in maintaining muscle homoeostasis, preventing sarcopenia and preserving functional ability [7]. However, the relationships between total PA and depressive symptoms in rural and urban groups established an inconsistent mediation structure, in which the indirect and direct effects had different signs [35]. The direct effect suggested that high levels of total PA were associated with high occurrences of depressive symptoms; however, PA within different contexts (e.g., LTPA and non-LTPA) may explain this unexpected finding. Previous research has demonstrated that PA within different contexts might reveal different associations with depression [36], and LTPA might be more beneficial for depression than PA within other domains [37]. Chen and colleagues [38] showed that only LTPA but not domestic and occupational PA were significantly associated with depressive symptoms among older adults in Taiwan. Moreover, higher levels of household PA were associated with greater depressive symptoms among older Latino adults in the USA [39]. Prior literature showed that domestic and occupational PA were major sources of activity in the Chinese population [40], especially in low-income and less educated groups [41]. Therefore, one might surmise that such obligatory activities may offer little or no benefit to mental health, and the concurrence of high levels of total PA and elevated depressive symptoms may somehow be explained by the life constraints related to socioeconomic status. In order to gain an in-depth understanding of the association between PA and depressive symptoms in future research, we may need to consider the contexts of PA.
Although all models in this study showed negative direct associations between the availability of recreational facilities and depressive symptoms, it is premature to deduce that available recreational facilities promotes engagement in PA and thus mitigates depressive symptoms. The models showed heterogeneous associations between the availability of recreational facilities and PA between rural and urban settings. Specifically, our results indicated that the availability of recreational facilities was positively associated with LTPA in urban communities, but not in rural villages. This relationship in urban communities is similar to evidence reported from Hong Kong, where the majority of older people live in high density urban communities [10]. In rural settings, on the other hand, the results showed that participants living in better developed villages with more recreational facilities actually engaged in less total PA, which is different from the evidence found in developed countries [42]. Since the amount of non-LTPA (such as occupational PA) may decline due to China’s rapid urbanization [40], total PA may decrease without increases in LTPA. In addition, inactive lifestyles may be gaining popularity in rural residents because of a lower awareness of the health benefits of PA, resulting in low participation in LTPA. Therefore, the promotion of LTPA may be critical to prevent negative health impacts from the potential decline of PA in rural residents.
The main strength of the present study is that the multigroup analysis provided moderated mediation assessment of multiple microsystem components among rural and urban populations in the macrosettings. Moreover, this study used nationally representative samples of Chinese middle-aged and older adults, which increased generalizability of the findings. Despite significant findings, there are several notable limitations. First of all, although directed graphs were used for model construction, no conclusions on causation may be made. Therefore, longitudinal study designs are recommended to explore the complex causal structure of geriatric depression. Secondly, the possibility of perception bias cannot be ruled out while using self-reported PA instruments. Objective PA measurements (such as accelerometers) may reduce the possibility of perception bias but may have difficulty observing distinctions between LTPA and PA within other contexts. Last but not least, this study did not include other aspects of recreational facilities such as density, proximity, and accessibility. Nor were the assessments standardized for size and population of the community. Future research should examine these factors to present a comprehensive picture on the usage of recreational facilities.
Conclusions
The present study delineated rural-urban differences in PA patterns at the individual level and the availability of recreational facilities at the community level in the middle-aged and older Chinese population. This study goes further by demonstrating the relationships of PA and the availability of recreational facilities with functional health status and depressive symptoms. Future investigations studying the relationships between active living and mental health may consider the heterogeneous attributes of PA within different contexts. As rapid urbanization continues in China, health policy responses and urban planning practices should create joint efforts to optimize the benefits of PA for healthy aging by promoting LTPA and creating active living communities.
References
Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet. 2007;370(9590):851–8.
Xu Y, Yang J, Gao J, Zhou Z, Zhang T, Ren J, et al. Decomposing socioeconomic inequalities in depressive symptoms among the elderly in China. BMC Public Health. 2016;16(1):1214.
Turvey CL, Schultz SK, Beglinger L, Klein DM. A longitudinal community-based study of chronic illness, cognitive and physical function, and depression. Am J Geriatr Psychiatry. 2009;17(8):632–41.
Jiang J, Tang Z, Futatsuka M, Zhang K. Exploring the influence of depressive symptoms on physical disability: a cohort study of elderly in Beijing, China. Qual Life Res. 2004;13(7):1337–46.
Feng Q, Zhen Z, Gu D, Wu B, Duncan PW, Purser JL. Trends in ADL and IADL disability in community-dwelling older adults in Shanghai, China, 1998–2008. J Gerontol B Psychol Sci Soc Sci. 2013;68(3):476–85.
Cooney G, Dwan K, Mead G. Exercise for depression. JAMA. 2014;311(23):2432–3.
Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381(9868):752–62.
Paterson DH, Warburton DE. Physical activity and functional limitations in older adults: a systematic review related to Canada’s Physical Activity Guidelines. Int J Behav Nutr Phys Act. 2010;7(1):38.
Sallis JF, Bowles HR, Bauman A, Ainsworth BE, Bull FC, Craig CL, et al. Neighborhood environments and physical activity among adults in 11 countries. Am J Prev Med. 2009;36(6):484–90.
Cerin E, Lee KY, Barnett A, Sit CH, Cheung MC, Chan WM. Objectively-measured neighborhood environments and leisure-time physical activity in Chinese urban elders. Prev Med. 2013;56(1):86–9.
Day K. Built environmental correlates of physical activity in China: a review. Prev Med Rep. 2016;3:303–16.
Bronfenbrenner U, Morris PA. The bioecological model of human development. In: Handbook of child psychology. John Wiley & Sons: New York; 2006.
Greenfield EA. Using ecological frameworks to advance a field of research, practice, and policy on aging-in-place initiatives. Gerontologist. 2012;52(1):1–12.
Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China health and retirement longitudinal study (CHARLS). Int J Epidemiol. 2014;43:61–8.
Irwin M, Artin KH, Oxman MN. Screening for depression in the older adult: criterion validity of the 10-item Center for Epidemiological Studies Depression Scale (CES-D). Arch Intern Med. 1999;159(15):1701–4.
Schroevers MJ, Sanderman R, Van Sonderen E, Ranchor AV. The evaluation of the Center for Epidemiologic Studies Depression (CES-D) scale: depressed and positive affect in cancer patients and healthy reference subjects. Qual Life Res. 2000;9(9):1015–29.
Chen H, Mui AC. Factorial validity of the Center for Epidemiologic Studies Depression Scale short form in older population in China. Int Psychogeriatr. 2014;26(01):49–57.
Katz S. Assessing self-maintenance: activities of daily living, mobility, and instrumental activities of daily living. J Am Geriatr Soc. 1983;31(12):721–7.
IPAQ committee. Guidelines for data processing and analysis of the International Physical Activity Questionnaire (IPAQ). 2005. http://www.ipaq.ki.se/scoring.htm.
Cohen J. Statistical power analysis for the behavioral sciences. Hillsdale: Lawrence Erlbaum Associates; 1988.
White IR, Royston P, Wood AM. Multiple imputation using chained equations: issues and guidance for practice. Stat Med. 2011;30(4):377–99.
Buuren S, Groothuis-Oudshoorn K. mice: multivariate imputation by chained equations in R. J Stat Softw. 2011;45(3)
Anderson JC, Gerbing DW. Structural equation modeling in practice: a review and recommended two-step approach. Psychol Bull. 1988;103(3):411–23.
Vandenberg RJ, Lance CE. A review and synthesis of the measurement invariance literature: suggestions, practices, and recommendations for organizational research. Organ Res Methods. 2000;3(1):4–70.
Shrout PE, Bolger N. Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychol Methods. 2002;7(4):422–45.
MacKinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivariate Behav Res. 2004;39(1):99–128.
Muthén LK, Muthén BO. Mplus Version 8 user’s guide. Los Angeles, CA: Muthén & Muthén.: 1998–2017.
Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55.
Cheung GW, Rensvold RB. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct Equ Modeling. 2002;9(2):233–55.
Jöreskog KG, Sörbom D. LISREL 8: structural equation modeling with the SIMPLIS command language. Chicago: Scientific Software International; 1993.
Mezuk B, Edwards L, Lohman M, Choi M, Lapane K. Depression and frailty in later life: a synthetic review. Int J Geriatr Psychiatry. 2012;27(9):879–92.
Yang Y. How does functional disability affect depressive symptoms in late life? The role of perceived social support and psychological resources. J Health Soc Behav. 2006;47(4):355–72.
Feng L, Nyunt MSZ, Feng L, Yap KB, Ng TP. Frailty predicts new and persistent depressive symptoms among community-dwelling older adults: findings from Singapore Longitudinal Aging Study. J Am Med Dir Assoc. 2014;15(1):76. e7-. e12.
Rejeski W, Mihalko S. Physical activity and quality of life in older adults. J Gerontol A Biol Sci Med Sci. 2001;56:23–35.
MacKinnon DP, Fairchild AJ, Fritz MS. Mediation analysis. Annu Rev Psychol. 2007;58:593–614.
Teychenne M, Ball K, Salmon J. Associations between physical activity and depressive symptoms in women. Int J Behav Nutr Phys Act. 2008;5:27.
Pickett K, Yardley L, Kendrick T. Physical activity and depression: a multiple mediation analysis. Ment Health Phys Act. 2012;5(2):125–34.
Chen L-J, Stevinson C, Ku P-W, Chang Y-K, Chu D-C. Relationships of leisure-time and non-leisure-time physical activity with depressive symptoms: a population-based study of Taiwanese older adults. Int J Behav Nutr Phys Act. 2012;9(1):1–10.
Bustamante EE, Wilbur J, Marquez DX, Fogg L, Staffileno BA, Manning A. Physical activity characteristics and depressive symptoms in older Latino adults. Ment Health Phys Act. 2013;6(2):69–77.
Ng SW, Howard AG, Wang H, Su C, Zhang B. The physical activity transition among adults in China: 1991–2011. Obes Rev. 2014;15(S1):27–36.
Bauman A, Ma G, Cuevas F, Omar Z, Waqanivalu T, Phongsavan P, et al. Cross-national comparisons of socioeconomic differences in the prevalence of leisure-time and occupational physical activity, and active commuting in six Asia-Pacific countries. J Epidemiol Community Health. 2011;65(1):35–43.
Shores KA, West ST, Theriault DS, Davison EA. Extra-individual correlates of physical activity attainment in rural older adults. J Rural Health. 2009;25(2):211–8.
Acknowledgements
The authors thank the CHARLS research and field team and all respondents for their contributions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Deng, Y., Paul, D.R. The Relationships Between Depressive Symptoms, Functional Health Status, Physical Activity, and the Availability of Recreational Facilities: a Rural-Urban Comparison in Middle-Aged and Older Chinese Adults. Int.J. Behav. Med. 25, 322–330 (2018). https://doi.org/10.1007/s12529-018-9714-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-018-9714-3