
Abstract
Background
Rb-82 positron emission tomography (PET) myocardial perfusion imaging (MPI) is a robust tool for the evaluation of coronary artery disease (CAD). However, gastric uptake and spillover can be seen in 10% of Rb-82 PET MPI studies, commonly affecting the inferior wall, and can preclude the accurate identification of myocardial ischemia. We sought to understand the relationship between Rb-82 gastric uptake and the use of proton pump inhibitors (PPI).
Methods
600 consecutive patients who presented for a clinically indicated Rb-82 PET MPI study were prospectively enrolled. In addition to the clinical history, PPI use was ascertained (medication, dose, frequency and duration of use, and time of last dose). Patients were categorized as PPI and non-PPI users. Rb-82 uptake in the gastrium, myocardium, and liver were measured at rest. Absolute uptake values and gastric:hepatic ratios were compared in PPI and non-PPI users.
Result
Of 600 enrolled patients, 181 (30.2%) patients were using PPI. The gastric Rb-82 uptake in PPI users was 23% higher than non-PPI users (146 ± 52 kBq/cc vs 119 ± 40 kBq/cc, respectively; P < 0.001). The resting gastric:hepatic Rb-82 uptake ratio was also 23% higher in PPI vs non-PPI users (2.7 ± 1.0 vs 2.2 ± 0.8, respectively; P < 0.001).
Conclusion
The gastric uptake of Rb-82 appears to be greater in patients actively using PPI and may identify a group who might be at greater risk of non-diagnostic Rb-82 PET MPI.
Spanish Abstract
Antecedentes
la imagen de perfusión cardiaca con tomografía por emisión de positrones (PET) usando Rb-82, es una herramienta sólida en la evaluación de la enfermedad arterial coronaria (CAD). Sin embargo, el exceso de captación en la cámara gástrica puede verse hasta en el 10% de los estudios con PET-MPI y Rb-82, y comúnmente afecta la pared inferior del miocardio, y puede impedir la identificación precisa de la isquemia a este nivel. En el presente trabajo intentamos comprender la relación entre la absorción gástrica de Rb-82 y el uso de inhibidores de la bomba de protones (PPI).
Métodos
se captaron prospectivamente 600 pacientes consecutivos que se presentaron para estudio PET-MPI y Rb-82 clínicamente indicado. Además de los antecedentes clínicos, se determinó el uso de PPI (fármaco, dosis, frecuencia y duración del uso, así como el tiempo desde la última dosis), de tal forma que los pacientes fueron categorizados como usuarios de PPI y sin uso de PPI. Se midió la absorción de Rb-82 en estómago, miocardio e hígado en reposo. Los valores absolutos de absorción y la relación gástro:hepática se compararon en usuarios de PPI y sin PPI.
Resultado
de los 600 pacientes incluidos, 181 (30.2%) pacientes estaban usando PPI. La captación gástrica de Rb-82 en los usuarios de PPI fue un 23% más alta que en los que no usaron PPI (146 ± 52 kBq/cc frente a 119 ± 40 kBq/cc, respectivamente; P < 0.001). La relación de captación gastro:hepática de Rb-82 en reposo también fue un 23% mayor en usuarios de PPI frente a usuarios sin PPI (2.7 ± 1.0 frente a 2.2 ± 0.8, respectivamente; P < 0.001).
Conclusión
La captación gástrica de Rb-82 parece ser mayor en pacientes que usan activamente PPI y esto puede identificar un grupo en mayor riesgo de tener un diagnóstico incorrecto con el uso de PET-MPI y Rb-82.
Chinese Abstract
背景
Rb-82正电子发射断层扫描(PET)心肌灌注成像(MPI)是评估冠状动脉疾病(CAD)的有力工具。 然而,在10%的Rb-82 PET MPI样本中可以看到胃的摄取和溢出,通常会影响(心脏)下壁,并且会影响心肌缺血鉴定的准确性。 本文试图了解Rb-82胃的摄取与使用质子泵抑制剂(PPI)之间的关系。
方法
对600名有临床适应症行Rb-82 PET MPI的连续患者进行了前瞻性研究。 除临床病史外,还确定了PPI的使用(药物,剂量,使用频率和持续时间以及最后一次使用时间)。 患者被分类为PPI和非PPI组。 在休息时测量胃肠,心肌和肝脏中的Rb-82摄取。 在PPI和非PPI使用者中比较绝对摄取值以及胃:肝的摄取比率。
结果
在600名入组患者中,181名(30.2%)患者使用PPI。 PPI使用者的胃Rb-82摄取比非PPI使用者高23%(分别为146±52kBq / cc和119±40kBq / cc; P < 0.001)。 与非PPI使用者相比,PPI患者的静息图像下,胃:肝Rb-82摄取率也高出23%(分别为2.7±1.0和2.2±0.8; P < 0.001)。
结论
在积极使用PPI的患者中,Rb-82的胃摄取更加明显,该标准可成为低诊断价值Rb-82 PET MPI的重要风险因素之一。
French Abstract
Contexte
l’imagerie de perfusion myocardique par tomographie par émission de positrons (TEP) Rb-82 est un outil robuste pour l’évaluation de la maladie coronarienne. Cependant l’absorption et sécrétion gastrique du tracer sont visibles dans 10% des études TEP au Rb-82 interférant avec la distribution du traceur au niveau de la paroi inferieure et peut empêcher l’identification précise de l’ischémie myocardique. Nous avons cherché à comprendre la relation entre l’absorption gastrique de Rb-82 et l’utilisation de la pompe à proton inhibiteurs (IPP).
Méthodes
nous avons enrôlé de manière consécutive dans cette étude prospective 600 patients qui nous ont été confie pour une étude de perfusion myocardique au Rb-82. En plus des antécédents cliniques, l’utilisation d’IPP a été établie (médicament, dose, fréquence et durée d’utilisation, heure de la dernière dose). Les patients étaient classés comme utilisateurs ou non de IPP. Absorption de Rb-82 au niveau de l’estomac, le myocarde et le foie ont été mesurés au repos. Les valeurs d’absorption absolue et les rapports gastro/hépatique ont été comparés chez les deux groupes (IPP et non IPP).
Résultat
Sur les 600 patients inscrits, 181 (30,2%) utilisaient un IPP. Le Rb-82 gastrique Le taux d’absorption gastrique chez les utilisateurs d’IPP s’est avéré de 23% plus élevé que chez les utilisateurs non-IPP (146 ± 52 kBq/cc contre 119 ± 40 kBq/cc, respectivement; P < 0,001). Le rapport d’absorption gastrique/hépatique au repos s’est également avérée de 23% plus élevé chez IPP vs utilisateurs non-IPP (2,7 ± 1,0 vs 2,2 ± 0,8, respectivement; P < 0,001).
Conclusion
l’absorption gastrique de Rb-82 paraît être plus importante chez les patients utilisant activement l’IPP; l’identification des patients prenant des IPPs permettrait d’anticiper un examen de perfusion myocardique non diagnostique.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Rb-82 positron emission tomography (PET) myocardial perfusion imaging (MPI) is a robust tool for the evaluation for coronary artery disease (CAD), and has very good sensitivity and specificity.1,2 However, gastric uptake and spillover in Rb-82 PET studies can be extensive and may affect the image quality and diagnostic accuracy. Gastric spillover can be seen in 10% of studies, which most commonly affects the inferior wall and precludes the accurate identification of myocardial ischemia.3,4
Rb-82 gastric uptake is variable and anecdotally has been more frequently observed. Concomitantly, the use of proton pump inhibitors (PPI) has also been on the rise.5,6,7,8 We sought to understand the relationship between Rb-82 gastric uptake and PPI use.
Methods
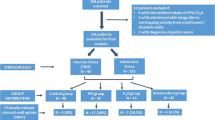
600 consecutive patients who presented for a clinically indicated Rb-82 PET MPI study were prospectively enrolled. No patients were excluded from analysis. In addition to the clinical history, PPI use was ascertained (medication, dose, frequency and duration of use, and time of last dose). Patients were categorized as active PPI users and non-PPI users. Active PPI users were further categorized based on the time interval between last PPI use and the PET MPI scan.
Each patient underwent dipyridamole Rb-82 PET MPI as per our local protocol and image acquisition was performed adhering to ASNC guidelines.9 After a rest CT for attenuation correction, rest and stress images were acquired using either the GE Discovery PET/CT 690 or GE Discovery PET/CT 600 (GE Healthcare, Waukesha, WI) using 3D acquisition mode.10,11,12,13
Myocardial perfusion images were reviewed and qualitatively scored using the 17 segment model and 5 point scoring system (normal (0), mildly abnormal (1), moderately abnormal (2), severe abnormal (3), and absence (4) of radiotracer uptake).
The fused CT/perfusion images were used to identify cardiac and extracardiac structures. The maximal resting Rb-82 uptake (Bq/cc) was measured in the myocardium, stomach wall, and liver (Figure 1). Using axial images, measurements were performed by placing a large ROI over the organ of interest, ensuring the area with greatest Rb-82 uptake was within the ROI. Maximal SUV values within each ROI were recorded. Absolute uptake ratios (gastric(max):myocardium(max) and gastric(max):hepatic(max)) were calculated and compared between the 2 groups.

Regions of interest used to measure activity (Bq/cc) in the myocardium (A), gastric wall (B), and liver (C) using fused CT/PET images
Statistical Analysis
Continuous variables are presented as means and standard deviation, while categorical variables are presented as frequencies. Statistical analyses were performed using SPSS version 24 (IBM, Armonk, NY, USA). The comparison between groups was performed with the student t-test and chi-square test. A P value of < 0.05 was considered statistically significant.
Results
Of 600 enrolled patients, 181 (30.2%) patients were actively using PPI (Table 1). The most commonly used PPI was pantoprazole and PPI users were more likely to have hypertension, dyslipidemia, and history of percutaneous coronary intervention.
The gastric Rb-82 uptake in PPI users was 23% higher than non-PPI users (146 ± 52 kBq/cc and 119 ± 40 kBq/cc, respectively (P < 0.001)) (Table 2, Figure 2). Of 419 non-PPI users, patients were further stratified as those using H2 blocking agents (12 patients). Since there was no difference in gastric uptake between those using H2 blocking agent and all other non-PPI users, they were combined (Table 2).

Box-Whisker plots of absolute gastric, myocardial, and hepatic uptake (A) and gastric/myocardial and gastric/hepatic ratios (B) in patients using PPI (red) and not using PPI (blue)
There was similar hepatic Rb-82 uptake in PPI and non-PPI users (56 ± 11 kBq/cc and 56 ± 12 kBq/cc, respectively (P = 0.78)) (Table 2). The gastric:hepatic Rb-82 uptake ratio was 23% higher in PPI users (2.7 ± 1.0) than non-PPI users (2.2 ± 0.8; P < 0.001).
Myocardial Rb-82 uptake was 5% higher in the PPI users than the non-PPI users (122 ± 20 kBq/cc and 116 ± 21 kBq/cc, respectively (P = 0.002)). The gastric:myocardial Rb-82 uptake ratio was 16% higher in PPI users compared to non-PPI users (1.22 ± 0.43 and 1.05 ± 0.37, respectively (P < 0.001)).
Time Interval Between PPI Use and PET Imaging
PPI users were further categorized based on the time interval between PPI ingestion and the Rb-82 PET scan (< 36 and ≥ 36 hours) with each group comprising of 170 and 11 patients, respectively. The gastric:hepatic ratio was higher in the < 36 hour group than the ≥ 36 hour group (2.71 ± 0.96 and 1.98 ± 1.12, respectively (P = 0.016)). The gastric:myocardial ratio was also higher in the early group (1.2 ± 0.4 and 0.9 ± 0.4, (P = 0.006)).
Of patients for whom PPI dose was available, we also categorized PPI users as low, standard, and double PPI dose usage.14 The number of patients using low dose, standard dose, and double dose were 4, 140, and 37 patients, respectively. The gastric:hepatic ratio for standard and high PPI doses were similar (2.72 ± 1.03 and 2.60 ± 0.69, respectively (P = 0.508)) as were the mean gastric:myocardial ratios (1.23 ± 0.43 and 1.22 ± 0.36, respectively (P = 0.960)).
We categorized patients into those with and without hiatus hernia. Both gastric uptake and gastric:hepatic ratios did not differ in patients with and without hiatus hernia. The differences in gastric uptake and gastric:hepatic ratios between PPI and non-PPI patients were still significantly different in those without hiatus hernia. There was a trend observed in those with hiatus hernia, but was underpowered to demonstrate a statistically significant difference (Table 3).
Discussion
Rubidium, like thallium, is a potassium analogue and thus the myocardial uptake is dependent on Na+/K+ ATPase active transporters.15 Gastric uptake of Rb has been well studied and relates to the presence of H+/K+ ATPase transporter located in the apical membrane of the gastric parietal cells.16,17. The impact of PPI on H+/K+ ATPase transporter activity, upregulation, and density is less well understood. This hypothesis generating study attempts to understand the impact of PPI on Rb-82 gastric uptake and its time-related effects. The results of our study confirm that PPI use is associated with greater Rb-82 gastric uptake and may identify a population that may be more susceptible to gastric spillover artifact (Figure 3).

Rb-82 PET MPI and gastric uptake in a patient treated with PPI (A) and a patient without PPI (b)
Subdiaphragmatic spillover artifact remains a limitation in MPI studies and can conceal perfusion defects or cause photopenic defects (negative ramp or ringing artifact). Minimizing sources of spillover would potentially improve diagnostic accuracy. Goel et al. studied 138 Tc-99m sestamibi SPECT patients and found that prolonged use of PPI was associated with increased gastric wall activity.18 Our study confirms that a similar issue exists with Rb-82 PET.
Identifying methods for minimizing gastric uptake would be clinically useful. Patient preparation such as timing for withholding medications prior to Rb-82 PET MPI could optimize image quality. In our subgroup analysis, gastric uptake was lower in patients who had stopped their PPIs for ≥ 36 hours and perhaps instructions for PPI abstinence should be considered. Withholding PPI > 36 hours prior to Rb-82 PET MPI may reduce the potential spillover from gastric uptake. Given the small sample size, we could not evaluate the relationship between PPI doses. Further studies are needed to better understand the relationship between timing and dose of PPI use and gastric Rb-82 uptake for further optimization of patient preparation.
The mechanism by which PPI patients have increased Rb-82 gastric uptake has not been well elucidated. The inhibition of H+/K+-ATPase active transporter reduces hydrogen secretion by parietal cells. Theoretically, this inhibition would reduce the uptake of K+ and thus the Rb-82 uptake by parietal cells; however, PPIs may have other effects on the gastric mucosa that impact on potassium utilization. A meta-analysis of 16 studies (1920 patients) found that long-term use of PPI causes hyperplasia of enterochromaffin-like cells and moderate hypergastrinemia.19 A randomized, placebo-controlled, double-blinded, multicenter study showed that long-term PPI therapy increased parietal cell protrusion, swelling and bulging, and the gradual development of fundic gland cysts.20 The impact on these findings on gastric potassium utilization is unknown and further understanding is needed.
New Knowledge Gained: Proton pump inhibitor use is associated with an increased gastric uptake of Rb-82. Spillover from gastric uptake could impact on the interpretation of adjacent myocardium on Rb-82 PET MPI studies. Withholding PPI > 36 hours prior to Rb-82 PET MPI may reduce the potential spillover from gastric uptake.
Study Limitations
Our prospective study examines the impact of PPI on gastric uptake and suggests a relationship between PPI use and increased gastric uptake. Although we found slightly lower Rb-82 uptake in patients who had held PPI ≥ 36 hours, our relatively small sample size precluded in-depth analysis of timing and varying doses. Further prospective studies are needed to study the effect of PPI cessation. Similarly, the potential benefit of acute PPI administration at the time of Rb-82 PET could also be explored.
Indications for the use of PPI and the presence of concomitant conditions such as gastroesophageal reflux disease were not available. Although such conditions may be confounders, gastric measures were performed below the diaphragm and therefore should limit confounding effect of structural abnormalities.
The clinical ramifications of PPI-induced gastric uptake are unknown. Since patients did not undergo routine angiography, FFR, or invasive CFR measurements, the true false positive and false negative rates are unknown. The clinical impact of increased gastric uptake on Rb-82 PET MPI is uncertain and warrants further investigation. The impact of gastric uptake on measurements of myocardial blood flow was not specifically collected or analyzed. Future studies examining its clinical impact would be important to understand if extracardiac uptake potentially affects the accuracy of quantitative myocardial blood flow.
Conclusions
The gastric uptake of Rb-82 appears to be greater in patients actively using PPI and may identify a group who might be at greater risk of a non-diagnostic Rb-82 PET MPI study.
Abbreviations
- Rb-82:
-
Rubidium-82
- PET:
-
Positron emission tomography
- Bq:
-
Becquerel
- PPI:
-
Proton pump inhibitors
- H2B:
-
H2 blocker
- MPI:
-
Myocardial perfusion imaging
- LV:
-
Left ventricle
- BMI:
-
Body mass index
References
Mc Ardle BA, Dowsley TF, deKemp RA, Wells GA, Beanlands RS. Does rubidium-82 PET have superior accuracy to SPECT perfusion imaging for the diagnosis of obstructive coronary disease?: A systematic review and meta-analysis. J Am Coll Cardiol. 2012;60:1828–37.
Bateman TM, Heller GV, McGhie AI, Friedman JD, Case JA, Bryngelson JR, et al. Diagnostic accuracy of rest/stress ECG-gated Rb-82 myocardial perfusion PET: Comparison with ECG-gated Tc-99m sestamibi SPECT. J Nucl Cardiol. 2006;13:24–33.
Thompson RC. The problem of radiotracer abdominal activity in myocardial perfusion imaging studies. J Nucl Cardiol. 2008;15:159–61.
Orton EJ, Al Harbi I, Klein R, Beanlands RS, deKemp RA, Glenn Wells R. Detection and severity classification of extracardiac interference in 82Rb PET myocardial perfusion imaging. Med Phys. 2014;41:102501.
Pottegard A, Broe A, Hallas J, de Muckadell OB, Lassen AT, Lodrup AB. Use of proton-pump inhibitors among adults: A Danish nationwide drug utilization study. Therap Adv Gastroenterol. 2016;9:671–8.
Haastrup P, Paulsen MS, Zwisler JE, Begtrup LM, Hansen JM, Rasmussen S, et al. Rapidly increasing prescribing of proton pump inhibitors in primary care despite interventions: A nationwide observational study. Eur J Gen Pract. 2014;20:290–3.
Halfdanarson OO, Pottegard A, Bjornsson ES, Lund SH, Ogmundsdottir MH, Steingrimsson E, et al. Proton-pump inhibitors among adults: A nationwide drug-utilization study. Ter Adv Gastroenterol. 2018;11:1–11.
Tett SE, Sketris I, Cooke C, van Zanten SV, Barozzi N. Differences in utilisation of gastroprotective drugs between 2001 and 2005 in Australia and Nova Scotia. Canada. Pharmacoepidemiol Drug Saf. 2013;22:735–43.
Dilsizian V, Bacharach SL, Beanlands RS, Bergmann SR, Delbeke D, Dorbala S, et al. ASNC imaging guidelines/SNMMI procedure standard for positron emission tomography (PET) nuclear cardiology procedures. J Nucl Cardiol. 2016;23:1187–226.
Renaud JM, Yip K, Guimond J, Trottier M, Pibarot P, Turcotte E, et al. Characterization of 3-dimensional pet systems for accurate quantification of myocardial blood flow. J Nucl Med. 2017;58:103–9.
Mc Ardle BA, Davies RA, Chen L, Small GR, Ruddy TD, Dwivedi G, et al. Prognostic value of rubidium-82 positron emission tomography in patients after heart transplant. Circ Cardiovasc Imaging. 2014;7:930–7.
Renaud JM, Mylonas I, McArdle B, Dowsley T, Yip K, Turcotte E, et al. Clinical interpretation standards and quality assurance for the multicenter PET/CT trial rubidium-ARMI. J Nucl Med. 2014;55:58–64.
Ziadi MC, Dekemp RA, Williams KA, Guo A, Chow BJ, Renaud JM, et al. Impaired myocardial flow reserve on rubidium-82 positron emission tomography imaging predicts adverse outcomes in patients assessed for myocardial ischemia. J Am Coll Cardiol. 2011;58:740–8.
Internal Clinical Guidelines Team. Dyspepsia and gastrooesophageal reflux disease: investigation and management of dyspepsia, symptoms suggestive of gastro-oesophageal reflux disease, or both 2014 [Available from: https://www.nice.org.uk/guidance/cg184/evidence/full-guideline-193203757.
Di Carli MF, Dorbala S, Meserve J, El Fakhri G, Sitek A, Moore SC. Clinical myocardial perfusion PET/CT. J Nucl Med. 2007;48:783–93.
Kimura T, Yoshida A, Tabuchi Y, Ikari A, Takeguchi N, Asano S. Stable expression of gastric proton pump activity at the cell surface. J Biochem. 2002;131:923–32.
Durr KL, Abe K, Tavraz NN, Friedrich T. E2P state stabilization by the N-terminal tail of the H, K-ATPase beta-subunit is critical for efficient proton pumping under in vivo conditions. J Biol Chem. 2009;284:20147–54.
Goel S, Bommireddipalli S, DePuey EG. Effect of proton pump inhibitors and H2 antagonists on the stomach wall in 99mTc-sestamibi cardiac imaging. J Nucl Med Technol. 2009;37:240–3.
Lundell L, Vieth M, Gibson F, Nagy P, Kahrilas PJ. Systematic review: the effects of long-term proton pump inhibitor use on serum gastrin levels and gastric histology. Aliment Pharmacol Ther. 2015;42:649–63.
Cats A, Schenk BE, Bloemena E, Roosedaal R, Lindeman J, Biemond I, et al. Parietal cell protrusions and fundic gland cysts during omeprazole maintenance treatment. Hum Pathol. 2000;31:684–90.
Acknowledgments
Benjamin Chow holds the Saul and Edna Goldfarb Chair in Cardiac Imaging Research. He receives research support from CV Diagnostix and AusculSciences and educational support from TeraRecon Inc. He has equity interest in GE.
Disclosures
Dr. Ruddy reports grants from GE Healthcare. RB is supported by the Heart and Stroke Foundation of Ontario (HSFO) University of Ottawa Tier 1, and the Ottawa Heart Institute Vered Chair in Cardiology. RB is a consultant and receives research funding from Lantheus Medical Imaging, Jubilant DraxImage, and GE.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The authors of this article have provided a PowerPoint file, available for download at SpringerLink, which summarizes the contents of the paper and is free for reuse at meetings and presentations. Search for the article DOI on SpringerLink.com.
The authors have also provided an audio summary of the article, which is available to download as ESM, or to listen to via the JNC/ASNC Podcast.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Alzahrani, A.H., Arasaratnam, P., Massalha, S. et al. Effect of proton pump inhibitors on Rubidium-82 gastric uptake using positron emission tomography myocardial perfusion imaging. J. Nucl. Cardiol. 27, 1443–1451 (2020). https://doi.org/10.1007/s12350-019-01954-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-019-01954-y