
Abstract
Background
Recent literature suggests that the frequency of abnormal SPECT myocardial perfusion imaging (MPI) has decreased over the past two decades despite an increase in the prevalence of many cardiac risk factors. This study examined the trends in the prevalence of obstructive coronary artery disease (CAD) by abnormal and ischemic MPI and invasive angiography.
Methods
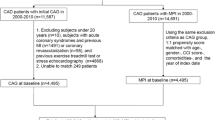
We analyzed all patients who underwent stress MPI or invasive angiography at two academic centers between January 1996 and December 2012, for their demographic data and study results.
Results
A total of 108,654 MPI studies were performed. Over time, the percentage of patients with hypertension, hyperlipidemia, diabetes, and a history of smoking increased. There was a decline in the prevalence of abnormal MPI studies in all patients as well as in those with and without known CAD (from 47.2%, 71.8%, and 31.4% in 1996 to 33.9%, 64.8%, and 18.8% in 2012, respectively, all P < .0001). Similarly, there was a decline in the prevalence of ischemic MPI studies in all patients as well as in those with and without known CAD. A total of 142,924 invasive angiograms were performed. There was a decline in the prevalence of one-vessel and multi-vessel coronary disease (from 29.1% and 53.6% in 1996 to 22.4% and 35.9% in 2012, respectively, all P < .0001).
Conclusions
There has been a temporal decline in the prevalence of abnormal and ischemic MPI studies as well as the frequency and extent of obstructive CAD on angiography. However, this decline was not to the same extent as previously reported, and the overall 34% abnormal MPI rate, with 19% in patients with no known CAD and 65% in patients with known CAD, remains a clinically relevant percentage of patients tested.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Stress myocardial perfusion imaging (MPI) remains the most commonly used non-invasive modality for the assessment of coronary artery disease (CAD). While CAD remains the leading cause of mortality in the United States,1 epidemiologic data indicate that improved control of cardiac risk factors has resulted in a temporal decline in the incidence and severity of CAD as well as its associated mortality.2,3 Recent literature from a large academic center has suggested a progressive decline in the frequency of both abnormal and ischemic single-photon emission computed tomography (SPECT) MPI studies over the past two decades among patients without known CAD.4 Interestingly, this temporal MPI trend occurred within all demographic, clinical, risk factor, and stress modality subgroups despite a concomitant increase in the prevalence of some risk factors and an increased pre-test probability of CAD. While the apparent decline in CAD prevalence and its associated mortality has important implications with regard to stress MPI utilization, confirmation of the aforementioned findings is needed before contemplating alternative strategies. In the previous study, patients with known CAD were not evaluated which make up a sizeable proportion of most nuclear cardiology laboratory’s patient volume. Hence, we examined the temporal trends of the prevalence of abnormal and ischemic MPI studies in two large academic centers as well as investigated the frequency of obstructive CAD by invasive angiography at these institutions in a multiyear clinical database review.
Methods
Study Design
We included all patients who underwent clinically indicated stress MPI (SPECT or PET) at Hartford Hospital (a 900 bed urban teaching hospital) and Mount Sinai Hospital (a 1,200 bed inner city teaching hospital) between January 1996 and December 2012 and were part of ongoing prospective databases at both institutions. This study was approved by and conducted within guidelines of the Institutional Review Board at Hartford Hospital and Mount Sinai Hospital. Patients with repeat studies were included, and each study was considered individually in the analysis in order to consider the laboratory’s complete patient volume over this time period. Tl-201 or PET studies performed for the sole purpose of cardiac viability assessment were excluded. The prospectively collected MPI database at Hartford Hospital began in 1996 and was consistent through 2012, while the Mount Sinai Hospital database was upgraded in 2004, and prior to 2004 some demographic variables were not consistently available. The study group was divided into 4 temporal subgroups for the purposes of analysis: 1996 to 2000, 2001 to 2004, 2005 to 2008, and 2009 to 2012.
At the time of testing, pertinent demographic and clinical information, past cardiac history, and CAD risk factors were recorded based on patient report or available medical records. A family history of premature CAD was defined as a diagnosis of CAD in a first-degree relative prior to or at 55 years of age. Smoking history was defined as prior or current tobacco use. A patient was considered to have known CAD at the time of their stress test based on a provided history of previously diagnosed atherosclerotic coronary disease, history of myocardial infarction, history of percutaneous coronary intervention (PCI), or history of coronary artery bypass grafting (CABG). An abnormal ECG was defined as any abnormal findings short of atrial or ventricular premature beats and first-degree AV block. This included nonspecific or abnormal T waves or ST segments, pathologic Q waves, bundle branch blocks, paced rhythms, atrial fibrillation, atrial flutter, and second or higher degree AV block.
Stress and Imaging Protocols
Standard exercise and pharmacologic protocols as endorsed by ASNC were employed.5 For ambulatory patients with known or perceived functional limitations at the time of testing, a combined stress protocol of vasodilator stress with adjunctive exercise was also utilized. In such cases, exercise stress began after completion of dipyridamole infusion, at the start of adenosine infusion, and if a patient was unable to reach a standard exercise testing endpoint, regadenoson was used only as needed. Standard imaging and radionuclide dosing protocols (for SPECT and PET) as endorsed by ASNC were used for all patients.5
Image Interpretation
Semi-quantitative perfusion scoring of the stress and rest images was performed by board certified nuclear cardiologists. Using a 17-segment model and visual semi-quantitative scoring system, each segment was scored at the time of the clinical performance of the test with access to the patient’s clinical and stress test data.6 With the introduction and routine utilization of attenuation correction (both Gd-153 line source and prone imaging), all images were visually interpreted and scored in sequence, non-attenuation-corrected data first followed by attenuation-corrected data using the same 17-segment model and semi-quantitative scoring system. Summed stress scores (SSS), summed rest scores (SRS), and summed difference score (SDS) were calculated, and a stress and difference total perfusion defect (TPD) % was calculated by dividing the SSS and SDS, respectively, by the maximum score possible to compare the severity of defects. A normal study was defined as a normal clinical interpretation (typically a SSS ≤3 for non-attenuation-corrected images and a SSS ≤1 for attenuation-corrected images), and an ischemic study was defined as an abnormal clinical interpretation with a SDS ≥1. Ischemic studies were further classified as having >5% or >10% ischemia based on the difference TPD%.
Coronary Angiography
Patients who underwent a clinically indicated invasive coronary angiogram from 1996 to 2012 at Hartford Hospital and 2004 to 2012 at Mount Sinai had the results of their angiogram prospectively recorded in a clinical database. These patients included elective outpatient and inpatient angiograms as well as emergent acute coronary syndrome procedures. Luminal diameter narrowing for the left main and the three major coronary arteries and their major branches at the time of cardiac catheterization were visually estimated by the performing board certified interventional cardiologist. Obstructive disease was defined as ≥70% stenosis in any of the three major coronary arteries (or their major branches) or ≥50% stenosis of the left main coronary artery. Patients were classified as having non-obstructive, single-vessel, multi-vessel, or left main disease.
Statistical Analysis
Clinical and baseline characteristics were expressed as mean ± standard deviation or as percentages. Inter-group comparisons were performed using a one-way ANOVA for continuous variables and the Chi square for a trend for categorical variables. Binary Logistic regression was performed to calculate odds ratios with 95% confidence intervals.
Propensity scores were generated from logistic regression. A nearest neighbor 1:1 match was used as the basis for matching, with matching distance calculation using Mahalanobis distances.
A P < .05 was considered statistically significant. Statistical analyses were performed with SPSS software version 19 (IBM/SPSS, Armonk, NY USA 2012).
Results
Demographics and Clinical Characteristics
During this 17-year time period, a total of 108,654 studies were performed at the two institutions. The demographic, clinical characteristics and stress test results over time in all patients are shown in Table 1. The mean age of patients and proportion of males undergoing testing over this time remained relatively unchanged. The mean body mass index (BMI) increased with an increase in the percentage of obese individuals (BMI >30) and decrease in normal weight subjects (BMI <25). Over time, the percentage of outpatients decreased, while the percentage of inpatient and ED patients increased and the proportion of patients with traditional risk factors of hypertension, hyperlipidemia, diabetes, and a history of smoking increased. The percentage of patients with known CAD decreased which was accompanied by an increase in the history of PCI and decrease in the history of CABG. Over this period, there was an increase in the frequency of patients undergoing pharmacologic stress. The temporal patterns for demographic and clinical characteristics in patients with no known CAD (Table 2) and known CAD (Table 3) were generally similar to those observed in all patients, but with a higher prevalence of older patients, males, cardiac risk factors, and pharmacologic stress observed in those with known vs no known CAD.
Stress MPI Results
As shown in Tables 1, 2 and 3, there was a decline in the prevalence of abnormal stress MPI studies in all patients (from 53.8% during the earliest time period to 31.8% during the most recent, P < .0001) as well as in those without and with known CAD (from 32.2% and 74.7% during the earliest time period to 18.0% and 60.8% during the most recent respectively, both P < .0001). In patients with abnormal studies, the mean stress TPD fluctuated while the mean difference TPD remained relatively constant over time. The trend for the mean stress TPD for patients with abnormal perfusion was the same with and without known CAD, but the mean difference TPD decreased in patients with no known CAD and increased in those with CAD. There was also a decline in the prevalence of ischemic MPI studies in all patients over this time period (from 23.0% during the earliest to 19.1% during the most recent, P < .0001). In patients with no known CAD, a decrease in the prevalence of ischemic studies was seen between the first and last time periods (from 16.9% to 10.7%, P < .0001). However, in patients with known CAD, there was an increase in the prevalence of ischemic results (from 33.6% during the earliest time period to 37.0% during the most recent, P < .0001).
As shown in Figure 1A, there was a temporal decline in the prevalence of abnormal stress MPI studies in all patients (from 54.0% in 1996 to 33.7% in 2012, P < .0001) as well as in those with and without known CAD (from 76.4% and 31.4% in 1996 to 64.5% and 18.8% in 2012, respectively, both P < .0001). Similarly, as shown in Figure 1B, there was a temporal decline in the prevalence of ischemic MPI studies in all patients (from 29.4% in 1996 to 18.3% in 2012, P < .0001) as well as in those with and without known CAD (from 41.8% and 21.3% in 1996 to 37.8% and 8.8% in 2012, respectively, both P < .0001). However, by 2004, the reduction in the number of abnormal studies in the full cohort had been completed with a decline of 20% points (54.0% to 24.0%) over those eight years and only a 0.3% point decline over the next 8 years. A similar phenomenon was seen in the subgroup of patients with and without known CAD (13.0% and 8.9% point decline followed by a 1.0 point increase and 3.7 point decline, respectively). This trend parallels the decrease in the total volume of MPI studies, which peaked between 2004 and 2006 and decreased thereafter (Figure 2). Figure 3 illustrates the decline in the prevalence of studies with ischemia based on the degree of ischemia, any, >5%, or >10%. In patients with no known coronary disease, the prevalence of >10% ischemic burden declined from 8.2% in 1996 to 2.2% in 2012, while in patients with known coronary disease, it declined from 15% to 9.4%. The trend for >5% ischemia falls between the prevalence of any ischemia and >10% ischemia.

Trends in abnormal and ischemic myocardial perfusion imaging studies over 17 years

Myocardial perfusion imaging volume over time

Trends in the severity of ischemic myocardial perfusion imaging studies over 17 years in patients with and without known CAD
Temporal Predictors of Abnormal Stress MPI Studies
The prevalence of abnormal MPI results based on patient demographics and clinical characteristics was examined over time and is shown in Table 4. There was a progressive decline in the prevalence of abnormal stress MPI studies within all ages, genders, BMI’s, and within all traditional cardiac risk factors. There was a larger decline seen among outpatients and ED patients compared to inpatients and a larger decline seen in exercise stress compared to pharmacologic stress. There was little clinically significant change in patients with a history of PCI or CABG.
Odds ratios for having an abnormal stress MPI study by time period are shown in Table 5. Age and BMI showed no change in their association with an abnormal study over time. The odds ratios for male gender, outpatient, and ED setting showed a decrease, while traditional cardiac risk factors, known CAD, history of PCI, and CABG demonstrated an increase. The odds ratio for pharmacologic as well as pharmacologic plus exercise stress was higher than exercise stress throughout the time periods with an increase over time, likely reflecting more comorbidities and greater risk factor burden in the non-exercise stress group. The odds ratio for PET imaging was higher than SPECT imaging likely reflecting a degree of referral bias of “sicker” or more complex patients to PET.
Temporal MPI Trends After Propensity Matching
We compared 1,000 propensity-matched patients and matching variables included age (P = .88), gender (P = .97), BMI (P = .98), patient location (P = 1.0), hypertension (P = 1.0), diabetes (P = 1.0), hyperlipidemia (P = 1.0), smoking (P = 1.0), CAD (P = 1.0), PCI (P = 1.0), and CABG (P = 1.0) (Table 6). Within this cohort, there remained a temporal decrease in the frequency of abnormal MPI studies from 39.1% to 32.4% (P = .014) similar to, but smaller in magnitude to the results seen in the non-matched cohort. In patients with abnormal results, the mean total stress perfusion defect size increased over time, while the mean difference in TPD size did not significantly change.
Temporal Trends of Invasive Coronary Angiography
A total of 142,924 invasive angiograms performed at the two institutions during this 17-year time period were reviewed. Similar to the observations with stress MPI, there was a progressive decline in the prevalence of obstructive CAD by angiography (77.2% during the 1996 to 2000 period, 74.5% during the 2001 to 2004 interval, 71.1% during the 2005 to 2008 time period, and 67.9% during the 2009 to 2012 interval, P < .001). Furthermore, and as shown in Figure 4, there was a temporal decline in the prevalence of one-vessel CAD, multi-vessel CAD, and LM disease (from 29.1%, 53.6%, and 12.2% in 1996 to 22.4%, 35.9%, and 5.7% in 2012, respectively, all P < .0001) with a corresponding temporal increase in the prevalence of non-obstructive CAD (from 11.8% in 1996 to 17.6% in 2012, P < .0001).

Occurrence of coronary artery disease by invasive angiography over time
Specific Populations
The emergency department chest pain unit patient and the pre-liver transplant patient are two known low-risk populations which may not be found at all institutions.7,8 A total of 6,494 patients were studied from the ED (overall 20.1% rate of abnormal MPI studies), and 5,165 patients were studied as part of their pre-transplantation evaluation (overall 21.3% rate of abnormal MPI studies). When the ED patients are removed from the cohort, the percent of abnormal studies increases 1.6% points to 33.4% in the 4th time period, and when the pre-transplant patients are removed from the cohort, the percent of abnormal studies increases 1.8% points to 33.6% in the 4th time period. If both groups are removed, the prevalence of abnormal studies increases 3.7% points to 35.5% in the 4th time period.
Two higher risk subgroups include patients undergoing PET MPI and patients receiving Tl-201 as the imaging isotope because of potential referral bias of perceived “sicker” patients to these imaging modalities. Over the entire study period, PET imaging had a 55.2% rate of abnormal studies compared to 38.7% for SPECT imaging. The subgroup of patients imaged with Tl-201 also had a higher percentage of abnormal patients, 56.1% during the study period, compared to 38.1% with Tc-99m agents. This is in spite of excluding from analysis patients referred for viability testing. Interestingly, during the 2009-2012 time period when Tl-201 was substituted for Tc-99m due to shortages, a 38.0% prevalence of abnormal studies was seen which was similar to Tc-99m.
Discussion
Our study demonstrates that in patients who underwent clinically indicated stress MPI between 1996 and 2012, the frequency of abnormal and ischemic studies declined over time. There was a 14% decrease in the prevalence of abnormal stress MPI studies between the 1996-2000 and 2009-2012 time periods (P < .0001) both in patients with no known CAD and in those with known CAD. The declining frequency of abnormal stress MPI was observed among all age groups, both genders, in inpatients and outpatients, and across all cardiac risk factors similar to the previous report.4 However, the most recent prevalence of abnormal and ischemic MPI results was not as low as previously reported in patients with no known CAD, and in patients with known CAD, the prevalence of abnormal studies remains high.
Rozanski et al noted that over the past two decades, the frequency of abnormal stress SPECT-MPI studies has declined markedly.4 In their study, the prevalence of abnormal studies decreased from 40.9% in 1991 to 8.7% in 2009 (a decrease of 32.2%). In addition, the frequency of myocardial ischemia decreased from 29.6% to 5.0% (a decrease of 24.6%). Our results in patients without known CAD demonstrate a less dramatic decline (14.2%) with abnormal MPI studies in 18.4% of patients in 2009 and 18.8% in 2012, with a 12.4% decline in ischemic studies resulting in 11.3% ischemic studies in 2009 and 8.8% in 2012. Compared to the West Coast population, the East Coast population in the current study included a smaller proportion of outpatients, had a larger BMI, and had a greater prevalence of hypertension, high cholesterol, smoking, and diabetes which may have been responsible for the different results. In the subgroup of known CAD patients which was not studied in the previous paper, we found that the decline was less pronounced. Furthermore, the rate of decline in the prevalence of abnormal studies has been minimal in the second half of the time period after 2004 with only a 0.3% point decrease in the entire cohort during that time. In patients with known CAD, the percentage of abnormal studies actually increased by 1% point, while there was a minimal 3.7% point decrease in the no known CAD group. This reduction in the rate of decline of the proportion of abnormal studies correlated with the beginning of a national trend of reduction in SPECT-MPI patient volume and roughly corresponds to decreasing annual volumes in this study.9
Countercurrent to the decreasing proportion of abnormal MPI studies, there was a changing pattern of risk factors noted over this entire time period, with patients carrying a heavier burden of traditional risk factors over time. This included a greater proportion of obese patients and an increase in the prevalence of all of the traditional cardiac risk factors except family history. In spite of the rising trend of the risk factors, there was a temporal decrease in patients with a history of known CAD, with fewer post-CABG patients but a greater degree of post-PCI patients. Rozanski et al found a similar trend with increasing frequency of hypertension, diabetes, and hyperlipidemia but a declining prevalence of smoking and family history.4 A number of studies have evaluated the prevalence of CAD risk factors in different populations and in contrast to our study and that of Rozanski et al, most have shown a declining prevalence of hypertension, hyperlipidemia, and smoking but an increase in the prevalence of diabetes.2,10-12 Ford et al13 examined US deaths from cardiovascular disease over a twenty-year time period and noted a decline in cardiovascular deaths nationally, attributing this to risk factor reduction. While they noted significant reductions in systolic blood pressure, cholesterol levels, and smoking prevalence, there was an increase in the burden of diabetes and obesity, suggesting that it is the control of these risk factors with medical therapy despite increasing absolute numbers of people with the diseases that are affecting outcomes. Supporting this, a recent study using data from the National Health Interview Survey found that the prevalence of diabetes in the US population increased threefold between 1990 and 2010, but the number of patients who suffered acute myocardial infarction within this group declined significantly.14 These findings are similar to the trend of decreasing abnormal MPI studies in spite of increased risk factor burden observed in our study.
Other factors to explain the decreasing prevalence of abnormal MPI studies may be in play besides the early recognition of cardiac risk factors resulting in aggressive medical therapy to prevent the development of clinically significant obstructive disease including changes in patient referral patterns to other modalities and testing of lower risk patients. With advances in the safety and efficacy of coronary angiography and percutaneous coronary intervention over this time period, there might be a lower threshold for referring patients directly to cardiac catheterization, thereby decreasing the proportion of abnormal MPI studies among those referred for non-invasive testing. Given the increasing prevalence of non-obstructive invasive angiograms over time seen in this study and in other reports,15-18 this factor may have played a role. Another explanation for the increase in normal MPI studies may be the use of improved SPECT imaging technology. New SPECT cameras, reconstruction software, and attenuation correction all debuted during this time period. The frequency of abnormal results decreased more dramatically through 2004 after which the downward trend was slower, which roughly corresponded to the introduction of the new technologies.
Two subsets that tend to have a high prevalence of normal MPI results are patients referred for transplant evaluation and low-risk patients triaged through the emergency department chest pain unit. Zoghbi et al reported high incidence of normal MPI results (91%) in a retrospective study evaluating patients who underwent SPECT MPI for pre-operative evaluation prior to liver transplantation.8 In addition, low-risk chest pain unit patients from the emergency room have been shown to have low rates of abnormal MPI results.7 Our findings confirm these previous observations as each subgroup had low rate of abnormal MPI (approximating 20%) and our rate of abnormal MPI increased when they were excluded from the analysis.
Another important finding from our investigation is the declining prevalence of obstructive CAD revealed on cardiac catheterization during the same time period (77.2%, 74.5%, 71.1%, and 67.9%, respectively, in the 4 temporal groups). There have been previous studies15-18 also demonstrating a lower prevalence of angiographically significant CAD in patients with typical angina. Similar to our observations, findings from these angiographic studies may be indicative of earlier and improved medical therapy in patients at risk of CAD resulting in less obstructive coronary disease.
Limitations
This is a retrospective review with all of the limitations inherent to retrospective studies. We do not have information on cardiac medications at the time of testing and thus are unable to examine these trends in relation to the decreasing prevalence of abnormal MPI studies and obstructive CAD on angiography. We did not have access to data on preceding MPI studies in patients who underwent coronary angiograms and therefore it could not be analyzed. Outcomes data, such as cardiac events or mortality, were not available on all patients to correlate with the MPI and angiography findings. All patients, patients with no known CAD, patients with known CAD, and SPECT and PET perfusion studies, were all analyzed in order to demonstrate the complete, unselected trends in clinical study results over this time period. The two sites in this study were not analyzed separately as the purpose of the study was to get a multi-center experience that would mitigate the idiosyncrasies that might exist at a single clinical center. During the course of the study, there were changes in the SPECT imaging technology including improved SPECT cameras, the use of attenuation correction, and new reconstruction software all of which could potentially have impacted the results.
New Knowledge Gained
This study confirms the decrease in the detection of CAD from MPI in two large nuclear cardiology laboratories between 1996 and 2012, although not to the extent previously reported. The overall 34% abnormal rate, with 19% in patients with no known CAD and 65% in patients with known CAD, remains a clinically relevant percentage of patients tested for an important diagnostic screening test.
Conclusions
Our study of patients who underwent a clinically indicated stress MPI at two large academic nuclear cardiology laboratories between 1996 and 2012 confirms the decrease in the detection of CAD from MPI although not to the extent reported previously. Concurrently, there was also a decrease in the incidence and extent of obstructive epicardial CAD on coronary angiographies performed during the same time period. However, the overall 34% abnormal rate, with 19% in patients with no known CAD and 65% in patients with known CAD, remains a clinically relevant percentage of patients tested and similar to other major disease states like the 23% positive rate seen for pulmonary emboli in the PIOPED II study.19 But with a declining prevalence of abnormal results, it is prudent to maximize the cost-effectiveness of non-invasive approaches in the assessment of patients with suspected CAD. Solutions may include re-evaluation of pre-test risk stratification, wider use of exercise stress testing without imaging, and the use of stress-only imaging (with concomitant radiation dose reduction and cost savings).
References
Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, et al. Heart disease and stroke statistics-2014 update: A report from the American Heart Association. Circulation 2014;129:e28-292.
Sytkowski PA, Kannel WB, D’Agostino RB. Changes in risk factors and the decline in mortality from cardiovascular disease. The Framingham Heart Study. N Engl J Med 1990;322:1635-41.
Myerson M, Coady S, Taylor H, Rosamond WD, Goff DC Jr. Declining severity of myocardial infarction from 1987 to 2002: the Atherosclerosis Risk in Communities (ARIC) Study. Circulation 2009;119:503-14.
Rozanski A, Gransar H, Hayes SW, Min J, Friedman JD, Thomson LE, et al. Temporal trends in the frequency of inducible myocardial ischemia during cardiac stress testing: 1991 to 2009. J Am Coll Cardiol 2013;61:1054-65.
Henzlova MJ, Cerqueira MD, Mahmarian JJ, Yao SS. Stress protocols and tracers. J Nucl Cardiol 2006;13:e80-90.
Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. J Nucl Cardiol 2002;9:240-5.
Duvall WL, Wijetunga MN, Klein TM, Hingorani R, Bewley B, Khan SM, et al. Stress-only Tc-99m myocardial perfusion imaging in an emergency department chest pain unit. J Emerg Med 2012;42:642-50.
Zoghbi GJ, Patel AD, Ershadi RE, Heo J, Bynon JS, Iskandrian AE. Usefulness of preoperative stress perfusion imaging in predicting prognosis after liver transplantation. Am J Cardiol 2003;92:1066-71.
McNulty EJ, Hung YY, Almers LM, Go AS, Yeh RW. Population trends from 2000-2011 in nuclear myocardial perfusion imaging use. JAMA 2014;311:1248-9.
Carroll MD, Lacher DA, Sorlie PD, Cleeman JI, Gordon DJ, Wolz M, et al. Trends in serum lipids and lipoproteins of adults, 1960-2002. JAMA 2005;294:1773-81.
Cutler JA, Sorlie PD, Wolz M, Thom T, Fields LE, Roccella EJ. Trends in hypertension prevalence, awareness, treatment, and control rates in United States adults between 1988-1994 and 1999-2004. Hypertension 2008;52:818-27.
Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. JAMA 2001;286:1195-200.
Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, Kottke TE, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980-2000. N Engl J Med 2007;356:2388-98.
Gregg EW, Li Y, Wang J, Burrows NR, Ali MK, Rolka D, et al. Changes in diabetes-related complications in the United States, 1990-2010. N Engl J Med 2014;370:1514-23.
Patel MR, Peterson ED, Dai D, Brennan JM, Redberg RF, Anderson HV, et al. Low diagnostic yield of elective coronary angiography. N Engl J Med 2010;362:886-95.
Cheng VY, Berman DS, Rozanski A, Dunning AM, Achenbach S, Al-Mallah M, et al. Performance of the traditional age, sex, and angina typicality-based approach for estimating pretest probability of angiographically significant coronary artery disease in patients undergoing coronary computed tomographic angiography: Results from the multinational coronary CT angiography evaluation for clinical outcomes: An international multicenter registry (CONFIRM). Circulation 2011;124:1-8.
Ko DT, Tu JV, Austin PC, Wijeysundera HC, Samadashvili Z, Guo H, et al. Prevalence and extent of obstructive coronary artery disease among patients undergoing elective coronary catheterization in New York State and Ontario. JAMA 2013;310:163-9.
Levitt K, Guo H, Wijeysundera HC, Ko DT, Natarajan MK, Feindel CM, et al. Predictors of normal coronary arteries at coronary angiography. Am Heart J 2013;166:694-700.
Stein PD, Fowler SE, Goodman LR, Gottschalk A, Hales CA, Hull RD, et al. Multidetector computed tomography for acute pulmonary embolism. N Engl J Med 2006;354:2317-27.
Acknowledgments
The authors would like to thank Deborah Katten and Ramana Maddula for their efforts in retrieving the data from the various nuclear cardiology databases. There was no external funding for this research. All funding came from within the Mount Sinai School of Medicine and Hartford Hospital.
Disclosure
The authors have no financial disclosures related to this research.
Author information
Authors and Affiliations
Corresponding author
Additional information
See related editorial, doi:10.1007/s12350-015-0072-0.
Rights and permissions
About this article

Cite this article
Duvall, W.L., Rai, M., Ahlberg, A.W. et al. A multi-center assessment of the temporal trends in myocardial perfusion imaging. J. Nucl. Cardiol. 22, 539–551 (2015). https://doi.org/10.1007/s12350-014-0051-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-014-0051-x