
Abstract
Background
For a 1-day myocardial perfusion SPECT (MPS) the recommendations for administered activity stated in the EANM guidelines results in an effective dose of up to 16 mSv per patient. Recently, a gamma camera system, based on cadmium zinc telluride (CZT) technology, was introduced. This technique has the potential to reduce the effective dose and scan time compared to the conventional NaI gamma camera. The aim of this study was to investigate if the effective dose can be reduced with a preserved image quality using CZT technology in MPS.
Methods
In total, 150 patients were included in the study. All underwent a 1-day 99mTc-tetrofosmin stress-rest protocol and were divided into three subgroups (n = 50 in each group) with 4, 3, and 2.5 MBq/kg body weight of administered activity in the stress examination, respectively. The acquisition time was increased in proportion to the decrease in administered activity. All examinations were analyzed for image quality by visual grading on a 4-point scale (1 = poor, 2 = adequate, 3 = good, 4 = excellent), by two expert readers.
Results
The total effective dose (stress + rest) decreased from 9.3 to 5.8 mSv comparing 4 to 2.5 MBq/kg body weight. For the patients undergoing stress examination only (35%) the effective dose, administrating 2.5 MBq/kg, was 1.4 mSv. The image acquisition times for 2.5 MBq/kg body weight were 475 and 300 seconds (stress and rest) compared to 900 seconds for each when using conventional MPS. The average image quality was 3.7 ± 0.5, 3.8 ± 0.5, and 3.8 ± 0.4 for the stress images and 3.5 ± 0.6, 3.6 ± 0.6, and 3.5 ± 0.6 for the rest images and showed no statistically significant difference (P = .62) among the 4, 3, and 2.5 MBq/kg groups.
Conclusions
The new CZT technology can be used to considerably decrease the effective dose and acquisition time for MPS with preserved high image quality.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Myocardial perfusion single photon emission computed tomography (MPS) is an established non-invasive imaging technique for detection of myocardial perfusion defects. The conventional technology with a NaI-crystal was introduced more than 50 years ago and is the most widely used nuclear medicine imaging technique. Conventional MPS is associated with time-consuming image acquisition and a relatively high administered activity is required to enable adequate image quality.
Recently, a new generation of gamma camera systems was introduced based on a novel detector technology utilizing semiconductor detectors of cadmium zinc telluride (CZT).1,2 This technology is associated with higher sensitivity and better spatial and energy resolution compared to conventional MPS and its agreement with conventional MPS using a NaI-crystal technology has been clinically validated in several studies.3-7 Furthermore, the CZT camera system enables complete 3D coverage and simultaneous image acquisition of the heart using a stationary gantry with 19 pinhole collimators. Therefore, the CZT system allows for a significant reduction of acquisition times compared to conventional systems and have shown the potential for high patient throughput. Previous studies have reported a decrease of scan time from approximately 15 down to a few minutes1,4,6 with the administered activity recommended in guidelines.8-10 For a 1-day MPS the activity recommendations in the guidelines will result in an effective dose of up to 16 mSv per patient. Thus, MPS is one of the procedures in diagnostic nuclear medicine that gives the highest effective dose contribution.11,12 Instead of using the advantages with the CZT camera systems to perform fast myocardial perfusion imaging,3,5-7 this technology could be used to reduce the administered activity to decrease the effective dose to the patient. One previous study 13 indicates that reduced activity could be used but further validation is needed.
The aim of this study was therefore to investigate if the administered activity can be reduced with preserved image quality using the new CZT technology.
Methods
Study Design
The study group comprised 150 consecutive patients referred for MPS due to known or suspected coronary artery disease. All patients underwent a 1-day 99mTc-tetrofosmin stress protocol according to clinically established protocols. Exclusion criteria were a patient weight more than 100 kg, patients undergoing a 2-day protocol and patients undergoing the rest examination before the stress examination.
The patients were consecutively included into three different subgroups. The first 50 patients were injected with 4 MBq/kg, the following 50 patients with 3 MBq/kg, and the last 50 patients with 2.5 MBq/kg body weight of 99mTc-tetrofosmin at stress (exercise or pharmacologic) according to clinically established protocols. Imaging was performed with a CZT camera (Discovery NM 530c, GE Healthcare) approximately 1 hour after injection at stress. The rest examination was undertaken according to a predefined, in-house developed time schedule designed to meet the ASNC recommended guidelines. Thus, individually adjusted activity was administered at rest depending on the duration between the two examinations, with a minimum of 2 hour, resulting in decreased activity with increased duration. The rest examination was only performed if the stress examination images were interpreted as abnormal.
All patients provided written informed consent to participate in the study and the study was approved by the regional ethics committee.
Acquisition and Reconstruction
The Discovery NM 530c equipment consists of 19 stationary CZT detectors simultaneously imaging 19 views of the heart. Each CZT detector contains 32 × 32 pixel elements (2.46 × 2.46 mm) and is equipped with pinhole collimators made of tungsten focusing on the heart. The CZT semiconductor detector operates at room temperature. The compact system design allows acquisition without any detector motion as the detectors are aligned around the patient and all 19 projections of the heart are acquired simultaneously.
Performance assessment of the Discovery NM 530c camera shows a linear count rate response below 800 MBq of 99mTc. Acquisition after stress with injection of 4 MBq/kg body weight was made with a scan time of 300 seconds based on the study by Herzog et al.6 When the injected activity was decreased to 3 and 2.5 MBq/kg body weight, the acquisition time was increased linearly to compensate for a count loss due to the decreased activity to keep the number of counts in the image constant. Patients were imaged in supine position with the arms positioned over the head. A 15% symmetrical energy window at 140 keV was used. Electrocardiogram-gated scans were acquired using 8 bins. No correction for scatter or attenuation was performed.
For the rest examinations, up to three times higher activity of 99mTc-tetrofosmin was injected depending on the time interval between injection at stress and rest. Image acquisition at rest was made with the same protocol as at stress but with a decreased image acquisition time. For the 4 MBq/kg body weight group an acquisition time of 180 seconds, as recommended from GE Healthcare based on the study by Herzog et al,6 was used. For the patient groups with injected activities of 3 and 2.5 MBq/kg at stress, the acquisition time was increased linearly. The syringe was measured before and after injection of 99mTc-tetrofosmin to calculate the administered activity.
Penalized maximum likelihood iterative reconstruction adapted to the Discovery NM 530c three-dimensional geometry was used to create transaxial images of the left ventricle. For the gated images, 30 iterations with an alpha of 0.4 and a beta of 0.4 was used for both stress and rest investigations and the images were post-filtered with a Butterworth filter with cut-off frequency of 0.4 and power 10. For the non-gated images, 40 and 50 iterations with an alpha parameter of 0.51 and 0.41 and a beta of 0.3 and 0.2 were used for the stress and rest studies, respectively. The non-gated images were post-filtered with a Butterworth filter with a cut-off frequency of 0.37 and a power of 7. All reconstruction parameters used followed the recommendations from the manufacturer. The images were reconstructed on a dedicated workstation (GE Healthcare). All images were reconstructed in the standard axes (short axis, vertical long axis, horizontal long axis) and polar maps of the left ventricle were created.
Quantitative Analysis
The total number of counts collected in the study was calculated for all patients by multiplying the detector counts by the scale factor of the value derived from the DICOM information of the study.
Image Analysis
The software package Quantitative Gated SPECT (QGS) (version 4.0, Cedars Sinai Medical Centre, Los Angeles, CA) was used for image analysis. All examinations were analyzed in a randomized sequence by two expert readers (HE and JJ), both with approximately 10 years of experience with MPS. The observers were blinded to information of scan time, injected activity, and patient data as well as to each other. The image quality was visually graded on a 4-point scale (1 = poor, 2 = adequate, 3 = good, 4 = excellent). When grading the images for image quality the following variables were considered: rotating raw data projection, noise level, the homogeneity of the uptake as seen on both the tomographic short- and the long-axis slices and on the polar plot representation. The gated images were graded as either diagnostic or non-diagnostic based on uptake homogeneity and the ability to estimate wall thickening. After the evaluation of all this available information, the observer appointed a grade based on the confidence level for stating normal findings, fixed perfusion defect, or stress-induced ischemia. In the cases where there was a disagreement with regards to diagnosis, consensus reading was undertaken.
Dosimetry
The effective dose was determined based on data in the ICRP publication 106.14 The mean weight (79 kg in all groups) and the mean administered activity were used for the calculation of the effective dose for rest and stress. For comparison, the effective dose was also calculated based on the EANM recommendations on administered activity for MPS.8,9
Statistical Analysis
The data are presented as mean ± SD. Statistical analysis was performed using IBM SPSS Statistics v.20.0 (Chicago, Illinois, USA). ANOVA was used to compare continuous variables and a χ2 test was used to compare categorical variables. The inter-observer agreement for image quality was expressed as mean difference ± SD. For assessment of inter-observer agreement rate for the presence of perfusion defects on a per-patient basis prior to consensus reading, Kappa statistics was used. Statistical significance was defined as P < .05.
Results
Patient characteristics and MPS study results are shown in Table 1. All 150 patients successfully underwent stress examination with mean activity of 318, 238, and 203 MBq at stress for the 4, 3, and 2.5 MBq/kg protocols, respectively (Table 2). Examination at rest was performed in 97 patients (65%) based on the interpretation of the stress images. The mean duration between stress and rest activity administration was 3.5 ± 1.1 hour resulting in a mean administered activity for the rest examination of 892, 636, and 547 MBq for the 4, 3, and 2.5 MBq/kg protocols, respectively (Table 2). Scan time duration was 300, 400, and 475 seconds for the stress examination and 180, 240, and 285 seconds for the rest examination for the 4, 3, and 2.5 MBq/kg protocols, respectively.
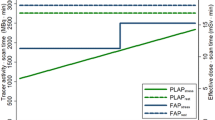
The mean value of the total number of counts in the images for each study group was similar, with 1168000 ± 251000, 1124000 ± 310000, 1130000 ± 268000 counts for the stress examinations and 2144000 ± 418000, 2039000 ± 480000, 2211000 ± 501000 counts for the rest examinations for the 4, 3, and 2.5 MBq/kg group, respectively. No statistically significant difference could be seen between the groups (P = .46 stress, P = .45 rest) (Figure 1). Taken into account that the image acquisition time for the stress examination was 1.7 times that of the rest examination and the decay of the administered activity for the stress examination, the mean ratio between rest and stress activity was 3.9 ± 0.3 at the time of the rest acquisition.

Number of total counts in the stress and rest images ± the standard error of the mean versus administered activity for the three activity groups. The number of patients that underwent stress examination is 50 in each group, for rest examination the number of patients is 32, 32, and 35 for the 4, 3, and 2.5 MBq/kg groups, respectively
Typical image quality of one patient study from each activity group is shown in Figure 2. The image quality on the 4-point scale for both expert readers was 3.7 ± 0.5, 3.8 ± 0.5, and 3.8 ± 0.4 for the stress images and 3.5 ± 0.6, 3.6 ± 0.6, and 3.5 ± 0.6 for the rest images for the 4, 3, and 2.5 MBq/kg group, respectively. There was no significant difference in image quality between the three groups (P = .62). The inter-observer variability between the two expert readers on the 4-point scale was 0.04 ± 0.5. In no cases, the difference between the observers exceeded 1 point. The three activity groups, 97%, 96%, and 98%, of the studies, respectively, were graded as “good” or “excellent” by the expert readers (Table 3). None of the studies had an image quality graded as “poor”. For the gated studies, two studies in the 2.5 MBq/kg group was interpreted as non-diagnostic by both expert readers. In the 3 MBq/kg group and the 4 MBq/kg group, all gated studies were interpreted as diagnostic. The inter-observer agreement rate for the presence of perfusion defects (fixed or stress-induced) on a per-patient basis was 94% with a Kappa value of 0.87.

Perfusion images, with typical image quality, showing normal perfused myocardium of one patient from each activity group examined with a 1-day 99mTc-tetrofosmin protocol at stress and rest. Images are shown as short axis (SA), vertical long axis (VLA), and horizontal long axis (HLA)
The total effective dose (stress and rest) decreased from 9.3 mSv in the 4 MBq/kg group to 5.8 mSv in the 2.5 MBq/kg group (Table 4).
Discussion
This study shows that it is possible to perform MPS with the new CZT technology with both a significantly reduced effective dose and a shorter scan time with a preserved image quality as compared to conventional MPS technology and the EANM guidelines.
There was no statistically significant difference in image quality between the three activity groups. Also, the image quality was graded as “good” or “excellent” in the vast majority of the studies by both expert readers. These results are consistent with those shown by Duvall et al,13 confirming that high image quality can be obtained also with low administered activity. Even though the two expert readers performed the image quality grading separately and the scale used is subjective, the inter-observer variability was low.
The number of counts in an examination is linear to the acquisition time. Therefore, the acquisition time was prolonged proportional to the amount of administered activity in the three activity groups, respectively. The mean total number of counts in the examinations did not differ between the three activity groups, which probably explains why there was no difference in image quality between the three groups. A proportional prolonged acquisition time can be used to receive an adequate examination in the case of low administered activity, e.g., due to high residual activity in the syringe. In three patients, examined after the study of the 150 patients was concluded, measurement of the syringe after activity injection showed that too low amounts of activity had been administered to the patients at stress—1.5, 1.6, and 1.7 MBq/kg body weight, respectively. In these cases, the acquisition time was therefore prolonged proportional to the low administered activity to obtain the same amount of total counts in the images as if the administered activity had been normal. The image quality was considered good and diagnostic in all three cases and the total number of counts was equal to the number of counts in an examination with normal amount of administered activity (Figure 3).

Perfusion images at stress of three patients administered with a low amount of activity at stress due to residual activity in the syringe. The administered activity was 1.5, 1.6, and 1.7 MBq/kg body weight, respectively, and the acquisition time was therefore prolonged in proportion to the reduced activity. Images are shown as short axis (SA), vertical long axis (VLA), and horizontal long axis (HLA)
Compared to conventional MPS technology, the acquisition time was decreased from approximately 900 seconds for rest and stress examination, respectively, down to approximately 300 and 475 seconds for rest and stress examination, respectively. The advantages with a decreased acquisition time are shorter time for the patients in the camera and a possibility for an increased patient throughput. In addition, the risk for patient motion during acquisition decreases with a decreased acquisition time. A large decrease of the administered activity and a proportional increase of acquisition time increase the risk for motion artifacts since the Discovery NM 530c has, at this date, no possibility to correct for patient motion.
In this study, the total effective dose was decreased from 9.3 to 5.8 mSv when the administered activity was reduced from 4 to 2.5 MBq/kg body weight at stress. An effective dose of 5.8 mSv for a 79 kg patient means a dose reduction of 63% compared to the 15.7 mSv recommended by the EANM guidelines. A total effective dose of 5.8 mSv is consistent with the effective dose shown by Duvall et al.13
Millions of MPS studies are performed each year worldwide. Reducing the administered activity to this patient group will result in a decreased collective dose and consequently a decreased risk associated with ionizing radiation exposure for this group of patients. This study clarifies the possibility to decrease the administrated activity down to 2.5 MBq/kg body weight with high clinical image quality. Previously published recommendations from ASNC aim to decrease the effective dose for MPS to 9 mSv in the year 2014.15 Nine mSv (9 mSv) corresponds to the initial effective dose in this study before activity reduction. Decreased administered activity is not only beneficial for the patient but it is also advantageous for the staff working with the patient. Exposure to radioactivity in this range adds a very small risk for stochastic effects of radiation. However, hypothetically there is no threshold for the occurrence of cancer or genetic effects based on the probability for chromosomal damage. Therefore, it is of importance to reduce the administered activity as much as possible, following the principle of As Low As Reasonably Achievable (ALARA).16
Several different methods could be used to decrease the administered activity and effective dose. Starting the MPS protocol with examination at stress and analyzing the stress images before deciding of the need for rest examination reduce the effective dose. In this study, myocardial perfusion defects could be excluded in 35% (53/150) of the cases after stress imaging. In the case of a 1-day protocol, the majority of the total effective dose comes from the second examination. In this study, 75% of the total effective dose was received from the second examination. The effective dose for a patient undergoing stress examination only was 1.4 mSv. The use of a 2-day protocol is another means to decrease the effective dose to the patient. A lower amount of activity can be administered for the second examination using a 2-day protocol (due to the decay of 99mTc), compared to using a 1-day protocol. Thus, the administered activity in the second examination can be decreased approximately by a factor of 3. Consequently, an MPS study including both stress and rest examinations can be performed with an effective dose of 3.6 mSv for a 79 kg patient if a 2-day protocol is applied. A decrease in the injected activity also enables MPS to be performed during times of limited 99mTc availability.
Conclusions
The effective radiation dose and the acquisition time can be considerably decreased with preserved high image quality when MPS is performed with the novel CZT technology. A stress and rest examination, using a 1-day protocol, can be performed with an effective dose of 37% compared to the dose recommended in international guidelines.
References
Bocher M, Blevis IM, Tsukerman L, Shrem Y, Kovalski G, Volokh L. A fast cardiac gamma camera with dynamic SPECT capabilities: Design, system validation and future potential. Eur J Nucl Med Mol Imaging 2010;37:1887-902. doi:10.1007/s00259-010-1488-z.
Gambhir SS, Berman DS, Ziffer J, Nagler M, Sandler M, Patton J, et al. A novel high-sensitivity rapid-acquisition single-photon cardiac imaging camera. J Nucl Med 2009;50:635-43. doi:10.2967/jnumed.108.060020.
Berman DS, Kang X, Tamarappoo B, Wolak A, Hayes SW, Nakazato R, et al. Stress thallium-201/rest technetium-99m sequential dual isotope high-speed myocardial perfusion imaging. JACC Cardiovasc Imaging 2009;2:273-82. doi:10.1016/j.jcmg.2008.12.012.
Buechel RR, Herzog BA, Husmann L, Burger IA, Pazhenkottil AP, Treyer V, et al. Ultrafast nuclear myocardial perfusion imaging on a new gamma camera with semiconductor detector technique: First clinical validation. Eur J Nucl Med Mol Imaging 2010;37:773-8. doi:10.1007/s00259-009-1375-7.
Esteves FPRP, Folks RD, Keidar Z, Askew JW, Rispler S, O’Connor MK, et al. Novel solid-state-detector dedicated cardiac camera for fast myocardial perfusion imaging: Multicenter comparison with standard dual detector cameras. J Nucl Cardiol 2009;16:927-34.
Herzog BA, Buechel RR, Katz R, Brueckner M, Husmann L, Burger IA, et al. Nuclear myocardial perfusion imaging with a cadmium-zinc-telluride detector technique: Optimized protocol for scan time reduction. J Nucl Med 2010;51:46-51. doi:10.2967/jnumed.109.065532.
Sharir T, Ben-Haim S, Merzon K, Prochorov V, Dickman D, Berman DS. High-speed myocardial perfusion imaging initial clinical comparison with conventional dual detector anger camera imaging. JACC Cardiovasc Imaging 2008;1:156-63. doi:10.1016/j.jcmg.2007.12.004.
Hesse B, Lindhardt TB, Acampa W, Anagnostopoulos C, Ballinger J, Bax JJ, et al. EANM/ESC guidelines for radionuclide imaging of cardiac function. Eur J Nucl Med Mol Imaging 2008;35:851-85. doi:10.1007/s00259-007-0694-9.
Hesse B, Tagil K, Cuocolo A, Anagnostopoulos C, Bardies M, Bax J, et al. EANM/ESC procedural guidelines for myocardial perfusion imaging in nuclear cardiology. Eur J Nucl Med Mol Imaging 2005;32:855-97. doi:10.1007/s00259-005-1779-y.
Holly TA, Abbott BG, Al-Mallah M, Calnon DA, Cohen MC, DiFilippo FP, et al. Single photon-emission computed tomography. J Nucl Cardiol 2010;17:941-73. doi:10.1007/s12350-010-9246-y.
Gerber TC, Gibbons RJ. Weighing the risks and benefits of cardiac imaging with ionizing radiation. JACC Cardiovasc Imaging 2010;3:528-35. doi:10.1016/j.jcmg.2010.03.003.
Eisenberg MJ, Afilalo J, Lawler PR, Abrahamowicz M, Richard H, Pilote L. Cancer risk related to low-dose ionizing radiation from cardiac imaging in patients after acute myocardial infarction. CMAJ 2011;183:430-6. doi:10.1503/cmaj.100463.
Duvall WL, Croft LB, Ginsberg ES, Einstein AJ, Guma KA, George T, et al. Reduced isotope dose and imaging time with a high-efficiency CZT SPECT camera. J Nucl Cardiol 2011;18:847-57. doi:10.1007/s12350-011-9379-7.
ICRP Publication 106: Radiation dose to patients from radiopharmaceuticals (Addendum 3 to ICRP publication 53). Ann ICRP 2008;38:1-197.
Cerqueira MD, Allman KC, Ficaro EP, Hansen CL, Nichols KJ, Thompson RC, et al. Recommendations for reducing radiation exposure in myocardial perfusion imaging. J Nucl Cardiol 2010;17:709-18. doi:10.1007/s12350-010-9244-0.
ICRP Publication 105. Radiation protection in medicine. Ann ICRP 2007;37:1-63. doi:10.1016/j.icrp.2008.08.001.
Acknowledgments
The authors would like to thank Christel Kullberg for excellent technical assistance. This study was supported in part by research funding from Region of Scania, Swedish Research Council, Swedish Heart and Lung Foundation, and Lund University Faculty of Medicine.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Oddstig, J., Hedeer, F., Jögi, J. et al. Reduced administered activity, reduced acquisition time, and preserved image quality for the new CZT camera. J. Nucl. Cardiol. 20, 38–44 (2013). https://doi.org/10.1007/s12350-012-9634-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-012-9634-6