
Abstract
Background
New iterative algorithms for scatter compensation (SC), noise suppression, and depth-dependent collimator resolution (RR) can shorten rest and stress SPECT acquisitions by 50% while maintaining quality and accuracy equivalent to conventional scans. Full-time stress-only myocardial perfusion SPECT is accurate and efficient when combined with line-source attenuation correction (LSAC). We investigated the potential for half-time stress-only LSAC-SPECT by comparing this to conventional rest/stress SPECT in patients imaged for suspected CAD at three different centers.
Methods
One hundred and ten patients (58% men, 53% exercise) had 64 projection rest/stress Tc-99m ECG-gated SPECT with simultaneous Gd-153 LSAC: 18 had ≤5% CAD likelihood and 92 had coronary angiography. The stress scans were retrospectively ‘stripped’ to create equally spaced 32 projection “half-time” (HT) scans for the emission and transmission (TX) projections. Astonish (Philips, Milpitas, CA) processing with AC, SC, and RR was applied to the HT data with the HT TX maps reconstructed using a Bayesian iterative method. The conventional rest/stress image sets processed using filtered back projection and without AC and the HT-AC stress-only images were interpreted in random sequence by consensus of two readers blinded to clinical information in separate reading sessions.
Results
Comparing rest/stress FBP and HT-LSAC, stress perfusion quality was excellent/good in 82 and 89% (P = .13); interpretive certainty (definitely normal or abnormal) was 88 and 95% (P = .14); sensitivity was 77 and 83% (P = .38); specificity was 67 and 71% (P = .65); normalcy was 94 and 100% (P = 1.0); SSS for CAD pts was 7.4 vs 7.8 and for non-CAD pts was 0.7 vs 0 (P = .44 and .16, respectively). Mean stress LVEF was 60% in both groups.
Conclusion
Stress-only imaging with HT-LSAC using the Astonish acquisition/processing method provides results equivalent to conventional rest/stress scanning. This new approach has the potential to significantly improve operational efficiency without sacrificing accuracy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Over the past decade, SPECT myocardial perfusion imaging has become an important test for assessing patients with suspected or known coronary artery disease (CAD). Because of its frequent utilization, there has been considerable interest in reducing its costs,1,2 shortening acquisition protocols,3-9 and limiting radiation dosimetry.10 One beneficial solution suggested is to eliminate rest imaging in patients in which it is not likely to be useful. Stress-only imaging when paired with attenuation correction has been shown to be both diagnostically accurate4 and to predict low risk for subsequent events when normal.3
Efficiency can also be improved by reducing acquisition time from that currently recommended by ASNC Imaging Guidelines,11 by employing iterative reconstructions combined with derived or measured resolution recovery and noise-reduction techniques.9,12 Preliminary data have demonstrated adequacy of simultaneously acquired line-source transmission maps for attenuation correction using one of these rapid-acquisition protocols (Astonish, Philips, Milpitas, CA).13,14 To date, reduced acquisition time with new algorithms has not been evaluated with stress-only imaging techniques. Important considerations include image quality, interpretive confidence, diagnostic accuracy, and comparability of extent and severity of defects and quantitative function parameters. The purpose of this investigation was to determine the clinical feasibility of a stress-only protocol using rapid and simultaneous acquisition of both emission and transmission data.
Methods
Study Design
The basic design of this study was a consensus blinded interpretation of half-time attenuation-corrected stress-only data compared against conventional rest-stress SPECT imaging without attenuation correction. The gold standard was either a statistical low likelihood for CAD or the results of temporally related coronary angiography. The rest/stress image data were interpreted at a single setting and the stress-only data at a separate session separated by 1 month. To reduce potential bias, the stress-only session included both full-time and half-time stress-only images presented in random sequence.
Patients
This was a retrospective study in which patient studies were derived from the databases of three SPECT laboratories: Cardiovascular Consultants P.A. (Mid America Heart Institute, Kansas City, MO) (n = 26), Hartford Hospital (Hartford, CT) (n = 26), and Cardiology Associates of Central Connecticut (Wallingford, CT) (n = 58). The studies included consecutive patients from each site that had either a statistical low (≤5%) likelihood for CAD according to symptoms, age, gender, and the results of treadmill exercise tests15 but excluding the results of SPECT (n = 18), or had coronary angiography within 181 days (mean 19 ± 34) of SPECT with no change in clinical status (n = 92). Exclusion criteria were prior percutaneous coronary intervention within 180 days, coronary bypass surgery, prior cardiac transplants, and moderate-severe valvular heart disease. The stress tests were performed using treadmill exercise in 53% while the remainder underwent either adenosine (Adenoscan, Astellas, Hospira) or dipyridamole vasodilator stress. All stress testing was performed in accordance with ASNC procedural guidelines.11 Institutional Review Board approval was obtained from the three sites that contributed data.
Image Acquisitions
All the SPECT studies were acquired using Philips CardioMD small field of view systems with Vantage™ Gadolinium-153 scanning line sources. In accordance with ASNC imaging guidelines,11 data were acquired over 64 projections at 20 seconds per projection for the stress and 30 seconds per projection for the rest images, using a 180° RAO-LPO orbit beginning 15-45 minutes after 25-35 mCi of Tc-99m sestamibi (n = 107) or Tc-99m tetrofosmin (n = 3) injection. The collimators were low-energy high resolution, and the energy windows were set at 140 keV ± 20% for the emission and 100 keV ± 20% for the Gd-153 transmission data. An additional 118 keV ± 12% photopeak window was used to compensate for downscatter of Tc-99m into the Gd-153 energy window.11,16 All data were acquired using 16-frame ECG-gating.
Image Processing
Three datasets were processed. The first was the traditional 64-projection rest/stress image set processed using filtered back projection (Butterworth filter, order 5, cutoff 0.45) without attenuation correction. ECG-gated images were filtered using the same filter except with a cutoff = 0.4. The second (intermediate dataset) was stress-only “full-time” 64-projection data processed with Astonish12 and attenuation correction. The transverse images were reconstructed with OSEM-based Astonish using four iterations and eight subsets and a Hanning match filter of cutoff 1.0. The ECG-gated images were reconstructed with Astonish12 using four iterations, eight subsets, and a Hanning match filter of cutoff 0.8. The third (test set) was stress-only “half-time” data in which the 64 projection data were used to generate 32 projections by a ‘stripping’ algorithm that removed every other projection. Therefore this dataset consisted of 32 projections over 180° that had been acquired for 20 seconds each. The corresponding 64-projection ECG-gated images were also handled in this same manner consistent with a 32-projection acquisition.
The transmission maps for the 32 and 64 projection studies were reconstructed using the previously validated method for 64 projections.17 The application to 32 projections was described in prior reports.13,14 For all studies, a uniform initial estimate and 30 iterations were applied to the downscatter compensated projection data.17 Truncation compensation for any artifacts occurring when the patient’s body becomes outside of the small field of view in the transmission images as described earlier18 was applied to the 32 and 64 projection stress-only images identically. Attenuation correction was applied to the Astonish reconstructed emission images using four iterations and eight subsets and match filter cutoff 1.0. When applying attenuation correction, Astonish incorporates an attenuation map-based scatter correction algorithm in addition to the resolution recovery.14
Image Interpretation and Scoring
A total of 330 images were interpreted by consensus of two readers. In case of discordance of interpretations, a third reader adjudicated. The readers were blinded to all clinical information and to whether the stress-only images were full or half-time datasets. For the rest/stress images, which were not attenuation corrected, readers viewed rotating projection, emission, and gated images; for the stress-only images, all of which were attenuation corrected, the rotating projection images were not made available in order to avoid the potential interpretation bias through recognition of 32 or 64 frame data. One-third of the images were rest/stress acquisitions processed with filtered back projection and without attenuation correction (the current standard), one-third were stress-only full-time (64 projections, 20 seconds per projection) Astonish scans with attenuation correction, and one-third were stress-only half-time (32 projections, 20 seconds per projection) Astonish scans with attenuation correction. The gated images were not attenuation corrected.
Both perfusion and gated image quality were interpreted using a 4-point scale of excellent, good, fair, or poor. Fair quality was defined as interpretable but with sources of image degradation such as suboptimal counts or excessive background activity; poor quality was defined as difficult or impossible to fully interpret because of factors such as very poor count statistics or overlap of portions of the myocardium by adjacent count-rich structures. For analysis, quality was merged into two categories (excellent or good, and fair or poor) to reflect the practical implications of image quality on ability to arrive at definitive interpretations. Studies were categorized into one of five diagnoses as recommended by ASNC guidelines,11 after consideration of both the perfusion images and the gated images: definitely abnormal, probably abnormal, equivocal, probably normal, and definitely normal. Each perfusion image was interpreted using a 5-point scale (normal, mildly reduced perfusion, moderately reduced perfusion, severely reduced perfusion, and absent perfusion) for each of 17 segments.19 The segmental scores were then added together to derive a “summed stress score” (SSS). The post-stress-gated images were quantitated for ejection fraction and for both end-diastolic and end-systolic volume using Quantitative Gated SPECT (QGS, Cedars-Sinai, Los Angeles, CA).
For the stress-only scans, the readers indicated whether or not a rest scan would be needed to arrive at a definitive diagnosis (normal, ischemic, or scarred). Scans that showed perfusion defects and abnormal wall motion were interpreted as requiring a rest image to determine whether dysfunctional myocardium was scarred or hibernating. Scans with normal perfusion and normal wall motion/thickening or abnormal perfusion and normal or near-normal wall motion/thickening were interpreted as not requiring rest imaging to interpret a study as either normal or ischemic.
Coronary Angiography
The clinical angiographic reports from each center were submitted to a single investigator who extracted from the reports the visually estimated luminal diameter narrowing for the left main and the 3 major coronary arteries and their major branches. The images were not re-read for this study. Significant disease was defined separately at 70 and 50% thresholds.
Statistical Analysis
The primary comparison was conventional rest/stress FBP datasets versus half-time stress-only datasets. These were compared for quality of both perfusion and gated images and for interpretive certainty using the Χ2 test of independence. All other categorical variables were analyzed with the X2 test of independence, or Fischer’s exact test, as appropriate. For accuracy, definitely normal or definitely abnormal interpretations were used for computations of sensitivity, specificity, and positive and negative predictive values, while probably normal or abnormal and equivocal interpretations were categorized as errors.4 Summed stress scores, along with all other quantitative variables were compared using the Student’s t-test. ROC curves, using coronary angiography as the reference standard, were compared using the methods of Mandrekar and Mandrekar.20 All analyses were conducted using SAS Version 9.1 (SAS Institute, Cary NC) using a P value of <.05 as the criterion for statistical significance. For completeness, a three-way comparison was also performed between rest/stress FBP, HT stress-only LSAC, and FT stress-only LSAC of the same variables, analyzed using ANOVA with Bonferroni-corrected probability values.
Results
There were 64 men (58%) and 46 women (Table 1). The mean body mass index was 32 ± 7 kg/m2 ranging from 21 to 59. The mean age of the low-likelihood group was 44 ± 9 years, compared to 64 ± 12 years for those who had coronary angiography. Of those with angiographic correlation, 27 patients had no significant CAD, 34 had one-vessel CAD, 26 had two-vessel CAD, and 5 had three-vessel CAD. For this study, a significant stenosis was defined as ≥70% luminal diameter narrowing. For completeness, data were also analyzed using a criterion for significance of ≥50% diameter narrowing; at this cut-point, 20 patients had no significant CAD, 27 had one-vessel CAD, 32 had two-vessel CAD, and 13 had three-vessel CAD.
Image Quality
Ninety-eight of the 110 (89%) half-time stress-only perfusion scans were scored as excellent or good in quality, compared with 82% of the traditional rest/stress FBP scans (P = .13) (Figures 1, 2). Twelve of the half-time stress-only perfusion images were scored as fair (7%) or poor (4%), because of less than desired count density in relation to adjacent structures such as liver. By McNemar test, fair or poor quality scans by traditional FBP were the ones most likely to be fair or poor quality by half-time acquisitions (P = .09).

Image quality: stress perfusion (top), stress gating (bottom). Rest/stress filtered back projection (open bars), half-time stress only with attenuation correction (cross-hatched bars), full-time stress only with attenuation correction (dotted bars). P value = .269 for perfusion and .049 for gating, rest/stress versus half-time stress only versus full-time stress only

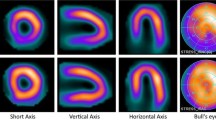
Example of a normal patient. All of the image sets were scored as excellent/good in quality
Ninety (82%) of the half-time 16-frame-gated acquisitions were scored as excellent or good in quality, compared to 93 (85%) of the stress FBP-gated acquisition images (P = . 59). The major cause (80%) of fair or poor quality of the 20 half-time-gated images was suboptimal count statistics.
Interpretive Certainty
In a final interpretation analysis of each study, considering both perfusion and gated images, 105 (95%) of the half-time stress-only acquisitions were interpreted as definitely normal or definitely abnormal compared to 97 (88%) of the traditional rest/stress scans (Figure 3). The reasons for interpretive uncertainty (probably normal or abnormal, or equivocal) were the same for all three types of data: regions of myocardium that were difficult to interpret because of excessive counts in liver or bowel overlapping portions of the inferior wall.

Interpretive confidence. Rest/stress filtered back projection (open bars), half-time stress only with attenuation correction (cross-hatched bars), full-time stress only with attenuation correction (dotted bars) (P value .339)
Diagnostic Accuracy
The normalcy rate (% of low-likelihood studies that were read as normal) was 18/18 (100%) for the half-time stress-only acquisitions compared to 14/18 17/18 (94%) for traditional rest/stress data (P = .125) (Figure 4). Sensitivity and specificity values (CAD defined as ≥70% stenosis) for half-time stress-only acquisitions (83 and 71%) were not different from the traditional rest/stress image sets (77 and 67%) (P values = .171 and .283, respectively).

Diagnostic accuracy of the 3 datasets. Rest/stress filtered back projection (open bars), half-time stress only with attenuation correction (cross-hatched bars), full-time stress only with attenuation correction (dotted bars). There were no statistical differences between half-time stress-only versus rest/stress or half-time stress-only versus full-time stress-only results
Eleven patients with significant (≥70% diameter narrowing) CAD were missed with half-time stress-only acquisitions: 6 had one-vessel CAD and 5 had 2-vessel CAD. Fifteen patients were missed by conventional rest/stress imaging (9 with one-vessel CAD, 5 with 2-vessel CAD, and 1 triple vessel disease). By McNemar comparison, the patients with CAD that were missed by half-time were the same patients missed by traditional rest/stress FBP (P = .16).
There were a total of 17 patients who had transient ischemic dilation (TID) on rest/stress images; all 17 were interpreted as definitely abnormal. One of these was interpreted as normal on half-time stress-only imaging and the remainder were interpreted as definitely abnormal. The one missed patient had a 70% stenosis in the right coronary artery.
By individual coronary artery, there were no significant differences in sensitivity or specificity for half-time stress-only images compared to conventional rest/stress FBP images. The ROC curves for each of the coronary arteries at both 50 and 70% CAD severity thresholds were not different. The ROC curves for the three coronary arteries combined for the two approaches are shown in Figure 5.

ROC curves for the coronaries combined, with the top graph showing results for 50% CAD threshold (P = .84) and the bottom graph for 70% CAD threshold (P = .27). Red line—stress-only half-time; blue line—rest/stress images
Perfusion Defect Extent and Severity
The summed stress scores for the low-likelihood and for the angiography patients by half-time stress-only and FBP images are shown in Table 2. There were no clinically significant differences for either the low-likelihood or the angiography patients by image set. The only difference was in the low-likelihood population, where the summed stress score was 0 for all the half-time stress-only images and was a mean of 0.67 ± 1.4 (range 0-4) for FBP stress images (P = .047). For patients who underwent angiography, the mean summed stress score for half-time stress-only images was 7.8 ± 6.6 (range 0-25) compared to 7.4 ± 6.5 (range 0-30) for conventional FBP stress images (P = .69).
Function Parameters
Mean post-stress LVEF by half-time Astonish was 59.7 ± 12.2%, compared to 59.8 ± 11.9% for the traditional FBP post-stress images (P = .96). The Bland-Altman plot values demonstrate no systematic bias with a mean agreement at 0 (Figure 6). The end-diastolic and end-systolic volumes were also not different (Table 2).

Bland-Altman analysis of the FBP stress versus the Astonish half-time stress-only LVEF
Half-Time Compared to Full-Time Astonish Stress-Only Results
There were no significant differences between half-time and full-time Astonish stress-only results for any of the tested variables. Table 2 shows the combined data for all three approaches.
The perceived need for a rest image for half-time versus full-time stress-only images was 23 and 21%, respectively (P = .744). Of the 25 half-time stress-only images interpreted as needing a rest image for complete diagnosis, 10 (40%) were because of needing greater certainty about presence of CAD, while 10 (40%) were to determine whether or not regional abnormalities were completely fixed in the presence of corresponding regional wall motion abnormalities, and 5 (20%) were to determine the full extent of viability in patients with more than one region of abnormal perfusion and function.
Discussion
The most important finding of this study was that “half-time” stress-only images processed using attenuation correction and the Astonish algorithm were statistically equivalent in quality, interpretive certainty, and diagnostic accuracy compared to both traditional rest/stress filtered backprojection images and to full-time Astonish stress-only attenuation-corrected images. Furthermore, the study demonstrated the feasibility and clinical validity of abbreviated stress-only attenuation-corrected SPECT in that the perfusion image quality was excellent or good in 89% of studies and normalcy, sensitivity, and specificity values were high given the clinically blinded and consensus interpretation approach used in this study.
Approaches to Enable “Half-Time” Acquisitions
Several approaches to reduce SPECT acquisition time while maintaining image quality and diagnostic accuracy have been proposed. This is the first study to comprehensively investigate performance and accuracy, using coronary angiography as the gold standard, of such an approach and to examine the role and value of attenuation correction. The method used in this study (Astonish, Philips Medical Systems, Milpitas CA) employed only 32 projections, but retained the recommended 20 seconds per projection for the stress acquisition. Collimator-to-heart distance at each angular projection was incorporated into an iterative reconstruction algorithm to compensate for spatial resolution and to minimize effects of image noise using a proprietary matched filtering algorithm. In this study the stress perfusion image quality was high for both full-and half-time acquisitions and equivalent to conventional filtered back projection data. Another similar recently described approach using 64 projections acquired for only 10 seconds each8 showed equivalent results between half-time images and conventional images, but did not include coronary angiographic data.
Rapidly Acquired Transmission Map Integrity
An advantage of the scanning line-source approach compared to CT-based attenuation correction is that both emission and transmission data are acquired simultaneously. This avoids potential problems associated with sequential acquisitions such as misregistration of the separately acquired emission and transmission images.21,22 The challenge with line-source attenuation is achieving sufficient counts within the transmission map given the short acquisition time at each projection. We recently studied the transmission maps attained using half-time acquisition times to establish lower limits for fast imaging.13,14 We showed in phantoms and retrospective analysis of patient studies that the attenuation maps were equivalent to full time acquisitions including quantitative attenuation coefficient values for all key tissue regions and important boundaries for registration were equivalent. We also demonstrated that the downscatter correction method developed for full-time acquisition was accurate when applied to fast acquisitions showing no difference when compared to studies with no Tc-99m activity present, especially important for the higher amounts of downscatter from stress activity levels. Additionally, we showed in the anthropomorphic phantom studies that accuracy was sufficient when the line sources decayed to one-fourth their initial activity, suggesting the method remains robust even for shortened acquisitions.
Efficiency Implications
The standard rest/stress SPECT protocol is time-inefficient. It entails injection of a tracer at rest, a 15-60 minute time delay before acquiring rest images for approximately 15 minutes (30 seconds for each of 64 angular projections or 32 camera stops for the most commonly utilized dual-detector systems), a 2-4 hours wait before performing the stress test and injecting the stress bolus of tracer, and another 15-60 minute time delay before acquiring the stress images for approximately 11 minutes (20 seconds for each angular projection). Stress-only imaging reduces SPECT acquisition time by more than 50%, and markedly reduces total patient time. Earlier studies have shown the importance of attenuation correction when performing stress-only imaging, as 40-50% of images are reclassified in comparison to non-attenuation-corrected stress-only images.3 The current investigation demonstrates the feasibility of reducing scanner time to less than 6 minutes and total patient time to approximately 40 minutes for exercise stress (assuming that the post-stress acquisitions began, as in this study, at 15 minutes after stress injection) and just over 1 hour for vasodilator stress (assuming that the post-stress acquisitions began, as in this study, at 45 minutes after stress injection).
One significant element of inefficiency is introduced if patients need to return for rest imaging on a separate day. Because we used 25-35 mCi of Tc-99m perfusion tracer for the stress injection, rest imaging could not be performed until approximately 12-18 hours later to allow for 2-3 half-lives of tracer decay. In our study, 21% of patients needed rest imaging, the majority to differentiate scar from hibernating myocardium in myocardial segments that had both perfusion defects and akinesis. In clinical practice, ideal patients for a stress-only imaging protocol are those without prior myocardial infarction and left ventricular dysfunction, which would be associated with a lower percentage requiring rest imaging to differentiate scar from hibernating myocardium.
Expense and Resource-Utilization Implications
While this study was not designed to track relative costs associated with rest/stress and stress-only studies, the factors determining the relationship between the two can be defined. Compared to conventional rest/stress filtered background studies, the current half-time Astonish stress-only attenuation-corrected approach negates all of the costs associated with a rest scan, and avails the camera, space and personnel for more than double the number of patient studies daily. Additional incurred costs include line-source hardware, new sources every 1-2 years, Astonish software, attenuation-correction software, and higher costs associated with rest scanning for the proportion of patients found to need this.
Radiation Dosimetry Implications
The appropriateness of exposing a patient to the additional radiation associated with a radionuclide injection at rest when the stress image is normal has recently been questioned.10 The effective dose equivalent from a conventional rest/stress Tc-99m sestamibi study is approximately 10-14 mSv23 compared to approximately 8 mSv for a stress-only scan.10 The contribution from the Gd-153 line sources for attenuation correction is nearly negligible (estimated at 0.05 mSv).23 If the assumption that 10 mSv increases lifetime risk of fatal cancer by 0.05%, as suggested in some models23,24 is correct, the risk-benefit ratio associated with an estimated 10,000,000 SPECT scans performed annually in the United States could be positively affected if just 30% of these were performed with stress-only imaging.
Comparison to Prior Stress-Only SPECT Publications
Despite its conceptual attractiveness, the peer-reviewed literature relevant to stress-only imaging is not large. Schroeder6 reported that all 94 out of 460 patients who had a normal stress scan were normal at rest, despite 39 having an abnormal exercise ECG. Thus, rest imaging was shown to be unnecessary in 20% of the patients. Heller et al4 showed the importance of attenuation correction for both interpretive confidence and reduction of need for bringing patients back for a rest image when stress-only imaging was used. Ten experienced readers interpreted 90 studies in either low-likelihood or catheterized patients, arriving at conclusions for each of non-gated and non-attenuation-corrected images, gated but non-attenuation-corrected images, and finally with attenuation correction. Diagnostic certainty more than doubled with the combination of gating and attenuation correction to 85%, with sensitivity and specificity of 97 and 84%, respectively. The lower sensitivity in the current study probably reflects a patient population with less severe disease: in the Heller paper 43% had prior myocardial infarction compared to only 12% in this study, and 51% had multivessel CAD compared to only 34% in this study. Gibson et al3 reported on 729 intermediate likelihood patients tested with stress-only imaging; when the attenuation-corrected scan was normal (including 39% in whom the non-attenuation-corrected stress scan showed an apparent defect), the event rate was only 0.6% over 22 months of follow-up. While the current investigation does not address utilization of stress-only imaging for management decisions or in relation to patient outcomes, it does offer encouragement that this innovative approach can be performed in a complicated cohort of patients and achieve results comparable to conventional rest/stress SPECT.
Study Limitations
The major limitation of this study is that the half-time stress-only data were derived from full-time acquisitions rather than actually acquired in half-time. The half-time images were obtained using every other projection from the 64 20-second angular projections in the clinical study. In practice, the 32 angular projections would be acquired in one-half the time of the 64 projection study. We considered differences between the tracer kinetics and physical decay in the appropriateness of this approach. Myocardial redistribution of Tc-99m-sestamibi or Tc-99m tetrofosmin after initial uptake is less than 5%/hour. Thus any change in distribution over the 7.5 minute difference between the 15 minute conventional scan and the half-time scan is negligible (<1%). This 7.5 minute difference relative to the 6 hour physical half-life of Tc-99m is also negligible. In fact, the shortened scan time minimizes any time-dependent projection data inconsistencies, especially for dual head detector systems where the merging of projections from the last projection of the first detector and the first projection of the second detector differ by the total acquisition time. These arguments would need reconsideration for tracers with rapid redistribution (e.g., thallium-201 or Tc-99m-teboroxime) or short physical half-lives. Finally, the results might be expected to be even better had the half-time stress-only studies been acquired prospectively, as the longer acquisitions employed in this investigation were more likely to be affected by patient motion, a major source of reduced interpretive certainty and accuracy.
Conclusions
The current study extends the understanding about the capabilities of attenuation-corrected SPECT imaging to newer reconstruction algorithms that permit reducing stress acquisition time by one-half and obviating the need for rest imaging in most patients referred for perfusion imaging. The improvements in throughput efficiency, patient convenience, incurred costs, and radiation dosimetry are important reasons for expanding experience with this technique.
References
Medicare Payment Advisory Commission. Report to the Congress: Medicare payment policy. Washington, D.C.: Medicare Payment Advisory Commission; 2005.
Medicare Payment Advisory Commission. Report to the Congress: Medicare payment policy. Washington, D.C.: Medicare Payment Advisory Commission; 2007.
Gibson PB, Demus D, Noto R, Hudson W, Johnson LL. Low event rate for stress-only perfusion imaging in patients evaluated for chest pain. J Am Coll Cardiol 2002;20:999-1004.
Heller GV, Bateman TM, Johnson LL, et al. Clinical value of attenuation correction in stress-only Tc-99m sestamibi SPECT imaging. J Nucl Cardiol 2004;11:273-81.
Santana CA, Garcia EV, Vansant JP, Krawczynska EG, Folks RD, Cooke CD, et al. Gated stress-only 99mTc myocardial perfusion SPECT imaging accurately assesses coronary artery disease. Nucl Med Commun 2003;24:241-9.
Schroeder-Tanka JM, Tiel-van Buul MM, van der Wall EE, Roolker W, Lie KI, van Royen EA. Should imaging at stress always be followed by imaging at rest in Tc-99m MIBI SPECT? A proposal for a selective referral and imaging strategy. Int J Card Imaging 1997;13:323-9.
Snapper HJ, Shea NL, Konstam MA, Oates E, Udelson JE. Combined analysis of resting regional wall thickening and stress perfusion with electrocardiographic—gated technetium 99m-labeled sestamibi single-photon emission computed tomography: Prediction of stress defect. J Nucl Cardiol 1997;4:3-10.
Patton JA, Slomka PJ, Germano G, Berman DS. Recent technologic advances in nuclear cardiology. J Nucl Cardiol 2007;14:501-13.
Borges-Neto S, Pagnanelli RA, Shaw LK, et al. Clinical results of a novel wide beam reconstruction method for shortening scan time of Tc-99m cardiac SPECT perfusion studies. J Nucl Cardiol 2007;14:555-65.
Einstein AJ, Moser KW, Thompson RC, Cerqueira MD, Henzlova MJ. Radiation dose to patients from cardiac diagnostic imaging. Circulation 2007;116:1290-305.
American Society of Nuclear Cardiology. Imaging guidelines for nuclear cardiology. J Nucl Cardiol 2006;13:e25-41. http://www.asnc.org/imageuploads/Imaging%20Guidelines.pdf.
Ye J, Song X, Zhao Z, DaSilva AJ, Wiener JS, Shao L. Iterative SPECT reconstruction using matched filtering for improved image quality. Nuclear Science Symposium Conference Record, 2006. IEEE 2006;4:2285-7.
Cullom SJ, Krishnendu S, Hsu B, et al. Downscatter compensation for attenuation correction with rapid 32-angle simultaneous Tc-99m emission—gadolinium-153 transmission scanning. J Nucl Cardiol 2007;14:S98. (Abstract).
Cullom SJ, Saha K, Case JA, et al. Accurate reconstruction of rapidly acquired 32-angle Gd-153 scanning line source transmission projections for myocardial perfusion SPECT attenuation correction. J Nucl Cardiol 2007;14:S98. (Abstract).
Diamond GA, Forrester JS. Analysis of probability as an aid in the clinical diagnosis of coronary-artery disease. N Engl J Med 1979;300:1350-8.
Case JA, Cullom SJ, Bateman TM. Myocardial perfusion SPECT attenuation correction. In: Iskandrian AE, Verani MS, editors. Nuclear cardiac imaging: Principles & applications. 3rd ed. New York, NY: Oxford University Press; 2002.
Case JA, Hsu BL, Bateman TM, Cullom SJ. A Bayesian iterative transmission gradient reconstruction algorithm for cardiac SPECT attenuation correction. J Nucl Cardiol 2007;14:324-33.
Kokkilara A, Kadakia HH, Ahlberg A, Navare S, Noble G, Cyr G, et al. Validation of attenuation correction using transmission truncation compensation with a small field of view SPECT camera. J Nucl Cardiol 2007;14:S102. (Abstract).
Cerqueira MD, Weissman NJ, Dilsizian V, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. Circulation 2002;105:539-42.
Mandrekar JN, Mandrekar SJ. Statistical methods in diagnostic medicine using SAS® software. In: Proceedings of the thirtieth annual SAS® users group international conference. Cary, NC: SAS Institute Inc. 2005. http://www2.sas.com/proceedings/sugi30/211-30.pdf.
Fricke H, Fricke E, Weise R, Kammeier A, Lindner O, Burchert W. A method to remove artifacts in attenuation-corrected myocardial perfusion SPECT introduced by misalignment between emission scan and CT-derived attenuation maps. J Nucl Med 2004;45:1619-25.
Goetze S, Wahl RL. Prevalence of misregistration between SPECT and CT for attenuation-corrected myocardial perfusion SPECT. J Nucl Cardiol 2007;14:200-6.
Thompson RC, Cullom SJC. Issues regarding radiation dosage of cardiac nuclear and radiography procedures. J Nucl Cardiol 2006;13:19-23.
Whole body scanning: What are the radiation risks from CT? United States Food and Drug Administration, Center for Devices and Radiological Health Web site, updated 4 May 2005. http://www.fda.gov/cdrh/ct/risks.html. Accessed 26 Nov 2007.
Acknowledgments
The authors would like to recognize Ryan Phillips MS, Kyle Robison MS, and Jan Bryngelson BSN for their assistance in gathering data and conducting the blinded reads; Julie Assel BA for her editorial assistance; and Kevin Kennedy MA for statistical support. This research was supported in part by an unrestricted clinical research grant from Philips Medical Systems, Milpitas, CA. TMB, SJC, and JAC receive royalties from the sale of attenuation correction software.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bateman, T.M., Heller, G.V., McGhie, A.I. et al. Multicenter investigation comparing a highly efficient half-time stress-only attenuation correction approach against standard rest-stress Tc-99m SPECT imaging. J. Nucl. Cardiol. 16, 726–735 (2009). https://doi.org/10.1007/s12350-009-9109-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-009-9109-6