
Abstract
Background
Appropriate use criteria (AUC) for single-photon emission computed tomography myocardial perfusion images (SPECT-MPI) were developed to address the growth of cardiac imaging studies. However, these criteria have not been vigorously validated. We sought to determine the rate of abnormal stress SPECT-MPI studies and subsequent revascularization procedures as categorized by AUC.
Methods
We retrospectively examined 280 patients who underwent stress SPECT-MPI and categorized these studies as appropriate, inappropriate, or uncertain based on AUC. Data regarding subsequent angiography and revascularization within 6 months after stress SPECT-MPI were collected from the electronic medical record.
Results
280 patients met the inclusion criteria (mean age 67.3 ± 11.4 years, 36 % female). When categorized by AUC, 62.9 % (N = 176) of stress SPECT-MPI were considered appropriate, 13.6 % (N = 38) uncertain, and 23.6 % (N = 66) inappropriate. Appropriate stress SPECT-MPI studies were more likely to have intermediate or high risk results than uncertain or inappropriate studies [40 % (N = 71) vs. 21 % (N = 8) and 18 % (N = 12), respectively; P = 0.008)]. Appropriate studies were associated with an increased rate of coronary angiography [14 % (N = 25)] compared to the uncertain (0 %) and inappropriate [3 % (N = 2)] studies (P = 0.003). There was also an increased rate of revascularization after appropriate studies [9 % (N = 16)] compared to the uncertain (0 %) and inappropriate (0 %) studies (P = 0.006).
Conclusions
Appropriate stress SPECT-MPI studies are more likely to result in abnormal results requiring subsequent revascularization compared to inappropriate and uncertain stress studies. Inappropriate and uncertain stress SPECT-MPI did not lead to subsequent revascularization.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Rapidly increasing healthcare costs, especially cardiovascular imaging services to Medicare beneficiaries, have garnered significant attention in recent years. Between 1993 and 2001, there was a 6.1 % average annual increase in cardiac stress imaging1. In subsequent years, the growth increased to >15 % per year2. To address these concerns, the American College of Cardiology Foundation (ACCF) and the American Society of Nuclear Cardiology (ASNC) developed appropriate use criteria (AUC) for stress single-photon emission computed tomography myocardial perfusion images (SPECT-MPI) in 2005 and updated these AUC in 20093,4. Since 2006, it was noted that the growth of cardiac stress imaging in general and particularly SPECT has plateaued and may have slightly decreased as well. However, utilization of advanced imaging such as coronary computed tomography, magnetic resonance, and positron-emission tomography continues to grow substantially5. The AUC were designed to provide guidance regarding the appropriateness of stress SPECT-MPI based on common clinical scenarios. Previous work from this laboratory has retrospectively categorized stress SPECT-MPI based on appropriateness criteria from both the original 2005 AUC and the updated 2009 version6,7.
The AUC were created by an expert panel who were asked to rate 67 clinical indications for SPECT-MPI as being appropriate, uncertain, or inappropriate4. A criticism of AUC is that they have not been validated in clinical practice. To address this concern, several studies have described the rate of abnormal stress SPECT-MPI results in each appropriateness category8,9. However, no studies have examined the downstream clinical consequences of an abnormal stress SPECT-MPI based on appropriateness categories. It may be useful to understand whether the AUC can predict significant changes in clinical management (e.g., revascularization) resulting from an abnormal stress SPECT-MPI as it would provide further validation of the AUC.
The purpose of this study was to describe the rate of abnormal stress SPECT-MPI results and subsequent revascularization procedures when categorized by AUC. We hypothesized the prevalence of intermediate or high risk stress SPECT-MPI results and subsequent revascularization would be higher in appropriate studies compared to inappropriate and uncertain studies.
Methods
Overall Study Design
The general methodology employed in this study was nearly identical to our earlier study6 except as noted below. This study was approved by the Mayo Clinic Institutional Review Board.
Study Group
The study group consisted of all patients who underwent stress SPECT-MPI at Mayo Clinic, Rochester, MN from May 1, 2005 to May 15, 2005 (before the publication of AUC criteria). Exclusions were as follows:
-
1.
Patients who did not grant research authorization in accordance with Minnesota state law (N = 6).
-
2.
Patients who underwent testing at an off-site location as part of Mayo outreach programs.
-
3.
One patient was excluded due to SPECT-MPI acquisition at rest only.
Database
The Mayo Clinic Rochester Nuclear Cardiology Laboratory maintains a prospective electronic database on all patients undergoing stress SPECT-MPI procedures. Chest pain is categorized as typical angina, atypical angina, or non-cardiac chest pain according to the criteria of Diamond10. The database was used in our initial study of appropriateness6.
Patient Classification of AUC
Patients were classified by the 2009 AUC criteria as previously described in earlier work by the authors with the same assumptions described in those studies6,7. Appropriateness category allocation was a very intensive process. This included hiring two independent registered nurses (RN) who were not employed by our nuclear cardiology laboratory. This process was very rigorous and insured unbiased appropriateness allocation for each patient enrolled in our study.
SPECT-MPI Study Methods
These methods have been described previously11,12. Technetium-99 m (Tc-99m) sestamibi (8-12 mCi) was administered for the resting images and 32-48 mCi of Tc-99m sestamibi for the stress images. Depending on the patients’ functional capacity and comorbidities, they either underwent a symptom-limited treadmill test (Bruce, modified Bruce, or Naughton protocol) or pharmacologic stress testing using adenosine, dipyridamole, or dobutamine. SPECT images were acquired 45-60 min after the Tc-99m sestamibi injection using a rotating gamma camera with a low-energy, all-purpose collimator. Processing and reconstruction were performed using standard back-projection algorithms and a Ramp-Hanning filter. Gated SPECT left ventricular ejection fraction was measured using QGS software (Cedars-Sinai Medical Center, Los Angeles, California)13. Attenuation correction was not used. Image interpretation was performed by consensus of two experienced observers using a 16-segment short-axis model and a five-point scoring system (0 = absent uptake, 1 = severely decreased uptake, 2 = moderately decreased uptake, 3 = mildly decreased uptake, and 4 = normal uptake). The summed stress score (SSS), reflecting the extent and severity of the defect on stress images, was calculated from the 16 short-axis segments with scores inverted to the previously described scoring system of the Cedars-Sinai group14,15. SSS results were divided into 3 groups: 0-3 (low risk), 4-8 (intermediate risk), and ≥9 (high risk).
Follow-Up Data
For all patients, we determined if angiography and/or revascularization procedure [percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG)] was performed within 6 months of the stress SPECT-MPI study at Mayo Clinic Rochester. Individual patients with high-risk SSS and coronary angiography or revascularization, who underwent SPECT-MPI of either uncertain or inappropriate AUC, were reviewed on an individual basis.
Statistical Analysis
Statistical analyses were performed using computer software (SAS v9.1.3). Continuous data are summarized as mean ± standard deviation, unless otherwise stated. Categorical data are summarized as frequency and group percentage. The comparison of the categorical factors was completed using the chi-square (χ2) test for independence.
Results
Overall, 280 subjects met the inclusion criteria. Table 1 describes the baseline clinical characteristics. The mean age of study subjects was 67.3 ± 11.4 years and 36.1 % (N = 101) were females. When categorized by 2009 AUC criteria, 62.9 % (N = 176) stress SPECT-MPI studies were considered appropriate, 13.6 % (N = 38) uncertain, and 23.6 % (N = 66) inappropriate. Figure 1 displays the breakdown of our study participants by AUC, SSS, and downstream coronary angiography/ revascularization.

Breakdown of the study participants by appropriate use criteria (AUC), summed stress score (SSS), and downstream coronary angiography/revascularization [percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG)]
Relationship of Appropriateness to SPECT-MPI Results, Coronary Angiography, and Revascularization
Appropriateness category was strongly associated with SSS category. Appropriate SPECT-MPI studies were less likely to have completely normal results than uncertain or inappropriate SPECT-MPI scans [34 % (N = 59) vs. 58 % (N = 22) and 58 % (N = 38), respectively; P < 0.001]. Patients with appropriate SPECT-MPI studies were also less likely to have low risk scans (SSS 0-3) compared to patients with uncertain or inappropriate AUC [60 % (N = 105) vs. 79 % (N = 30) and 82 % (N = 54), respectively; P < 0.001]. Moreover, stress SPECT-MPI studies categorized as appropriate were more likely to have an intermediate (SSS 4-8) or high risk (SSS ≥ 9) result compared to uncertain and inappropriate studies as shown in Figure 2A [N = 71 (40 %) vs. N = 8 (21 %) and N = 12 (18 %), respectively; P = 0.008)].

Summed stress and difference scores as assessed by AUC (A) summed stress score (SSS) histogram among AUC groups shows a higher rate of intermediate (SSS: 4-8) and high risk (SSS ≥ 9) tests in the appropriate group compared to uncertain and inappropriate groups. (B) Uncertain and inappropriate tests were also associated with a higher frequency of low summed difference score (SDS) compared to patients in the appropriate group
Summed difference score (SDS) was also associated with appropriateness category. Appropriate SPECT-MPI studies were more likely to have an SDS > 0 compared to uncertain and inappropriate studies [45 % vs. 21 % and 24 %, respectively; P = 0.001] as demonstrated in Figure 2B. In addition, mean SDS (±SD) of the appropriate SPECT-MPI studies was almost twofold higher compared to the other appropriateness categories although it was not statistically significant (1.76 ± 2.99 vs. 1 ± 2.4 and 0.95 ± 2.08, respectively; P = 0.066).
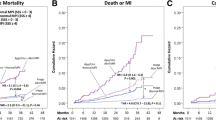
The rates of coronary angiography and subsequent revascularization were significantly associated with appropriateness category. Appropriate studies were associated with an increased rate of coronary angiography (14 %, N = 25) compared to the uncertain (0 %) or inappropriate studies (3 %, N = 2); P = 0.003 (Figure 3A). Similarly, there was an increased rate of revascularization after appropriate studies (9 %, N = 16) compared to the uncertain (0 %) or inappropriate studies (0 %); P = 0.006 (Figure 3B). When obstructive coronary artery disease is defined as being present in patients with ≥50 % stenosis in any major epicardial or branch vessel on coronary angiography, none of the patients in the inappropriate group had significant coronary artery disease (N = 2). Among 25 patients in the appropriate group who underwent coronary angiography, 11 patients (44 %) had left main or 3 vessel disease, 6 patients (24 %) had 2 vessel disease, 6 patients with single vessel disease (24 %), and only 2 patients (8 %) had no significant coronary artery disease.

Downstream coronary angiography and revascularization as assessed by AUC (A) patients in the appropriate group were more likely to undergo coronary angiography compared to patients in the uncertain and inappropriate groups. (B) Similarly, coronary revascularization with either percutaneous coronary intervention or coronary artery bypass grafting was more prevalent in patients in the appropriate group compared to the other groups
In order to address potential interaction between SSS risk category, appropriateness, and downstream catheterization/ revascularization, we first attempted to perform a logistic regression analysis but since we had very few catheterizations and no revascularization in the uncertain and inappropriate group, logistic regression was not feasible. Therefore, we aimed to visually demonstrate the interaction between SSS risk category, appropriateness group, and downstream intervention via a 3 × 3 fashion (Figure 4). This figure shows that SSS had a significant impact on downstream catheterization and revascularization after appropriate tests. On the other hand, SSS had no impact on subsequent catheterization or revascularization after uncertain or inappropriate tests bearing in mind that the overall numbers in these two groups were small. The two patients in the inappropriate group who underwent angiography both had low risk SSS, no ischemia on SPECT (SDS = 0), and only mild coronary atherosclerosis on angiography.

Interaction between summed stress score (SSS), appropriateness group, and downstream coronary angiography and revascularization each column in the above figure represents the appropriateness category (appropriate, uncertain, or inappropriate) while each row represents SSS risk category. SSS risk category had a significant impact on downstream catheterization and revascularization after appropriate tests while it had no impact on subsequent catheterization or revascularization after uncertain or inappropriate tests (P = NS). Patients with appropriate tests and high risk SSS were the most likely to subsequently undergo coronary angiography and/or revascularization
Individual Patients in the Inappropriate Group
Among the patients in the inappropriate group with high risk SPECT-MPI (N = 5), two patients underwent stress testing for 2009 ACCF/ASNC AUC indication #27 (risk assessment with known coronary artery disease, asymptomatic status, and prior stress study done <2 years ago) and the remaining three patients underwent testing for indication #59 (post-revascularization risk assessment, asymptomatic status, and less than 2 years after PCI). None of these patients underwent angiography or revascularization. Two patients in the inappropriate group with low risk SSS underwent angiography but not revascularization. One of these patients had SPECT-MPI performed for indication #24 (intermediate to high risk of coronary artery disease, normal prior stress imaging study done less than 2 years ago) and the SPECT study was again normal. However, since the patient’s exercise capacity during the test was suboptimal, he underwent angiography, which revealed minimal coronary atherosclerosis. The other patient underwent angiography after a low risk SPECT study due to occupational governmental regulations. It is noteworthy that both of these patients had only minimal coronary artery atherosclerosis and had no obstructive lesions.
Individual Patients in the Uncertain Group
Four patients in the uncertain group had high risk SPECT-MPI tests. Two of these patients underwent testing for indication #60 (post-revascularization risk assessment, asymptomatic status, and ≥2 years after PCI). One patient had a stress test for indication #57 (post-revascularization risk assessment, asymptomatic status, and <5 years after CABG) while the other patient was tested for indication #28 (risk assessment with known coronary artery disease, asymptomatic status, and prior stress study done ≥2 years ago). None of these four patients had subsequent angiography or revascularization.
Discussion
Our results show that SPECT-MPI appropriateness category is strongly associated with the severity of SSS, SDS, and subsequent patient management. Appropriate stress SPECT-MPI studies are more likely to have an intermediate/high risk SSS and SDS > 0 than uncertain or inappropriate studies. Appropriate stress SPECT-MPI studies are also more likely to lead to subsequent revascularization than uncertain or inappropriate studies. Only two patients who underwent SPECT-MPI for inappropriate indications had subsequent angiography with no significant coronary artery disease. None of the patients in the uncertain or inappropriate groups underwent coronary revascularization.
Several studies have previously described the frequency of appropriateness of stress SPECT-MPI studies performed in the clinical setting6,7,9,16. Mehta et al8 described the distribution of abnormal stress SPECT-MPI results according to AUC. In that study, 45 % of appropriate, 68 % of inappropriate, and 53 % of uncertain stress SPECT-MPI studies were normal. Thirty-two percent of the inappropriate stress SPECT-MPI studies were abnormal with a mean summed stress score (SSS) of 1.49. Askew et al17 also demonstrated that routine CAD screening for asymptomatic patients with atrial fibrillation (AUC indication #17, uncertain) yielded imaging findings that were no different than in age- and gender-matched patients without atrial fibrillation. However, no data was provided on the downstream clinical consequences of the abnormal stress SPECT-MPI studies.
Our study is the first to describe both the stress SPECT-MPI study results and the downstream clinical consequences with regard to subsequent angiography and revascularization. Appropriate studies were more likely to be followed by coronary revascularization when compared to uncertain or inappropriate studies. Another interesting finding in our study was that characteristics of stress SPECT-MPI studies classified as uncertain were very similar to those classified as inappropriate. Among patients in the uncertain appropriateness group 58 % (N = 22) had normal studies while 79 % (N = 30) had low risk SSS compared to 58 % (N = 38) normal studies and 82 % (N = 54) low risk SPECT-MPI studies in the inappropriate group. This suggests that uncertain and inappropriate studies rarely detect high risk CAD. Furthermore, very few inappropriate studies resulted in coronary angiography and no patients underwent revascularization as a result of an inappropriate stress SPECT-MPI study. These findings should reassure clinicians that inappropriate studies have a low diagnostic yield and will not significantly alter the management of the patient in most cases.
The rate of inappropriate studies reported in our manuscript (24 %) is higher than older studies that utilized the 2005 AUC rather than the 2009 AUC. Lower rates of inappropriate studies were reported using the 2005 AUC including Mehta et al (13 %)8, Hendel et al (14.4 %)16, and Gibbons et al (14 %)6. The 2009 AUC are considered more comprehensive compared to the 2005 AUC. We have reported that they eliminate the “unclassified” category and increase inappropriate and uncertain studies7. Nelson et al recently assessed SPECT appropriateness at the Miami VA Medical Center and University of Miami Hospital using the 2009 AUC and demonstrated that inappropriate studies constituted 22 % of tests performed at the Miami VA Medical Center and 16.6 % at the University of Miami Hospital (P = 0.24). The rate of inappropriate studies that we report is closer to the results of this recent study18.
Some patients in the uncertain and inappropriate groups had high or intermediate risk SPECT-MPI results. However, all of these patients had known coronary artery disease, and were expected to have abnormal test results. In our study, none of the patients in the uncertain and inappropriate groups with intermediate and high risk SSS underwent coronary revascularization. Thus, even these clearly abnormal studies did not appear to alter clinical management.
In the appropriate group, of the 37 patients with high-risk scans, only 12, or about one-third, underwent coronary angiography. Of the patients who underwent angiography, only one-half underwent revascularization. This finding is similar to previous studies from both Cedars-Sinai Medical Center and Mayo Clinic, indicating that a minority of patients with high-risk scans undergo angiography19,20. At the other end of the spectrum, 8 of the 105 patients with low-risk scans underwent coronary angiography, and 5 of these underwent revascularization.
Limitations
There are several limitations to our study. This study was performed at a single tertiary academic medical center and the sample size is limited due to the effort required in our institution to accurately classify the appropriateness of all studies. Our methodology employs database and chart review by personnel who are not involved in ordering or performing the test, and are therefore independent of the clinical process. The assumptions made to apply the criteria may not be accepted by others. We did not assess the appropriateness of the revascularization that occurred on the basis of the stress SPECT-MPI studies. Incomplete documentation may explain some of the inappropriate studies. Further, the sample size of this study did not provide sufficient power to detect differences in hard cardiac events based on appropriateness categories.
The data presented in this study only compare different categories of appropriateness with respect to coronary angiography and revascularization. Alternative definitions of appropriateness might increase the value of perfusion imaging. Given the small number of patients who underwent revascularization in this cohort, much larger cohorts would be required to address this issue. Given the intensive and time-consuming process of appropriateness allocation described earlier, we were not able to evaluate newer or larger cohorts in this study.
New Knowledge Gained
Appropriate stress SPECT-MPI studies are more likely to result in abnormal results requiring subsequent revascularization compared to uncertain or inappropriate studies. Inappropriate and uncertain SPECT-MPI studies did not lead to revascularization, affirming the AUC.
Conclusion
Appropriate stress SPECT-MPI studies are more likely to result in abnormal results requiring subsequent revascularization compared to uncertain or inappropriate studies. Inappropriate stress SPECT-MPI studies rarely change the clinical management of the patient, affirming the AUC recommendations. More importantly, our study demonstrates that uncertain stress SPECT-MPI studies are also less likely to be associated with high risk SSS or downstream angiography and coronary revascularization.
References
Lucas FL, DeLorenzo MA, Siewers AE, Wennberg DE. Temporal trends in the utilization of diagnostic testing and treatments for cardiovascular disease in the United States, 1993-2001. Circulation. 2006;113:374-9.
Levin DC, Rao VM, Parker L, Frangos AJ, Intenzo CM. Recent payment and utilization trends in radionuclide myocardial perfusion imaging: comparison between self-referral and referral to radiologists. J Am Coll Radiol. 2009;6:437-41.
Brindis RG, Douglas PS, Hendel RC, Peterson ED, Wolk MJ, Allen JM, Patel MR, Raskin IE, Bateman TM, Cerqueira MD, Gibbons RJ, Gillam LD, Gillespie JA, Iskandrian AE, Jerome SD, Krumholz HM, Messer JV, Spertus JA, Stowers SA. Accf/asnc appropriateness criteria for single-photon emission computed tomography myocardial perfusion imaging (spect mpi): A report of the American college of cardiology foundation quality strategic directions committee appropriateness criteria working group and the American society of nuclear cardiology endorsed by the American heart association. J Am Coll Cardiol. 2005;46:1587-605.
Hendel RC, Berman DS, Di Carli MF, Heidenreich PA, Henkin RE, Pellikka PA, Pohost GM, Williams KA. Accf/asnc/acr/aha/ase/scct/scmr/snm 2009 appropriate use criteria for cardiac radionuclide imaging: A report of the american college of cardiology foundation appropriate use criteria task force, the american society of nuclear cardiology, the american college of radiology, the american heart association, the american society of echocardiography, the society of cardiovascular computed tomography, the society for cardiovascular magnetic resonance, and the society of nuclear medicine. Circulation. 2009;119:e561-87.
Shaw LJ, Marwick TH, Zoghbi WA, Hundley WG, Kramer CM, Achenbach S, Dilsizian V, Kern MJ, Chandrashekhar Y, Narula J. Why all the focus on cardiac imaging? JACC Cardiovasc Imaging. 2010;3:789-94.
Gibbons RJ, Miller TD, Hodge D, Urban L, Araoz PA, Pellikka P, McCully RB. Application of appropriateness criteria to stress single-photon emission computed tomography sestamibi studies and stress echocardiograms in an academic medical center. J Am Coll Cardiol. 2008;51:1283-9.
Carryer DJ, Hodge DO, Miller TD, Askew JW, Gibbons RJ. Application of appropriateness criteria to stress single photon emission computed tomography sestamibi studies: A comparison of the 2009 revised appropriateness criteria to the 2005 original criteria. Am Heart J. 2010;160:244-9.
Mehta R, Ward RP, Chandra S, Agarwal R, Williams KA. Evaluation of the American college of cardiology foundation/american society of nuclear cardiology appropriateness criteria for spect myocardial perfusion imaging. J Nucl Cardiol. 2008;15:337-44.
Koh AS, Flores JL, Keng FY, Tan RS, Chua TS. Evaluation of the American college of cardiology foundation/american society of nuclear cardiology appropriateness criteria for spect myocardial perfusion imaging in an Asian tertiary cardiac center. J Nucl Cardiol. 2011;18:324-30.
Diamond GA. A clinically relevant classification of chest discomfort. J Am Coll Cardiol. 1983;1:574-5.
Sorajja P, Chareonthaitawee P, Rajagopalan N, Miller TD, Frye RL, Hodge DO, Gibbons RJ. Improved survival in asymptomatic diabetic patients with high-risk spect imaging treated with coronary artery bypass grafting. Circulation. 2005;112:I311-6.
Kane GC, Hauser MF, Behrenbeck TR, Miller TD, Gibbons RJ, Christian TF. Impact of gender on rest tc-99m sestamibi-gated left ventricular ejection fraction. Am J Cardiol. 2002;89:1238-41.
Germano G, Kiat H, Kavanagh PB, Moriel M, Mazzanti M, Su HT, Van Train KF, Berman DS. Automatic quantification of ejection fraction from gated myocardial perfusion spect. J Nucl Med. 1995;36:2138-47.
Hachamovitch R, Berman DS, Kiat H, Cohen I, Cabico JA, Friedman J, Diamond GA. Exercise myocardial perfusion spect in patients without known coronary artery disease: incremental prognostic value and use in risk stratification. Circulation. 1996;93:905-14.
Miller TD, Christian TF, Clements IP, Hodge DO, Gray DT, Gibbons RJ. Prognostic value of exercise thallium-201 imaging in a community population. Am Heart J. 1998;135:663-70.
Hendel RC, Cerqueira M, Douglas PS, Caruth KC, Allen JM, Jensen NC, Pan W, Brindis R, Wolk M. A multicenter assessment of the use of single-photon emission computed tomography myocardial perfusion imaging with appropriateness criteria. J Am Coll Cardiol. 2010;55:156-62.
Askew JW, Miller TD, Hodge DO, Gibbons RJ. The value of myocardial perfusion single-photon emission computed tomography in screening asymptomatic patients with atrial fibrillation for coronary artery disease. J Am Coll Cardiol. 2007;50:1080-5.
Nelson KH, Willens HJ, Hendel RC. Utilization of radionuclide myocardial perfusion imaging in two health care systems: assessment with the 2009 accf/asnc/aha appropriateness use criteria. J Nucl Cardiol. 2012;19:37-42.
Miller TD, Roger VL, Hodge DO, Hopfenspirger MR, Bailey KR, Gibbons RJ. Gender differences and temporal trends in clinical characteristics, stress test results and use of invasive procedures in patients undergoing evaluation for coronary artery disease. J Am Coll Cardiol. 2001;38:690-7.
Hachamovitch R, Berman DS, Kiat H, Bairey-Merz N, Cohen I, Cabico JA, Friedman JD, Germano G, Van Train KF, Diamond GA. Gender-related differences in clinical management after exercise nuclear testing. J Am Coll Cardiol. 1995;26:1457-64.
Disclosures
Dr. Todd D. Miller has consulting agreements with Astellas Pharma and Lantheus Medical Imaging. Dr. Miller receives research funds from Forest Research Institute. Dr. Raymond J. Gibbons serves as a consultant to Lantheus Medical Imaging. All other authors report that they have no relationships to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Khawaja, F.J., Jouni, H., Miller, T.D. et al. Downstream clinical implications of abnormal myocardial perfusion single-photon emission computed tomography based on appropriate use criteria. J. Nucl. Cardiol. 20, 1041–1048 (2013). https://doi.org/10.1007/s12350-013-9794-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-013-9794-z