
Abstract
Purpose
This study seeks to investigate and compare the efficacy of self-monitoring and implementation intentions—two post-intentional behaviour change techniques—for improving sleep hygiene behaviours and sleep outcomes in university students.
Method
Seventy-two undergraduate students completed baseline measures of four sleep hygiene behaviours (making the sleep environment restful, avoiding going to bed hungry/thirsty, avoiding stress/anxiety-provoking activities near bed time and avoiding caffeine in the evening), as well as the Pittsburgh sleep quality index (PSQI) and the insomnia severity index (ISI). Participants were randomly assigned to an active-control diary-keeping, self-monitoring condition or completed implementation intentions for each behaviour. Post-intervention measurement was completed 2 weeks after baseline.
Results
Repeated measures analyses of variance found significant main effects of time for improvements in making the sleep environment restful and avoiding going to bed hungry or thirsty, as well as PSQI and ISI scores. Non-significant interactions suggested no group differences on any variable, except for increasing avoidance of stress and anxiety-provoking activities before bed time, for which only implementation intentions were found to be effective. Attrition was higher amongst self-monitoring participants.
Conclusion
Both self-monitoring and implementation intentions appear to be promising behaviour change techniques for improving sleep hygiene and sleep. Future research should examine the acceptability of the two behaviour change techniques and the relationship with differential attrition, as well as effect size variations according to behaviour and technique. Researchers should investigate potential additive or interactive effects of the techniques, as they could be utilised in a complementary manner to target different processes in effecting behaviour change.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sleep hygiene refers to the performance of behaviours that are believed to support the body’s natural sleep–wake rhythms and promote restful sleep [1, 2]. Poor sleep has been linked to reduced mental, emotional and physical wellbeing, as well as daily functioning [3–5]. Students are known to have particularly poor sleep hygiene, sleeping patterns and sleep quality [3, 6–8]. Maintaining healthy sleep patterns in this population represents a challenge as they juggle gaining independence around their sleep, demanding academic and part-time work commitments, new social opportunities and irregular schedules [3, 6]. Additionally, students often consume stimulants and use mobile phones and computers late at night in the bedroom [9], which further impacts sleep. The development of sleep-based interventions for students is, therefore, an important area of research. In a sample of university students, the four sleep hygiene behaviours that were rated as priorities for intervention were making the sleep environment restful for sleeping (i.e. quiet, dark and a comfortable temperature, with electronic devices turned off), avoiding going to bed hungry or thirsty, avoiding caffeine in the evening and avoiding stress and anxiety-provoking activities before bed (e.g. stopping studying early enough to allow time to relax before bed, or scheduling problem-solving time for the next day) [8].
A prominent task within the field of health psychology recently has been the development of taxonomies of behaviour change techniques (BCTs) that can be used in interventions to target the stages and psychological processes theorised to be involved in the enactment of health behaviours [10–13]—for example, environmental control, self-efficacy enhancement, attitude shaping, motivation and intention formation, goal-setting, planning and self-monitoring. Although using multiple BCTs to target pre- and post-intentional predictors of behaviour is a common approach in behaviour-change interventions [14, 15], and may be justified to maximise the likelihood of real-world outcomes [16], a limitation is the difficulty of determining which BCT or combination was responsible for the effect [16]. In order to establish the best techniques or combinations, and to design the most effective and parsimonious interventions, it is first necessary to determine the efficacy of particular BCTs in isolation [11, 13, 14, 16].
To date, few studies have attempted to improve sleep hygiene using an isolated BCT. One of these studies investigated self-monitoring [17]. Self-monitoring (performed either deliberately or automatically) is a technique that impacts behaviour through a negative feedback loop by providing continuous information about deficits in achieving goal states [18], which makes it a good candidate for increasing performance of goal-driven behaviours. Examples of deliberate self-monitoring include recording performance of goal behaviours [19], reflecting on where behavioural performance was successful/unsuccessful and behavioural consequences [20]. In the aforementioned single BCT study, self-monitoring, which had previously been used in multi-technique interventions to improve sleep hygiene [21–23], was used to improve self-regulation deficitis [17], which have been linked to poor sleep and other health behaviours. Specifically, it was shown that self-monitoring alone, in the form of a daily sleep diary, reduced students’ engagement in stress and anxiety-provoking activities before bed. It was unclear why self-monitoring was not effective for the other two behaviours investigated—making the sleep environment restful and avoiding going to bed hungry or thirsty. One potential explanation is that participants did not specifically monitor their performance of the target behaviours. To better establish the efficacy of self-monitoring for improving sleep hygiene, replication is therefore needed, with a particular focus on ensuring that target behaviours are being monitored.
Beyond the initial lack of studies that have employed single BCTs for changing behaviour, another limitation within health behaviour change interventions is the lack of experimental comparisons of single BCTs using factorial designs [16]. This is necessary to determine the relative effectiveness of individual BCTs, before testing combinations of them. Building on the demonstration that self-monitoring alone is an effective technique for improving sleep hygiene, this study was concerned with the comparison to another post-intentional BCT targeting different psychological mechanisms, also shown to impact goal performance.
Implementation intentions are a BCT that prompts problem-solving and planning for goal achievement, beyond the conscious direction of attention to current performance and potential for improvement through “self-reactive influence”, which characterise self-monitoring [20]. They are a volitional BCT that aids translation of intention into behaviour and has been applied in theory of planned behaviour [24–27] and Health Action Process Approach-based interventions [28]. Implementation intentions are distinct from goal or motivational intentions (“I intend to perform x goal”) [29, 30], as they specifically entail when, where and how one intends to enact the goal behaviour. A critical implementation intentions feature that increases goal performance is an explicit conditional statement in the form of “If x antecedent occurs… then I will perform y behaviour” [31]. This mental stimulus–response association between anticipated cues and goal behaviours makes behaviour more automatic, reducing the need for conscious decision-making and for potential distraction from one’s goal, at the critical point when the behaviour needs to occur [29]. Perception, attention and memory for goal-related cues are also heightened [29], further increasing performance likelihood.
Evidence for the effectiveness of implementation intentions has been found across a range of health behaviours [26, 27, 32–35]. Nevertheless, investigating the effects on sleep hygiene is important in determining efficacy across health behaviours [16]. In one multi-technique, sleep-related study [23], a routine involving daily visualisation of implementation intentions (plus monitoring of sleep hygiene and sleep, and the use of environmental cues) improved sleep hygiene and sleep in daytime workers, relative to controls. This technique has not yet, however, been explored as a stand-alone BCT for improving sleep hygiene. This was the impetus for selecting it as the comparator for self-monitoring.
Aims and Hypotheses
The aims of the current study were firstly, to expand on the previously mentioned self-monitoring intervention [17] to determine whether the observed effects could be extended to additional sleep hygiene behaviours (specifically, the four behaviours rated as priority in the previous study) [8], and secondly, to compare the effects of self-monitoring with the alternate BCT of implementation intentions. Given its previous effectiveness in improving the sleep hygiene behaviour of avoiding anxiety/stress-provoking activities before bedtime, self-monitoring was used as an active control condition. Both selected techniques have previously been associated with medium effect sizes [17, 35]; however, due to methodological changes in the operationalisation of self-monitoring in this study and large variations in previous implementation intentions effects, it could not be predicted whether one BCT would demonstrate greater effectiveness. In line with previous research though, it was hypothesised that both BCTs would improve sleep hygiene. Based on mixed and inconclusive evidence regarding the impact of sleep hygiene behaviour on sleep outcomes [1, 2, 21, 23, 36–42], a final aim was to determine whether sleep hygiene improvements translated to better sleep outcomes.
Method
Recruitment, Procedure and Design
Australian university students participated in exchange for course credit, after responding to an advertisement for participants wishing to improve their sleep. The study was single-blinded. Participants were advised that they would be randomly assigned to one of two groups to complete unspecified tasks in a study investigating simple psychological techniques to improve sleep hygiene. Upon allocation to the condition, they were informed of days and durations of participation requirements. Researchers were aware of allocated conditions in order to check and instruct participation progress throughout the study schedules for each group, via standardised emails. All study components were completed online and researchers only had participant contact via email. The University’s Human Research Ethics Committee granted ethical approval.
Participants commenced the study on a day of their own choosing (weekday or weekend). The 15-day study schedule ran over weekdays and weekends. Although differences in sleep patterns between weekdays and weekends were likely, in order to avoid skewing the results, baseline and follow-up measurement periods referred to the previous 2 weeks, including weekdays and weekends, for all participants.
Participants were randomly allocated to the active-control, diary-keeping group or the experimental, implementation intentions group, using the random number generator function in Microsoft Excel. Participants were assigned the next available identification number, with its attached condition, in the order in which they consented to participate. At baseline, participants completed demographic items and received a definition of sleep hygiene behaviours. They then rated their performance of the four target behaviours and completed sleep outcome measures. Following baseline measurement on day 1, diary-keeping participants were instructed to complete a daily online sleep diary via a weblink from days 2 to 8, and emailed a reminder if this was more than 1 day overdue. The implementation intentions group completed implementation intentions after baseline measurement on day 1. On days 2 and 8 participants were emailed their self-formulated “if-then” sentences, asked to confirm whether they were correct and instructed to edit them if desired. The total time spent on all intervention components in each group was equivalent, at ∼30 min. Follow-up measurement was completed approximately 2 weeks from baseline. Upon follow-up survey completion, students received an electronic debriefing statement outlining the study aims, design and background literature. Participants were requested not to discuss the study with other actual or potential participants.
Intervention Materials
Self-Monitoring Sleep Diary
The diary comprised items from the Pittsburgh sleep diary [43] (employed by Todd and Mullan [17]); e.g. bed, sleep and wake times, sleep disturbances/awakenings, an overall subjective rating of sleep quality and mood and alertness upon wakening. Additionally, participants were asked whether they had completed each of the four target sleep hygiene behaviours on the previous day and to reflect upon whether not practicing them may have influenced waking during the night. Participants identified strengths and areas for improvement in their sleep preparation and recorded reflections on their sleep preparation and quality.
Implementation Intentions
Participants were given the same instructions to formulate two implementation intentions for each of the four target sleep hygiene behaviours (total of 8). The first instruction was to generate a situation when, or reason why, they might have difficulty enacting the behaviour. For example, for avoiding stress and anxiety-provoking activities before bed, “When tempted to work until bedtime on an assignment due the next day”. The second step was to nominate a behaviour consistent with the sleep hygiene goal, e.g. “Doing a relaxing activity for half-an-hour before bed”. Participants then noted when and where this was to occur, e.g. “when I am working late on an assignment due the next day” and “at home”. In the final step, participants were provided with an example and instructed to summarise their plan in a sentence taking the form “If [insert situation], then I will [insert solution]”, e.g. “If I am working late on an assignment, I will take half an hour to listen to relaxing music before bed”.
Measures
Sleep Hygiene Performance
Sleep hygiene behaviours were measured using an adapted version of a theory of planned behaviour-based scale developed by Kor and Mullan [8]. The primary reason for selecting this measure over alternate measures of sleep hygiene was to maintain consistency with the previous studies [8, 17] upon which this study was designed to build and to allow for more accurate and specific measurement of the frequency of each individually targeted sleep hygiene behaviour—making the sleep environment restful, avoiding going to bed hungry or thirsty, avoiding stress and anxiety-provoking activities before bed and avoiding caffeine within eight hours of bedtime. Participants indicated the number of days during the past 2 weeks that they performed each of the four target behaviours; e.g. “How many times during the past 2 weeks have you gone to bed hungry or thirsty?” Internal reliability analyses across the four behaviours indicated a Cronbach’s alpha of 0.01 at baseline and 0.45 at follow-up. Although low, this is consistent with Mastin et al.’s [1] suggestion that performance of different sleep hygiene behaviours is not necessarily expected to be related.
Sleep Outcomes
The Pittsburgh sleep quality index (PSQI) [44], a self-report questionnaire, uses 19 items to measure seven sleep components: subjective sleep quality, latency, duration, efficiency, disturbances, sleep medication use and daytime dysfunction. Participants respond regarding their sleep over the past month, however to match the timeframe of the present study, participants were asked to reflect on the past 2 weeks. The component scores produce a global PSQI score, ranging from 0 to 21, where higher scores reflect poorer sleep quality. Cut-off scores denote “good” (0–5) and “poor” sleepers (>5). The scale has been found to have good psychometric properties in healthy controls and sleep-disordered and depressed patients—including test–retest reliability (r = 0.85, <.001), discriminant validity and internal consistency (Cronbach’s alpha = 0.83) [44]. The Cronbach’s alphas for the current study were 0.55 at baseline and 0.52 at follow-up.
The insomnia severity index (ISI) [45], designed for insomnia screening, captures the functional impairment and emotional distress associated with poor sleep more effectively than the PSQI [45]. Although participants were not expected to meet diagnostic criteria, the ISI identifies sub-threshold insomnia, indicative of lower grade sleeping problems, common amongst students. Items measure difficulty falling asleep, maintaining sleep, waking early, satisfaction with sleep pattern, interference with daily functioning, perceived noticeability of impairment and level of distress at the sleep problem (e.g. “How worried/distressed are you about your current sleep problem?”). Total scores range from 0 to 28, and cut-offs denote no “clinically significant insomnia”, “sub-threshold insomnia”, “moderate” and “severe clinical insomnia”. The scale has demonstrated good concurrent and predictive validity, and internal consistency (α = 0.74–0.78) [45]. Cronbach’s alphas for this study were comparable at 0.79 (baseline) and 0.83 (follow-up).
Data Analysis
Power analyses were conducted for repeated-measures analyses of variance (ANOVA) using G*Power Version 3.1 software. A sample of N = 34 was recommended to detect medium-sized, within-subject main effects, based on α = .05, power of .80, within-subjects correlations of .50 and an expected medium-sized main effect (Cohen’s F = .25, d = .50)—the mid-point between previously reported effect sizes for self-monitoring (d = .42) [17] and implementation intentions (d = .59) [35]. Within–between interaction effect size calculations could not be based on prior effects, due to the exploratory nature of BCT group-difference investigations. However, in acknowledging the greater difficulty in detecting group differences using an active control, a sample of 100 was determined as necessary to detect a small effect (η 2 = .02, Cohen’s F = .1428). Sensitivity analyses were conducted to determine detectable effect sizes based on the final sample sizes, the found repeated-measures correlations, an alpha of .05 and power of .80.
Per-protocol analyses were first used to maximise chances of detecting effects. Differential attrition rates were tested for using Pearson chi-square tests of independence. Intention-to-treat analyses were conducted to account for attrition rates when interpreting the results. Independent samples t tests and Pearson chi-square tests of independence assessed whether the experimental groups differed at baseline on demographic or outcome variables, for continuous and categorical variables respectively.
Repeated measures ANOVAs were used to test for time, condition and interaction effects for each of the four sleep hygiene behaviours, PSQI and ISI scores. ANOVA (eta squared) and simple effect sizes (Cohen’s d) were calculated. Post hoc, paired samples t tests clarified the nature of significant interaction effects.
For per-protocol repeated measures analyses, missing data was dealt with using the list-wise deletion method in SPSS. For intention-to-treat analyses where there was missing follow-up data, the last-observation-carried-forward method was employed.
Results
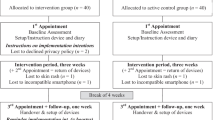
Participant flow is illustrated in Fig. 1. Final total sample sizes were 72 (per-protocol) and 90 (intention-to-treat), for all variables except the PSQI (N = 62; 77). Sensitivity analyses predicted the ability to detect main and interaction effect sizes ranging from η 2 = .01 to .04 (per-protocol analyses) and η 2 = < .01 to .02 (intention-to-treat analyses), corresponding to small effect sizes, according to Cohen’s guidelines for interpreting eta squared in factorial ANOVA (.02 = small, .13 = medium, and .26 = large) [46, 47].

Participant flow diagram
Attrition was significantly higher for the diary-keeping group (n = 14) than the implementation intentions group (n = 4; χ 2(1) = 5.89, p = .015). Final group sizes for per-protocol analyses were 33 and 39 respectively. There were no baseline differences between those who dropped out and those who completed the study for any demographic or outcome variable.
Of the per-protocol sample (N= 72), 53 participants were female; the mean age was 20.7 years (SD = 5.8; range = 17–49). The majority of the sample were Asian (51 %) or Caucasian (35 %); lived at home with family and had their own bedroom (n = 50; 69 %); and slept alone every night (n = 56; 78 %).
Sample-wide baseline means for all outcome variables are shown in Table 1. Sixty-four participants completed baseline PSQI items satisfactorily in order to calculate a global PSQI score. Most of the sample (n = 54, 84 %) were classified as “poor sleepers”. Mean sleep latency was 39.2 min (n = 71, SD = 37.4, range = 3–200). Participants slept an average of 7.45 h per night (n = 65, SD = 1.5, range = 3.2–12), with a mean sleep efficiency of 87.7 % (n = 65, SD = 8.7, range = 63.3–100). According to the ISI, most participants were classed as having “sub-threshold insomnia” (n = 42, 58 %); 21 (29 %) had “no insomnia”, 8 (11 %) had “moderate insomnia” and 1 had “severe insomnia”. There were no baseline differences between groups for any demographic or outcome variable.
Experimental Results
Per-Protocol
A small main effect of time for making the sleep environment restful and a large main effect for avoiding going to bed hungry/thirsty, combined with an absence of interaction effects, suggested that both BCTs were effective for increasing performance of these behaviours (see Table 2). There were no main effects for avoiding caffeine or avoiding stress-and-anxiety-provoking activities, however there was a significant interaction effect for the latter behaviour. Simple effect analyses showed only implementation intentions were effective for improving avoidance of stress/anxiety-provoking activities (self-monitoring: MD = −.54, t(32) = 1.026, p = .315, d = .16; implementation intentions: MD= 1.15, t(38) = 2.351, p = .024, d = .39). Global PSQI and ISI scores showed large main effects of improvement across time, with a lack of interaction effects, suggesting no group differences on these outcomes.
Simple effect sizes in the self-monitoring group were medium for making the sleep environment restful and avoiding hunger/thirst, and approaching medium for PSQI and ISI improvements (see Table 1). In the implementation intentions group, effects were small for making the sleep environment restful and avoiding stress/anxiety-provoking activities and medium-sized for avoiding going to bed hungry/thirsty, the PSQI and the ISI.
Intention-to-Treat
The same pattern of test results was observed. Main effect sizes reduced from large to medium for avoiding hunger/thirst and the PSQI.
Discussion
The purpose of this study was to assess and compare the effectiveness of self-monitoring and implementation intentions as separate BCTs for improving sleep hygiene and sleep outcomes. The hypothesis that both BCTs would be effective was supported through significant main effect findings and an absence of between-group differences, and reinforced through observation of simple effect sizes, for making the sleep environment restful, avoiding going to bed hungry or thirsty and both sleep outcome scales. The null between-group differences are a valuable finding as they suggest that both BCTs may be useful techniques of behaviour change. Establishing the efficacy of BCTs separately is an essential first step in selection of BCTs for intervention development. The findings also suggest that implementation intentions can be separated from self-monitoring in their effect on avoiding stress and anxiety-provoking activities. This is an important finding as it suggests implementation intentions may be the preferred BCT for this behaviour.
The results are consistent with previous research showing self-monitoring alone to be effective for improving sleep hygiene [17] and when combined with implementation intentions [23] and other techniques [21, 22]. The current research also adds to the literature by suggesting that sleep diaries may be more effective when targeted specifically to the sleep hygiene behaviours being addressed.
The non-significant effect of self-monitoring for avoidance of stress and anxiety-provoking activities near bed time is in contrast to Todd and Mullan’s [17] previous finding. This may be due to instruction differences allowing diary completion late at night rather than only in morning, as focusing on sleeping problems or pressure to meet the daily deadline may in itself have generated stress or anxiety close to bed time. Research into optimal timing of self-monitoring may therefore be warranted. Avoiding stress and anxiety-provoking activities may also be more difficult to achieve than the other behaviours, which entail more obvious steps to enact them. It may be especially difficult to stop engaging in a stressful activity and find a replacement behaviour, when this taps into trait or state anxiety, or worry behaviour [6, 38]. In this way, implementation intentions may have given participants an advantage compared to self-monitoring by helping participants identify replacement behaviours. Although, the lower effect size for this behaviour may still tap into its greater difficulty in controlling.
It is unclear why neither BCT was effective for avoidance of caffeine. Numerous participants claimed not to consume caffeine at baseline, possibly contributing to a ceiling effect for a section of the sample. At the same time, many participants who did consume caffeine believed that this was not problematic for them and did not intend to stop. As research suggests that people may differ in the effects caffeine has on their sleep [48], the relevance of this sleep hygiene behaviour may need to be considered on a individual basis.
While intention-to-treat analyses indicated the same pattern of results as per-protocol analyses, effect sizes were reduced. The greater reduction and higher attrition rate for diary-keepers in particular, may indicate lower acceptability of self-monitoring, related to the daily commitment [49]. As low acceptability can reduce efficacy [50, 51], future research might incorporate acceptability testing. It is possible that more individualized self-monitoring arrangements might be more acceptable [49].
Consistent with previous research, increases in sleep hygiene were also matched by improved sleep outcomes [1, 2, 21, 23]. It is promising that sleep hygiene improvements for just two-to-three behaviours, and for only a few days over 2 weeks, seemed to improve sleep. Nevertheless, further research is needed to clarify causal relationships between individual sleep hygiene behaviours and sleep outcomes.
Limitations
There are several limitations that should be considered when interpreting the results. Firstly, the final sample sizes were smaller than intended, thus the analyses may not have been sensitive enough to detect very small differences between BCTs, which are more expected within the context of an active control, equivalence trial. To be clearer on the absence of even very small effects across all variables, replication with a slightly larger sample would be optimal. However, sensitivity analyses based on actual repeated-measures correlations suggested there was enough power in intention-to-treat analyses to detect the minimum small effect size value across all outcome variables. Although for some variables per-protocol analyses were found to be only sensitive enough to detect effect sizes slightly above the small threshold, the test results were identical to intention-to-treat results, suggesting that slightly-reduced sensitivity did not affect the results. Furthermore, if such small differences between BCTs were to exist, their practical relevance would likely be limited.
Mixed-model analyses, capturing the intervention effects on a daily basis, may improve sensitivity. Future research employing this method should, however, control for the potential confound between the BCT of self-monitoring and daily measurements of sleep hygiene performance and sleep outcomes.
The present study employed self-monitoring as an active control; however, whilst self-monitoring was previously found effective for improving sleep hygiene behaviour, its efficacy had not been established across all the target behaviours. It is possible that learning about sleep hygiene for the first time influenced sleep hygiene improvements. Nevertheless, the efficacy of both BCTs is consistent with previous studies using no-treatment controls [17, 31, 35]. Furthermore, research suggests sleep hygiene knowledge only partially explains sleep hygiene practices [6] and does not guarantee performance [52, 53].
Self-report measures of sleep and hygiene may have biased the results [54]; however, alternatives (e.g. objective measures) would be difficult without compromising external validity and are less conducive to online research formats. The PSQI and the ISI are practical alternatives, which correlate well with objective measures [44, 45]. It is noted that the low PSQI internal reliability in the study contrasted with previous research [44], while other studies in similar populations have not reported reliability estimates [3, 6, 8]. Despite this, improvements were observed and PSQI and ISI scores correlated strongly, suggesting the measure still captured valuable sleep information.
Low internal reliability may be due to some PSQI components being less relevant to a young student population, mostly without severe sleep disorders (e.g. medication use and daytime functioning). As was found, despite “poor sleepers” dominating the sample, few had clinically significant insomnia. Thus, caution should also be used when generalising the effectiveness of these BCTs to more serious sleep disorders. Avoiding stress/anxiety-provoking activities in particular may tap into more pervasive difficulties with stress and anxiety, for which there is stronger evidence of links with sleep problems than the other three behaviours [38, 55, 56]. More extensive interventions may be required to target these underlying factors [38].
The behaviours targeted were based on previous research [8]; however, they are not exhaustive [1, 2, 39]. In particular, irregular sleep–wake hours and daytime napping, which are common amongst this population [6], may also warrant investigation. Due to the short-term nature of the study, long-term effects also remain unknown and deserve attention. Theory suggests that the behavioural automaticity generated by implementation intentions should have good temporal stability, providing there is contextual stability [29]. Encouragingly, previous research has shown effects lasting up to six months [32].
Finally, the effects of implementation intentions may have been underestimated. Attention was not given in the study instructions to the potential effects of giving participants behavioural goals with a positive or “approach” framing (e.g. “make the sleep environment restful”) versus a negative or “avoidance” framing, which the other three goals employed. An avoidance framing means people may be more likely to form implementation intentions with negating structures (i.e. “I will not do x behaviour”), as opposed to a positive structure (“I will do y behaviour”). Although participants in the current study were provided with positive structure exemplars, to be applied across all sleep hygiene goals, they were not told to avoid negating structures. Adriaanse et al. [57] demonstrated that implementation intentions employing a negating structure can sometimes have the ironic effect of increasing the undesired behaviour, in contrast to those with a positive structure or a replacement structure (“I will do y behaviour instead of x behaviour”). This may have contributed to the weaker and null effects for avoiding stress and anxiety-provoking activities and avoiding caffeine, where 22 and 20 % of implementation intentions formed employed a negating structure respectively. By contrast, only 2 % of implementation intentions for avoiding going to bed hungry or thirsty (the behaviour with the largest effects) used the negating structure, perhaps because this goal entailed an obvious, positive solution. Careful instructions and close monitoring are, therefore, needed to ensure that the appropriate structures are used to achieve the intended effects, whether for positive/approach or negative/avoidance-framed goals.
Implications, Future Directions and Conclusions
Future research could investigate improving effect sizes by combining self-monitoring and implementation intentions, and exploring other BCTs and multi-technique designs. Whether the comparative effects of self-monitoring and implementation intentions extend to different sleep-impaired populations (e.g. shift-workers) or other health behaviours should also be explored [16]. Potential moderators of BCT effects might be considered—e.g. conscientiousness and strong planning skills might negate the effect of implementation intentions [58, 59], whilst strong executive function might reduce self-monitoring effects.
Both BCTs are simple and conveniently deliverable online, without practitioner contact, making them cost-effective and viable interventions for diverse populations. The results have additional implications for health behaviour change theory—for example, by implying that interventions based on an extended Health Action Process Approach (HAPA) model [28, 60] may be effective, as they nominate both implementation intentions and self-monitoring/regulation (plus self-efficacy) as important yet separate, proximal predictors of behaviour. Overall, this study represents an important first step in disentangling the effects of distinct BCTs for particular behaviours, which is necessary for effective and efficient behaviour change intervention design.
References
Mastin DF, Bryson J, Corwyn R. Assessment of sleep hygiene using the sleep hygiene index. J Behav Med. 2006;29:223–7.
Stepanski EJ, Wyatt JK. Use of sleep hygiene in the treatment of insomnia. Sleep Med Rev. 2003;7:215–25.
Pilcher JJ, Ginter DR, Sadowsky V. Sleep quality versus sleep quantity: relationships between sleep and measures of health, well being and sleepiness in college students. J Psychosom Res. 1997;42:583–96.
Medeiros A, Mendes D, Lima P, Araujo J. The relationships between sleep-wake cycle and academic performance in medical students. Biol Rhythm Res. 2001;32:263–70.
Wolfson AR, Carskadon MA. Sleep schedules and daytime functioning in adolescents. Child Dev. 1998;69:875–87.
Brown F, Buboltz WC, Soper B. Relationship of sleep hygiene awareness, sleep hygiene practices, and sleep quality in university students. Behav Med. 2002;28:33–8.
Medeiros ALD, Mendes DB, Lima PF, Araujo JF. The relationships between sleep-wake cycle and academic performance in medical students. Biol Rhythm Res. 2001;32:263–70.
Kor K, Mullan B. Sleep hygiene behaviours: an application of the theory of planned behaviour and the investigation of perceived autonomy support, past behaviour and response inhibition. Psychol Health. 2011;26:1208–24.
Dahl RE, Lewin DS. Pathways to adolescent health sleep regulation and behavior. J Adolesc Health. 2002;31:175–84.
Abraham C, Kok G, Schaalma H, Luszczynska A. Health promotion. In: Martin PR, Cheung F, Kyrios M, Littlefield L, Knowles L, Overmier M, et al., editors. The international association of applied psychology handbook of applied psychology. Oxford: Wiley-Blackwell; 2010.
Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008;27:379–87.
Michie S, Johnston M, Francis J, Hardeman W, Eccles M. From theory to intervention: mapping theoretically derived behavioural determinants to behaviour change techniques. Appl Psychol Int Rev. 2008;57:660–80.
Michie S, Johnston M, Abraham C, Francis J, Eccles MP. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46:81–95.
Michie S, Abraham C. Interventions to change health behaviours: evidence-based or evidence-inspired? Psychol Health. 2004;19:29–49.
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new medical research council guidance. Int J Nurs Stud. 2013;50:587–92.
Peters G-JY, de Bruin M, Crutzen R. Everything should be as simple as possible, but no simpler: towards a protocol for accumulating evidence regarding the active content of health behaviour change interventions. Health Psychol Rev. 2013. doi:10.1080/17437199.2013.848409.
Todd J, Mullan B. The role of self-monitoring and response inhibition in improving sleep behaviours. Int J Behav Med. 2014;21:470–7.
Carver CS, Scheier MF. Control theory: a useful conceptual framework for personality-social, clinical, and health psychology. Psychol Bull. 1982;92:111–35.
Burke LE, Wang J, Sevick MA. Self-monitoring in weight loss: a systematic review of the literature. J Am Diet Assoc. 2011;111:92–102.
Bandura A. Health promotion from the perspective of social cognitive theory. Psychol Health. 1998;13:623–49.
Adachi Y, Sato C, Kunitsuka K, Hayama J. A brief behavior therapy administered by correspondence improves sleep and sleep-related behavior in poor sleepers. Sleep Biol Rythms. 2008;6:16–21.
Yamatsu K, Adachi Y, Kunitsuka K, Yamagami T. Self-monitoring and bibliotherapy in brief behavior therapy for poor sleepers by correspondence. Sleep Biol Rythms. 2004;2:73–5.
Loft MH, Cameron LD. Using mental imagery to deliver self-regulation techniques to improve sleep behaviors. Ann Behav Med. 2013;46:260–72.
Higgins A, Conner M. Understanding adolescent smoking: the role of the theory of planned behaviour and implementation intentions. Psychol Health Med. 2003;8:173–86.
Gratton L, Povey R, Clark‐Carter D. Promoting children’s fruit and vegetable consumption: interventions using the theory of planned behaviour as a framework. Br J Health Psychol. 2007;12:639–50.
Orbell S, Hodgkins S, Sheeran P. Implementation intentions and the theory of planned behavior. Pers Soc Psychol Bull. 1997;23:945–54.
Sheeran P, Orbell S. Implementation intentions and repeated behaviour: augmenting the predictive validity of the theory of planned behaviour. Eur J Soc Psychol. 1999;29:349–69.
Sniehotta FF, Scholz U, Schwarzer R. Bridging the intention-behaviour gap: planning, self-efficacy, and action control in the adoption and maintenance of physical exercise. Psychol Health. 2005;20:143–60.
Gollwitzer PM. Implementation intentions: strong effects of simple plans. Am Psychol. 1999;54:493–503.
Gollwitzer PM. Goal achievement: the role of intentions. Eur Rev Soc Psychol. 1993;4:141–85.
Armitage CJ. A volitional help sheet to encourage smoking cessation: a randomized exploratory trial. Health Psychol. 2008;27:557–66.
Luszczynska A. An implementation intentions intervention, the use of a planning strategy, and physical activity after myocardial infarction. Soc Sci Med. 2006;62:900–8.
Prestwich A, Lawton R, Conner M. The use of implementation intentions and the decision balance sheet in promoting exercise behaviour. Psychol Health. 2003;18:707–21.
Verplanken B, Faes S. Good intentions, bad habits, and effects of forming implementation intentions on healthy eating. Eur J Soc Psychol. 1999;29:591–604.
Gollwitzer PM, Sheeran P. Implementation intentions and goal achievement: a meta-analysis of effects and processes. In: Zanna MP, editor. Advances in experimental social psychology. San Diego: Elsevier; 2006. p. 69–119.
LeBourgeois MK, Giannotti F, Cortesi F, Wolfson AR, Harsh J. The relationship between reported sleep quality and sleep hygiene in Italian and American adolescents. Pediatrics. 2005;115(Supplement 1):257–65.
Morin CM, Hauri PJ, Espie CA, Spielman AJ, Buysse DJ, Bootzin RR. Nonpharmacologic treatment of chronic insomnia. An American academy of sleep medicine review. Sleep. 1999;22:1134–56.
Ebben MR, Spielman AJ. Non-pharmacological treatments for insomnia. J Behav Med. 2009;32:244–54.
Vyas UK. Non-pharmacological management of insomnia. Br J Med Pract. 2013;6:a623.
Bonnet MH, Arand D. Caffeine use as a model of acute and chronic insomnia. Sleep. 1992;15:526–36.
Thimgan MS, Suzuki Y, Seugnet L, Gottschalk L, Shaw PJ. The perilipin homologue, lipid storage droplet 2, regulates sleep homeostasis and prevents learning impairments following sleep loss. PLoS Biol. 2010;8:1–13.
Karacan I, Thornby J, Anch M, Booth G, Williams R, Salis P. Dose-related sleep disturbances induced by coffee and caffeine. Clin Pharmacol Ther. 1976;20:682–9.
Monk TH, Reynols CF, Kupfer DJ, Buysse DJ, Coble PA, Hayes AJ, et al. The Pittsburgh sleep diary. J Sleep Res. 1994;3:111–20.
Buysse DJ, Reynolds C, Monk T, Berman S, Kupfer D. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213.
Bastien CH, Vallieres A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2:197–307.
Cohen J. Statistical power analysis for the behavioral sciences 2nd ed. New Jersey: Lawrence Erlbaum Associates; 1988.
Bakeman R. Recommended effect size statistics for repeated measures designs. Behav Res Methods. 2005;37:379–84.
Retey J, Adam M, Khatami R, Luhmann U, Jung H, Berger W, et al. A genetic variation in the adenosine A2A receptor gene (ADORA2A) contributes to individual sensitivity to caffeine effects on sleep. Clin Pharmacol Ther. 2007;81:692–8.
Burke LE, Swigart V, Turk MW, Derro N, Ewing LJ. Experiences of self-monitoring: successes and struggles during treatment for weight loss. Qual Health Res. 2009;19:815–28.
Bartholomew LK, Parcel GS, Kok G, Gottlieb NH, Fernandez ME. Planning health promotion programs: an intervention mapping approach. 3rd ed. San Francisco: Jossey-Bass; 2011.
Chambless DL, Hollon SD. Defining empirically supported therapies. J Consult Clin Psychol. 1998;66:7.
Lacks P, Rotert M. Knowledge and practice of sleep hygiene techniques in insomniacs and good sleepers. Behav Res Ther. 1986;24:365–8.
Holbrook MI, White MH, Hutt MJ. Increasing awareness of sleep hygiene in rotating shift workers: arming law-enforcement officers against impaired performance. Percept Mot Skills. 1994;79:520–2.
Murdock B. The serial position effect of free recall. J Exp Psychol. 1962;64:482–8.
Alfano CA, Ginsburg GS, Kingery JN. Sleep-related problems among children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry. 2007;46:224–32.
Ramsawh HJ, Stein MB, Belik S-L, Jacobi F, Sareen J. Relationship of anxiety disorders, sleep quality, and functional impairment in a community sample. J Psychiatr Res. 2009;43:926–33.
Adriaanse MA, van Oosten JM, de Ridder DT, de Wit JB, Evers C. Planning what not to eat: ironic effects of implementation intentions negating unhealthy habits. Pers Soc Psychol Bull. 2011;37:69–81.
Simmons VN, Webb MS, Brandon TH. College-student smoking: an initial test of an experiential dissonance-enhancing intervention. Addict Behav. 2004;29:1129–36.
Sniehotta FF. Towards a theory of intentional behaviour change: plans, planning, and self-regulation. J Health Psychol. 2009;14:261–73.
Scholz U, Nagy G, Göhner W, Luszczynska A, Kliegel M. Changes in self-regulatory cognitions as predictors of changes in smoking and nutrition behaviour. Psychol Health. 2009;24:545–61.
Acknowledgments
The authors wish to thank the members of the former University of Sydney Health Psychology Research Lab and the current members of the Curtin University Health Psychology and Behavioural Medicine Group for their ideas and feedback throughout the study development, implementation and reporting. Additional thanks to Kirby Sainsbury for her support and advice.
Ethics Declaration
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study.
Conflict of Interest
Lucinda Mairs and Barbara Mullan declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mairs, L., Mullan, B. Self-Monitoring vs. Implementation Intentions: a Comparison of Behaviour Change Techniques to Improve Sleep Hygiene and Sleep Outcomes in Students. Int.J. Behav. Med. 22, 635–644 (2015). https://doi.org/10.1007/s12529-015-9467-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-015-9467-1