
Abstract
Background
There are racial health disparities in many conditions for which oxidative stress is hypothesized to be a precursor. These include cardiovascular disease, diabetes, and premature aging. Small clinical studies suggest that psychological stress may increase oxidative stress. However, confirmation of this association in epidemiological studies has been limited by homogenous populations and unmeasured potential confounders.
Purpose
We tested the cross-sectional association between self-reported racial discrimination and red blood cell (RBC) oxidative stress in a biracial, socioeconomically heterogeneous population with well-measured confounders.
Methods
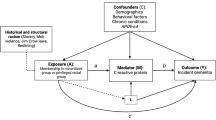
We performed a cross-sectional analysis of a consecutive series of 629 participants enrolled in the Healthy Aging in Neighborhoods of Diversity across the Life Span (HANDLS) study. Conducted by the National Institute on Aging Intramural Research Program, HANDLS is a prospective epidemiological study of a socioeconomically diverse cohort of 3,721 Whites and African Americans aged 30–64 years. Racial discrimination was based on self-report. RBC oxidative stress was measured by fluorescent heme degradation products. Potential confounders were age, smoking status, obesity, and C-reactive protein.
Results
Participants had a mean age of 49 years (SD = 9.27). In multivariable linear regression models, racial discrimination was significantly associated with RBC oxidative stress (Beta = 0.55, P < 0.05) after adjustment for age, smoking, C-reactive protein level, and obesity. When stratified by race, discrimination was not associated with RBC oxidative stress in Whites but was associated significantly for African Americans (Beta = 0.36, P < 0.05).
Conclusions
These findings suggest that there may be identifiable cellular pathways by which racial discrimination amplifies cardiovascular and other age-related disease risks.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Racial disparities in health are persistent, and in some cases worsening [1]. Reducing and eliminating these health disparities are major emphases of Healthy People 2010 and the Institute of Medicine. One factor in racial health disparities may be the chronic experience of racial discrimination [2]. Conditions associated with perceived racial discrimination are higher blood pressure, increased obesity, cardiovascular reactivity, worse self-reported health, and earlier morbidity (see, e.g., Williams and Mohammed 2009 for a review [2]). These conditions may be worsened by racial discrimination, in part, due to perceived racial discrimination as a psychological stressor. Judgment based on external factors, such as racial discrimination, has been shown to be a potent psychological stressor [3]. However, there has been limited research on the physiologic pathways through which racial discrimination may result in poor health outcomes.
Cellular oxidative stress is a candidate pathway that may link perceived racial discrimination and poor health outcomes. Oxidative stress is the process by which “free radicals” or reactive oxygen species damage cellular components including DNA, proteins, and lipids. “Oxidative stress” is the term for the imbalance between the production of reactive oxygen species and intrinsic protection mechanisms. There is a small literature suggesting that psychological stress may increase oxidative stress. Oxidative stress is a pathogenic mechanism common to insulin resistance [4], hypertension [5], and cognitive aging [6]. If oxidative stress is causally associated with a psychological stressor such as racial discrimination, then disparities in psychological stress could help explain some health disparities.
Standard measures of oxidative stress (lipid peroxidation, protein carbonyls, and 8-hydroxyguanosine) reflect particular targets of oxidative stress (lipids, proteins, and DNA, respectively). We focus here on heme degradation, which is predominantly a measure of oxidative stress originating from the hemoglobin oxidative reactions in the red blood cells (RBCs) [7, 8]. These heme degradation reactive species are sensitive to changes in blood flow and tissue oxygenation that can be triggered by psychological stress through the sympathetic nervous system stress reaction. Over time, they could be chronically altered due to an allostatic load-type recalibration of the set point [9]. The reactive oxygen species formed in the RBCs can be released to the vascular system and other tissues [10] and may, therefore, be used as a marker of overall oxidative stress.
Although the relationship between perceived racial discrimination and oxidative stress has not been studied, studies have examined the relationship between oxidative stress and other forms of psychological stress [11–14]. Because oxidative stress is elevated in many diseases, if there is a reliable link between psychological distress and oxidative stress, it could provide a mechanism to explain the relationship between psychological distress and subsequent disease. In small studies, psychological stress has correlated with markers of oxidative stress. This was observed in both cross-sectional [13, 15] and longitudinal studies [14–17]. Also, in two small studies, those who underwent stress reduction or stress management had reduced oxidative stress levels compared to their own prior values [17] or those of a comparison group [18]. However, studies of the association between psychological distress and oxidative stress have been hampered by limited research designs including small, homogenous populations and inadequate confounder adjustment. Studying racial discrimination as a particularly deleterious type of psychological stress could add to this developing literature.
In the present investigation, we examined the cross-sectional association between self-reported racial discrimination and RBC oxidative stress in a demographically heterogeneous population with well-measured confounders. To our knowledge, this is the first investigation of the relationship between the perception of racial discrimination and oxidative stress.
Methods
Study Population
The Healthy Aging in Neighborhoods of Diversity across the Life Span (HANDLS) study is a prospective, population-based, longitudinal study [19]. The sample is a fixed cohort of participants based on household screenings from an area probability sample of 13 neighborhoods (areas of contiguous census tracts) in Baltimore City, Maryland. HANDLS is designed to examine the effects of race and socioeconomic status on risk factors for morbidity and mortality. The baseline sample of 3,721 adults aged 30–64 was recruited from 2004 to 2008. Data collection was performed in two phases in which participants were screened at their homes and physical examinations and other data were collected in Mobile Research Vehicles parked in participants’ neighborhoods. All participants provided informed consent, and the study was approved by the National Institute of Aging Institutional Review Board at the Medstar Research Institute. The sample for the current analysis consisted of (N = 629) consecutive participants (16 September 2004–19 July 2005) whose red blood cells had been analyzed for heme degradation as an ancillary study initiated after baseline recruitment began. The subset differed slightly from the full cohort. The ages, gender, and poverty level of the subset were statistically the same, but the full cohort is 59% Black while the subset with heme degradation is 49% Black.
Racial Discrimination Measure
Racial discrimination is assessed by, “Overall, how much have you experienced prejudice or discrimination because of your race?” with response possibilities of “not at all,” “a little/some,” or “a lot” [20]. For the multivariable models, we allowed more variability so that the categories remained “not at all,” “a little/some,” and “a lot.”
Oxidative Stress Measure
RBC oxidative stress was measured by determining the level of fluorescent heme degradation products for each participant according to standard measurement procedures [21]. Briefly, washed RBCs were lysed in deionized double distilled water. The emission fluorescence spectrum was measured from 400 nm to 600 nm at an excitation wavelength of 321 nm using a Perkin Elmer model LS 50B spectrofluorometer. A relative measure of fluorescent heme degradation products inside RBCs was determined from the emission at 465 nm [22]. The fluorescent heme degradation products are formed, in part, by reactive oxygen species like superoxide and peroxide ions released in the RBCs as a result of hemoglobin auto-oxidation. It is this same pool of reactive oxygen species that are also responsible for RBC membrane damage and the release of reactive oxygen species from the RBC. The fluorescent value is not an absolute measure of heme degradation products because the fluorescent signal is partially quenched by the level of hemoglobin present. It is for this reason that all measurements are made at a constant concentration of 50 μM of hemoglobin after lysis of RBCs. Under these conditions, fluorescent intensities in the range of 5–10 are found for normal healthy subjects. However, alterations within this normal range can reflect subclinical alterations in oxidative stress that can contribute to pathology. For diseases like sickle cell anemia where the hemoglobin molecule is less stable, values of heme degradation can be as high as 25–30 [23].
Covariates
We included variables that have been or are plausibly associated with either discrimination exposure or RBC oxidative stress, and might confound the relationship rather than mediate it [24, 25]. Age was measured in years. Race was determined by self-report as White or Black. Smoking status was self-reported. Smokers are divided into “never tried,” “tried but never consistently used,” “former user,” and “current user.” Obesity was characterized as those with a BMI of ≥30. High-sensitivity C-reactive protein (CRP) was measured by Quest Diagnostics. CRP is a measure of systemic inflammation and was log transformed due to non-normality.
Statistical Analysis
We tested first for mean and proportional differences for the demographic characteristics, health-related factors, racial discrimination measures, and RBC oxidative stress measures by race using Student’s t and Chi-square tests, respectively. For the primary analyses, we used multivariable regression models to estimate the association between racial discrimination and the level of heme degradation products as a measure of RBC oxidative stress unadjusted and then with appropriate adjustments.
To determine the impact of the additional variables on the parameter estimate for oxidative stress, we examined three different multiple regression models using pre-planned hierarchical effects. Because our main interest was in the association between racial discrimination and RBC oxidative stress, our first model includes just racial discrimination and RBC oxidative stress; model 2 includes RBC oxidative stress plus age and smoking history; and model 3 includes C-reactive protein and obesity. P values <0.05 were considered statistically significant, and all tests were two-sided. Analyses were conducted using STATA version 10 (College Station, TX).
Results
Table 1 presents the characteristics of the study population by race. Mean age was 48 (range, 30–64 by study design), and 47% were men. Forty-three percent were obese with equal percentages of White and African American participants obese. African Americans reported more racial discrimination than Whites. African Americans had higher RBC oxidative stress than Whites (see Table 1).
In univariate analyses, reported racial discrimination was associated with increased RBC oxidative stress (P < 0.05). In multivariable linear regression models, racial discrimination was still significantly associated with RBC oxidative stress (Beta = 0.55, P < 0.00) after adjustment for age, smoking, obesity, and level of C-reactive protein. When we stratified by race, racial discrimination was no longer associated with RBC oxidative stress for Whites but remained associated for African Americans (Table 2).
Discussion
This study is the first of which we are aware that tests an association between racial discrimination and a measure of oxidative stress. Although we found that self-report of racial discrimination was associated with increased RBC oxidative stress across the biracial sample, once we stratified by race, the association remained statistically significant for African Americans and not for Whites.
Oxidative stress includes multiple processes which can produce reactive species [26]. The associated functional impairment depends on where in the body these reactive species are produced and the availability of antioxidants. To help identify the nature of the relationship between oxidative stress and racial discrimination, we have used the level of fluorescent heme degradation products, which specifically measures oxidative stress originating from the RBCs [8]. The functional impairment of RBCs due to heme degradation involves altered RBC flow properties and the potential transfer of reactive species from RBCs to adjacent tissues [10]. This form of oxidative stress can result in significant RBC functional impairment, but depends on the stability of hemoglobin inside the cells [23] or exposure to hypoxia [22]. In this study, we have also measured smoking, obesity, and C-reactive protein, which are generally thought to be associated with oxidative stress. Interestingly, although there was a significant increase in heme degradation associated with increased racial discrimination, there was a decrease in heme degradation associated with obesity and smoking and no significant association between heme degradation and C-reactive protein (Table 1). The negative correlations shown in Table 2 for these covariates and the significant cross-sectional association between racial discrimination and heme degradation after controlling for covariates suggest that the functional impairment induced specifically by RBC oxidative stress is associated with racial discrimination. Moreover, we found that experience of racial discrimination did not increase RBC oxidative stress in Whites but did in African Americans.
These findings have implications for understanding health disparities. If increased RBC oxidative stress is associated in African Americans with experiencing racial discrimination, this could be one reason that diabetes, cardiovascular disease, and premature aging occur disparately in African Americans. Racial discrimination has been associated with hypertension [27], inflammation [28], e-selectin levels [29], and coronary calcification [30]. We hypothesize that in low SES populations and in minority populations with high rates of early-onset age-associated disease, the interaction of biologic, psychosocial, socioeconomic, environmental, and genetic factors may result in a phenotype of premature or accelerated aging. The underlying biologic processes may be the same as those postulated in theories of normal human aging. The Harman Free Radical Theory of Aging states that the accumulation of oxidative stress and damage to DNA and other cellular components and tissues over the lifespan lead to aging, disease, and death [25]. The health disparities induced phenotype of accelerated aging may be biologically similar to heritable “progeroid” syndromes whose manifestations include increased susceptibility to oxidative stress, premature accumulation of oxidative DNA damage, defects in DNA repair, and higher levels of biomarkers of oxidative stress and inflammation. Although genetic background, environmental, and behavioral factors influence health outcomes in all populations over the lifespan, health disparities may be the end product of an accelerated trajectory of dysfunctional interactions of these factors in populations at high risk or with high levels of risk exposure. As Williams et al. [2] describe, the research on racial discrimination and morbidity will benefit from an understanding of potential mechanisms for racial discrimination’s association with increased morbidity.
How could discrimination lead to greater oxidative stress? One of the likely pathways is the arousal of the stress reactivity systems. As examples, reports of discrimination have been associated with cardiovascular reactivity to acute stress [31] and higher basal level of cortisol [32]. Both exposure to chronic stress and excessive level of cortisol are in turn associated with greater oxidative stress [33, 34]. The increase in heme degradation, our primary measure of oxidative stress, can result from changes in blood flow or oxygen utilization that may be trigged by psychological stress. The same pool of reactive species formed in the RBCs that produces heme degradation can also leak out of the cell into the plasma where they can produce protein carbonyls and damage other cells and tissues.
Racial discrimination could theoretically be associated with RBC oxidative stress through health behavior pathways as well. For example, greater exposure to discrimination may lead to internalized racism and less self-care behaviors. Discrimination is linked to less slow wave sleep and greater fatigue [35]. Those experiencing overt racial discrimination could react by eating more comfort food [36] which is prooxidant and may increase oxidative stress burden.
Almost 40% of Whites in this sample reported “some” or “a little” racial discrimination. Other studies that have measured both White and Black perceived racial discrimination have found that 20–40% fewer Whites report racial discrimination than Blacks. In this regard, this HANDLS sample is similar with 81% of Blacks reporting some or a lot of racial discrimination and 43% of White reporting the same [37–39]. Baltimore is a majority Black city, and Whites may be reporting incidents such as a Black bus driver not stopping for them at a bus stop.
This is a preliminary report of an association between racial discrimination and oxidative stress, and as such, several limitations deserve mention. First, this study cannot infer causality because all measures were assessed contemporaneously. Second, our measure of racial discrimination is one question with ordinal responses. This is an important limitation. However, there are many one-item measures in the literature that are associated prospectively with important health outcomes such as health-related quality of life [40] and self-rated health [41]. Both of these single questions have been shown to be a useful measure of overall health for which a research participant sums his or her overall sense of a particular aspect of experience. Third, our measure of racial discrimination largely captures overt discrimination. There is no consensus on an optimal measure of perceived racial discrimination [2]. However, our measure does not address covert nor institutional discrimination such as living in a residentially segregated neighborhood [2, 42]. The majority of health effects of racial discrimination are likely due to such factors as neighborhood segregation, school segregation, differential sentencing by race, and other factors that are not necessarily reported by a discrimination scale. These institutional factors may or may not square with individual perception. We investigate the association between individual perception and a plausible biological mechanism that could be related to poor health outcomes. This perception of discrimination is a limitation in that it leaves out much discrimination, but it is also a strength as it may describe the effect of discrimination that is psychologically noticeable to participants and thus can be used as a model for the relationship between psychological stress and oxidative stress. Future research should include a multidimensional scale that can measure discrimination more comprehensively. Strengths of the present study are that it is the first we know of to examine the relationship between racial discrimination and oxidative stress, and that it has well-characterized data with well-measured confounders.
In summary, these findings suggest that there could be identifiable physiologic pathways by which psychological stress amplifies risk of cardiovascular and other age-related diseases. This study is a first step to understanding whether there is a relationship between racial discrimination and oxidative stress. To understand whether oxidative stress associated with racial discrimination affects health outcomes, we will need longitudinal data. The HANDLS study is designed to collect data for 20 years which will provide this opportunity.
Abbreviations
- RBC:
-
Red blood cells
- CRP:
-
C-reactive protein
References
Kung HC, Hoyert DL, Xu J, Murphy SL. Deaths: final data for 2005. Natl Vital Stat Rep. 2008;56:4–26.
Williams DR, Mohammed SA. Discrimination and racial disparities in health: evidence and needed research. J Behav Med. 2009;32:20–47.
Pascoe EA, Smart RL. Perceived discrimination and health: a meta-analytic review. Psychol Bull. 2009;135:531–54.
Meigs JB, Larson MG, Fox CS, Keaney Jr JF, Vasan RS, Benjamin EJ. Association of oxidative stress, insulin resistance, and diabetes risk phenotypes: the Framingham Offspring Study. Diabetes Care. 2007;30:2529–35.
de Champlain J, Wu R, Girouard H, Karas M, EL Midaoui A, Laplante MA, et al. Oxidative stress in hypertension. Clin Exp Hypertens. 2004;26:593–601.
Droge W, Schipper HM. Oxidative stress and aberrant signaling in aging and cognitive decline. Aging Cell. 2007;6:361–70.
Nagababu E, Mohanty JG, Bhamidipaty S, Ostera GR, Rifkind JM. Role of the membrane in the formation of heme degradation products in red blood cells. Life Sci. 2010;86:133–8.
Nagababu E, Rifkind JM. Heme degradation by reactive oxygen species. Antioxid Redox Signal. 2004;6:967–78.
McEwen BS. Stress, adaptation, and disease. Allostasis and allostatic load. Ann N Y Acad Sci. 1998;840:33–44.
Kiefmann R, Rifkind JM, Nagababu E, Bhattacharya J. Red blood cells induce hypoxic lung inflammation. Blood. 2008;111:5205–14.
Vlachopoulos C, Xaplanteris P, Alexopoulos N, Aznaouridis K, Vasiliadou C, Baou K, et al. Divergent effects of laughter and mental stress on arterial stiffness and central hemodynamics. Psychosom Med. 2009;71:446–53.
Kupper N, Gidron Y, Winter J, Denollet J. Association between type D personality, depression, and oxidative stress in patients with chronic heart failure. Psychosom Med. 2009;71:973–80.
Casado A, De Lucas N, Lopez-Fernandez E, Sanchez A, Jimenez JA. Lipid peroxidation, occupational stress and aging in workers of a prehospital emergency service. Eur J Emerg Med. 2006;13:165–71.
Eskiocak S, Gozen AS, Yapar SB, Tavas F, Kilic AS, Eskiocak M. Glutathione and free sulphydryl content of seminal plasma in healthy medical students during and after exam stress. Hum Reprod. 2005;20:2595–600.
Epel ES, Blackburn EH, Lin J, Dhabhar FS, Adler NE, Morrow JD, et al. Accelerated telomere shortening in response to life stress. Proc Natl Acad Sci USA. 2004;101:17312–5.
Sivonova M, Zitnanova I, Hlincikova L, Skodacek I, Trebaticka J, Durackova Z. Oxidative stress in university students during examinations. Stress. 2004;7:183–8.
Yadav RK, Ray RB, Vempati R, Bijlani RL. Effect of a comprehensive yoga-based lifestyle modification program on lipid peroxidation. Indian J Physiol Pharmacol. 2005;49:358–62.
Sharma H, Sen S, Singh A, Bhardwaj NK, Kochupillai V, Singh N. Sudarshan Kriya practitioners exhibit better antioxidant status and lower blood lactate levels. Biol Psychol. 2003;63:281–91.
Evans MK, Lepkowski JM, Powe NR, LaVeist T, Kuczmarski MF, Zonderman AB. Healthy aging in neighborhoods of diversity across the life span (HANDLS): overcoming barriers to implementing a longitudinal, epidemiologic, urban study of health, race, and socioeconomic status. Ethn Dis. 2010;20:265–75.
LaVeist TA, Rolley NC, Diala C. Prevalence and patterns of discrimination among U.S. health care consumers. Int J Health Serv. 2003;33:331–44.
Rifkind JM, Nagababu E, Ramasamy S, Ravi LB. Hemoglobin redox reactions and oxidative stress. Redox Rep. 2003;8:234–7.
Rifkind JM, Ramasamy S, Manoharan PT, Nagababu E, Mohanty JG. Redox reactions of hemoglobin. Antioxid Redox Signal. 2004;6:657–66.
Nagababu E, Fabry ME, Nagel RL, Rifkind JM. Heme degradation and oxidative stress in murine models for hemoglobinopathies: thalassemia, sickle cell disease and hemoglobin C disease. Blood Cells Mol Dis. 2008;41:60–6.
Block G, Dietrich M, Norkus EP, Morrow JD, Hudes M, Caan B, et al. Factors associated with oxidative stress in human populations. Am J Epidemiol. 2002;156:274–85.
Harman D. Aging: a theory based on free radical and radiation chemistry. J Gerontol. 1956;11:298–300.
Dalle-Donne I, Rossi R, Colombo R, Giustarini D, Milzani A. Biomarkers of oxidative damage in human disease. Clin Chem. 2006;52:601–23.
Steffen PR, McNeilly M, Anderson N, Sherwood A. Effects of perceived racism and anger inhibition on ambulatory blood pressure in African Americans. Psychosom Med. 2003;65:746–50.
Lewis TT, Aiello AE, Leurgans S, Kelly J, Barnes LL. Self-reported experiences of everyday discrimination are associated with elevated C-reactive protein levels in older African-American adults. Brain Behav Immun. 2010;24:438–43.
Friedman EM, Williams DR, Singer BH, Ryff CD. Chronic discrimination predicts higher circulating levels of E-selectin in a national sample: the MIDUS study. Brain Behav Immun. 2009;23:684–92.
Lewis TT, Everson-Rose SA, Powell LH, Matthews KA, Brown C, Karavolos K, et al. Chronic exposure to everyday discrimination and coronary artery calcification in African-American women: the SWAN Heart Study. Psychosom Med. 2006;68:362–8.
Richman LS, Bennett GG, Pek J, Siegler I, Williams Jr RB. Discrimination, dispositions, and cardiovascular responses to stress. Heal Psychol. 2007;26:675–83.
Richman LS, Jonassaint C. The effects of race-related stress on cortisol reactivity in the laboratory: implications of the Duke lacrosse scandal. Ann Behav Med. 2008;35:105–10.
Liu J, Mori A. Stress, aging, and brain oxidative damage. Neurochem Res. 1999;24:1479–97.
Mercanoglu G, Safran N, Uzun H, Eroglu L. Chronic emotional stress exposure increases infarct size in rats: the role of oxidative and nitrosative damage in response to sympathetic hyperactivity. Methods Find Exp Clin Pharmacol. 2008;30:745–52.
Thomas KS, Bardwell WA, Ancoli-Israel S, Dimsdale JE. The toll of ethnic discrimination on sleep architecture and fatigue. Heal Psychol. 2006;25:635–42.
Jackson JS, Knight KM. Race and self-regulatory health behaviors: the role of the stress response and the HPA axis in physical and mental health disparities. In: Schaie KW, Carstensen LL, editors. Social structures, aging, and self-regulation in the elderly. New York: Springer; 2006. p. 189–208.
Borrell LN, Diez RAV, Jacobs Jr DR. Perceived racial/ethnic discrimination, smoking and alcohol consumption in the multi-ethnic study of atherosclerosis (MESA). Prev Med. 2010;51:307–12.
Dailey AB, Kasl SV, Holford TR, Lewis TT, Jones BA. Neighborhood- and individual-level socioeconomic variation in perceptions of racial discrimination. Ethn Heal. 2010;15:145–63.
Krieger N, Sidney S. Racial discrimination and blood pressure: the CARDIA study of young black and white adults. Am J Public Health. 1996;86:1370–8.
The EuroQol group. EuroQol—a new facility for the measurement of health-related quality of life. Health Policy. 1990;16:199–208.
Martin LG, Schoeni RF, Freedman VA, Andreski P. Feeling better? Trends in general health status. J Gerontol B Psychol Sci Soc Sci. 2007;62:S11–21.
Barnes LL, de Leon CF, Lewis TT, Bienias JL, Wilson RS, Evans DA. Perceived discrimination and mortality in a population-based study of older adults. Am J Public Health. 2008;98:1241–7.
Acknowledgments
The National Institute on Aging Intramural Research Program of the National Institutes of Health supported this research. This publication was also made possible by 1KL2RR025006-01 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), as well as the John A. Hartford Foundation’s Building Academic Geriatric Nursing Capacity Award Program.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Szanton, S.L., Rifkind, J.M., Mohanty, J.G. et al. Racial Discrimination Is Associated with a Measure of Red Blood Cell Oxidative Stress: A Potential Pathway for Racial Health Disparities. Int.J. Behav. Med. 19, 489–495 (2012). https://doi.org/10.1007/s12529-011-9188-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-011-9188-z