
Abstract
This study, conducted in Tala Upazila (with > 0.3 million people) situated in a coastal district of Bangladesh, endeavors to identify the water quality situation and to assess people’s willingness to pay for safe drinking water; with a view to develop policies and programs to improve people’s access to safe and affordable drinking water in the coastal area. A total of 4500 households were surveyed for getting relevant information on willingness to pay of households, while water quality test was performed at 649 high dependent drinking water sources (basically tubewells) for identifying arsenic, salinity and iron concentration. Arsenic test results revealed that overall 36.5% of tested drinking water sources; 63% shallow tubewells and 14% deep tubewells were unsafe due to the presence of high levels of arsenic beyond Bangladesh standard. Electrical conductivity, which is a measure of salinity was very high in about 94% of the tested water sources; while 61% of tested sources had iron concentration higher than the Bangladesh standard. It is evident from the study that people are aware of these problems and on an average, 91% of the households were willing to pay for improving access to safe drinking water. Regardless of economic class, most of the households (75%) were willing to pay BDT 20.0 (0.25 USD) per week for 20 L safe water per day, which is equivalent to 2–6% of their respective monthly income to access safe drinking water. Logistic regression model identified monthly household income, tubewell ownership, distance of drinking water source, etc., as some determinants of households’ willingness to pay for safe drinking water. Encouraging peoples who are currently drinking arsenic-contaminated tubewell water to shift their sources to nearby arsenic free tubewells may be a cost-effective solution to this problem. Engaging community-based WatSan committee (a local committee comprising the user communities for supervising water and sanitation related activities) including local government representatives to design an affordable water tariff structure and generating sufficient revenue to cover the cost of water services in the community would be an effective and sustainable solution to improve access of safe and affordable drinking water in the coastal area of Bangladesh.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ensuring access to clean and affordable water is one of the greatest challenges in attaining Sustainable Development Goal 6 for most of the developing countries. Water is required for all usual domestic purposes, and is an essential ingredient of household, economic and agricultural activities (Wu et al. 2017); while inadequate water supplies prevent good sanitation and hygiene practices (Hunter et al. 2010; Dey et al. 2015). However, rapid population growth and migration together with changes in production and consumption are placing unsustainable demands on local and global water resources. Water contaminated with invisible toxic chemicals appears to be clean but may not be safe for drinking and cooking. Therefore, water should be clean and safe for both drinking and cooking purposes.
Globally, eight out of ten people without access to an improved drinking water source live in rural areas (WHO and UNICEF 2015). Similarly, regional and socio-economic disparities in access to quality water exist across Bangladesh (Dey and Rabbi 2013). Bangladesh has not been able to achieve 100% safe water supply coverage till now. Different agency reports show variability in national coverage of improved drinking water sources, i.e., the Government of Bangladesh (GoB 2016) reported 97.6% coverage, whereas the WHO and UNICEF (2015) reported only 87%. Access to safe and clean water is hindered by a number of factors such as arsenic contamination, high groundwater salinity in the coastal region, microbiological contamination of drinking water, declining groundwater levels, urban and industrial pollution, anticipated increase in human excreta load, and natural disasters (Dey et al. 2016). Groundwater, which is the main source of drinking water in Bangladesh, is being over-exploited and depleted in many areas beyond natural replenishment of aquifers from rainfall and river flow (Dey et al. 2017). Moreover, the presence of pit latrines, pollution sources (i.e., household waste dumping point/poultry/dairy farm), the absence of concrete-built platform facilitates the contamination of shallow aquifers, from which tubewells withdraw water; and thus deteriorates the groundwater quality (Dey et al. 2016). Therefore, problems still persist in many areas of Bangladesh not only because of inadequate quantity, but also in terms of quality of drinking water.
The discovery of widespread arsenic contamination in groundwater has effectively lowered access of tubewell water in rural settings of Bangladesh, including the south-west coastal region since the 1990s (Flanagan et al. 2012). The three south western districts of Bangladesh bordering India, namely Bagerhat, Satkhira and Kushtia, was first reported to be contaminated by arsenic in as early as 1996 (Kurokawa et al. 2001). Despite a significant overall progress has been made in supplying arsenic-free safe drinking water widespread, arsenic contamination of shallow aquifers is still a major challenge in ensuring safe drinking water in many areas of south-western part of Bangladesh. In recent years, salinity intrusion has also increasingly affected these sources, contributing to a scarcity of safe drinking water. The resultant sea-water intrusion is increasing salinity in coastal drinking water with severe health consequences to surrounding populations. Approximately 20 million people living along the coast are affected by varying degrees of salinity in drinking water obtained from various natural sources (Rasheed et al. 2016).
There is an acute shortage of safe drinking water in the villages of the Tala Upazila in the Satkhira district. Due to silting and drainage congestion of the Kobadak River, the major river in Tala, flooding and waterlogging during the rainy season is a major problem in many areas. Furthermore, surface water salinity (e.g., in rivers and ponds) is very high. Some areas have very deep aquifers, making it very difficult to install functional deep tubewells, and when installed, tubewells in some areas of Tala are severely affected by arsenic and iron contamination. There is, therefore, an urgent need for and improved and well-planned water project that ensures the availability of safe drinking water for the local people in the study area.
If rural water projects are to be sustainable and replicable, improved planning is required that includes a procedure to elicit information about the value placed on different levels of service (Tussupova et al. 2015). The concept of willingness to pay (WTP) is an important tool in designing an efficient and effective water project in rural areas. According to Tussupova et al. (2015), the WTP is a measure of the maximum amount that a person would be willing to pay for a service rather than do without. With this background in mind, there is a need to examine the demand and WTP for improved drinking water services according to income to help policy makers design an appropriate water tariff structure and generate sufficient revenue to cover the cost of water services (Asim et al. 2015). WTP also gives a monetary value to the benefits obtained from improving access to safe drinking water, which is of great use to policy makers in decision-making with respect to cost-benefit ratios for improving access to safe drinking water.
A BRAC Research and Evaluation Division (RED) research team recently conducted a study in Tala Upazila to understand more about the current situation and to devise appropriate and sustainable solutions to drinking water-related problems considering quality of water used and the WTP by the local community people. The goal of the research was to understand local problems and preferences about safe drinking water sources and the amount of money the people are prepared to pay for access to safe drinking water. The specific objectives of the study were to assess drinking water quality and identify the most used and preferred drinking water options, and to determine the WTP status and amount of money available to buy or access safe drinking water.
Methodology
Household-level information on socio-economic status, drinking water source, household water demand, preferred drinking water source, and WTP for improved drinking water supply was collected by survey in each Union of Tala Upazila in April and May 2015.
Study Area
The study was conducted in Tala Upazila of the Satkhira district, located in south-western coastal region of Bangladesh (Fig. 1). Geographically, the study area extends from 22°32′N to 22°50′N latitudes and 89°05′E to 89°20′E longitudes. All 12 unions of Tala Upazila, namely Khesra, Jalalpur, Dhandia, Khalilnagar, Sarulia, Magura, Nagarghata, Islamkati, Khalishkhali, Tentulia, Kumira, and Tala Sadar were covered for the study. The area of Tala Upazila is about 337.24 sq km. Number of households in Tala Upazila is about 72,465 (BBS 2013). Kobadak and Betna are the two main rivers of Tala. Like other areas of south-western Bangladesh, Tala has a tropical monsoon climate characterized by seasonal variations in rainfall, temperatures and humidity with an average annual rainfall of 1464 mm. Being a part of the most disaster-prone area of the country due to frequent cyclones, tidal surges, and flooding, silent and invisible disasters such as increased salinity, arsenic contamination, and waterlogging mostly affect local livelihoods, people, and their environments in Tala. According to the Bangladesh Poverty Maps 2010, about 35% of the southwestern coastal population is poor, which is much higher than the national rural average (Ahmed et al. 2010) that has made this situation more complex.

The study area
Sampling Procedure
The sample size estimation for the household survey was done following stratified random sampling procedure, where the selected Upazila was divided into two strata according to union severity ranking. To determine severity ranking of the unions, information was collected from in-depth interview (IDI) of stakeholders including BRAC WASH program personnel and through focus group discussion (FGD) with local people. In IDIs, questions were asked about which union is more severe as per their understanding, about availability of drinking water options in different unions, and where problem in water quality, e.g., arsenic, iron, salinity is high. Information on water crisis; distance to collect water, water selling business and economic condition was collected though FGD; as well as from the review of secondary literature including BRAC WASH program’s Household Census-2012. The range of the severity scale considering the above mentioned indicators was 0.0–3.0. A union with average above 2.0 point was considered as high severe union, whereas average value less or equal to 2.0 was considered as low severe union. The formula of sample size calculation is given below:
where n is the required sample size, z is the standard normal distribution with mean 0 and variance 1, α is the level of significance (0.05), 1 – β is the power of the test (0.90), p is the population proportion (assumed to be 0.50 since this would provide the maximum sample size), e is the degree of accuracy expressed as a proportion (0.03), d is the design effect (1.5).
The required sample size was calculated as 4372 households. After adjustment, 4500 households were proposed as desired sample size. Villages were selected randomly from each union. An interval sampling procedure was used to select households within each village. From the six most severe unions (Dhandia, Sarulia, Magura, Khesra, Jalalpur, Khalilnagar), 500 samples were selected from each union and 250 samples were selected from each less severe union (Nagarghata, Kumira, Tentulia, Tala Sadar, Islamkati, Khalishkhali).
Development of the Questionnaire
The questionnaire for conducting household surveys and collecting primary data was developed after consultation with appropriate specialists within the Research and Evaluation Division of BRAC. The major sections of the questionnaire were general information about the households, socio economic status of households, source of water, collection, demand and water quality related information, willingness to pay for drinking water, information on water source location, water test results and dependent households on a source. The draft questionnaire was shared with BRAC program personnel and multidisciplinary sector specialists for feedback and comments. The draft questionnaire was pre-tested and slightly modified as per feedback from the field. The final draft questionnaire also went through some internal and external review once again before being finalized.
Data Collection and Quality Control
Local enumerators, who were inhabitants of Tala Upazila, were selected to conduct baseline surveys. Selection was based on their previous record, relevant work experience, and educational qualifications. A week of rigorous training was given to enumerators in the local field office followed by a field test to acclimatize to the survey procedure and questionnaire.
Forty enumerators were selected for data collection. Enumerators were divided into four groups, each with ten members. Additionally, four monitors/supervisors were appointed to oversee their respective group’s work. To identify inconsistencies in the questionnaire, the four supervisors re-interviewed/re-checked/back checked at least 5% of completed questionnaires daily. Researchers and field management unit staff also rigorously visited the field to ensure quality data.
The location of surveyed households and their current drinking water sources in one union (Tala Sadar union) were recorded with a GPS receiver, which was later processed in ArcGIS to develop maps for visualization of dependency on water sources.
Data Analysis
Primary data from 4500 households were processed in STATA 12.1 for descriptive statistics. Tables and graphs were prepared in Microsoft Office Excel 2013. Processed data are represented as graphs, figures, tables and maps (ArcGIS 10 software).
Water Quality Analysis
In situ measurement of water quality parameter, such as salinity by Hach HQD digital Conductivity/TDS meter and arsenic by the Econo Quick (EQ) kit were carried out. The level of salinity (measure of EC), arsenic and iron was tested at 649 high dependent drinking water sources, most of which are tubewells. The sources which were being used by at least ten and more households as source of drinking water were considered as high dependent water sources. Drinking water sources of the remaining households (15%) were not considered for arsenic testing because tube-wells of these 15% households had already been tested within the last 1 year and were declared arsenic free. Before carrying out the water quality analysis, wells were pumped for five minutes to avoid stagnation of sampling water in the tubewell piping. Total iron concentration was analyzed with the colorimeter, to the nearest 0.01 mg/L, using the FerroVer method (Rebecca et al. 2009). Analysis was initiated with no dilution, and if the 3.30 mg/L limit was exceeded, was repeated sequentially with 2-, 5-, 10- and 20-fold dilutions. However, if the limit was exceeded when using the 20-fold dilution, total iron concentration was recorded as > 66.00 mg/L. Finally, ferrous iron concentration, to the nearest 0.01 mg/L, was measured by the colorimeter using 1,10-phenanthroline at dilution factors of 1, 2, 5, 10, and 25, as required based on a detection limit of 3.30 mg/L. Arsenic testing at high dependent sources was done using “Econo Quick (EQ) Arsenic Test Kit” made in the USA by Innovators for water quality testing (ITS). The EQ kit was preferred to use in field test because of its high accuracy (about 90%) of measuring arsenic status of the tube-wells (George et al. 2012). 50 mL of water sample was collected from each tubewell for Arsenic testing. Tartaric acid, which is the first reagent of the EQ kit mixed with small amounts of iron and nickel sulfate, used as catalysts, was added to the sample with a scoop. Then potassium peroxymonosulfate, which is the second reagent provided with the EQ kit was then added to the sample to oxidize any available hydrogen sulfide to prevent potential suppression of the signal. The EQ kit contains a temporary cap for shaking the sample to ensure the complete dissolution of tartaric acid before adding the final reagent, Zn powder which reduces inorganic arsenic compounds (As + 3 and As + 5) to arsine gas. A test strip was used to measure the arsine gas concentration in the water sample. When arsine gas comes in contact with the test strip, the Mercuric bromide indicator on the test strip changes in color from white to shades of yellow or brown. The test strip was matched to a calibrated color chart to obtain a quantitative measure of arsenic in the tested sample. The reference chart provided with the EQ kit displays the yellow to brown range of colors expected for As concentrations of 0, 10, 25, 50, 100, 200, 300, 500, and 1000 μg/L. To confirm the ground water arsenic contamination level by the EQ arsenic testing kit, 5% of collected water samples were picked randomly for laboratory validation, and were re-tested in NGO Forum for Public Health’s laboratory based in Dhaka. The samples were analyzed by flow-injection hydride generation atomic absorption spectrometry (FI-HG-AAS) method for arsenic detection. The minimum detection level for this method was 3.0 μg/L. For arsenic level detection, AAS of Shimadzu (model: AA-6300) was used at the laboratory (Rashid et al. 2016). We found 85% accuracy of the EQ kit reading for arsenic contents during laboratory test.
Results and Discussion
Demographic Profile of the Study Area
The socioeconomic and demographic profiles of the study area are presented in Table 1. 4,500 households were surveyed in total. The average family size was 4.1. About 42% of respondents never went to school, 23% attended to primary level and 30% to secondary level. The maximum literacy rate was found in Keshra and Sarulia unions (82%), whereas the literacy rate was lowest in the Tala Sadar union (76%). To determine the economic condition of the households, Bangladesh’s new poverty numbers at $1.90 per capita per day in 2011 purchasing power parity (PPP) prices were considered (World Bank 2016). Households earning 1.90 USD per capita per day were considered as ultra-poor, while households with daily per capita income of 1.9–2.50 USD and more than 2.50 USD were considered as poor and non-poor households, respectively. According to this classification, most of the households in Tala Upazila were ultra-poor (63%), with 33 and 4% poor and non-poor households, respectively. The main occupation of the household head was laboring (35%). Farming (31%), business (19%), and service industry (5%) were other notable occupations of the household heads. Most of the surveyed people (74%) were aged between 0 and 40 years.
In the study area, overall 14% people claimed that they have suffered from water borne diseases such as diarrhea, dysentery and cholera in last 15 days. It was found that about one-fourth of the surveyed people suffered from these water borne diseases in Nagarghata and Sarulia union, whereas less percent of people suffered from these diseases in Tala Sadar, Tentulia and Kumira union. Diarrhea was the most common single water-borne disease with 8% of the population in Tala suffering from it. 89% of households claimed that they had spent money on health in the last month where 51.4% households reportedly expended between 1001 and 2000 BDT (12.3–24.6 USD) for medical/health related issues.
Drinking Water Sources, Collection Process, and Demand
Almost all the households in Tala relied on shallow tubewells (STWs) and deep tubewells (DTWs) for collecting drinking water. Over two-thirds (about 70%) of the surveyed households in the study area used STWs for drinking purposes, of which 46% were using their own STWs. About 90% people in Khalilnagar, Tala Sadar, and Khesra unions used STWs for drinking purposes. In contrast, only 30% of households in Kumira union used STWs for drinking purposes.
On average, 22% households used DTWs as drinking water source, 13% using government-installed DTWs. DTWs were the main source of drinking water in Kumira union, where 69% of households used DTWs for drinking purposes. DTWs as a drinking water source were relatively less common in Khesra and Khalilnagar unions, with only 5% of households using DTWs for drinking purposes. On average, only 5% of households in the study area were found to rely on pond sand filters (PSFs) for drinking water collection. Notably, in Khalishkhali union, about 27% used PSFs for drinking purposes. Most of the STWs used as a drinking water source had a depth less than 50 m and only 14% of households in the study area used tubewells with a depth of 200 to > 300 m (47% in Kumira union and only 2% in Khesra union). Household daily drinking water demand was about 3–15, 16–20, and 21–115 L in 30, 37, and 33%, respectively.
Over half of the households (54%) collected drinking water from their own yards. In fact, 78% households reported collecting drinking water from either drinking water sources located in their own yard or from sources within five minutes walking distance. The time required to collect drinking water in different unions is shown in Fig. 2. Khalishkhali union was most vulnerable in terms of drinking water accessibility, as 16% of households reported taking 20–30 min or more to collect water on foot.

The time required to collect drinking water in different unions of Tala Upazila
Some unions such as Khesra, Jalalpur, and Kumira were more susceptible to this problem, with a significant percentage of households reporting 20–30 min or more walking time to collect water. A map showing the distances between the dependent households and drinking water collection points in a part of Tala union is presented in Fig. 3, confirming that some households needed to go long distance to collect drinking water.

Map showing distances between drinking water sources and dependent households in a part of Tala union
An interesting finding was that some households travel long distances although having a closer deep tubewell. For instance, some households in Rahimabad travel to Tala Sadar to reach a deep tubewell, although there was a much closer deep tubewell in Rahimabad. From FGDs it was identified that local people of Tala have their own preferences and reasons behind using a source for collecting drinking water. Actually, when people are habituated in collecting drinking water from a source for a long period of time; and find the source safe, they usually do not want to shift their drinking water source. Besides, some deep tubewells reportedly had better quality of water than others, according to the local peoples. Social relationship may also influence in collecting water from far distances. These may be the possible reasons that are why some households in Rahimabad travel to Tala to fetch water although having a deep tubewell at closer distance.
Water Quality Status of Some High-Dependent Water Sources: Seeking the Reasons Behind Willingness to Pay
To better understand the water quality at some of the drinking water sources and to identify the reasons behind households’ WTP, a few high-dependent drinking water sources across Tala Upazila were selected to measure arsenic, salinity and iron concentration.
Arsenic in Drinking Water
Arsenic testing was conducted at high-dependent drinking water sources situated across the study area. Union-wise arsenic contamination is shown in Fig. 4. It is evident that in all the unions, a significant percentage of sources were unsafe, exceeding the permissible limit (Bangladesh standard: 50 ppb arsenic) in drinking water. The highest percentage of unsafe water sources due to the presence of arsenic was identified in Khesra union followed by Dhandia, Sarulia, Magura, and Islamkati. Arsenic contamination was found least common in Kumira. In most unions, unsafe tubewells were scattered throughout the union. In some unions, such as Khesra and Khalishkhali, unsafe water sources were concentrated at specific locations. Considering allowable standard for safe arsenic level in drinking water (BGD limit: 50 ppb), 36.5% of tested tubewells were deemed unsafe, which is higher than the reported percentage of country-wide unsafe tubewells in Bangladesh (12.6% unsafe) (BBS and UNICEF 2009). Arsenic contamination was higher in STWs (63%) than DTWs (> 150 m deep) (14%). However, considering the WHO standard (Allowable limit: 10 ppb), a staggering 74% of tested drinking water sources were unsafe in the study area. A recent study conducted in the nearby district, Gopalganj also shows similar findings that in case of most of the tubewells, most of the water quality parameters including Arsenic (As), EC and Iron (Fe) exceeds the limits stipulated by different standards for drinking water (Rahman et al. 2017).

Arsenic contamination status of tested water sources (STW, DTW) in different unions of Tala Upazila
The study has discovered that 14% of DTWs in the study area are contaminated by high level of arsenic which is unsafe for drinking. This is an alarming news to the practitioners, researcher and policy makers who are working to protect the deep aquifers, which is considered as the main source of safe drinking water and generally thought to be free from arsenic contamination. It was also found that 93% tubewells used as primary source of water for drinking purpose had no color-marked (neither red as unsafe nor green as safe to drink) to identify whether arsenic free or contaminated, and 71% of respondents did not know whether tubewells used for dinking were tested for identifying arsenic contamination in the last one/two years. This is likely a forgotten issue or lack of awareness among the community people about the adverse effect of arsenic on health. In addition, results show that knowledge about the health benefits of drinking arsenic-safe water are still not clear in the community. A study conducted in Bangladesh after 5–6 years of detection showed that over 60% of people have no idea about arsenic (Misbahuddin 2015). Therefore, targeting the mostly affected areas for improving access of arsenic free water is very crucial and a basic right of the people who had no alternative source of safe water without tubewell.
Salinity in Drinking Water (by Electrical Conductivity)
Salinity level of the high-dependency drinking water sources in different unions measured by electrical conductivity (EC) is shown in Table 2. Actually, electrical conductivity is a measure of capacity of water to conduct electrical current and is directly related to the total dissolved solids (TDS). The permissible limit of EC in drinking water is 250 and 500 μS/cm according to WHO and Bangladesh standard, respectively (Sultana et al. 2015). Results show that almost all sources had EC values above permissible limits in respect to Bangladesh (94%) and WHO (99%) standards.
Electrical conductivity (EC) is an important measure of salinity from dissolved solids in water. In the current study area, almost all the drinking water sources had significantly higher level of EC, while range of EC was quite higher in deep tubewells than shallow tubewells. A study in the coastal area of Bangladesh also reported that the salinity level in water from deep tubewell (depth 270–450 m) was much higher (six times or more than recommended level) comparing shallow tubewell (Khanom and Salehin 2012). The problem of drinking high level of salinity water has multiple causes on health. In 2002, the WHO recognized health impacts of consumption of highly saline waters as a priority for investigation under its public health initiatives (WHO 2008). According to the Intergovernmental Panel on Climate Change (IPCC), groundwater, crop soils and many rivers in the coastal area are likely to become increasingly saline from higher tidal waves and storm surges, as a result of climate change impacts (Parry et al. 2007). Therefore, protective measures should be taken how to protect the coastal people from adverse effect form salinity.
Iron Concentration
Analysis revealed that iron concentration varied between 0 and 18 ppm in the tested samples. Overall, 61 and 83% of tested sources exceeded the permissible limit of iron in drinking water according to Bangladesh (permissible limit: 1.0 ppm) and WHO standard (permissible limit: 0.3 ppm), respectively. Almost all the STWs (97%) found to have excess iron beyond Bangladesh standard, whereas half of the tested DTWs had iron concentration beyond Bangladesh permissible limit. Compared to other unions, tested water sources of Dhandia and Khesra union had excess iron concentration. Drinking water with high Fe concentration is assumed to be non-toxic and health impacts are not broadly documented (Merrill et al. 2011). Another study reported that absorption of a high amount of Fe could create health problems including development of kidney stone (Gupta et al. 2009).
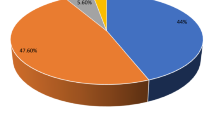
Preferred Option for Buying Drinking Water
In general, DTW water was considered the best source of drinking water by most households (88%) in Tala. In Sarulia union, about of 14% households said that they preferred rainwater for drinking. However, when respondents were asked about their preferred option for buying safe drinking water, most demanded a piped water supply system (40%) to buy drinking water. Buying water from a specific place (23%) or water being delivered to the home by the gallon (21%) were other favored options (Fig. 5). A pipe water supply system was most favored in Magura, Nagarghata, Khalilnagar, Khesra, and Tentulia unions, while households in Jalalpur union preferred water delivery by the gallon. Buying water from a specific place was the most desirable option in Khalishkhali union. One of the main objectives of this study was to determine the amount of money each household is willing to pay per week for buying drinking water. So understanding their preference was vital, since it was evident from earlier focus group discussions (FGDs) that most people of Tala would only pay money if their preferred option is installed.

Union-wise preferred option for buying drinking water
Willingness to Pay for Safe Drinking Water
Most of the households (90%) (Fig. 6a) showed interest to obtaining access to improved drinking water sources. This interest was highest in Dhandia (97%) union and lowest in Khalilnagar union (76%). Overall, only 10% of households had no interest in purchasing water for reasons such as already having access to pure and safe drinking water or low cost water supply facilities or facilities to properly store water. When people were asked about the causes behind their WTP, most (84%) reported that they wanted a new drinking water option to ensure access to clean and safe water.

a Households willing to get improved drinking water sources in their house in Tala Upazila. b Overall willingness to pay status in Tala Upazila
To measure perceptions about WTP for access to safe drinking water, the question was split into six categories: willing to pay 20 BDT, 50 BDT, 100 BDT, 200 BDT, 300 BDT, or 500 BDT per week for 20L safe water per day. 91% of respondents of Tala Upazila were willing to pay for a safe drinking water supply (Fig. 6b).
From the WTP status in different unions (Fig. 7), it is evident that, in all the unions, most households were willing to pay 20 BDT (1 USD = 80.0BDT) per week. Overall, 75% of households in Tala Upazila were willing to pay 20 BDT per week, while another 20% households were willing to pay 50 BDT per week. A significant percentage of households were willing to pay 50 BDT per week in Nagarghata and Sarulia unions only. Although only 4% households were willing to pay 100 BDT or more per week, in some unions a notable percentage of households were ready to spend such amounts for drinking water (i.e., Sarulia and Nagarghata).

Union-wise willingness to pay for safe drinking water status in Tala Upazila
The WTP status of households based on their economic condition in different unions (Fig. 8) shows that, regardless of their economic condition, most households were willing to pay 20.0 BDT per week.

Union-wise WTP for safe drinking water status in Tala Upazila according to economic condition
The monthly estimated mean willingness to pay (WTP) for safe drinking water was about 2% of the reported median monthly household income of 5000 BDT, which is below the Organization for Economic Co-operation and Development (OECD) suggested affordability threshold of 3% of household income (OECD 2003).
Factors Affecting the Willingness to Pay for Safe Drinking Water
Logistic regression model showing factors associated with willingness to pay for safe drinking water is presented in Table 3. Households having higher monthly income were more willing to spend money for better access to quality water. Households with monthly income of 4000–10,000 BDT and > 10000 BDT, respectively, were 2.6 and 2.8 times more willing to pay for safe drinking water than households with a monthly income of < 4000 BDT and these differences were statistically significant. Households who collect drinking water from sources more than 100 meters walking distance had higher willingness to pay for safe drinking water than households having drinking water source within 50 meters of their own courtyards. Similarly, households which were dissatisfied with existing water source had 1.5 times higher odds of willingness to pay for drinking water compared to households which were satisfied with the existing sources of drinking water. Meanwhile, households collecting drinking water from their own tubewells had 1.9 times more willing to pay than households relying on others/shared tubewells for collecting drinking water. Willingness to pay for safe drinking water among the arsenic free tubewell users was lower than the users of arsenic contaminated tubewells. However, this arsenic contamination status of tubewells was reported by the respondents. Households who faced problems in water collection during disasters were more willing to pay for safe drinking water compared to households with no problem in collecting water during disasters.
National Strategy for Water and Sanitation (2011) for Hard to Reach Areas of Bangladesh has given emphasis on providing subsidies to the poorest and disadvantaged groups of people living in vulnerable areas without definitive livelihood opportunities. Respondents reported that many initiatives from the local government, development partners and NGOs, such as supply of safe water from reverse osmosis (RO), pond sand filter (PSF) in the community have already been implemented to improve access of safe and affordable water in the coastal areas. However, improper management, non-availability of spare-parts (e.g., filter) in the local markets and cost burden to replace spare-parts have forced many of them to become non-functional, thus illustrating existing challenges to ensure sustainability of services for the community. It is expected that government’s current efforts to increase access of clean and affordable water to the community people would be effective if priority can be given to those areas such as coastal area where access of safe and clean water access is relatively less.
Conclusion
Water quality parameters such as arsenic, salinity (EC) and iron at high-dependent water sources confirmed that good quality drinking water is quite scarce in the study area. As one-third of high-dependent tubewells are contaminated by arsenic beyond permissible limit of Bangladesh standard, continuous exposure to drinking arsenic contaminated water may cause serious health problems in near future. It is also evident from the study that people are aware of these problems and are willing to pay to improve the situation. Most people were interested in paying some weekly amount of money to obtain safe drinking water. On average, the weekly estimated mean WTP for safe drinking water was 30.1 BDT, while the mean weekly WTP for non-poor, poor and ultra-poor households were 54.5 BDT, 33.6 BDT and 26.4 BDT (1 USD = 80.0 BDT), respectively. Economic status appears to have a significant effect on households’ WTP amount. Logistic regression model identified monthly household income, tubewell ownership, distance of drinking water source from household, satisfaction about existing water source as some determinants of willingness to pay of households for safe drinking water.
The WTP estimates obtained in this study indicate that a demand-driven program that aims to expand rural drinking water systems in the study area can be introduced. If a well-studied and structured business model could be developed to sell drinking water, it is likely to be successful. However, a pilot program is recommended before introducing any large-scale project. Local preferences for buying drinking water and WTP vary from place to place, so emphasis should be given on area-specific solutions. Since, majority of the households are willing to pay for buying drinking water, entrepreneurship development for water selling business can be encouraged to create employment opportunity for local peoples as well as to provide safe drinking water for the local community at minimum cost. Periodic monitoring of vendor’s services, such as cleanliness of water bottles used for supply of drinking water from door to door, quality of water by the water quality expert would be essential to increase access of safe drinking water at households. Engaging community-based WatSan (Water and Sanitation) committee including local government representatives to design an affordable water tariff structure and generate sufficient revenue to cover the cost of water services including salary of caretaker would be an effective and sustainable solution to improve access of safe and affordable drinking water in the coastal area of Bangladesh.
References
Ahmed F, Ahmad N, Khan MA, Jolliffe D, Mahbub MA, Sharif I, Yoshida N, Zaidi S, Swaroop V, Zutt J (2010) Poverty maps of Bangladesh 2010: key findings. World Bank Group, Washington, DC. http://documents.worldbank.org/curated/en/2010/01/20191359/poverty-maps-bangladesh-2010-key-findings
Asim S, Lohano HD, Ahmad I (2015) Households’ willingness to pay for improved tap water services in Karachi, Pakistan/comments. Pak Dev Rev 54(4):507
Bangladesh Bureau of Statistics (BBS) (2013) District statistics 2011. Statistics Division, Ministry of Planning, Government of the Peoples’ Republic of Bangladesh
BBS and UNICEF (2009) Bangladesh multiple indicator cluster survey 2009; Progotir Pathey: final report. BBS and UNICEF Dhaka, Bangladesh
Dey NC, Rabbi S (2013) Use of tubewell water for different purposes at household level: safety practices in rural Bangladesh, In: Achievement of BRAC-WASH program towards Millennium Development Goal and beyond 2013. BRAC, Dhaka, pp 9–30. (Research Monograph 60)
Dey NC, Akter T, Hossain M (2015) Environment: Water, sanitation and hygiene. In: Hossain M, Bayes A (eds) Leading issues in rural development—Bangladesh perspective. AH Development Publishing House, Dhaka, pp 147–163
Dey NC, Parvez M, Dey D, Saha R, Ghose L, Barua M, Islam A, Chowdhury M (2016) Microbial contamination of drinking water from risky tubewells situated in different hydrological regions of Bangladesh. Int J Hyg Environ Health 220(3):621–636. https://doi.org/10.1016/j.ijheh.2016.12.007
Dey NC, Saha R, Parvez M, Bala SK, Islam AKM, Hossain M (2017) Sustainability of groundwater use for irrigation for dry-season crops in the northwest Bangladesh. Groundw Sustain Dev 4:66–77. https://doi.org/10.1016/j.gsd.2017.02.001
Flanagan SV, Johnston RB, Zheng Y (2012) Arsenic in tubewell water in Bangladesh: health and economic impacts and implications for arsenic mitigation. Bull World Health Organ 90(11):839–846
George CM, Zheng Y, Graziano JH, Rasul SB, Hossain Z, Mey JL, van Geen A (2012) Evaluation of an arsenic test kit for rapid well screening in Bangladesh. Environ Sci Technol 46:11213–11219
GoB (National Institute of Population Research and Training), Mitra and Associates, and ICF International (2016) Bangladesh demographic and health survey 2014. NIPORT, Mitra and Associates, and ICF International, Dhaka, Bangladesh, and Rockville, Maryland, USA
Gupta P, Vishwakarma M, Rawtani PM (2009) Assessment of water quality parameters of Kerwa Dam for drinking suitability. Int J Theor Appl Sci 1(2):53–55. http://researchtrend.net/tas12/14%20MONIKA%202.pdf
Hunter PR, MacDonald AM, Carter RC (2010) Water supply and health. PLos Med 7:1–9. www.plosmedicine.org (accessed on 8 November 2015)
Khanom S, Salehin M (2012) Salinity constraints to different water uses in coastal area of Bangladesh: a case study. Bangladesh J Sci Res 25(1):33–42. http://banglajol.ubiquity.press/index.php/BJSR/article/download/13048/9379
Kurokawa M, Ogata K, Idemori M, Tsumori S, Miyaguni H, Inoue S, Hotta N (2001) Investigation of skin manifestations of arsenicism due to intake of arsenic-contaminated groundwater in residents of Samta, Jessore, Bangladesh. Arch Dermatol 137:102–103
Merrill RD, Shamim AA, Ali H, Jahan N, Labrique AB, Schulze K, West KP (2011) Iron status of women is associated with the iron concentration of potable groundwater in rural Bangladesh. J Nutr 141(5):944–949
Misbahuddin M (2015) Arsenicosis: a global issue. Science Publishing Group, New York
OECD (2003) Social issues in the provision and pricing of water services. Organization for Economic Co-operation and Development (OECD) Publishing, Paris
Parry ML, Canziani OF, Palutikof JP, van der Linden PJ, Hanson CE (2007) Climate change 2007: impacts, adaptation and vulnerability. Contribution of Working Group II to the Fourth Assessment Report of the Intergovernmental Panel on Climate Change (eds). Cambridge University Press, Cambridge
Rahman M, Islam MA, Bodrud-Doza M, Muhib MI, Zahid A, Shammi M, Tareq SM, Kurasaki M (2017) Spatio-temporal assessment of groundwater quality and human health risk: a case study in Gopalganj, Bangladesh. Exposure Health. https://doi.org/10.1007/s12403-017-0253-y
Rasheed S, Siddique AK, Sharmin T, Hasan AMR, Hanifi SMA, Iqbal M, Bhuiya A (2016) Salt intake and health risk in climate change vulnerable coastal Bangladesh: what role do beliefs and practices play? PLoS ONE 11(4):e0152783
Rashid MH, Fardous Z, Chowdhury MAZ, Alam MK, Bari ML, Moniruzzaman M, Gan SH (2016) Determination of heavy metals in the soils of tea plantations and in fresh and processed tea leaves: an evaluation of six digestion methods. Chem Cent J 10(1):7
Rebecca D, Merrill RD, Shamim AA, Labrique AB, Ali H, Schulze K, Rashid M, Christian P, West KP (2009) Validation of two portable instruments to measure iron concentration in groundwater in rural Bangladesh. J Health Popul Nutr 27(3):414–418
Sultana M, Saifullah ASM, Latif MB, Mamun SA, Sultana DS (2015) Drinking water quality at academic institutions of Tangail municipality. J Environ Sci Nat Res 6(1):247–252
Tussupova K, Berndtsson R, Bramryd T, Beisenova R (2015) Investigating willingness to pay to improve water supply services: application of contingent valuation method. Water 7(6):3024–3039
WHO (2008) Guidelines for drinking-water quality. Third edition incorporating the first and second addenda. Vol. 1. Recommendations. World Health Organization, Geneva
WHO and UNICEF (2015) Progress on drinking water and sanitation: 2015 update and MDG assessment. WHO/UNICEF Joint Monitoring Program, Switzerland. http://apps.who.int/iris/bitstream/10665/177752/1/9789241509145_eng.pdf
World Bank (2016) Bangladesh development update, October 2016: sustained development progress. World Bank, Washington, DC. © World Bank. https://openknowledge.worldbank.org/handle/10986/25274 License: CC BY 3.0 IGO
Wu J, Wang L, Wang S, Tian R, Xue C, Feng W, Li Y (2017) Spatiotemporal variation of groundwater quality in an arid area experiencing long-term paper wastewater irrigation, northwest China. Environ Earth Sci 76(13):460. https://doi.org/10.1007/s12665-017-6787-2
Acknowledgements
The paper is based on research funded in part by DFID through Strategic Partnership Assistance (SPA) through the BRAC WASH program. We are grateful to participants who provided valuable information for this study. Thanks to WASH program personnel for their contribution during field work. Thanks to the Data Management Unit of RED for providing necessary support for cleaning the data in time. Thanks also to the Center for Water, Environment and Health Research and Development, Social Innovation and Development Foundation for their support during the study.
Funding
The study was funded from DFID through Strategic Partnership Assistance (SPA) through the BRAC WASH program.
Author information
Authors and Affiliations
Contributions
NCD: conceived and conducted the study; analyzed and interpreted the data and wrote the paper. MP: analyzed and interpreted the data, and assisted in report writing. RS: conducted household level survey, assisted in data analysis and GIS mapping. MRI: data analysis and interpretation of data. TA: questionnaire development, training to enumerators, and data collection. MR: coordinated in data collection and reviewed manuscript. MKB: field management during household level survey. AI: field management during household level survey.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Dey, N.C., Parvez, M., Saha, R. et al. Water Quality and Willingness to Pay for Safe Drinking Water in Tala Upazila in a Coastal District of Bangladesh. Expo Health 11, 297–310 (2019). https://doi.org/10.1007/s12403-018-0272-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12403-018-0272-3