
Abstract
Background
Global functional parameters are available from electrocardiographic gated Rubidium-82 positron emission tomography/computed tomography (82Rb-PET/CT). However, the reproducibility of these data is not clarified. We aimed to investigate reproducibility of left ventricular ejection fraction (LVEF), endsystolic volume (ESV), enddiastolic volume (EDV), and left ventricular (LV) mass between two scans and between two commercially available software packages.
Methods and Results
Forty healthy young volunteers underwent two 82Rb-PET/CT rest and adenosine stress scans obtaining global functional parameters. Corridor4DM (4DM) and Quantitative Gated SPECT (QGS) were used for analyses. Mean (± SD) age was 24 ± 4 years and 50% were men. High reproducibility of all parameters was found between scans and this was true for both software packages. LVEF at rest with 4DM: mean difference (95% CI) − 1.1 (− 3.0 to 0.8), P = .25, limits of agreement: − 12.8 to 10.6. Significant differences were found between software packages on all functional parameters (P < .0001).
Conclusion
High reproducibility was found between scans when measuring LVEF, ESV, EDV, and LV mass from 82Rb-PET/CT. However, concordance between parameter measures was poor when comparing the two software packages. Thus, global functional parameter measures are reliable, but the same software package should be used within a study and when comparing absolute values.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The role of myocardial perfusion imaging (MPI) in diagnosing patients with ischemic heart disease is well established.1 The clinical use of cardiac positron emission computed tomography (PET) especially 82Rb-PET/CT for semi-quantitative myocardial perfusion imaging has increased significantly over the past decades.2,3,4 Global functional parameters including left ventricular ejection fraction (LVEF), endsystolic volume (ESV), enddiastolic volume (EDV), and left ventricular (LV) mass are available from electrocardiographic gated 82Rb-PET/CT. However, the clinical validity of these data is less evident. A previous study has shown that LVEF, ESV, and EDV at rest and during stress can be measured reproducibly from gated 82Rb-PET/CT using different software packages compared with contrast-enhanced CT ventriculography, with some underestimation of LVEF and EDV by 82Rb-PET/CT.5 LVEF and LV volumes measured by PET using other tracers have also been shown to correlate well with both cardiac magnetic resonance imaging (cMRI) and single-photon emission computerized tomography (SPECT).6,7,8 Other studies have shown that LVEF reserve (change in LVEF from rest to stress) measured with 82Rb-PET/CT predicted adverse events and all-cause mortality9,10 and that a high LVEF reserve could be used to exclude left main/3-vessel coronary artery disease.11 Furthermore, LV mass has been shown to be constant with changes in LVEF and LV volumes from rest to stress.12
Different commercially available software packages for analyses of 82Rb-PET/CT scans have previously been compared with regard to LVEF and LV volumes.13 However, no former studies have addressed the reproducibility of global functional parameters between two different scans assessed by rest and adenosine stress 82Rb-PET/CT. Therefore, we investigated reproducibility of left ventricular ejection fraction (LVEF), endsystolic volume (ESV), enddiastolic volume (EDV), and left ventricular (LV) mass between two scans and between two commercially available software packages.
Methods
Study Population
In a time span from September 2016 to March 2017, we scanned 40 healthy volunteers using rest and adenosine stress myocardial perfusion 82Rb-PET/CT. All participants, with one exception, underwent two PET scans. Volunteers aged 20 to 40 years were recruited primarily from the surrounding universities using advertisements approved by the Scientific Ethics Committee [protocol number H-15009293]. The following inclusion criteria were used for recruitment: age >18 years, no known medical condition, no regular consumption of medicine, no use of tobacco or euphoric substances (except alcohol) within the last three months, and no current participation in drug testing studies. The following exclusion criteria were used: any prior medical history of asthma, allergy or intolerance to theophylline or adenosine, pregnancy, or inability to adhere to the protocol. Informed oral and written consents were obtained from all volunteers, and the Scientific Ethics Committee of the Capital Region of Denmark and the Danish Data Protection Agency approved the protocol [protocol number H-15009293]. One of the two scans investigated in this study was used as control scans in another study so that only one extra scan was made of each participant in order to conduct these reproducibility data. We performed the trial in accordance with the principles of the Declaration of Helsinki.
PET Imaging
Participants underwent two PET scans separated by at least 24 hours. Each scan consisted of a single session, where the volunteer underwent PET myocardial perfusion at rest and during adenosine stress. We instructed the participants not to consume substances and medications containing caffeine and theophylline for 24 hours before each scan. Volunteers received (mean±SD) 1058 ± 142 MBq and 1055 ± 145 MBq 82Rb for rest and stress imaging, supplied from a CardioGen-82Sr/82Rb generator manufactured for Bracco Diagnostics Inc., Princeton, NJ. We utilized a Siemens Biograph mCT/PET 128-slice scanner (Siemens Healthcare, Knoxville, TN, USA). Both rest and stress images were acquired ECG-gated in list mode for 7 minutes from the 82Rb infusion start point. For the stress sequence, we used adenosine infusion (0.14 mg/kg/min) for 6 minutes, and the stress 82Rb infusion was started 2.5 minutes after initiating the adenosine administration. Moreover, we performed a low-dose CT for attenuation correction before the rest study, and in case of participant motion we repeated it after the stress study. As per clinical routine, we acquired coronary artery calcium score (CACS) images from a non-contrast breath-hold CT in all volunteers at their first scan.14
Quantitative and Semi-quantitative Analyses
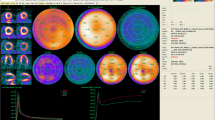
To quantify global functional parameters, we used static ECG-gated perfusion image reconstruction performed between 2.5 and 7 minutes after start of Rb-tracer infusion for both stress and rest images using 3D Ordered Subset Expectation Maximization (OSEM) reconstruction (2 iterations, 21 subsets) with point spread function modeling and time of flight.15 A 128 × 128 matrix, 2 × zoom (voxel dimensions 3.18 × 3.18 × 2.03 mm), 6.5 mm Gaussian post filter, attenuation and scatter correction (including prompt gamma correction) and 8 bins for gating. Quantification of functional parameters was conducted with Corridor4DM v 2015.0.0.44 (INVIA, LLC, Ann Abor, USA) and Quantitative Gated SPECT (QGS) v 2015.5 (Cedars-Sinai Cardiac Suite, Los Angeles, USA) (Figure 1). All data quantification with 4DM was automatically processed with an accurate LV contour. Furthermore, manual valve plane adjustments were performed on all 4DM data for comparison with the automatic quantification. If nothing else is indicated, 4DM data are the automatically processed without manual correction. Using QGS in 217 cases of 480, the automatic data processing algorithm was unable to generate an accurate LV contour. In those cases, it was necessary to reprocess data or apply constraints. Indexed parameters were calculated as parameters divided by body surface area in m2 (BSA).

Representative 82Rb-PET images from the two scans at rest during end-systole and end-diastole. Slices of horizontal long axis (first and fourth columns), vertical long axis (second and fifth column), and short axis (third and sixth columns), including contours as created by the two software packages
Statistical Analyses
SAS version 9.4 (SAS Institute, Cary, NC, USA) was used for statistical analyses. Continuous variables were expressed as means with standard deviations. Differences between scans and between software packages were analyzed with paired t tests and the Bland-Altman method with 95% confidence intervals and limits of agreement. P values < .05 were considered statistically significant.
Results
Study Population and Hemodynamic Parameters
Characteristics of participants are summarized in Table 1. The 40 healthy volunteers had a mean (± SD) age of 24 ± 4 years and 50% were men. Mean body mass index was 23 ± 3 kg/m2. Time between the two scans was 17 ± 14 days. All participants had CACS of 0. There was a tendency of lower heart rate and blood pressures at the second scan compared with the first. However, we found no significant difference in hemodynamic parameters from rest to stress between the two scans.
Reproducibility of LVEF, LV Volumes, and LV Mass Between Scans
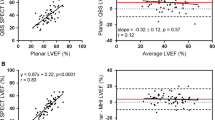
Resting and stress mean values of LVEF, ESV, EDV, and LV mass for the two scans and by the two different software packages are summarized in Table 2. Furthermore, 4DM data are shown without and with manual valve plane adjustment. LV mass was only available from 4DM. LV mass was higher by stress scans compared with rest scans: mean difference (95% CI) 3.0 (1.5 to 4.5), P < .001, limits of agreement: − 9.8 to 15.8. Both at rest and during stress, we found high reproducibility of all parameters between scans and this was true for both software packages (Table 2). Additionally, reproducibility was similar for 4DM without and with manual valve plane adjustment. The reproducibility between scans of LVEF reserve was also high for both software packages. In Figure 2A and B are shown Bland-Altman plots comparing LVEF at rest from the two scans measured by 4DM as an example.

Bland-Altman plots of LVEF at rest: (A) comparison of scan 1 and 2 using 4DM (automatically processed data); (B) comparison of scan 1 and 2 using QGS; (C) comparison of QGS and 4DM (automatically processed data)
Reproducibility of LVEF and LV Volumes Between Software Packages
When comparing LVEF, ESV, and EDV at rest and during stress between the two different software packages, we found significant differences between software packages on all functional parameters both at rest LVEF: mean difference (95% CI) 8.7 (8.1 to 9.4), P < .0001, limits of agreement: 3.1; 14.4; ESV: mean difference (95% CI) − 18.2 (− 20.0 to − 16.5), P < .0001, limits of agreement: − 33.1; − 3.3; and EDV: mean difference (95% CI) − 17.2 (− 18.6 to − 15.9), P < .0001, limits of agreement: − 28.9; − 5.6; and during stress LVEF: mean difference (95% CI) 8.0 (7.4 to 8.5), P < .0001, limits of agreement: 3.2; 12.7; ESV: mean difference (95% CI) − 13.4 (− 14.7 to − 12.1), P < .0001, limits of agreement: − 24.6; − 2.1; and EDV: mean difference (95% CI) − 6.9 (− 8.3 to − 5.4), P < .0001, limits of agreement: − 19.8; 6.1. Results were similar after manually adjusting the valve plane for 4DM measures. The minimum and maximum LVEF for QGS were 48% and 77% during rest and 53% and 82% during stress. For 4DM minimum and maximum values were 34% and 69% at rest and 46% and 74% during stress. After manually adjusting the valve plane, 4DM minimum and maximum values were 48% and 74% at rest and 52% and 79% during stress. LVEF reserve also differed significant between software packages: mean difference (95% CI) − 0.8 (− 1.6 to − 0.04), P < .04, limits of agreement: − 7.3 to 5.7. This difference, however, became non-significant after adjustment of 4DM valve plane: mean difference (95% CI) 0.5 (− 0.6 to 1.6), P < .36, limits of agreement: − 9.1 to 10.1. Figure 2C illustrates the Bland-Altman plot comparing LVEF at rest from 4DM and QGS as an example.
Indexed Functional Parameters in Men and Women
Table 3 shows LVEF and indexed ESV, EDV, and LV mass for men and women at rest and during stress for the two scans using both software packages for LVEF and volume indexes and using 4DM for LV mass index. 4DM LVEF and volume data are valve plane-adjusted measures. In all scan parameters in both scans at all times and using both software packages, women differed significantly from men. LVEF was significantly higher in women than in men and ESV index and EDV index were significantly smaller in women as was LV mass index.
Discussion
In this study, we investigated the reproducibility of different global functional parameters assessed by 82Rb-PET/CT between two scans and between two commercially available software packages in 40 healthy young volunteers. We found high reproducibility between scans for all parameters but poor concordance between software packages. In addition, we found that women differed significantly from men in all parameters and that LV mass was systematically higher measured during stress than at rest.
The reproducibility that we showed between scans has not previously been assessed and previous correlation studies with other scan modalities6,7,–8 combined with our results substantiate that global functional parameters measured by PET can be suitable for clinical use. In accordance with a study by Bravo et al, we also found poor reproducibility between software packages.13 Explanations for these differences between software packages may to some extend be explained by nuances of edge detection or valve plane determination; however, we did not have access to the algorithms of the software.
When comparing our results analyzed by 4DM both with and without manual valve plane adjustment with the results by Bravo et al also using 4DM, our results for LVEF were comparable. Contrary, we found higher ESV and EDV with 4DM than Bravo et al. This could in part be explained by the fact that 91% of patients in the study by Bravo et al were women contrary to 50% in our study. In our study and in the literature, investigated by SPECT and cMRI, women has been shown to have lower ESV and EDV and higher LVEF than men.16,17,–18 That LVEF was not correspondingly higher in the study by Bravo et al compared with ours may be explained by the fact that these patients were older. Another explanation of the differences could be that we used a newer version of 4DM than Bravo et al and that the two versions may differ. When comparing our results on LVEF, ESV, and EDV assessed by QGS with results from QGS by Bravo et al, LVEF was markedly higher in our study, whereas ESV was equivalent and EDV was higher. This may also been explained by the fact that we used a newer software version.
Previous studies have suggested associations between LVEF reserve and clinical outcomes.9,10,–11 We found high reproducibility of this parameter between scans but a significant, although not pronounced, difference between software packages. However, this significant difference disappeared, when using 4DM data with manual valve plane adjustment. Our findings question whether LVEF reserve can be used as a prognostic marker in general or only within the software packages previously investigated.
Our finding that LV mass analyzed with 4DM was systematically higher during stress than at rest was in contrast to a previous study, suggesting that LV mass remains unchanged between the two conditions and thereby can be used as a quality control check on rest and stress LVEF computed from 82Rb-PET data.12 Our results indicate that this may not be true for all software packages. An explanation could be that mass is calculated on the basis of the endo- and epicardial borders, which will naturally vary slightly between rest and stress, as they are probably not taken in the exact same frame due to change in heart rate from rest to stress.
The use of 3D acquisition has been shown to be feasible for quantifying myocardial blood flow.19 However, studies comparing functional parameters between 2D and 3D acquisition has not been performed. Therefore, our findings may not be applicable for systems using 3D acquisition.
Study Limitations
This study has some limitations that should be considered. This study was conducted in healthy young volunteers with LVEF in the normal range and we cannot rule out that the results would have differed in older individuals and in patients with comorbidities and in patients with different degrees of heart failure; therefore, results cannot necessarily be used as reference values for patients in general. However, we find establishment of data in normal subjects important to test reproducibility and for later comparison with older individuals and patients with cardiovascular disease.
New Knowledge Gained
This study is, to our knowledge, the first to compare functional parameters from 82Rb-PET/CT between two scans and between different software packages in healthy young volunteers of both sexes equally represented. Our results indicate that the global functional parameter measures are reliable, but that each software package should have its own normal reference range and that the same software package should be used when interpreting functional parameters. Thus, it is possible to use functional parameters from 82Rb-PET/CT in a clinical setting, but sex-specific normal range in older individuals needs to be better established.
Conclusion
In healthy volunteers, we found high reproducibility between scans when measuring the global functional parameters LVEF, LVEF reserve, ESV, EDV, and LV mass from 82Rb-PET/CT using the same software package. In contrast, we found poor concordance between parameter measures when comparing the two commercially available software packages.
Abbreviations
- 82Rb-PET/CT:
-
Rubidium-82 positron emission tomography/computed tomography
- BSA:
-
Body surface area
- CACS:
-
Coronary artery calcium score
- cMRI:
-
Cardiac magnetic resonance imaging
- EDV:
-
Enddiastolic volume
- ESV:
-
Endsystolic volume
- LV:
-
Left ventricle
- LVEF:
-
Left ventricular ejection fraction
- SPECT:
-
Single-photon emission computerized tomography
References
2014 ESC/EACTS. Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of percutaneous cardiovascular interventions (EAPCI). Eur Heart J 2014;35:2541-619.
Di Carli MF, Dorbala S, Meserve J, El Fakhri G, Sitek A, Moore SC. Clinical myocardial perfusion PET/CT. J Nucl Med Off Publ Soc Nucl Med 2007;48:783-93.
El Fakhri G, Kardan A, Sitek A, Dorbala S, Abi-Hatem N, Lahoud Y, Fischman A, Coughlan M, Yasuda T, Di Carli MF. Reproducibility and accuracy of quantitative myocardial blood flow assessment with (82)Rb PET: Comparison with (13)N-ammonia PET. J Nucl Med Off Publ Soc Nucl Med 2009;50:1062-71.
Yoshinaga K, Chow BJW, Williams K, Chen L, deKemp RA, Garrard L, Lok-Tin Szeto A, Aung M, Davies RA, Ruddy TD, Beanlands RSB. What is the prognostic value of myocardial perfusion imaging using rubidium-82 positron emission tomography? J Am Coll Cardiol 2006;48:1029-39.
Chander A, Brenner M, Lautamaki R, Voicu C, Merrill J, Bengel FM. Comparison of measures of left ventricular function from electrocardiographically gated 82Rb PET with contrast-enhanced CT ventriculography: A hybrid PET/CT analysis. J Nucl Med 2008;49:1643-50.
Hofman HA, Knaapen P, Boellaard R, Bondarenko O, Götte MJW, van Dockum WG, Visser CA, van Rossum AC, Lammertsma AA, Visser FC. Measurement of left ventricular volumes and function with O-15-labeled carbon monoxide gated positron emission tomography: Comparison with magnetic resonance imaging. J Nucl Cardiol Off Publ Am Soc Nucl Cardiol 2005;12:639-44.
Schaefer WM, Lipke CSA, Nowak B, Kaiser H-J, Reinartz P, Buecker A, Krombach GA, Buell U, Kühl HP. Validation of QGS and 4D-MSPECT for quantification of left ventricular volumes and ejection fraction from gated 18F-FDG PET: Comparison with cardiac MRI. J Nucl Med Off Publ Soc Nucl Med 2004;45:74-9.
Ben Bouallègue F, Mariano-Goulart D, Agostini D, Manrique A. Feasibility of biventricular volume and function assessment using first-pass gated 15O-water PET. EJNMMI Res 2018;8:92.
Dorbala S, Hachamovitch R, Curillova Z, Thomas D, Vangala D, Kwong RY, Di Carli MF. Incremental prognostic value of gated Rb-82 positron emission tomography myocardial perfusion imaging over clinical variables and rest LVEF. JACC Cardiovasc Imaging 2009;2:846-54.
Lertsburapa K, Ahlberg AW, Bateman TM, Katten D, Volker L, Cullom SJ, Heller GV. Independent and incremental prognostic value of left ventricular ejection fraction determined by stress gated rubidium 82 PET imaging in patients with known or suspected coronary artery disease. J Nucl Cardiol Off Publ Am Soc Nucl Cardiol 2008;15:745-53.
Dorbala S, Vangala D, Sampson U, Limaye A, Kwong R, Di Carli MF. Value of vasodilator left ventricular ejection fraction reserve in evaluating the magnitude of myocardium at risk and the extent of angiographic coronary artery disease: A 82Rb PET/CT study. J Nucl Med Off Publ Soc Nucl Med 2007;48:349-58.
Van Tosh A, Reichek N, Phippen-Nater B, Palestro CJ, Nichols KJ. Consistency of myocardial mass computations as a quality control check on rest and stress left ventricular ejection fractions computed from (82)Rb PET data. Clin Nucl Med 2014;39:593-7.
Bravo PE, Chien D, Javadi M, Merrill J, Bengel FM. Reference ranges for LVEF and LV volumes from electrocardiographically gated 82Rb Cardiac PET/CT using commercially available software. J Nucl Med 2010;51:898-905.
Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990;15:827-32.
Armstrong IS, Tonge CM, Arumugam P. Impact of point spread function modeling and time-of-flight on myocardial blood flow and myocardial flow reserve measurements for rubidium-82 cardiac PET. J Nucl Cardiol 2014;21:467-74.
Sharir T, Kang X, Germano G, Bax JJ, Shaw LJ, Gransar H, Cohen I, Hayes SW, Friedman JD, Berman DS. Prognostic value of poststress left ventricular volume and ejection fraction by gated myocardial perfusion SPECT in women and men: Gender-related differences in normal limits and outcomes. J Nucl Cardiol Off Publ Am Soc Nucl Cardiol 2006;13:495-506.
Rozanski A, Nichols K, Yao SS, Malholtra S, Cohen R, DePuey EG. Development and application of normal limits for left ventricular ejection fraction and volume measurements from 99mTc-sestamibi myocardial perfusion gates SPECT. J Nucl Med Off Publ Soc Nucl Med 2000;41:1445-50.
Chung AK, Das SR, Leonard D, Peshock RM, Kazi F, Abdullah SM, Canham RM, Levine BD, Drazner MH. Women have higher left ventricular ejection fractions than men independent of differences in left ventricular volume: The Dallas Heart Study. Circulation 2006;113:1597-604.
Manabe O, Naya M, Aikawa T, Obara M, Magota K, Kroenke M, Oyama-Manabe N, Hirata K, Shinyama D, Katoh C, Tamaki N. PET/CT scanning with 3D acquisition is feasible for quantifying myocardial blood flow when diagnosing coronary artery disease. EJNMMI Res 2017;7:52.
Disclosures
Christina Byrne, Andreas Kjaer, Julie Lyng Forman, and Philip Hasbak declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The authors of this article have provided a PowerPoint file, available for download at SpringerLink, which summarizes the contents of the paper and is free for re-use at meetings and presentations. Search for the article DOI on SpringerLink.com.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Byrne, C., Kjaer, A., Forman, J.L. et al. Reproducibility of LVEF, LV volumes, and LV mass between Rubidium-82 PET/CT scans in young healthy volunteers using two commercially available software packages. J. Nucl. Cardiol. 27, 1237–1245 (2020). https://doi.org/10.1007/s12350-019-01698-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-019-01698-9