
Abstract
Background
Regadenoson is a coronary vasodilator that causes tachycardia via activation of the sympathetic nervous system. We determined whether β1-adrenergic blockade can attenuate tachycardia without significantly reducing coronary vasodilation induced by regadenoson.
Methods and Results
Hemodynamics and coronary blood flow (CBF) were measured in conscious dogs. Baseline CBF and heart rate (HR) were 42 ± 2 mL/min and 87 ± 8 bpm (mean ± SEM), respectively. Regadenoson (1, 2.5, and 5 μg/kg) increased peak CBF by 129 ± 10, 149 ± 7, and 174 ± 10 mL/min and HR by 48 ± 6, 67 ± 5, and 85 ± 11 bpm, respectively, (all P < .05 vs baseline). In the presence of metoprolol (1.5 mg/kg), the peak increases in CBF caused by these three doses of regadenoson were reduced by only 11 ± 7%, 10 ± 4%, and 21 ± 2% (P = NS, <.05, and <.05 vs regadenoson alone), respectively, whereas the regadenoson-induced tachycardia was significantly reduced by 55 ± 8%, 55 ± 4%, and 52 ± 5% (all P < .05). In the presence of metoprolol, the duration of the regadenoson-induced increase in CBF was reduced, but the duration of the 2-fold increase in CBF caused by 5 μg/kg regadenoson was still nearly 6 minutes.
Conclusion
β1-Adrenergic blockade with metoprolol attenuated the regadenoson-induced increase in HR more than the increase in CBF.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Regadenoson is an A2A adenosine receptor agonist that was approved by the US FDA in 2008 for use as a coronary vasodilator in pharmacologic stress testing for radionuclide myocardial perfusion imaging (MPI) using single-photon emission computed tomography (SPECT).1-3 Results of previous studies indicate that regadenoson is a selective and potent coronary vasodilator in conscious dogs and humans.4-9 In addition to the coronary vasodilator effect, regadenoson also causes an increase in heart rate (HR) in experimental animals and humans.5-9 Previous studies have indicated that the adenosine- and regadenoson-induced increases in HR are due to direct excitation of sympathetic nerves in humans,10 awake rats,11 and conscious dogs.12 The sympathetically induced increase in HR and cardiac work may contribute to the vasodilator effects of regadenoson (and of adenosine), and β-adrenergic receptor blockers would be expected to reduce the increase of coronary blood flow (CBF) caused by the drug. The use of beta blockers may, therefore, reduce the magnitude of the vasodilator response to regadenoson during pharmacologic stress testing. Therefore, the goal of this study was to determine the effect of β1-adrenergic blockade with a therapeutic dose of metoprolol on the regadenoson-induced changes in HR, left ventricular contractility, and CBF in conscious dogs.
Methods
Chronically instrumented male mongrel dogs (n = 7) weighing 24-28 kg were used in this study. The experimental protocols were approved by the Institutional Animal Care and Use Committee of New York Medical College and conform to the Guide for the Care and Use of Laboratory Animals by the United States National Institutes of Health.
Surgical Procedures
Dogs were sedated with acepromazine (0.3 mg/kg, im) and anesthetized with pentobarbital sodium (25 mg/kg, iv). After intubation, dogs were artificially ventilated with room air. A thoracotomy was made in the fifth intercostal space using sterile techniques. Tygon catheters (Cardiovascular Instruments, Wakefield, MA) were inserted into the descending thoracic aorta and the left atrium, respectively. An ultrasound flow transducer (Transonic Systems, Ithaca, NY) was placed around the left circumflex coronary artery. A solid-state pressure gauge (P6.5, Konigsberg Instruments, Pasadena, CA) was inserted into the left ventricle through the apex. The chest was closed in layers. The catheters and wires were tunneled subcutaneously and externalized through the skin at the back of the dog’s neck. Dogs were allowed to recover from surgery for 10 to 14 days before experiments were performed and were trained to lie on a table.
Coronary Blood Flow and Hemodynamic Measurements
Phasic arterial blood pressure was measured by connecting the aortic catheter to a strain gauge transducer (P23 ID, LDS Test and Measurement, Valley View, OH). Left ventricular systolic pressure (LVSP) was measured using a solid-state pressure gauge. CBF (mL/min) was measured from an ultrasound flow transducer using a Transonic flowmeter (T402, Transonic Systems, Ithaca, NY). Two indices were used to describe the regadenoson-induced coronary vasodilation: (1) the peak increase in CBF and (2) the duration of the 2-fold increase in CBF (the period of time that CBF was above a level ≥2-fold of baseline CBF). All measured parameters were acquired and analyzed using a Ponemah System (Version 4.90, DSI, Valley View, OH). Mean arterial pressure (MAP) and HR were calculated from phasic blood pressure data, and the maximum positive value of the first derivative of left ventricular pressure with time (LV + dP/dt) was calculated from LVSP. Mean coronary vascular resistance (MCVR) was calculated as CBF divided by MAP.
Experimental Protocols
On an experimental day, a dog was brought to the lab and placed on a table on its right side, where it laid quietly throughout the experiment. A catheter was inserted into a peripheral vein in the leg and attached to an infusion line to administer drugs without disturbing the animal. The experiment was begun after LVSP, MAP, HR, and CBF were stable, usually 20 to 30 minutes after connecting all recoding equipment.
Regadenoson (1, 2.5, and 5 μg/kg) was administered as a bolus iv injection. Blood samples were taken at 1, 3, 5, 15, and 30 minutes following administration of regadenoson from a catheter implanted previously in either the left atrium or the aorta. After the response to the last dose of regadenoson had returned to baseline, metoprolol (1.5 mg/kg, iv, 1 to 2 minutes bolus infusion) was administered, followed 10 minutes later by iv injection of regadenoson at doses of 1, 2.5, or 5 μg/kg. Blood samples were again taken at 1, 3, 5, 15, and 30 minutes following administration of regadenoson, in the presence of metoprolol. The blood samples were subjected to centrifugation for 15 minutes at 3,000×g at 4 °C and the plasma was collected. Plasma concentrations of regadenoson were measured using LC-MS/MS.
Reagents
Regadenoson was supplied by Gilead Sciences Palo Alto as a sterile stock solution (Lot#: 803604, 0.08 mg/mL), in 100 nM sodium phosphate buffer containing 15% propylene glycol and 0.1% disodium edetate (pH 7.0) and was diluted in normal saline before injection. Metoprolol was purchased from Sigma-Aldrich (St. Louis, MO) and was dissolved in normal saline (10 mg/mL).
Data Analysis
The statistical significance of a difference between the value of a parameter at baseline and at any time point after drug administration was determined using a one-way repeated measures ANOVA followed by Tukey’s Test. The statistical significance of a difference between responses to regadenoson in the absence and in the presence of metoprolol was determined using a two-way repeated measures ANOVA followed by Tukey’s Test. Results with P < .05 were considered to be significant. A computer-based software package (SigmaStat 2.03) was used for statistical analysis. All data are presented as mean ± SEM.
Results
Bolus iv injections of regadenoson at 1, 2.5, and 5 μg/kg caused brief (5-20 minutes), reversible, and dose-dependent increases of CBF in conscious dogs (Figures 1, 2, 3; Table 1). The peak increases in CBF caused by 1, 2.5, and 5 μg/kg regadenoson were 3.38 ± 0.31-, 3.80 ± 0.20-, and 4.10 ± 0.29-fold over baseline, respectively (all P < .05, Figures 1, 2, 3). Regadenoson (1, 2.5, and 5 μg/kg) significantly decreased peak MCVR by 79 ± 1%, 81 ± 1%, and 83 ± 1%, respectively (all P < .05, compared to baseline) (Figure 4). The durations of the 2-fold increases in CBF (i.e., CBF ≥ 200% of baseline) caused by 1, 2.5, and 5 μg/kg regadenoson were 95 ± 15, 293 ± 43, and 564 ± 68 seconds, respectively (Figures 2, 3). The individual data for baseline CBF, peak CBF in response to regadenoson, and the time to peak response are summerized in Table 1. Administration of regadenoson caused dose-dependent increases in HR (Figures 1, 5) and LV + dP/dt (Table 2). Regadenoson at 1, 2.5, and 5 μg/kg increased HR to 138 ± 9, 155 ± 13, and 168 ± 14 bpm (all P < .05 compared to baseline) from baseline values of 90 ± 8, 88 ± 8, and 84 ± 6 bpm, respectively. Regadenoson at 1, 2.5, and 5 μg/kg increased LV + dP/dt by 620 ± 36, 1083 ± 106, and 1127 ± 141 mm Hg/s from baseline values, respectively (all P < .05). There were slight decreases in systolic and diastolic pressures (Figure 6), MAP (Table 2), and LVSP (Table 2) following injections of regadenoson. The triple product (HR × LVSP × LV +dP/dt), an indirect index of cardiac work, and double product (MAP × HR) were calculated at baseline and after regadenoson administration. After administration of 1, 2.5, and 5 μg/kg regadenoson, the triple product (Table 2) and double product (Figure 7) were significantly increased relative to baseline, respectively.

Bolus iv injection of regadenoson at doses of 1, 2.5, and 5 μg/kg caused dose-dependent increases in peak CBF (top panel) and peak HR (bottom panel). In the presence of metoprolol (1.5 mg/kg), the regadenoson-induced peak increases in CBF were slightly, but significantly, reduced. Metoprolol caused a greater reduction in tachycardia induced by regadenoson. Baseline values of CBF in all treatment groups ranged from 40 ± 3 to 44 ± 3 mL/min and baseline HR were 73 ± 4 to 90 ± 8 beats/minute. Values are mean ± SEM, n = 6-7. *P < .05, compared to baseline; # P < .05, compared to regadenoson alone; $ P < .05, compared to 1.0-μg/kg regadenoson

Bolus iv injection of regadenoson at doses of 1, 2.5, and 5 μg/kg caused a dose-dependent increase in the duration of the 2-fold increase in CBF. In the presence of metoprolol (1.5 mg/kg), the regadenoson-induced duration of the 2-fold increase in CBF was moderately but significantly reduced. Values are mean ± SEM, n = 7. *P < .05, compared to baseline; # P < .05, compared to regadenoson alone

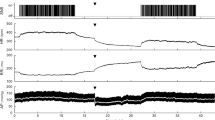
The time course of regadenoson-induced coronary vasodilation in conscious dogs in the absence and in the presence of metoprolol (1.5 mg/kg). Both the peak increase and the duration of the 2-fold increase (dashed lines) in CBF caused by regadenoson were slightly or moderately attenuated by metoprolol (1.5 mg/kg). The baseline values of CBF were from 40 to 44 mL/min in all treatment groups. Values are mean ± SEM, n = 7. *P < .05, compared to regadenoson alone

Regadenoson caused dose-independent decreases in MCVR, which were slightly but significantly attenuated by 1.5-mg/kg metoprolol at the indicated time points. Values are mean ± SEM, n = 6-7. *P < .05, compared to regadenoson alone

Regadenoson caused a dose-dependent increase in HR, which was significantly attenuated by metoprolol (1.5 mg/kg). Baseline values of HR were significantly lower after administration of metoprolol. Values are mean ± SEM, n = 6-7. *P < .05, compared to regadenoson alone

Regadenoson caused slight and mostly insignificant decreases in both systolic and diastolic blood pressures, which were not significantly altered by metoprolol (1.5 mg/kg), except at the indicated time points. Values are mean ± SEM, n = 6-7. *P < .05, compared to regadenoson alone

Regadenoson caused a dose-dependent increase in the double product (HR × MAP). The baseline values of double product were significantly reduced following administration of metoprolol (1.5 mg/kg). In the presence of metoprolol, regadenoson-induced increases in double product were significantly attenuated. Values are mean ± SEM, n = 6-7. *P < .05, compared to regadenoson alone
After the effects of regadenoson alone were recorded in each dog and values of all measured parameters had returned to baseline, metoprolol (1.5 mg/kg, iv, 1-2 minutes bolus infusion) was administered. Ten minutes after infusion of metoprolol (1.5 mg/kg), baseline HR, LV + dP/dt, double product, and triple product were significantly reduced, whereas baseline CBF, MAP, and LVSP were not markedly altered relative to control (no metoprolol) (Figures 3, 4, 5, 6, 7; Table 2).
In the presence of metoprolol (1.5 mg/kg), regadenoson caused an increase in CBF that was only slightly but significantly less than that in the absence of metoprolol (Figure 1). The duration of the 2-fold increase in CBF caused by regadenoson was also significantly shorter in the presence of metoprolol (Figures 2, 3). The peak increases in CBF caused by 1, 2.5, and 5 μg/kg regadenoson in the presence of metoprolol were 2.97 ± 0.18, 3.34 ± 0.15, and 3.43 ± 0.16-fold over baseline (41 ± 2, 43 ± 2, and 43 ± 3 mL/min), respectively. The percentage reductions in the peak increases in CBF caused by 1, 2.5, and 5 μg/kg regadenoson in the presence of metoprolol were 11 ± 7%, 10 ± 4%, and 21 ± 2%, respectively, lower than in the absence of metoprolol (P = NS, <.05, and <.05, respectively). The durations of 2-fold increases in CBF caused by 1, 2.5, and 5 μg/kg regadenoson in the presence of metoprolol were 47 ± 8, 195 ± 33, and 355 ± 32 seconds, respectively. These values indicate that 1.5 mg/kg metoprolol reduced the duration of the regadenoson-induced 2-fold increases in CBF by 47 ± 9%, 29 ± 9%, and 35 ± 4%. However, the duration of the 2-fold increase in CBF caused by 5 μg/kg regadenoson, a dose similar to that used clinically (i.e., a 400-μg bolus fixed dose), was still nearly 6 minutes in the presence of metoprolol. Regadenoson (1, 2.5, and 5 μg/kg) caused peak reductions of MCVR by 78 ± 1%, 80 ± 1%, and 81 ± 1%, respectively (Figure 4), and the magnitude of these reductions of MCVR was not altered by 1.5 mg/kg metoprolol. However, reduction of MCVR by regadenoson was slightly but significantly attenuated at various times in the presence of metoprolol (Figure 4).
Injection of regadenoson caused much smaller increases in HR (Figures 1, 5) and LV + dP/dt (Table 2) in the presence than in the absence of metoprolol. Regadenoson at 1, 2.5, and 5 μg/kg increased HR to 95 ± 5, 103 ± 6 and 111 ± 5 bpm from baseline values of 74 ± 5, 72 ± 4, and 73 ± 4 bpm, respectively. Increases in HR by regadenoson were lower by 55 ± 8%, 55 ± 4%, and 52 ± 5% in the presence than in the absence of metoprolol (all P < .05). Regadenoson at 1, 2.5, and 5 μg/kg increased LV + dP/dt by 387 ± 60, 364 ± 64, and 396 ± 32 mm Hg/s from baseline, respectively. Metoprolol (1.5 mg/kg) reduced the 1, 2.5, and 5 μg/kg regadenoson-induced increase in LV + dP/dt (peak) by 36 ± 10%, 67 ± 4%, and 63 ± 4% from control (no metoprolol), respectively (Table 2). The regadenoson-induced increase in the triple product (Table 2) and double product (Figure 7) were also significantly attenuated in the presence of metoprolol. Metoprolol reduced the 1, 2.5, and 5 μg/kg regadenoson-induced increases in the triple product (peak) by 64 ± 7%, 76 ± 4%, and 70 ± 5%, and in the double product by 31 ± 4%, 37 ± 6%, and 31 ± 4% from control (no metoprolol), respectively. On the other hand, the regadenoson-induced small and mostly insignificant decreases in systolic and diastolic blood pressures (Figure 6) and LVSP (Table 2) were not significantly altered by metoprolol.
Treatment of the dog with metoprolol (1.5 mg/kg) did not alter regadenoson pharmacokinetics (Figure 8). After administration of regadenoson at doses of 1, 2.5, and 5 μg/kg, the highest regadenoson plasma concentrations were measured at 1-minute post-dose. Regadenoson plasma concentrations decreased rapidly thereafter in the both absence and presence of metoprolol (Figure 8).

Regadenoson plasma concentrations following iv administration of 1, 2.5, and 5 μg/kg regadenoson. Regadenoson plasma concentrations were not significantly altered by metoprolol. Values are mean ± SEM, n = 7
Discussion
The most important finding of the study was that a therapeutic dose of metoprolol (1.5 mg/kg) significantly reduced the 1, 2.5, and 5 μg/kg regadenoson-induced increases in peak HR by 55 ± 8%, 55 ± 4%, and 52 ± 5%, respectively, in conscious dogs. In contrast, metoprolol attenuated the 1, 2.5, and 5 μg/kg regadenoson-induced peak increases in CBF by only 11 ± 7%, 10 ± 4%, and 21 ± 2%, respectively. Thus, metoprolol caused a greater reduction of the tachycardia than of the increase in CBF caused by regadenoson (Figure 1).
In the presence of metoprolol (1.5 mg/kg), the duration of the 2-fold increase in CBF caused by regadenoson was decreased from control (Figures 2, 3). This change may have implications for the timing of radiotracer injection following regadenoson administration in the presence of a beta blocker. However, 5-μg/kg regadenoson (similar to the clinical fixed dose of 400 μg) caused an increase of CBF by ≥2-fold for approximately 6 minutes in the dog treated with metoprolol (Figure 3). Results of a recent study indicated that the blood clearance half-times of thallium-201 and technetium-99m during vasodilator stress with regadenoson were 2.5 and 1.4 minutes, respectively, suggesting that the duration of coronary vasodilation produced by the drug combination of regadenoson and metoprolol may be suitable for distribution and clearance of the two radiotracers.13
Metoprolol is a β1-adrenergic receptor antagonist indicated for the treatment of hypertension, angina, and stable heart failure. The dose (1.5 mg/kg) used in this study is an initial dose for the treatment of hypertension in clinical practice.14 Metoprolol (1.5 mg/kg) completely abolished the isoproterenol-induced (0.1 μg/kg) increase in LV + dP/dt in one conscious dog (data not shown). This indicates that the dose of metoprolol used in this study is an effective dose to block the β1-adrenergic receptor. Regadenoson (1, 2.5, and 5 μg/kg)-induced peak increases in HR, LV + dP/dt, triple, and double products were significantly decreased by up to 55 ± 4%, 63 ± 4%, 76 ± 4%, and 37 ± 6%, respectively, in the presence of metoprolol. These findings indicate that the regadenoson-induced increases in HR, LV + dP/dt, triple, and double products are primarily mediated by indirect stimulation of β1-adrenergic receptors in the heart of conscious dogs, presumably in response to sympathetic activation.11,12 Although metoprolol significantly decreased baseline HR, LV + dP/dt, and both triple and double products, it did not significantly decrease baseline CBF. This finding, although unexplained, is consistent with the results of previous studies using conscious dogs.15,16
The effects of a bolus iv administration of regadenoson to increase both HR and CBF in conscious dogs in this study were consistent with results of previous studies of conscious dogs and human patients.2,6-9 The direct effect of regadenoson to increase CBF is primarily mediated by A2A adenosine receptors and their action to relax coronary arteries,7-9,17 but our results suggest that the regadenoson-induced increase in HR also contributed to the increase in CBF, because the effect of metoprolol to reduce HR in the presence of regadenoson was associated with a decrease in CBF. However, the regadenoson-induced increases in HR, LV + dP/dt, and triple product (an indirect index of cardiac work), were significantly attenuated by metoprolol, whereas the regadenoson-induced coronary vasodilation was reduced by a much smaller magnitude (Figure 1). Thus, the increase of CBF caused by regadenoson was at least partially independent of HR. Taken together, these findings suggest that the A2A adenosine receptor-mediated coronary vasodilation plays a greater role than the increase of HR to mediate the effect of regadenoson to increase CBF.
Previous studies have indicated that the adenosine- and regadenoson-induced increases in HR are due to direct excitation of sympathetic nerves in humans,10 awake rats,11 and conscious dogs.12 The present results support this conclusion. The small increase in HR induced by regadenoson after β1-adrenergic blockade is most likely due to the withdrawal of vagal tone mediated by a baroreflex response to the decrease of arterial blood pressure. This interpretation is supported by our previous study which showed that the regadenoson-induced increase in HR was completely abolished by the combination of β-adrenergic and muscarinic cholinergic blockade or by the ganglionic blocking agent, hexamethonium.12
There are limitations in the clinical application of the results of this study, including: (1) the use of a flow probe for measurement of CBF did not permit us to determine the distribution of blood flow across the wall of the heart (i.e., epi- and endocardial blood flow); (2) studies were performed using healthy dogs with no known coronary disease, and the effects of regadenoson and/or metoprolol may be different in the disease setting; (3) microsphere flow methodology was not used in this study, and therefore the effects of regadenoson and metoprolol on the kinetics of iv contrast dye or radiotracer distribution in the heart have not been assessed. In addition, phasic changes in CBF were not assessed, and therefore further studies are needed to understand the effects of regadenoson on CBF during diastole and systole in response to changes in HR and sympathetic stimulation/blockade.
In summary, the results of this study indicate that (1) 1, 2.5, and 5 μg/kg regadenoson caused a dose-dependent coronary vasodilation, and increases in HR and LV + dP/dt; (2) after β1-adrenergic blockade with metoprolol, the regadenoson-induced increases in HR and LV + dP/dt were significantly attenuated, whereas the regadenoson-induced coronary vasodilation was reduced by a relatively smaller magnitude. Hence, metoprolol at the therapeutic dose of 1.5 mg/kg is highly effective in reducing the positive chronotropic and inotropic effects of regadenoson, and presumably heart motion artifacts in MDCT. These results suggest that regadenoson may be used as a coronary vasodilator in the presence of β1-adrenergic receptor blockade.
References
Iskandrian AE, Bateman TM, Belardinelli L, Blackburn B, Cerqueira MD, Hendel RC, et al. Adenosine versus regadenoson comparative evaluation in myocardial perfusion imaging: Results of ADVANCE phase 3 multicenter international trial. J Nucl Cardiol 2007;14:645-58.
Jaroudi WA, Iskandrian AE. Regadenoson: A new myocardial stress agent. J Am Coll Cardiol 2009;54:1123-30.
Tejani FH, Thompson RC, Iskandrian AE, McNutt BE, Franks B. Effects of caffeine on SPECT myocardial perfusion imaging during regadenoson pharmacologic stress: Rationale and design of a prospective, randomized, multicenter study. J Nucl Cardiol 2011;18:73-81.
Cerqueira MD. The future of pharmacologic stress: Selective A2A adenosine receptor. Am J Cardiol 2004;94:33D-42D.
Hendel RC, Bateman TM, Cerqueira MD, Iskandrian AE, Leppo JA, Blackburn B, et al. Initial clinical experience with regadenoson, a novel selective A2A agonist for pharmacologic stress single-photon emission computed tomography myocardial perfusion imaging. J Am Coll Cardiol 2005;46:2069-75.
Lieu H, Shryock JC, von-Mering GO, Gordi T, Blackburn B, Olmsted AW, et al. Regadenoson, a selective A2A adenosine receptor agonist, causes dose-dependent increases in coronary blood flow velocity in humans. J Nucl Cardiol 2007;14:514-20.
Trochu JN, Zhao G, Post H, Xu X, Belardinelli L, Belloni F, et al. Selective A2A adenosine receptor agonist as a coronary vasodilator in conscious dogs: Potential for use in myocardial perfusion imaging. J Cardiovasc Pharmacol 2003;41:132-9.
Zhao G, Linke A, Xu X, Ochoa M, Belloni F, Belardinelli L, et al. Comparative profile of vasodilation by CVT-3146, a novel A2A receptor agonist, and adenosine in conscious dogs. J Pharmacol Exp Ther 2003;307:182-9.
Zhao G, Messina E, Xu X, Ochoa M, Sun HL, Leung K, et al. Caffeine attenuates the duration of coronary vasodilation and changes in hemodynamics induced by regadenoson (CVT-3146), a novel adenosine A2A receptor agonist. J Cardiovasc Pharmacol 2007;49:369-75.
Biaggioni I, Killian TJ, Mosqueda-Garcia R, Robertson RM, Robertson D. Adenosine increases sympathetic nerve traffic in humans. Circulation 1991;83:1668-75.
Dhalla AK, Wong MY, Wang WQ, Biaggioni I, Belardinelli L. Tachycardia caused by A2A adenosine receptor agonists is mediated by direct sympathoexcitation in awake rats. J Pharmacol Exp Ther 2006;316:695-702.
Zhao G, Serpillon S, Shryock J, Messina E, Xu X, Ochoa M, et al. Regadenoson, a novel pharmacologic stress agent for use in myocardial perfusion imaging, does not have a direct effect on the QT-interval in conscious dogs. J Cardiovasc Pharmacol 2008;52:467-73.
Mekkaoui C, Jadbabale F, Dione DP, Meoli DF, Purushothaman K, Belardinelli L, et al. Effects of adenosine and a selective A2A adenosine receptor agonist on hemodynamic and thallium-201 and technetium-99m-sestaMIBI biodistribution and kinetics. J Am Coll Cardiol Cardiovasc Imaging 2009;2:1198-208.
Kerins DM, Robertson RM, Robertson D. Drugs used for the treatment of myocardial ischemia. In: Hardman JG, Limbird LE, Gilman AG, editors. Goodman & Gilman’s the pharmacological basis of therapeutics 10th ed. New York, NY: McGraw-Hill; 2001. p. 843-70.
Vatner SF, Hintze TH, Macho P. Regulation of large coronary arteries by β-adrenergic mechanisms in the conscious dog. Circ Res 1982;51:56-66.
Vatner SF, Hintze TH. Mechanism of constriction of large coronary arteries by β-adrenergic receptor blockade. Circ Res 1983;53:389-400.
Gao Z, Li Z, Baker SP, Lasley RD, Mayer S, Elzein E, et al. Novel short-acting A2A adenosine receptor agonists for coronary vasodilation: Inverse relationship between affinity and duration of action of A2A agonists. J Pharmacol Exp Ther 2001;298:209-18.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by Gilead Sciences and by NIH PO-1-43023, RO-1-HL50142, and HL 61290 (to T. H. Hintze).
Rights and permissions
About this article
Cite this article
Zhao, G., Zhang, S., Shryock, J.C. et al. Selective action of metoprolol to attenuate regadenoson-induced tachycardia in conscious dogs. J. Nucl. Cardiol. 19, 109–117 (2012). https://doi.org/10.1007/s12350-011-9481-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-011-9481-x