
Abstract
Background
There are limited data on the effect of tracer dose on the reproducibility and accuracy of left ventricular (LV) mechanical dyssynchrony indices by phase analysis of gated single photon emission computed tomography (SPECT) myocardial perfusion imaging (MPI).
Methods and Results
We measured LV dyssynchrony in 54 patients with normal LV ejection and perfusion (group 1) and 54 age and gender matched patients with LV ejection <35% (group 2) using phase analysis of gated SPECT MPI from stress (high dose) and rest (low dose) studies with 2 software programs: Corridor4DM (4DM) and Emory Cardiac Toolbox (ECTb). Although the correlation between rest- and stress-derived standard deviation was good (R = 0.76, P < .0001, with both software programs), there was considerable variability between the measurements (P < .0001 by paired t test). In addition, the rest standard deviation was significantly higher than stress in group 1 (10.2° ± 4.6° vs 6.1° ± 2.5°, and 12.2° ± 6.4° vs 7.9° ± 4.6°, with 4DM and ECTb, respectively, P < .0001 for both) and group 2 patients (44.0° ± 18.0° vs 35.9° ± 21.0° and 47.3° ± 19.2° vs 38.8° ± 19.8°, with 4DM and ECTb, P = .03 and .02, respectively). Similarly, the rest standard deviations were higher than the stress values irrespective of the type of stress test (i.e., exercise vs pharmacological), and the body mass index. Finally, using rest-derived dyssynchrony indices was associated with 9%-13% and 22%-26% false positive rate of significant mechanical dyssynchrony using different cut-off values for groups 1 and 2, respectively.
Conclusion
LV mechanical dyssynchrony indices by phase analysis have more variation and are significantly higher if derived from rest gated SPECT images obtained with low-dose tracer.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Phase analysis of gated single photon emission computed tomography (SPECT) myocardial perfusion imaging (MPI) is a newly emerging technique to derive dyssynchrony indices.1-9 Despite the low frame rate of image acquisition (8-16 frames/cycle), the effective temporal resolution does not suffer greatly and approximates 15 ms (for an average heart rate of 60 beats per minute) when applying first harmonic phase analysis.10 Still, the strength of the technique lies with its ability to average over multiple cardiac cycles (a big advantage in patients with arrhythmias), acquire several hundreds of data points from a three-dimensional LV, being automated and with high reproducibility,1,9 which makes it an attractive alternative to echocardiography. The method depends on extracting count distribution from each slice of the left ventricular (LV) short axis data set and submitting it to a Fourier transform to generate a phase distribution.1 Since most studies are performed using a 1-day Tc-99m low dose-high dose protocol, analysis can be performed on either acquisition sets. There is also growing interest in performing rest gated SPECT with serial imaging to optimize LV lead programming and achieve better response to cardiac resynchronization therapy (CRT).11 While using low-dose tracer dose with gated imaging is important from a radiation exposure standpoint, there are lower counts per pixel, lower signal-to-noise ratio as compared to those obtained with the high tracer dose, and potentially more error in the measurement of dyssynchrony. There are limited studies on the effect of tracer dose (i.e., high vs low) on the reproducibility and accuracy of the derived dyssynchrony indices.12 We hypothesized that the phase standard deviation derived from gated SPECT with low-dose tracer will have more variability, error, and positive bias in calling more dyssynchrony as compared to high-dose MPI studies.
Methods and Materials
Patient Selection
We identified two groups of patients from the SPECT MPI clinical database maintained at the Cleveland Clinic and approved by the Institutional Review Board, between April 2007 and February 2008. Group 1 (N = 54) had normal MPI, LV ejection fraction (EF) ≥50%, and QRS duration <120 ms; Group 2 (N = 54) had LVEF <35% with no restriction on QRS duration, and had normal or fixed perfusion defects (PDS), but no reversible PDS. Both the groups were matched for age and gender. All patients had a gated SPECT MPI for low rest/high stress doses of Tc-99m tetrofosmin. Patients with hypertrophic cardiomyopathy, end-stage renal disease, congenital heart disease, and reversible perfusion defects were excluded. The demographics, co-morbidities, and medications were prospectively entered into an IRB approved data base at the time of testing, and subsequently retrieved for analysis.
Gated SPECT
Gated SPECT MPI was obtained at rest (low dose 10-15 mCi) and stress (exercise or pharmacological) (high dose ~30-45 mCi) using Tc-99m tetrofosmin according to American Society of Nuclear Cardiology.13 The images were obtained with a step and shoot protocol, 180° elliptical orbit with 64 total projections, using a dual-head detector gamma camera with high resolution and low energy collimator. Imaging was started 30-60 minutes after resting or pharmacological stress, and 10-20 minutes following exercise stress. A window of 15% was centered on the 140 keV gamma peak, and the gating was done with 16 frames per RR cycle. Images were reconstructed by filtered back projection using Butterworth and Ramp filters and a 64 × 64 matrix. Scatter and attenuation correction were not performed. All images were reviewed for quality by a nuclear technologist and a board certified nuclear cardiologist.
The LV volumes, mass, and EF were measured from the stress gated images (as this study was done with a larger tracer dose per the institution protocol). The presence and extent of infarction was assessed visually, and quantified using automated polar maps as previously described.14
Mechanical Dyssynchrony
The dyssynchrony index was measured by phase analysis using two semi-automated software programs: Emory Cardiac ToolBox (ECTb)1 and Corridor4DM.15 Extracardiac counts were excluded as permissible without reducing cardiac counts during raw image data processing, and proper alignment of the horizontal and vertical axes of the images was performed as needed. Manual corrections to the center, radius, and apex parameters were made only if there was gross visual misalignment of these parameters, and manual base parameter placement was performed to avoid low counts “scatter” from the base of the LV which might contribute to falsely abnormal phase histogram.16
The phase standard deviation (SD) was measured with the ECTb from the stress and rest gated SPECT by a single observer (board certified nuclear cardiologist) (observer 1). The method has been extensively described and reviewed1,3-5 (Figure 1). The phase SD was also derived with the 4DM software by observer 1 and repeated by observer 2. The method has been described previously and verified against the ECTb.15 Briefly, the maximum myocardial intensity as a function of the gating interval is recorded from a 3-dimensional sampling of the left ventricular myocardium. Each of the time-intensity curves are fitted to a first-order harmonic using Fourier analysis, from which the phase of the first-order harmonic approximates the time from end-diastole (typically the start of the cardiac cycle) to the time of the maximum counts for each region, which represents the peak of mechanical contraction. Even though the ECTb method defines the phase that measures the onset of mechanical contraction, the time point at which the maximal count curve crosses the DC or mean line,17 the time to peak mechanical contraction is the same as the onset of mechanical contraction of the ECTb method but shifted by +90°. This is because the angular distance between the point of the increasing curve intersecting with the DC line and the maximum point of the first harmonic sinusoid is always a constant 90°, as can be shown by taking the difference of the roots of a sinusoid and its derivative. By this equivalence, the temporal resolution of 4DM is also 1/64 of a cardiac cycle whether 8 or 16 frames/cycle per used for image acquisition.10 The phase distribution of the curves is displayed on a histogram, and the SD of the phase distribution is generated. The index is displayed as percentage of the RR cycle, and converted into degrees by multiplying by 3.6 (360/100) (Figure 1). The intra- and inter-observer reproducibility of the resting phase indices were assessed by two blinded experienced readers.

Representative contractility histograms. The figure illustrates the histogram of the phase distribution and polar maps of patients with LVEF < 35% using the Emory Cardiac Toolbox (left panels) and the Corridor4DM (right panels). The phase standard deviation is expressed as % of the R-R interval in the 4DM software, and converted into degrees by multiplying by 3.6 (360/100). SD (phase standard deviation)
Statistical Analysis
A descriptive analysis was performed examining pertinent variables for each group. Continuous variables were expressed as means ± standard deviation, and compared using the paired and unpaired Student’s t test as appropriate. Categorical variables were expressed as percentages and compared using the Pearson Chi-square test. Linear regression and Bland-Altman plots were used for the comparison of the dyssynchrony indices obtained from the high dose (stress) vs low dose (rest) tracer gated SPECT using both software. The results were also stratified based on the type of stress test (i.e., pharmacological vs exercise) and based on body mass index (BMI) ≥ or <30 kg/m2. Intra and inter-observer reproducibility was assessed using the Spearman correlation coefficient, coefficient of variability, and Bland-Altman plots. A P value <.05 was set a priori and considered statistically significant. All statistical analyses were performed using the Statistical Package for Social Sciences, version 11.5, for Windows (SPSS, Chicago, Illinois).
Results
The baseline characteristics and gated SPECT results are summarized in Table 1. There were 54 patients in group 1 (age 66 ± 11 years, 28% female, LVEF 70 ± 10, all with normal perfusion and QRS < 120 ms), and 54 patients in group 2, matched by age and gender (LVEF 29% ± 6%, 44% with QRS > 120 ms, 41 [76%] with perfusion abnormalities, and mean fixed perfusion defect size 26% ± 22%).
Values obtained for phase SD were similar to previously published.1,7 18/54 (33%) of patients in Group 2 had significant mechanical dyssynchrony (20% in those with narrow QRS vs 50% in those with wide QRS duration, P = .04). The intra- and inter-observer reproducibility of the rest phase SD using 4DM software is illustrated in Figure 2. Although the correlation between rest and stress dyssynchrony indices was high (R = 0.76, P < .0001 with both ECTb and 4DM), there was considerable variability (P < .0001 by paired t test with both software), scatter, and positive bias toward the rest indices (Figures 3, 4). Furthermore, the phase SD derived from rest (low dose) gated SPECT studies was significantly higher than the derived index from the stress (high dose) study in each group, irrespective of the software used (i.e., ECTb vs 4DM) (Figure 5) or the type of stress test (i.e., exercise vs pharmacological) (Figure 6).

Intra- and inter-observer variability. The intra- and inter-observer variability of the phase standard deviation obtained from rest gated studies (i.e., low dose tracer) is illustrated using linear regression, Bland-Altman plots, and correlation of variability. 4DM (Corridor4DM), CV (correlation of variability), R (correlation coefficient), SD (phase standard deviation)

Correlation of phase standard deviation with different tracer doses. The phase standard deviations were derived using the Emory Cardiac Toolbox and Corridor4DM software from stress (high tracer dose) and rest (low tracer dose) gated SPECT. The correlations of the indices are displayed on the linear regression plots. 4DM (Corridor4DM), ECTb (Emory Cardiac Toolbox), R (correlation coefficient), SD (phase standard deviation)

Variability of dyssynchrony indices with tracer dose. Bland-Altman plots of different phase standard deviation values obtained with stress, rest gated SPECT, and two available software. ECTb (Emory Cardiac Toolbox), R (correlation coefficient), SD (phase standard deviation), SPECT (single photon emission computed tomography)

Dyssynchrony indices in patients with preserved LVEF and those with cardiomyopathy. The mean phase standard deviation from rest (low tracer dose) gated studies were significantly higher than from the stress (high tracer dose) gated studies in Group 1 (normal LVEF and perfusion), and Group 2 (LVEF < 35%), using either software (ECTb or 4DM). 4DM (Corridor4DM), ECTb (Emory Cardiac Toolbox), LVEF (left ventricular ejection fraction), SD (standard deviation)

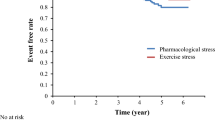
Dyssynchrony indices stratified by type of stress test. The mean phase-derived standard deviation was higher in rest (low-dose) vs stress (high dose) gated studies irrespective of the type of stress test (exercise vs pharmacological). In the subgroup of abnormal patients with exercise stress test (N = 8), there was a trend toward higher values that did not reach statistical significance (upper row). Similarly, there was significant difference between rest and stress indices by paired t test analysis (lower row)
Also, patients with BMI ≥ 30 kg/m2 has similar stress SD° to those with BMI < 30 kg/m2 and similarly for rest SD° for either group; however, the rest SD was significantly higher than stress SD irrespective of the BMI. For patients with BMI < 30 kg/m2, the mean differences of SD (rest-stress) were 3.9° ± 5.1° (paired t test P < .001) and 6.7° ± 20° (paired t test P = .02) for patients in groups 1 and 2, respectively (using the 4DM software). For patients with BMI ≥ 30 kg/m2, the corresponding values were 4.7° ± 4.4° (P < .0001) and 11.5° ± 6.5° (P = .03) for patients in groups 1 and 2, respectively. Similar values were obtained with the ECTb software.
Using a phase SD cut-off value = mean + 2× SD of Group 1 (values obtained from the stress gated studies and comparable to previous study18) to identify significant mechanical dyssynchrony, 7/54 (13%) patients in group 1 and 15/108 (14%) in the combined groups would be falsely labelled as having mechanical dyssynchrony if the rest-derived indices were used with the ECTb, and similarly with the 4DM. Also, using cut-off point for normalcy from previously published papers,1,18 5/54 (9%) in Group 1 and 19/108 (18%) in the combined groups would be falsely labelled as having significant dyssynchrony based on rest indices using the ECTb software, and similarly 4DM. Conversely, using a cut-off value of 43° in group 2 (cut-off value shown to predict response to CRT in patients with LVEF < 35%),19 12/54(22%) and 14/54 (26%) of patients would be falsely labelled as having significant dyssynchrony (and potentially responders to CRT) if SD was derived from the rest-gated studies, using the 4DM and ECTb software, respectively.
Discussion
This is the largest study to evaluate the impact of tracer dose on LV mechanical dyssynchrony index with phase analysis of gated SPECT. The main finding of our study is that phase SD derived from rest gated SPECT with low-dose tracer is higher than the corresponding index derived from standard high dose stress gated images, irrespective of LVEF, analysis software, type of stress test, or BMI. Furthermore, using the rest-dyssynchrony index may “falsely” label up to 9%-13% of patients in Group 1 as having mechanical dyssynchrony (cut-off mean + 2× SD), and 22%-26% of patients with LVEF ≤ 35% (SD cut-off 43°).19
Prior work evaluated the effect of tracer dose on dyssynchrony indices in 20 normal patients using the ECTb software.12 Although there was no significant change between low- and high-dose phase-derived indices, there was a trend toward higher values with low tracer dose scans (i.e., the stress images, per the other institution protocol) (18° ± 8° vs 19° ± 6° for SD, and 46° ± 16° vs 52° ± 12° for bandwidth, with high vs low tracer dose, respectively). The small sample size is probably one of the reasons there was no statistical significance in these values. The other reason is perhaps that the stress studies were performed with low-dose tracer, while rest with high-dose tracer (the opposite protocol). Stress gated images, whether exercise or pharmacological induced, are associated with hyperemia and therefore have more counts, which could affect the dyssynchrony parameters. In fact, in a small paper, an incidental finding was noted that phase SD was lower when derived from high-dose stress-exercise images vs high-dose rest images.20
The lower signal-to-noise ratio, which is associated with more pronounced measurement error, is postulated to be one of the main reasons why low-dose-derived indices are “falsely” higher than high-dose-derived corresponding values. In fact, the standard deviation of the count rate is proportional to the square root of the total counts, which are directly related to the tracer dose; therefore, the standard error of the counts is inversely proportional to the square root of the tracer dose.21 In other words, the smaller the tracer dose, the higher the standard error. The same concept applies when deriving LV volumes and EF; the higher the tracer dose used, the better the images and resolution are, and the more accurate are the measurements. However, one might argue that stress (high dose)-derived indices are intrinsically “smaller” than the rest one because of more synchronized contraction with exercise stress which is often acquired a shorter time after tracer injection, and with two physiologically different LV synchronicity. In fact, Li et al20 showed that exercise-SD was smaller than rest (both high dose gated images) (12.1° vs 15.2°, P = .0499) in a small sample size (N = 17), but concluded that this could be an incidental finding and needs to be verified in larger studies. While this might be true, this finding applied only to exercise stress test and not to pharmacological ones (10.6 vs 10.7, P = .9),20 and does not explain why rest (low dose)-derived SDs are higher than corresponding stress values in pharmacological tests as well (Figure 6). Furthermore, while 10-20 minutes of delay between tracer injection and image acquisition in exercise stress testing is shorter than the corresponding 30-60 minutes with pharmacological or rest, it is quite unusual that the heart rate remains significantly elevated to affect heart synchronicity. Although we did not collect the heart rate at time of image acquisition, a recent paper showed no significant effect on heart rate variability on dyssynchrony indices.22
The positive bias with low-dose-derived indices was observed in both the patient groups, irrespective of LV function, extent of scar, BMI, and type of stress test (Figure 6). Although there was a trend toward higher rest vs stress SD in patients undergoing exercise stress testing, the difference was not statistically different, predominately because of the small sample size (N = 8). Stratifying for BMI was of interest since patients large BMI might have more attenuation and less counts; however, the tracer dose they receive takes into consideration their BMI and is usually higher for those with large BMI.
The change in count distribution on gated SPECT images correlates with wall thickening,23 and is used to derive gated LV parameters such as EF, volumes and phase-derived dyssynchrony indices. Therefore, the amount of counts per pixel, which is directly proportional to the presence of ischemia or infarction, injected tracer-dose, degree of hyperemia, and image acquisition time, is crucial for the accuracy of LV parameters mentioned above.24,25 The less the counts per pixel, the higher are the noise and potential measurement errors.21 This is perhaps one of the reasons why gated SPECT images with Thalium-201 are not used to derived dyssynchrony indices, and why the indices from low dose Tc-99m are not as consistent as those from high-dose gated MPI.
While our study has shown statistically significant difference between low- and high-dose gated MPI to derive dyssynchrony indices, it might be premature to conclude that a low-dose gated SPECT MPI is not acceptable to evaluate dyssynchrony without further validation studies. The high “false positive” rate associated with low-dose rest images, is based on the assumption that the high-dose stress gated images are the “gold standard,” which may not be necessarily true. In fact, there is no gold standard to which study (i.e., stress or rest) or which dose are appropriate to use and to define normalcy. In fact, what would be the minimal acceptable dose of tracer to evaluate dyssynchrony with gated SPECT? This is important particularly when patients radiation exposure is considered, and in an era with growing interest in utilizing gated SPECT to optimize patient selection for CRT with serial gated imaging.11 Perhaps different cut-off values for mechanical dyssynchrony should be defined and used for the stress and rest gated images, and also to account for the tracer-dose used. Whether the differences in the dyssynchrony indices are mainly driven by the tracer dose or by imaging post-stress vs rest, which are two physiologically different states of LV synchrony, cannot be ascertained in this study. A comparison of dyssynchrony from high-dose stress vs high-dose rest gated images might clarify this point. However, this protocol is infrequently used in an era where awareness of radiation exposure is increasing. From a clinical standpoint, when comparing change in mechanical dyssynchrony indices post-CRT, for example, it is important to reproduce the post-CRT images using the same setting for the pre-CRT images (i.e., both stress or rest gated, and similar tracer dose) to minimize potential error when deriving dyssynchrony parameters. However, from a practical standpoint, serial resting images are easier to perform than stress gated images.
Limitations
The study has the limitations of a retrospective study from a single tertiary center. The stress gated SPECT MPI was used in this study as the reference point (high dose tracer study) as opposed to conventional high-dose rest gated studies3,4,7,26; however, this may not be necessarily true, and perhaps we should have different cut-off values for stress and rest gated images. We did exclude patients with stress-induced reversible perfusion defects to avoid any additional source of potential variability to the derived dyssynchrony indices. While a recent study has shown minimal effect of moderate reversible PDS on dyssynchrony indices in 20 patients, the effect of larger ischemic burden and LV stunning was not assessed.12 We did not evaluate the phase-derived histogram bandwidth; however, previous work has shown that SD and bandwidth go hand in hand, and most of the studies are simplifying things and focusing on SD alone.15 There was no separate and standard criterion for normalcy in patients with preserved LVEF and normal MPI; we defined normalcy as values up to 2× SD from the mean from our cohort and from previously published studies. The SD cut-off of 43° to define significant mechanical dyssynchrony in patients with cardiomyopathy and which has been used in many studies, on the other hand, was derived from a single center study and needs to be further validated and reproduced.19 Also, the effective temporal resolution of the 4DMSPECT software has not been tested or verified, but mathematically assumed to be equivalent to the ECTb.10
Mechanical dyssynchrony indices from gated SPECT are influenced by the type of gated images (stress vs rest) and/or tracer dose. In the absence of a gold standard to define normalcy, perhaps different cut-off values need to be established to define and follow-up on mechanical dyssynchrony based on the type of study and tracer dose. More importantly, when comparing change in dyssynchrony indices post-CRT for instance, the same tracer dose and type of testing should be performed to avoid potential error and eliminate confounders.
Further studies are warranted to validate these findings and identify the minimal acceptable tracer dose to evaluate mechanical dyssynchrony.
References
Chen J, Garcia EV, Folks RD, Cooke CD, Faber TL, Tauxe EL, et al. Onset of left ventricular mechanical contraction as determined by phase analysis of ECG-gated myocardial perfusion SPECT imaging: Development of a diagnostic tool for assessment of cardiac mechanical dyssynchrony. J Nucl Cardiol 2005;12:687-95.
Chen J, Bax JJ, Henneman MM, Boogers MJ, Garcia EV. Is nuclear imaging a viable alternative technique to assess dyssynchrony? Europace 2008;10:iii101-5.
Aljaroudi W, Aggarwal H, Venkataraman R, Heo J, Iskandrian AE, Hage FG. Impact of left ventricular dyssynchrony by phase analysis on cardiovascular outcomes in patients with end-stage renal disease. J Nucl Cardiol 2010;17:1058-64.
Aljaroudi W, Koneru J, Iqbal F, Aggarwal H, Heo J, Iskandrian AE. Left ventricular mechanical dyssynchrony by phase analysis of gated single photon emission computed tomography in end-stage renal disease. Am J Cardiol 2010;106:1042-7.
Aljaroudi WA, Hage FG, Hermann D, Doppalapudi H, Venkataraman R, Heo J, et al. Relation of left-ventricular dyssynchrony by phase analysis of gated SPECT images and cardiovascular events in patients with implantable cardiac defibrillators. J Nucl Cardiol 2010;17:398-404.
Atchley AE, Trimble MA, Samad Z, Shaw LK, Pagnanelli R, Chen J, et al. Use of phase analysis of gated SPECT perfusion imaging to quantify dyssynchrony in patients with mild-to-moderate left ventricular dysfunction. J Nucl Cardiol 2009;16:888-94.
Trimble MA, Borges-Neto S, Smallheiser S, Chen J, Honeycutt EF, Shaw LK, et al. Evaluation of left ventricular mechanical dyssynchrony as determined by phase analysis of ECG-gated SPECT myocardial perfusion imaging in patients with left ventricular dysfunction and conduction disturbances. J Nucl Cardiol 2007;14:298-307.
Samad Z, Atchley AE, Trimble MA, Sun JL, Shaw LK, Pagnanelli R, et al. Prevalence and predictors of mechanical dyssynchrony as defined by phase analysis in patients with left ventricular dysfunction undergoing gated SPECT myocardial perfusion imaging. J Nucl Cardiol 2010;18:24-30.
Chen J, Garcia EV, Bax JJ, Iskandrian AE, Borges-Neto S, Soman P. SPECT myocardial perfusion imaging for the assessment of left ventricular mechanical dyssynchrony. J Nucl Cardiol 2011;18:685-94.
Chen J, Faber TL, Cooke CD, Garcia EV. Temporal resolution of multiharmonic phase analysis of ECG-gated myocardial perfusion SPECT studies. J Nucl Cardiol 2008;15:383-91.
Friehling M, Chen J, Saba S, Bazaz R, Schwartzman D, Adelstein EC et al. A prospective pilot study to evaluate the relationship between acute change in LV synchrony after cardiac resynchronization therapy and patient outcome using a single-injection gated-spect protocol. Circ Cardiovasc Imaging 2011;5:532–539.
Aljaroudi W, Koneru J, Heo J, Iskandrian AE. Impact of ischemia on left ventricular dyssynchrony by phase analysis of gated single photon emission computed tomography myocardial perfusion imaging. J Nucl Cardiol 2011;18:36-42.
Hansen CL, Goldstein RA, Akinboboye OO, Berman DS, Botvinick EH, Churchwell KB, et al. Myocardial perfusion and function: Single photon emission computed tomography. J Nucl Cardiol 2007;14:e39-60.
Germano G, Kiat H, Kavanagh PB, Moriel M, Mazzanti M, Su HT, et al. Automatic quantification of ejection fraction from gated myocardial perfusion SPECT. J Nucl Med 1995;36:2138-47.
AlJaroudi W, Jaber WA, Grimm R, Marwick T, Cerqueira M. Alternative methods for the assessment of mechanical dyssynchrony by phase analysis of gated single photon emission computed tomography myocardial perfusion imaging. Int J Cardiovasc Imaging 2011 (in press).
Trimble MA, Velazquez EJ, Adams GL, Honeycutt EF, Pagnanelli RA, Barnhart HX, et al. Repeatability and reproducibility of phase analysis of gated single-photon emission computed tomography myocardial perfusion imaging used to quantify cardiac dyssynchrony. Nucl Med Commun 2008;29:374-81.
Boogers MM, Chen J, Bax JJ. Myocardial perfusion single photon emission computed tomography for the assessment of mechanical dyssynchrony. Curr Opin Cardiol 2008;23:431-9.
Pazhenkottil AP, Buechel RR, Husmann L, Nkoulou RN, Wolfrum M, Ghadri JR, et al. Long-term prognostic value of left ventricular dyssynchrony assessment by phase analysis from myocardial perfusion imaging. Heart 2010;97:33-7.
Henneman MM, Chen J, Dibbets-Schneider P, Stokkel MP, Bleeker GB, Ypenburg C, et al. Can LV dyssynchrony as assessed with phase analysis on gated myocardial perfusion SPECT predict response to CRT? J Nucl Med 2007;48:1104-11.
Li D, Zhou Y, Feng J, Yuan D, Cao K, Garcia EV, et al. Impact of image reconstruction on phase analysis of ECG-gated myocardial perfusion SPECT studies. Nucl Med Commun 2009;30:700-5.
Saha G. Statistics of radiation counting. In: Saha G, editor. Physics and radiobiology of nuclear medicine. 3rd ed. New York: Springer; 2006. p. 34-43.
Al-Jaroudi W, Iqbal F, Heo J, Iskandrian AE. Relation between heart rate and left ventricular mechanical dyssynchrony in patients with end-stage renal disease. Am J Cardiol 2011;107:1235-40.
Galt JR, Garcia EV, Robbins WL. Effects of myocardial wall thickness on SPECT quantification. IEEE Trans Med Imaging 1990;9:144-50.
Vallejo E, Chaya H, Plancarte G, Victoria D, Bialostozky D. Variability of serial same-day left ventricular ejection fraction using quantitative gated SPECT. J Nucl Cardiol 2002;9:377-84.
Thorley PJ, Smith JM. Repeatability of left ventricular ejection fraction and volume measurement for 99mTc-tetrofosmin gated single photon emission computed tomography (SPECT). Nucl Med Commun 2005;26:345-9.
Trimble MA, Borges-Neto S, Honeycutt EF, Shaw LK, Pagnanelli R, Chen J, et al. Evaluation of mechanical dyssynchrony and myocardial perfusion using phase analysis of gated SPECT imaging in patients with left ventricular dysfunction. J Nucl Cardiol 2008;15:663-70.
Author information
Authors and Affiliations
Corresponding author
Additional information
Funds and disclosures: none.
Rights and permissions
About this article
Cite this article
AlJaroudi, W., Jaber, W.A. & Cerqueira, M.D. Effect of tracer dose on left ventricular mechanical dyssynchrony indices by phase analysis of gated single photon emission computed tomography myocardial perfusion imaging. J. Nucl. Cardiol. 19, 63–72 (2012). https://doi.org/10.1007/s12350-011-9463-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-011-9463-z