
Abstract
Purpose
This systematic review aims to summarize eHealth studies with mindfulness- and relaxation-based interventions for medical conditions and to determine whether eHealth interventions have positive effects on health.
Method
A comprehensive search of five databases was conducted for all available studies from 1990 to 2015. Studies were included if the intervention was mainly technology delivered and included a mindfulness- or relaxation-based intervention strategy and if patients with a medical condition were treated. Treatment effects were summarized for different outcomes.
Results
A total of 2383 records were identified, of which 17 studies with 1855 patients were included in this systematic review. These studies were conducted in patients with irritable bowel syndrome, chronic fatigue syndrome, cancer, chronic pain, surgery, and hypertension. All but one study were delivered online through a web-based platform; one study delivered the intervention with iPods. The studies indicate that mindfulness- and relaxation-based eHealth interventions can have positive effects on patients’ general health and psychological well-being. No effects were found for stress or mindfulness. Only five studies reported economic analyses of eHealth interventions without any clear conclusion.
Conclusion
There is some evidence that mindfulness- and relaxation-based eHealth interventions for medical conditions can have positive effects on health outcomes. Therefore, such interventions might be a useful addition to standard medical care. No app studies were retrieved, even though a vast number of smartphone apps exist which aim at increasing users’ health. Therefore, more studies investigating those health apps are needed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
eHealth is defined by the World Health Organization (WHO) as the use of information and communication technologies for health [1]. The number of eHealth studies is increasing, and eHealth interventions are effective at improving patients’ health [2]. One of the most important advantages of eHealth is its high accessibility due to the well-established access to the Internet by the majority of people worldwide, which also allows remotely located people or those with reduced mobility access to care [3]. Another advantage of eHealth interventions is reduced healthcare costs, since relatively few economic and personnel resources are needed for delivery compared to face-to-face interventions [2]. eHealth interventions can use a variety of intervention strategies to improve patients’ health, such as education, feedback, exercise, and verbal support with a therapist or other patients [4]. Changing patients’ cognition and behavior can be regarded as the underlying working mechanism for such interventions. In recent years, setting up and maintaining an eHealth intervention were greatly facilitated due to technological advances like Web 2.0 [5].
The mode of delivery and format of eHealth interventions vary considerably. For instance, audio, video, or text can convey educational information or various exercises, while an eHealth intervention might incorporate contact with a therapist (e.g., via e-mail, chat, telephone) or with other users (e.g., via forum). Also, a variety of platforms like PCs, tablets, or smartphones can be used to deliver an eHealth intervention, making eHealth a broad topic with numerous different definitions [6].
A considerable number of eHealth studies also incorporate mindfulness- and relaxation-based intervention strategies. The rationale for this might be the evidence of many studies with a beneficial effect of mindfulness- and relaxation-based interventions in a face-to-face setting for patients with medical conditions [7,8,9,10]. The practice of mindfulness is rooted in Buddhist traditions [11] and has been implemented into Western healthcare interventions, independent of a religious and cultural context [12]. Mindfulness consists of intentional attention in the present moment and an openness and acceptance towards this experience [13]. The non-judgmental experience of body sensations is often part of mindfulness interventions. It is hypothesized that this experience leads to increased self-regulation and emotional, cognitive, and behavioral flexibility [12]. The underlying mechanism is therefore an adaptation to the present moment by reducing the impact of wearing information through acceptance.
On the contrary, traditional relaxation interventions such as progressive muscle relaxation [14] are rooted in Western society and focus directly on relaxation by means of exercises (e.g., progressive muscle relaxation) or imagination (e.g., guided imagery) [15]. The underlying mechanism is a physiological response (e.g., decreased heart rate and blood pressure) by body exercises or the manipulation of thoughts [16, 17].
Despite those differences, both mindfulness practices and relaxation methods elicit a relaxation response (i.e., decreased psychophysiological arousal) [15, 18]. These similar responses are congruent with findings indicating that mindfulness- and relaxation-based interventions are effective in reducing distress in patients with hard-to-treat or chronic medical conditions [19,20,21]. Mindfulness- and relaxation-based interventions can also be delivered in methodologically similar ways (e.g., multi-week and multimodal clinical interventions) [22]. In addition, both kinds of interventions are effectively used to increase patients’ self-care [23, 24] and, compared to other stress-reducing interventions such as biofeedback [25], no additional equipment is required.
Mindfulness- and relaxation-based eHealth interventions might be a good alternative or addition to face-to-face interventions for patients with high psychological burden, since eHealth interventions are low threshold (i.e., patients do not need to leave their home for the intervention) [26]. Therefore, eHealth interventions as an addition to standard care might be particularly suited for patients with a high frequency of medical visits or impaired mobility.
Two recent reviews [27, 28] summarized the effects of mindfulness-based eHealth interventions, indicating that these eHealth interventions can contribute to improve outcomes such as stress, depression, and anxiety. However, both reviews included studies with a large variety in the population, ranging from healthy volunteers (i.e., mainly student population) to patients with medical or psychological conditions. Patients with medical conditions often suffer from increased rates of depression, anxiety, and distress, as well as a reduced quality of life [29,30,31,32]. Therefore, a focused perspective on eHealth interventions for patients with medical conditions is advisable to allow conclusions for such users.
To draw more conclusive findings for patients with medical conditions, the aim of this systematic review was to summarize the effectiveness of mindfulness- and relaxation-based eHealth studies for patients with medical conditions. Since we were interested in summarizing the effectiveness (i.e., effects in a routine clinical setting) of mindfulness- and relaxation-based interventions, we included studies which combine various types of interventions.
Method
Eligibility Criteria
Studies were included if they conducted a pre- and post-assessment of a health outcome of interest (general health, depression or anxiety, stress, mindfulness, satisfaction with the intervention, self-efficacy or self-care, pain or other health-related outcomes) for an eHealth intervention in adult patients with medical conditions (e.g., cancer, hypertension, fibromyalgia). Studies were excluded if patients suffered solely from mental disorders (i.e., 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) diagnosis codes F01–F99), which also led to the exclusion of addiction or substance abuse (ICD-10 diagnosis code F10–F19). Studies with patients suffering from disorders which could be considered either a medical condition or a mental disorder (e.g., sleep disorders: ICD-10 code F51 or G47) were excluded.
In each study, a mindfulness or relaxation intervention strategy had to be a substantial part of the intervention (see Table 1). Studies with various intervention strategies (e.g., mindfulness meditation, relaxation, patient education, and biofeedback) were only included if the ratio of mindfulness or relaxation intervention strategy to the total number of intervention strategies was at least 1 to 5. Furthermore, the intervention had to be mainly technology delivered. We considered an intervention as technology delivered if it was accessed via the internet or a smartphone app, if face-to-face meetings between patients and the study team were restricted to data collection, and if the contact with a therapist was restricted to one face-to-face contact. However, we included studies if they comprised online, e-mail, or phone contact with the therapist as part of the intervention (see Table 1).
The studies had to include at least pre- and post-assessments of any kind of health-related outcome (e.g., quality of life, stress), but the design did not have to be controlled (i.e., including a comparison group). We included all journal publications published in any language between 1990 and April 2015. The reason for this timeframe for inclusion is that during the 1990s, the internet was established for public use [6]. During the screening process, we excluded dissertations due to limited access to unpublished work and a lack of clarity regarding peer review.
Search Strategy and Study Selection
For the literature search, we used three databases in EBSCO (PsycINFO, CINAHL, and AMED) and two additional databases (EMBASE and Medline). We searched for the following terms (full list of keywords in Appendix): “app or online context” AND “mindfulness or relaxation” AND “intervention or rct or treatment.” For exclusion, the following terms were used: “abuse or alcohol or addiction.”
Our team consisted of four researchers, who were trained with a screening manual for study inclusion. We based the screening manual on previous systematic reviews performed by our group and adapted it to the specific requirements (e.g., inclusion criteria, outcomes) for this systematic review. Three researchers conducted the abstract screening (JB, JoB, IM), and three researchers conducted the full-text screening (JB, JoB, MM). After the literature search and after the removal of duplicates, all abstracts were screened according to a structured manual. Subsequently, the full texts of included articles were screened using the same predefined eligibility criteria.
Data Extraction
All researchers involved in the data extraction (JB, JoB, MM) were trained using the extraction manual with five studies for training purposes. During the training, we discussed the results and clarified any terminological ambiguity. After the training, all studies were extracted in duplicate (JoB, MM) and the extraction of data was done in Excel according to a standardized extraction manual. In cases of disagreement regarding the extracted data, consensus was reached with a third researcher (JB).
We extracted general information about the study (first author and publication year), data on patients (number of patients in intervention and control groups, inclusion and exclusion criteria), intervention (mode of delivery, intervention strategy, dose, and length of intervention), comparators, outcomes, and study design.
For the extraction of intervention strategies, we prespecified the following categories: mindfulness, relaxation, patient education, biofeedback, cognitive intervention, exercise (including Yoga, Tai Chi), imagination or visualization, and meditation other than mindfulness.
As outcomes of interest, we prespecified the following categories: general health (defined as measures assessing physical functioning, disability or quality of life), depression or anxiety, stress, mindfulness, satisfaction with the intervention, self-efficacy or self-care, pain, or other health-related outcomes. The effectiveness of the eHealth intervention was evaluated by a vote counting approach, in which the number of studies with positive effects was compared to the number of studies with negative effects [33]. For randomized controlled trials (RCTs), a significant effect was defined as superior effectiveness if the results favored the intervention group. A non-significant effect was defined as equal effectiveness. A significant effect was defined as inferior effectiveness if the results favored the control group. For pretest-posttest studies without a control group, a significant change over time was considered a positive response. Insignificant improvement over time was considered no response, and deterioration over time was considered a negative response. p values lower than .05 were considered significant. We report standardized mean differences between groups which are either reported by the authors or derived from information given in the publication by transformation routines.
Quality Assessment
For the assessment of risk of bias, two researchers (JB, MM) assessed the adequate random sequence generation (κ = 0.70) and allocation concealment (κ = 0.86) for each study according to Cochrane standards [33] in duplicate. In cases of disagreement, consensus was reached in a discussion between the two researchers. Blinding of the Cochrane Risk of Bias Tool [33] was not rated, since blinding might be considered inadequate according to Cochrane standards in all studies with self-report measures, which is the gold standard in this type of research. We did not assess completeness of outcome assessment in a regular way, but we extracted the number of dropouts, which reflects the feasibility of the interventions. We defined dropouts as the number of patients who were allocated to the eHealth intervention or control group but did not complete the post-treatment assessment.
For the assessment of the external validity of each study, we used one item of the checklist by Downs and Black [34], namely if the patients in the study were representative for the entire patient population (i.e., patients comprise the entire source population, an unselected sample of consecutive patients, or a random sample) (κ = 0.61). Two researchers (JB, MM) rated the items individually for each study. In cases of disagreement, the same researchers reached consensus in a discussion.
Data Synthesis
We pooled the findings of the studies according to the six outcomes and stratified for the type of control condition (usual care, waitlist vs. active control, attention control). The findings were summarized in a vote counting approach, with all non-significant findings being reported as a null effect, which is a quite conservative approach. We used this approach since the outcomes of the studies and the underlying medical conditions vary substantially between studies and homogeneity in effects cannot be expected in a pooled meta-analysis.
Results
Study Selection
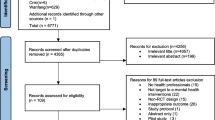
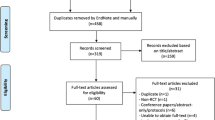
Through the literature search, a total of 2703 records were identified. After removal of 323 duplicates, titles and abstracts were screened in 2383 records. Subsequently, 2257 studies were excluded because they did not match our inclusion criteria. The full texts of the remaining 126 studies were screened; of these, 109 did not meet our inclusion criteria. Finally, a total of 17 studies met our inclusion criteria and were included in this review (Fig. 1).

PRISMA flow diagram
Study Characteristics
An overview of the 17 included studies [35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51] is presented in Table 2. Three studies [41, 42, 51] were published between 2000 and 2005, a further three studies [38, 47, 50] were published between 2006 and 2010, and 11 studies [35,36,37, 39, 40, 43,44,45,46, 48, 49] were published between 2011 and 2015. Regarding the study designs, 15 studies [35, 37,38,39,40,41,42,43,44,45, 47,48,49,50,51] were randomized. One study [36] used a control group without randomization, and one study [46] used a pretest-posttest design. Patients in the studies suffered from eight different medical conditions. Five studies [35, 45, 47,48,49] conducted an eHealth intervention for irritable bowel syndrome, three studies [41, 44, 51] for headache, two studies [37, 39] for cancer, two studies [38, 42] for chronic pain, two studies [40, 45] for fibromyalgia, one study [43] for surgery, and one study [50] for hypertension. All but one study were delivered online (i.e., access through a web browser). One study [43] delivered the eHealth intervention with iPods (i.e., relaxing music).
The study-specific characteristics are summarized in Table 3. The included studies involved a total of 1855 patients, with a range from 18 to 368 patients per study. The duration of the eHealth interventions ranged from 10 days to 10 weeks.
Congruent with our inclusion criteria, all studies had at least an intervention strategy consisting of mindfulness (11 studies [35,36,37, 39, 40, 42, 45,46,47,48,49]) or relaxation (9 studies [36,37,38,39, 41, 43, 44, 50, 51]). Three of those studies [36, 37, 39] used both mindfulness and relaxation intervention strategies. The majority of studies included additionally patient education (14 studies [35, 37,38,39,40,41,42, 44,45,46,47,48,49, 51]) or cognitive intervention (13 studies [35, 37,38,39,40,41,42, 44,45,46,47,48,49]) as an intervention strategy. Less commonly used intervention strategies were biofeedback [41, 50], other meditation techniques than mindfulness [36, 37], and imagination or visualization [36, 39]. None of the studies used body exercise as an intervention strategy. Furthermore, 11 studies used additional intervention strategies which were not included in our classification (e.g., exposure treatment, writing exercises).
Except for one [43], all studies used more than one intervention strategy according to our classification. Two studies [37, 39] used six intervention strategies, ten studies [35, 36, 38, 40, 41, 44,45,46,47,48] used four intervention strategies, three studies [42, 49, 51] used three intervention strategies, and one study [50] used two intervention strategies.
The intervention strategies in the active control groups were online chat forum [35], online symptom management program [36], information via website [37], health tips [40], online diary [41], online pain management with psychoeducation [42], internet-delivered stress management [48], and internet-delivered cognitive behavior therapy with exposure [49].
Quality of Studies
Concerning the quality of the sequence generation, 11 studies of the 15 RCTs [37,38,39,40, 42, 44, 45, 47,48,49, 51] had a low risk of bias and four studies [35, 41, 43, 50] had an unclear risk of bias. The allocation concealment was performed well in ten studies [37, 40, 42, 44, 45, 47,48,49,50,51] with a low risk of bias, and five studies [35, 38, 39, 41, 43] had an unclear risk of bias. In 12 studies [35, 37,38,39, 42,43,44,45, 48,49,50,51], the subjects were representative of the population; in four studies [36, 40, 41, 47], they were not, and in one study [46], representativeness could not be determined (see Table 4). The assessment of the risk of bias items was not applicable for one study by Ljotsson et al. [46], which was a pretest-posttest study without a control group.
Effectiveness of Mindfulness-Related eHealth Interventions
The most common outcome was general health, which was assessed in 13 studies [36, 37, 39,40,41, 44,45,46,47,48,49,50,51] (see Table 5). Depression or anxiety was assessed in 11 studies [37, 38, 40,41,42,43, 46,47,48,49, 51]. Pain was assessed in nine studies [38, 40,41,42,43,44, 46, 47, 51]. Self-efficacy or self-care [38,39,40, 43, 44], stress [37, 48], and mindfulness [36, 42], and satisfaction with the intervention [38, 39] were less commonly assessed. Most studies used validated questionnaires for the assessment of outcomes of interest (see Table 5). Exceptions were scales developed by investigators or modified items [40] and diaries [40, 44, 47, 51] which were used to complement questionnaires.
Twelve of 13 studies with general health as outcome were RCTs. Eight studies used an active control group, of which five studies [40, 41, 45, 47, 48] reported superior effectiveness of the eHealth intervention. One study reported equal effectiveness [37] for the eHealth intervention and control group, and two studies reported inferior effectiveness of the eHealth intervention [36, 49] compared to intervention strategies, which served as the most beneficial active comparator in the study (meaning that the eHealth intervention was considered as control condition). In the remaining four RCTs with general health, patients in the control group received treatment as usual. All four studies [39, 44, 50, 51] showed equal effectiveness of eHealth interventions and control groups. One study [46] used a pretest-posttest design indicating a positive response of the eHealth intervention.
Out of the 12 studies assessing depression or anxiety, seven studies used an RCT design with an active control group. Two studies [40, 47] reported superior effectiveness of eHealth intervention. Four studies [37, 41, 42, 48] reported equal effectiveness. One dismantling study [49] reported inferior effectiveness of a mindfulness-based eHealth intervention if compared to a more comprehensive online program. This can be considered the most promising treatment, since an effective treatment component (i.e., exposure for irritable bowel syndrome patients) was added to an otherwise similar mindfulness-based intervention. Four studies assessing depression [38, 43, 45, 51] used an RCT design with a treatment-as-usual control group, of which one showed superior effectiveness [45] and the remaining three showed equal effectiveness. One study [46] used a pretest-posttest design without a control group and showed a positive response.
Out of the nine studies assessing pain, four studies used an RCT design with an active control group. Two studies [41, 47] showed superior effectiveness. The remaining two studies [40, 42] showed equal effectiveness. Four studies assessing pain used an RCT design with treatment-as-usual control groups. One study [51] showed superior effectiveness and the remaining three studies [38, 43, 44] reported equal effectiveness. One study [46] used a pretest-posttest design without a control group and showed a positive response.
Out of the five studies assessing self-efficacy, one study [40] used an RCT design with an active control group, reporting superior effectiveness. Four studies assessing self-efficacy used an RCT design with treatment-as-usual control groups. Out of those studies, two [39, 44] reported superior effectiveness and two studies [38, 43] reported equal effectiveness.
Two studies [37, 48] with an RCT design using an active control group assessed stress and reported equal effectiveness. Similarly, two studies [36, 42] with an RCT design using active control groups assessed mindfulness and reported equal effectiveness.
Patients’ satisfaction with the eHealth intervention was assessed in two studies [38, 39]. In one study [38], the majority of patients considered the intervention to be helpful, found the intervention program easy to navigate, and would recommend the intervention to others. In another study [39], global satisfaction with the intervention was high and patients considered the interventions a good tool for their medical condition (breast cancer) and would recommend the intervention to a friend with a similar diagnosis.
These results are summarized in Table 6, in which the effectiveness of mindfulness- and relaxation-based eHealth interventions is listed for the outcomes of interest stratified for the type of control group: inactive control groups (i.e., treatment as usual or wait list) or active control groups.
Discussion
This systematic review found evidence that eHealth interventions with mindfulness- or relaxation-based strategies might be effective for increasing patients’ general health and well-being. More than half of the studies reported positive effects on general health (i.e., physical functioning, disability, quality of life), depression, anxiety, or self-efficacy. Fewer studies reported positive effects of eHealth interventions on pain, and no study reported positive effects on stress or mindfulness. Overall, these findings are of clinical relevance since all studies used eHealth interventions for difficult-to-treat or chronic medical conditions. These patient populations are particularly relevant for eHealth, for instance, due to their mobility limitations.
Our findings are mainly congruent with the results of a recent systematic review by Fish et al. [27] and a recent meta-analysis by Spijkerman et al. [28], which summarized the effects of mindfulness-based eHealth interventions. Fish et al. [27] as well as Spijkerman et al. [28] found positive effects of mindfulness-based eHealth interventions on anxiety and depression. Also, our findings support the positive effects of mindfulness-based eHealth interventions on well-being similar to Spijkerman et al. [28]. In contrast to our findings, Fish et al. [27] and Spijkerman et al. [28] also reported positive effects of eHealth interventions on stress and mindfulness. This discrepancy might be explained by different study populations. Our review included studies with patients, whereas in the review of Fish et al. [27], the three studies with positive effects on stress were conducted in healthy students [52,53,54]. Similarly, the four studies with positive effects on mindfulness in the review by Fish et al. [27] were conducted in healthy students [54,55,56] or in patients with recurrent depression [57] and were therefore not included in our systematic review. Similarly, in the review by Spijkerman et al. [28] with a total of 15 included studies, the majority of studies on stress (7 of 9 studies) or mindfulness (6 of 10 studies) were conducted in healthy subjects.
Compared to a face-to-face delivery of interventions, eHealth interventions may have the disadvantage of neglecting the potential of the therapeutic alliance, which is associated with larger treatment effects in psychological interventions [58, 59]. Current research indicates that eHealth interventions with therapist involvement show comparable effects to face-to-face interventions [60,61,62], but eHealth interventions without therapist involvement have lower effects [63]. So far, more patients prefer a face-to-face delivery over internet delivery of an intervention [64], which might change in the near future.
eHealth interventions have some advantages. First, eHealth interventions are low-threshold since the intervention can be accessed at home or on the move [26] and stigmatization due to the blaming for using specific intervention might be lowered [65]. Second, eHealth interventions can reach a lot of patients since eHealth interventions can be conceptualized without a dedicated therapist, which leads to a smaller limitation regarding attendance of the intervention [65]. The flexibility of such interventions is taken a step further with mHealth interventions, which use mobile devices to deliver an intervention [66]. Interestingly, only one study [43] delivered the intervention through a mobile device and no study used an app-based intervention (i.e., delivery through a smartphone).
Limitations
This review has a number of limitations. First, we did not extract data on symptom reduction for each specific medical condition, since the treatment response might largely differ between health conditions. Nevertheless, such information might be of importance to medical specialists in order to estimate the effects of eHealth interventions for a specific medical condition. However, the advantage of our approach is that our predefined outcomes, such as general health and psychological well-being, might allow comparisons across medical conditions.
Second, we looked at adherence using the number of dropouts from time points of allocation to post-intervention assessment. More precise indicators for adherence might be the time spent using the eHealth intervention program or the completion rate of intervention modules. However, such information was only reported in a few studies [37, 40, 42, 47].
Third, mindfulness- and relaxation-based interventions are treatments which can be part of more comprehensive treatment approaches or being used as main intervention strategy. For our systematic review, we used a pragmatic way for the inclusion of studies: if the ratio of mindfulness or relaxation intervention strategies to the total number of intervention strategies was at least 1 to 5, we included the study. Therefore, we might have excluded studies for this systematic review with related intervention strategies, but with a minor importance of mindfulness and relaxation in the overall program. The aforementioned systematic reviews by Spijkerman et al. [28] and Fish et al. [27] summarize mindfulness-based eHealth interventions from a slightly different angle, and the included number of studies (Spijkerman N = 15, Fish N = 10, our review N = 17) and the content of the interventions differ substantially. As an example, the review by Spijkerman et al. [28] included three studies [67,68,69] with an internet-delivered acceptance and commitment therapy (ACT) [70] for patients with a medical condition. These three studies were not included in the review by Fish et al. [27] or in our review. We did not include eHealth ACT studies per se since ACT is a form of behavioral psychotherapy which incorporates only singular elements of mindfulness practices, for instance, cultivating a non-judgmental presence [71]. This example illustrates that the identification of mindfulness- and relaxation-based eHealth intervention is difficult and, in turn, a clear description of intervention strategies and their relevance for the intervention at a glance would be of help.
Fourth, we summarized the effectiveness of mindfulness- and relaxation-based interventions and therefore included studies which combine various types of interventions, including mindfulness or relaxation. Hence, this summary provides information about mindfulness- and relaxation-based eHealth interventions in clinical relevant settings. However, due to the multitude of intervention types, a conclusion about active components of mindfulness- and relaxation-based interventions cannot be drawn and should be addressed in efficacy studies.
Fifth, we did not include gray literature in this systematic review, which could lead to a biased summary of the effectiveness of eHealth studies due to publication bias.
Recommendations for Future Research
The results regarding the effectiveness of eHealth studies were heterogeneous, with some studies showing positive effects across a variety of outcomes and some studies showing no effect. This heterogeneity might be caused by differences in the treatment dose between studies. One part of the treatment dose is the practice of exercises by the patients. Meditation and relaxation interventions are most effective when the exercises are practiced regularly [72, 73]. Therefore, future research should investigate adherence in greater detail and also possible ways of increasing adherence to an eHealth intervention.
We also recommend a more standardized assessment of cost-effectiveness, which would allow a comprehensive evaluation about healthcare benefits of this new technology compared to face-to-face interventions. Only five studies included in this review estimated cost-effectiveness [35, 41, 45, 46, 51] with different assessments, preventing a comprehensive evaluation of cost-effectiveness. The rationale to use eHealth interventions is also based in economic reasons. Therefore, rigorous cost-effectiveness analyses of eHealth studies might be needed to convince stakeholders to consider eHealth interventions as an appropriate intervention strategy for medical care.
As mentioned in the results, mindfulness- and relaxation-based eHealth studies often included oftentimes additional intervention strategies. The most common were cognitive and psychoeducation intervention strategies, which are in and of themselves effective intervention strategies for various medical conditions [74]. This leads to the question of whether mindfulness and relaxation intervention strategies have an additional benefit in cognitive and psychoeducational interventions, which should be addressed in upcoming dismantling studies.
Also, the comparison to the recent reviews by Fish et al. [27] and Spijkerman et al. [28] indicated that mindfulness-based eHealth interventions showed positive effects in stress and mindfulness in healthy subjects but not in patients with medical conditions. However, this difference might be the result of absent studies of patients with medical conditions: only two studies included in our review assessed stress [37, 48] and mindfulness [36, 42]. To determine whether patients with medical conditions similarly benefit in stress and mindfulness outcomes from mindfulness- and relaxation-based eHealth studies, such outcomes should be investigated in upcoming studies. If more studies about this topic are available, a formal meta-analysis can be conducted to explore moderators (e.g., dose) and biases (e.g., study quality).
This systematic review was not able to summarize evidence from mHealth studies which contradicts the vast number of available mHealth apps. In 2015, more than 45,000 mHealth apps were published [75]. Therefore, future studies should also use mHealth technology and assess feasibility and effectiveness.
Conclusion
There is evidence that mindfulness- and relaxation-based eHealth interventions for medical conditions can have positive effects on general health, as well as depression and anxiety. Therefore, eHealth interventions can be recommended as an addition to standard medical care, especially if the medical condition is linked with high psychological stress or burden and if patients’ access to face-to-face interventions is limited.
References
World Health Organization. http://www.who.int/topics/ehealth/en/. Accessed December 15, 2016.
Elbert NJ, van Os-Medendorp H, van Renselaar W, Ekeland AG, Hakkaart-van Roijen L, Raat H, et al. Effectiveness and cost-effectiveness of ehealth interventions in somatic diseases: a systematic review of systematic reviews and meta-analyses. J Med Internet Res. 2014;16(4):e110. doi:10.2196/jmir.2790.
Meier CA, Fitzgerald MC, Smith JM. eHealth: extending, enhancing, and evolving health care. Annu Rev Biomed Eng. 2013;15:359–82. doi:10.1146/annurev-bioeng-071812-152350.
Kuijpers W, Groen WG, Aaronson NK, van Harten WH. A systematic review of web-based interventions for patient empowerment and physical activity in chronic diseases: relevance for cancer survivors. J Med Internet Res. 2013;15(2):e37. doi:10.2196/jmir.2281.
Kamel Boulos MN, Wheeler S. The emerging Web 2.0 social software: an enabling suite of sociable technologies in health and health care education1. Health Inf Libr J. 2007;24(1):2–23.
Oh H, Rizo C, Enkin M, Jadad A. What is eHealth (3): a systematic review of published definitions. J Med Internet Res. 2005;7(1):e1. doi:10.2196/jmir.7.1.e1.
Fjorback LO, Arendt M, Ornbol E, Fink P, Walach H. Mindfulness-based stress reduction and mindfulness-based cognitive therapy: a systematic review of randomized controlled trials. Acta Psychiatr Scand. 2011;124(2):102–19. doi:10.1111/j.1600-0447.2011.01704.x.
Rainforth MV, Schneider RH, Nidich SI, Gaylord-King C, Salerno JW, Anderson JW. Stress reduction programs in patients with elevated blood pressure: a systematic review and meta-analysis. Curr Hypertens Rep. 2007;9(6):520. doi:10.1007/s11906-007-0094-3.
Luebbert K, Dahme B, Hasenbring M. The effectiveness of relaxation training in reducing treatment-related symptoms and improving emotional adjustment in acute non-surgical cancer treatment: a meta-analytical review. Psychooncology. 2001;10(6):490–502. doi:10.1002/pon.537.
Grossman P, Niemann L, Schmidt S, Walach H. Mindfulness-based stress reduction and health benefits: a meta-analysis. J Psychosom Res. 2004;57(1):35–43. doi:10.1016/S0022-3999(03)00573-7.
Kabat-Zinn J. Mindfulness-based interventions in context: past, present, and future. Clin Psychol (New York). 2003;10:144–56. doi:10.1093/clipsy.bpg016.
Shapiro SL, Carlson LE, Astin JA, Freedman B. Mechanisms of mindfulness. J Clin Psychol. 2006;62(3):373–86. doi:10.1002/jclp.20237.
Bishop SR, Lau M, Shapiro S, Carlson L, Anderson ND, Carmody J et al. Mindfulness: a proposed operational definition. Clin Psychol-Sci Pr. 2004;11:230–41. doi:10.1093/clipsy.bph077.
Jacobson E. Progressive relaxation. 2nd ed. Oxford: University of Chicago Press; 1938.
Jain S, Shapiro SL, Swanick S, Roesch SC, Mills PJ, Bell I et al. A randomized controlled trial of mindfulness meditation versus relaxation training: effects on distress, positive states of mind, rumination, and distraction. Ann Behav Med. 2007;33:11–21. doi:10.1207/s15324796abm3301_2.
Esch T, Fricchione GL, Stefano GB. The therapeutic use of the relaxation response in stress-related diseases. Med Sci Monit. 2003;9(2):RA23–34.
Hoffman JW, Benson H, Arns PA, Stainbrook GL, Landsberg G, Young JB, et al. Reduced sympathetic nervous system responsivity associated with the relaxation response. Science. 1982;215(4529):190–2.
Lazar SW, Bush G, Gollub RL, Fricchione GL, Khalsa G, Benson H. Functional brain mapping of the relaxation response and meditation. Neuroreport. 2000;11(7):1581–5.
Bohlmeijer E, Prenger R, Taal E, Cuijpers P. The effects of mindfulness-based stress reduction therapy on mental health of adults with a chronic medical disease: a meta-analysis. J Psychosom Res. 2010;68(6):539–44. doi:10.1016/j.jpsychores.2009.10.005.
Volpato E, Banfi P, Rogers SM, Pagnini F. Relaxation techniques for people with chronic obstructive pulmonary disease: a systematic review and a meta-analysis. Evid Based Complement Alternat Med. 2015; 2015. doi:10.1155/2015/628365.
Courtois I, Cools F, Calsius J. Effectiveness of body awareness interventions in fibromyalgia and chronic fatigue syndrome: a systematic review and meta-analysis. J Bodyw Mov Ther. 2015;19(1):35–56. doi:10.1016/j.jbmt.2014.04.003.
Feldman G, Greeson J, Senville J. Differential effects of mindful breathing, progressive muscle relaxation, and loving-kindness meditation on decentering and negative reactions to repetitive thoughts. Behav Res Ther. 2010;48(10):1002–11. doi:10.1016/j.brat.2010.06.006.
Cavanagh K, Strauss C, Forder L, Jones F. Can mindfulness and acceptance be learnt by self-help?: a systematic review and meta-analysis of mindfulness and acceptance-based self-help interventions. Clin Psychol Rev. 2014;34(2):118–29. doi:10.1016/j.cpr.2014.01.001.
Beatty L, Lambert S. A systematic review of internet-based self-help therapeutic interventions to improve distress and disease-control among adults with chronic health conditions. Clin Psychol Rev. 2013;33(4):609–22. doi:10.1016/j.cpr.2013.03.004.
Greenhalgh J, Dickson R, Dundar Y. Biofeedback for hypertension: a systematic review. J Hypertens. 2010;28(4):644–52. doi:10.1097/HJH.0b013e3283370e20.
Kreps GL, Neuhauser L. New directions in eHealth communication: opportunities and challenges. Patient Educ Couns. 2010;78(3):329–36. doi:10.1016/j.pec.2010.01.013.
Fish J, Brimson J, Lynch S. Mindfulness interventions delivered by technology without facilitator involvement: what research exists and what are the clinical outcomes? Mindfulness (N Y). 2016;7(5):1011–23. doi:10.1007/s12671-016-0548-2.
Spijkerman MP, Pots WT, Bohlmeijer ET. Effectiveness of online mindfulness-based interventions in improving mental health: a review and meta-analysis of randomised controlled trials. Clin Psychol Rev. 2016;45:102–14. doi:10.1016/j.cpr.2016.03.009.
Roy-Byrne PP, Davidson KW, Kessler RC, Asmundson GJ, Goodwin RD, Kubzansky L, et al. Anxiety disorders and comorbid medical illness. Gen Hosp Psychiatry. 2008;30(3):208–25. doi:10.1016/j.genhosppsych.2007.12.006.
Katon W, Lin EH, Kroenke K. The association of depression and anxiety with medical symptom burden in patients with chronic medical illness. Gen Hosp Psychiatry. 2007;29(2):147–55. doi:10.1016/j.genhosppsych.2006.11.005.
Sprangers MA, de Regt EB, Andries F, van Agt HM, Bijl RV, de Boer JB, et al. Which chronic conditions are associated with better or poorer quality of life? J Clin Epidemiol. 2000;53(9):895–907.
de Ridder D, Geenen R, Kuijer R, van Middendorp H. Psychological adjustment to chronic disease. Lancet. 2008;372(9634):246–55. doi:10.1016/s0140-6736(08)61078-8.
Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions. Chichester: Wiley; 2008.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–84. doi:10.1136/jech.52.6.377.
Andersson E, Ljótsson B, Smit F, Paxling B, Hedman E, Lindefors N, et al. Cost-effectiveness of internet-based cognitive behavior therapy for irritable bowel syndrome: results from a randomized controlled trial. BMC Public Health. 2011;11(1):215. doi:10.1186/1471-2458-11-215.
Arroll MA, Attree EA, Marshall CL, Dancey CP. Pilot study investigating the utility of a specialized online symptom management program for individuals with myalgic encephalomyelitis/chronic fatigue syndrome as compared to an online meditation program. Psychol Res Behav Manag. 2014;7:213–21. doi:10.2147/PRBM.S63193.
Beatty L, Koczwara B, Wade T. Evaluating the efficacy of a self-guided Web-based CBT intervention for reducing cancer-distress: a randomised controlled trial. Support Care Cancer. 2015;24(3):1043–51. doi:10.1007/s00520-015-2867-6.
Berman RL, Iris MA, Bode R, Drengenberg C. The effectiveness of an online mind-body intervention for older adults with chronic pain. J Pain. 2009;10(1):68–79. doi:10.1016/j.jpain.2008.07.006.
Carpenter KM, Stoner SA, Schmitz K, McGregor BA, Doorenbos AZ. An online stress management workbook for breast cancer. J Behav Med. 2014;37(3):458–68. doi:10.1007/s10865-012-9481-6.
Davis MC, Zautra AJ. An online mindfulness intervention targeting socioemotional regulation in fibromyalgia: results of a randomized controlled trial. Ann Behav Med. 2013;46(3):273–84. doi:10.1007/s12160-013-9513-7.
Devineni T, Blanchard EB. A randomized controlled trial of an internet-based treatment for chronic headache. Behav Res Ther. 2005;43(3):277–92. doi:10.1016/j.brat.2004.01.008.
Dowd H, Hogan MJ, McGuire BE, Davis MC, Sarma KM, Fish RA, et al. Comparison of an online mindfulness-based cognitive therapy intervention with online pain management psychoeducation: a randomized controlled study. Clin J Pain. 2015;31(6):517–27. doi:10.1097/AJP.0000000000000201.
Hansen MM. A feasibility pilot study on the use of complementary therapies delivered via mobile technologies on Icelandic surgical patients' reports of anxiety, pain, and self-efficacy in healing. BMC Complement Altern Med. 2015;15:92. doi:10.1186/s12906-015-0613-8.
Kleiboer A, Sorbi M, van Silfhout M, Kooistra L, Passchier J. Short-term effectiveness of an online behavioral training in migraine self-management: a randomized controlled trial. Behav Res Ther. 2014;61:61–9. doi:10.1016/j.brat.2014.07.009.
Ljótsson B, Andersson G, Andersson E, Hedman E, Lindfors P, Andréewitch S, et al. Acceptability, effectiveness, and cost-effectiveness of internet-based exposure treatment for irritable bowel syndrome in a clinical sample: a randomized controlled trial. BMC Gastroenterol. 2011;11(1):1. doi:10.1186/1471-230X-11-110.
Ljotsson B, Atterlof E, Lagerlof M, Andersson E, Jernelov S, Hedman E, et al. Internet-delivered acceptance and values-based exposure treatment for fibromyalgia: a pilot study. Cogn Behav Ther. 2014;43(2):93–104. doi:10.1080/16506073.2013.846401.
Ljotsson B, Falk L, Vesterlund AW, Hedman E, Lindfors P, Ruck C, et al. Internet-delivered exposure and mindfulness based therapy for irritable bowel syndrome-a randomized controlled trial. Behav Res Ther. 2010;48(6):531–9. doi:10.1016/j.brat.2010.03.003.
Ljotsson B, Hedman E, Andersson E, Hesser H, Lindfors P, Hursti T, et al. Internet-delivered exposure-based treatment vs. stress management for irritable bowel syndrome: a randomized trial. Am J Gastroenterol. 2011;106(8):1481–91. doi:10.1038/ajg.2011.139.
Ljotsson B, Hesser H, Andersson E, Lackner JM, El Alaoui S, Falk L, et al. Provoking symptoms to relieve symptoms: a randomized controlled dismantling study of exposure therapy in irritable bowel syndrome. Behav Res Ther. 2014;55:27–39. doi:10.1016/j.brat.2014.01.007.
Olsson EM, El Alaoui S, Carlberg B, Carlbring P, Ghaderi A. Internet-based biofeedback-assisted relaxation training in the treatment of hypertension: a pilot study. Appl Psychophysiol Biofeedback. 2010;35(2):163–70. doi:10.1007/s10484-009-9126-x.
Ström L, Pettersson R, Andersson G. A controlled trial of self-help treatment of recurrent headache conducted via the internet. J Consult Clin Psychol. 2000;68(4):722–7. doi:10.1037//0022-006X.68.4.722.
Krusche A, Cyhlarova E, King S, Williams JMG. Mindfulness online: a preliminary evaluation of the feasibility of a web-based mindfulness course and the impact on stress. BMJ Open. 2012;2(3):e000803. doi:10.1136/bmjopen-2011-000803.
Krusche A, Cyhlarova E, Williams JMG. Mindfulness online: an evaluation of the feasibility of a web-based mindfulness course for stress, anxiety and depression. BMJ Open. 2013;3(11):e003498. doi:10.1136/bmjopen-2013-003498.
Cavanagh K, Strauss C, Cicconi F, Griffiths N, Wyper A, Jones F. A randomised controlled trial of a brief online mindfulness-based intervention. Behav Res Ther. 2013;51(9):573–8. doi:10.1016/j.brat.2013.06.003.
Glück TM, Maercker A. A randomized controlled pilot study of a brief web-based mindfulness training. BMC Psychiatry. 2011;11(1):175. doi:10.1186/1471-244X-11-175.
Reid DT. Teaching mindfulness to occupational therapy students: pilot evaluation of an online curriculum. Can J Occup Ther. 2013;80(1):42–8. doi:10.1177/0008417413475598.
Dimidjian S, Beck A, Felder JN, Boggs JM, Gallop R, Segal ZV. Web-based mindfulness-based cognitive therapy for reducing residual depressive symptoms: an open trial and quasi-experimental comparison to propensity score matched controls. Behav Res Ther. 2014;63:83–9. doi:10.1016/j.brat.2014.09.004.
Del Re A, Flückiger C, Horvath AO, Symonds D, Wampold BE. Therapist effects in the therapeutic alliance–outcome relationship: a restricted-maximum likelihood meta-analysis. Clin Psychol Rev. 2012;32(7):642–9. doi:10.1016/j.cpr.2012.07.002.
Horvath AO, Symonds BD. Relation between working alliance and outcome in psychotherapy: a meta-analysis. J Couns Psychol. 1991;38(2):139.
Andersson G, Cuijpers P, Carlbring P, Riper H, Hedman E. Guided internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: a systematic review and meta-analysis. World Psychiatry. 2014;13(3):288–95. doi:10.1002/wps.20151.
Wagner B, Horn AB, Maercker A. Internet-based versus face-to-face cognitive-behavioral intervention for depression: a randomized controlled non-inferiority trial. J Affect Disord. 2014;152:113–21. doi:10.1016/j.jad.2013.06.032.
Lappalainen P, Granlund A, Siltanen S, Ahonen S, Vitikainen M, Tolvanen A, et al. ACT Internet-based vs face-to-face? A randomized controlled trial of two ways to deliver Acceptance and Commitment Therapy for depressive symptoms: an 18-month follow-up. Behav Res Ther. 2014;61:43–54. doi:10.1016/j.brat.2014.07.006.
Spek V, Cuijpers P, Nyklícek I, Riper H, Keyzer J, Pop V. Internet-based cognitive behaviour therapy for symptoms of depression and anxiety: a meta-analysis. Psychol Med. 2007;37(03):319–28. doi:10.1017/S0033291706008944.
Mohr DC, Siddique J, Ho J, Duffecy J, Jin L, Fokuo JK. Interest in behavioral and psychological treatments delivered face-to-face, by telephone, and by internet. Ann Behav Med. 2010;40(1):89–98. doi:10.1007/s12160-010-9203-7.
Griffiths F, Lindenmeyer A, Powell J, Lowe P, Thorogood M. Why are health care interventions delivered over the internet? A systematic review of the published literature. J Med Internet Res. 2006;8(2):e10. doi:10.2196/jmir.8.2.e10.
Gagneja APS, Gagneja KK, editors. Mobile health (mHealth) technologies. 2015 17th International Conference on E-health Networking, Application & Services (HealthCom); 2015: IEEE.
Buhrman M, Skoglund A, Husell J, Bergström K, Gordh T, Hursti T, et al. Guided internet-delivered acceptance and commitment therapy for chronic pain patients: a randomized controlled trial. Behav Res Ther. 2013;51(6):307–15. doi:10.1016/j.brat.2013.02.010.
Hesser H, Gustafsson T, Lundén C, Henrikson O, Fattahi K, Johnsson E, et al. A randomized controlled trial of Internet-delivered cognitive behavior therapy and acceptance and commitment therapy in the treatment of tinnitus. J Consult Clin Psychol. 2012;80(4):649–61. doi:10.1037/a0027021.
Trompetter HR, Bohlmeijer ET, Veehof MM, Schreurs KM. Internet-based guided self-help intervention for chronic pain based on acceptance and commitment therapy: a randomized controlled trial. J Behav Med. 2015;38(1):66–80. doi:10.1007/s10865-014-9579-0.
Hayes SC, Strosahl KD, Wilson KG. Acceptance and commitment therapy: an experiential approach to behavior change. New York: Guilford Press; 1999.
Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes and outcomes. Behav Res Ther. 2006;44(1):1–25. doi:10.1016/j.brat.2005.06.006.
Carmody J, Baer RA. Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. J Behav Med. 2008;31(1):23–33. doi:10.1007/s10865-007-9130-7.
De Vibe M, Bjørndal A, Tipton E, Hammerstrøm KT, Kowalski K. Mindfulness based stress reduction (MBSR) for improving health, quality of life, and social functioning in adults. Campbell Syst Rev. 2012; 8(3). doi:10.4073/csr.2012.3.
Cuijpers P, Van Straten A, Andersson G. Internet-administered cognitive behavior therapy for health problems: a systematic review. J Behav Med. 2008;31(2):169–77. doi:10.1007/s10865-007-9144-1.
Research2Guidance. mHealth App Developer Economics 2015: The current status and trends of the mHealth app market. 2015. www.research2guidance.com. Accessed March 17, 2016.
Acknowledgments
The authors acknowledge and thank for the contribution of Iara Meili, who supported the screening process.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was funded by the Swiss Cancer League (funding ID: KLS-3564-02-2015).
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
This article does not contain any studies with human participants performed by any of the authors.
Appendix
Appendix
Search strategy for EBSCO (PsycINFO, CINAHL, AMED)
(
TI (app OR mobile OR web OR online OR internet OR phone OR smart-phone OR smartphone OR cellphone OR cell-phone OR computer)
OR
AB (app OR mobile OR web OR online OR internet OR phone OR smart-phone OR smartphone OR cellphone OR cell-phone OR computer)
)
AND
(
TI (mindfulness OR meditat* OR stress-reduc* OR stress-manag* OR mind-body* OR breath* OR relax*)
OR
AB (mindfulness OR meditat* OR stress-reduc* OR stress-manag* OR mind-body* OR breath* OR relax* OR mbsr OR kabat zinn)
)
AND
(
TI (intervention OR rct OR (random* N3 trial*) OR treatment OR training OR exerci* OR practice OR clinical trial*)
OR
AB (intervention OR rct OR (random* N3 trial*) OR treatment OR training OR exerci* OR practice OR clinical trial*)
)
NOT
(
TI (abuse OR alcohol OR addiction OR smok* OR carbon* OR (acute N2 respiratory) OR asthma)
ORAB (abuse OR alcohol OR addiction OR smok* OR carbon* OR (acute N2 respiratory) OR asthma)
)
Limiters:
Date: January 1, 1990–April 7, 2015, 22:00
Source type: academic journals, journals, dissertations
Number of hits, 924
Duplicates found by EBSCOhost, 69
Number of unique hits, 855
Rights and permissions
About this article

Cite this article
Mikolasek, M., Berg, J., Witt, C.M. et al. Effectiveness of Mindfulness- and Relaxation-Based eHealth Interventions for Patients with Medical Conditions: a Systematic Review and Synthesis. Int.J. Behav. Med. 25, 1–16 (2018). https://doi.org/10.1007/s12529-017-9679-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-017-9679-7