
Abstract
Background
The goal of this study was to test whether myocardial triglyceride (TG) turnover including oxidation of TG-derived fatty acids (FA) could be assessed with PET and 11C-palmitate.
Methods and Results
A total of 26 dogs were studied fasted (FAST), during Intralipid infusion (IL), during a hyperinsulinemic-euglycemic clamp without (HIEG), or with Intralipid infusion (HIEG + IL). 11C-palmitate was injected, and 45 minutes were allowed for labeling of myocardial TG pool. 3D PET data were then acquired for 60 minutes, with first 15 minutes at baseline followed by 45 minutes during cardiac work stimulated with constant infusion of either phenylephrine (FAST, n = 6; IL, n = 6; HIEG + IL, n = 6) or dobutamine (FAST, n = 4; HIEG, n = 4). Myocardial 11C washout during adrenergic stimulation (AS) was fitted to a mono-exponential function (Km(PET)). To determine the source of this 11C clearance, Km(PET) was compared to direct coronary sinus-arterial measurements of total 11C activity, 11C-palmitate, and 11CO2. Before AS, PET curves in all groups were flat indicating absence of net clearance of 11C activity from heart. In both FAST groups, AS resulted in negligible net 11C activity and 11CO2 production higher than net 11C-palmitate uptake. AS with phenylephrine resulted in net myocardial uptake of total 11C activity and 11C-palmitate in IL and HIEG + IL, and 11CO2 production lower than 11C-palmitate uptake. In contrast, AS with dobutamine in HIEG resulted in net clearance of all 11C metabolites (total 11C activity, 11C-palmitate and 11CO2) with 11CO2 contributing 66% to endogenous FA oxidation. The AS resulted in significant Km(PET) in all the groups, except HIEG + IL. However, positive correlation between Km(PET) and 11CO2 was observed only in HIEG (R 2 = 0.83, P = .09).
Conclusions
This is the first study to demonstrate that using PET and pre-labeling of intracardiac TG pool with 11C-palmitate, noninvasive assessment of myocardial TG use is feasible under metabolic conditions that favor endogenous TG use such as increased metabolic demand (β-adrenergic stimulation of cardiac work) with limited availability of exogenous substrate (HIEG).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Long-chain fatty acids (FA) are the primary energy source for the heart.1,2 In the healthy heart, 70-90% of the FA entering the cell are immediately oxidized, with the remaining 10-30% stored in the intracardiac triglyceride (TG) pool.3-5 These stores serve as a buffer that compensates for short-term differences in FA supply and lipid oxidative demand, and provide FA when plasma FA concentrations reach low levels.6 Due to its small mass, the turnover of myocardial TG is quick,7 and is inversely related to the concentration of exogenous FA.4,8-10 In normal perfused rat hearts, 11% of mitochondrial ATP production is attributed to oxidation of the myocardial TG-derived FA,4,11 increasing to 50% when exogenous energy sources are limited.4 Myocardial TG turnover can be rapidly accelerated by adrenergic stimulation (AS).12-18
The contribution of endogenous TG-derived FA to overall energy metabolism appears to be altered in various animal models of cardiac disease. For example, in failing rat hearts, endogenous TG, measured with 13C-magnetic resonance spectroscopy, is not oxidized even though exogenous palmitate oxidation is unchanged.19 In contrast, TG turnover provides up to 70% of the ATP production in uncontrolled diabetes10,20 and during reperfusion of ischemic hearts.5 High levels of TG in the heart cause diminished contractile function, hypertrophy, and myocyte death.21-23 Therefore, lipolysis of intracardiac TG might also play an important physiologic role by protecting the heart from deleterious effects of surplus lipid accumulation.
Relatively little is known about regulation of myocardial TG metabolism in humans in either health or disease. This is primarily due to the lack of adequate methods for its measurement.7,24-26 At least in theory, myocardial lipolysis can be quantified based on the rate of glycerol release from the heart measured with arterio-coronary sinus balance.27 This method, however, requires the tenuous assumptions that all lipolysis is complete (i.e., hydrolysis of one TG molecule yields one glycerol molecule) and that the heart cannot oxidize glycerol. In any case, it is too invasive for routine use. Recently, 1H-MRS was used to detect myocardial TG content and net lipolysis.28-32 However, this approach does not allow for estimation of the rate of the TG turnover. On the other hand, to date the most common method for noninvasive measurement of myocardial FA metabolism is compartmental modeling of PET kinetics of 11C-palmitate.33-37 However, this approach measures only metabolism of exogenous FA and does not account for the contribution from the intracardiac TG pool.
Accordingly, the goal of this study was to investigate the feasibility of assessing myocardial TG turnover non-invasively using PET and 1-11C-palmitate. To do so, we pre-labeled the myocardial TG pool with 11C-palmitate and, taking advantage of the higher sensitivity of 3D (or septaless) PET,38 measured the rate of 11C washout from the myocardium during adrenergic stimulation in a well-controlled canine model studied over a wide range of substrate and hormonal conditions. To determine the source of the PET 11C clearance, direct coronary sinus-arterial measurements of the total 11C, 11C-palmitate, and 11CO2 counts were analyzed and compared with clearance rate of PET 11C activity.
Materials and Methods
Animal Preparation
All animal experiments were conducted in compliance with the Guidelines for the Care and Use of Research Animals established by Washington University’s Animal Studies Committee. Purpose bred 6.2-9.8-kg (7.65 ± 0.88 kg) male beagle dogs were fasted, anesthetized, and instrumented as reported previously.39,40 One femoral vein was cannulated to administer drugs. Catheters were placed in the thoracic aorta via the femoral arteries for arterial sampling and monitoring of arterial blood pressure. To obtain venous blood samples, a coronary sinus catheter was placed via the right external jugular vein under fluoroscopic guidance as previously described.37 The ECG, arterial blood pressure, and heart rate were monitored throughout the study.
To achieve a wide range in myocardial use and oxidation of endogenous TG, 26 dogs were studied under various conditions established 60 minutes prior to tracer injection. Ten dogs were studied after overnight fasting (FAST). To increase myocardial FA uptake, a continuous infusion of 20% Intralipid (IL) (Fresenius Kabi Clayton, LP; 1 mL/minute) was administered in six dogs. To switch myocardial substrate metabolism from primarily FA to glucose use, a hyperinsulinemic-euglycemic clamp (HIEG) was performed in ten dogs, using a continuous infusion of insulin (70 mU/kg/hour) along with an adjustable infusion of 20% dextrose.35 To assess the effect of competing exogenous substrates on the accuracy of the measurement of TG turnover, six out of the ten HIEG dogs received concomitant administration of IL (HIEG + IL). Since we wanted to investigate whether an acute increase in cardiac work alone was sufficient to stimulate myocardial TG mobilization, or whether direct activation of lipolysis was required as well, cardiac work was stimulated with either phenylephrine or dobutamine. Accordingly, in six FAST, and all IL and HIEG + IL dogs, cardiac work was increased with phenylephrine (0.84-1.6 μg/kg/minute). In four FAST and all HIEG dogs, cardiac work was increased with dobutamine (20 μg/kg/minute). The difference in these interventions was based on the fact that unlike phenylephrine, dobutamine stimulates lipolysis. Therefore to be able to compare these two groups, IL infusion was added to HIEG to mimic peripheral lipolysis during adrenergic stimulation with phenylephrine.
Experimental Protocol
All PET studies were performed on a microPET 220 (Concorde Microsystems Inc.) which operates solely in 3D mode. After a position scan, a bolus of 1110-1480 MBq of 11C-palmitate was injected, and 45 minutes were allowed41 to minimize uptake and oxidation of 11C-palmitate and maximize 11C labeling of myocardial TG. Continuous dynamic PET data acquisition was started after this waiting period. To determine the basal rate of 11C clearance from the myocardium, data were collected for 15 minutes while the heart was at rest. Cardiac work was then increased with a constant infusion of either phenylephrine or dobutamine, which was continued throughout the rest of the study. Simultaneous arterial and coronary sinus blood samples for 11C total activity and 11C-palmitate metabolites measurements (11C-palmitate and 11CO2) (in counts/mL/minute) were obtained after 11C-palmitate administration during baseline (at 2, 10, and 45 minute) and adrenergic stimulation (at 60, 62, 65, 70, 75, 85, 95, and 105 minute). Another set of arterial and coronary sinus blood samples were collected at 0, 10, 45, and 85 minute for plasma substrates measurements (glucose, free FA, and lactate) and insulin levels, blood gases, pH, hematocrit, and hemoglobin.
Measurements of Unlabeled Plasma Substrates
Plasma glucose and lactate levels were assayed enzymatically with a 2300 STAT Plus Analyzer (YSI Life Sciences, Yellow Springs, OH). Plasma free FA levels were measured using an enzymatic colorimetric method (Wako NEFA C kit, Wako Chemicals USA, Richmond, VA). Plasma insulin was measured by radioimmunoassay (Linco Research Co., St. Charles, MO).
Measurements of Plasma 11C-Palmitate and its Metabolites
Plasma 11C total activity was measured on a gamma counter in counts/mL/minute. All directly measured arterial and coronary sinus 11C data were normalized to injected dose as well as decay corrected by time lapsed from tracer injection to blood sampling time. The contribution of 11CO2 and 11C-palmitate to total 11C radioactivity in each of the arterial and coronary sinus samples was determined quantitatively as previously described.35 As we were interested only in clearance of pre-labeled intramyocardial TG, total myocardial 11C activity, 11C-palmitate, and 11CO2 were calculated as their coronary sinus minus arterial counts. The positive differences were considered as myocardial clearance of the corresponding measurements, while negative values indicated myocardial uptake of tracer.
PET Image Analysis
Myocardial 11C-palmitate transaxial composite PET images (10-60 minutes) were summed to place myocardial regions of interest. To minimize contamination from septum and liver, eight regions of interest for each study were placed on the anterior (n = 4) and lateral (n = 4) walls and traced into each dynamic frame to generate myocardial 11C time activity curves. To investigate whether myocardial clearance of PET 11C-activity during adrenergic stimulation reflected oxidation of endogenous TG, time-activity curves for each region corresponding to the first 30 minutes of adrenergic stimulation were fitted to a mono-exponential function. Due to low 11C activity after 45 minutes of PET data acquisition which led to increased data noise, the last 10-15 minutes of data collection were excluded from analysis.
For each intervention, the estimated rate constants, Km(PET) (minute−1), were averaged to generate a mean rate constant per study and compared to myocardial net 11C activity, 11C-palmitate, and 11CO2 direct measurements obtained from arterial and coronary sinus sampling.
Statistical Analysis
All data are presented as mean ± SD. Differences in myocardial total 11C activity, 11C-palmitate, or 11CO2 measurements between pre- and post-adrenergic stimulation for a given intervention were compared by means of two-way analysis of variance (ANOVA) for repeated measurements, where the post hoc Scheffé test was used to localize differences among measurements. Correlations between Km(PET) and 11C-palmitate or 11CO2 measurements were done by linear regression. A P value of <.05 was considered statistically significant.
Results
Hemodynamics
Hemodynamic data are shown in Table 1. At baseline, heart rate and diastolic blood pressure were comparable across groups except in HIEG + IL, where both parameters were the highest (P < .05 vs dobutamine FAST). Systolic blood pressure was the highest in HIEG group (P < .05 vs IL). There were no significant differences in rate pressure product among the study groups.
Adrenergic stimulation resulted in an overall increase in all hemodynamic measurements (Table 1, BL vs AS P < .0001). Post hoc analysis showed that compared to baseline, adrenergic stimulation resulted in (1) increased heart rate in dobutamine FAST only; (2) increased systolic blood pressure in all groups; (3) increased diastolic blood pressure in phenylephrine but not dobutamine groups, and (4) increased rate pressure product in all except the HIEG group. Phenylephrine increased the rate pressure product via increases in blood pressure, while dobutamine-induced increases in rate pressure product were due to increases in both heart rate and systolic blood pressure. Rate pressure product was higher during dobutamine than during phenylephrine infusion (ANOVA P < .0001, 18,073 ± 5,840 vs 12,503 ± 3,744, P < .01).
Plasma Substrate and Insulin Levels
Arterial plasma levels of substrate and insulin for all interventions are presented in Table 2. Adrenergic stimulation resulted in an overall increase in plasma glucose levels, with baseline levels the lowest in the FAST groups (P < .05 vs IL) and no differences among interventions during adrenergic stimulation. At baseline, plasma lactate concentrations were the highest in the IL group (P < .005 vs HIEG and both FAST groups). During adrenergic stimulation, while lactate levels remained significantly higher in the IL group, overall lactate levels were not different from baseline. There was a weak but significant increase in plasma FA during adrenergic stimulation (P = .04). Plasma FA levels by design were the highest in IL and HIEG + IL (P < .05 vs HIEG and both FAST groups) during both baseline and adrenergic stimulation. Plasma insulin levels by design were the highest in HIEG and HIEG + IL groups (P < .05 vs IL and both FAST groups) during both baseline and adrenergic stimulation. However, adrenergic stimulation did not alter baseline plasma insulin levels.
Direct Coronary Sinus-Arterial Measurements of Total 11C Activity, 11C-Palmitate, and 11CO2
Figure 1 shows directly measured differences between coronary sinus and arterial plasma for total 11C activity (black bars), 11C-palmitate (open bars), and 11CO2 production (gray bars) as an average of values obtained at baseline (2, 10, and 45 minute) pre-phenylephrine (Figure 1A) and pre-dobutamine (Figure 1C), and during adrenergic stimulation (60, 62, 65, 70, 75, 85, 95, and 105 minute) with phenylephrine (Figure 1B) and dobutamine (Figure 1D).

Directly measured averaged coronary sinus-arterial difference (CS-ART) for total 11C activity (black bars), 11C-palmitate (white bars) and 11CO2 (grey bars) before (A and C) and during adrenergic stimulation of cardiac work (B and D) with phenylephrine (A and B) and dobutamine (C and D). Data are presented as group mean ± SD
Net uptake of total 11C activity and 11C-palmitate, shown as negative values, as well as 11CO2 production, shown as positive values, were observed in all the five groups at rest, before adrenergic stimulation of cardiac work (Figure 1A, C), as well as in IL and HIEG + IL during phenylephrine stimulation (Figure 1B). Interestingly, 11CO2 production in these groups never exceeded 11C-palmitate uptake, suggesting that most, if not all, of the 11CO2 production was likely due to oxidation of exogenous FA. However, in both FAST groups, stimulation with either phenylephrine or dobutamine resulted in negligible total 11C-activity exchange while 11C-palmitate uptake was lower than 11CO2 production in both groups, suggesting oxidation of both exogenous 11C-palmitate and endogenous myocardial TG-derived 11C-palmitate. In contrast, in the HIEG group (Figure 1D) we observed net release for all the three 11C measurements (total 11C activity, 11C-palmitate and 11CO2), with two-thirds of 11C release accounted for by 11CO2 apparently produced from oxidation of myocardial 11C labeled TG, and one-third by the washout of non-11CO2 metabolites attributable to myocardial TG-derived 11C labeled FA.
PET Measurements During Adrenergic Stimulation
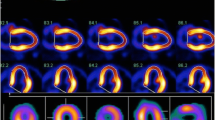
Figure 2 shows representative PET myocardial time activity curves (dots) before and during adrenergic stimulation with phenylephrine (Figure 2A-C) and dobutamine, mono-exponential fitting to PET clearance of myocardial 11C activity during adrenergic stimulation (solid lines), and the corresponding clearance rates (Km, minute−1) (Figure 2D-E). Before adrenergic stimulation, PET curves in all the groups were nearly flat demonstrating a lack of net clearance of 11C activity. During adrenergic stimulation with phenylephrine, PET Km (minute−1) rates were comparable in FAST and IL (0.002 ± 0.001 and 0.003 ± 0.003, respectively, P = NS), and negligible in HIEG + IL (0.0004 ± 0.0005, P = NS from zero).

Representative myocardial PET time-activity curves (dots) and mono-exponential fitting (lines) of total PET 11C activity (y-axes) during adrenergic stimulation of cardiac work with phenylephrine (A-C) and dobutamine (D-E). Km, rate of 11C clearance from myocardium
In contrast, during dobutamine stimulation, PET Km (minute−1) rates were significantly higher than during phenylephrine stimulation of cardiac work (0.006 ± 0.003 vs 0.002 ± 0.002, P < .001) with comparable rates in both FAST and HIEG groups (0.006 ± 0.003 vs 0.006 ± 0.003, respectively, P = NS).
During phenylephrine stimulation, there was no significant positive correlation between Km (minute−1) and either 11C activity, 11C-palmitate, or 11CO2 exchange (not shown). However, when individual dogs were examined, three in FAST, two in IL, and two in HIEG + IL studies showed net clearance of 11C activity with 11CO2 release greater than 11C-palmitate uptake. Thus, in these studies 11CO2 production must have been due, at least in part, to oxidation of endogenous FA.
Figure 3 shows correlation between PET Km (minute−1) (y-axis) and the difference in directly measured coronary sinus and arterial plasma net myocardial 11C activity (Figure 3A, D), 11C-palmitate (Figure 3B, E), and 11CO2 (Figure 3C, F) during cardiac work stimulated with dobutamine in FAST (Figure 3A-C) and HIEG (Figure 3D-F) groups.

Correlation between total 11C clearance measured by PET (Km(PET) (y-axes) (A-F) and averaged coronary sinus-arterial difference (x-axes) of total 11C activity (A and D), 11C-palmitate (B and E), and 11CO2 (C and F) during adrenergic stimulation of cardiac work with dobutamine in FAST (A-C) and HIEG (D-F) studies. Negative values on x-axes indicate tracer uptake and positive values tracer clearance
In FAST studies, there was a strong trend toward significant correlation between Km (minute−1) and directly measured net total 11C activity (Figure 3A, P = .06), with no correlation between Km (minute−1) and 11C-palmitate (Figure 3B) or 11CO2 (Figure 3C). While FAST studies averaged net uptake of 11C-palmitate (Figure 3B) and production of 11CO2 (Figure 3C), 11C-total net uptake was observed in two of the animals and net release in the other two (Figure 3A). In the two studies with 11C-activity release, uptake of net 11CO2 was also greater than 11C-palmitate uptake, indicating that there was oxidation of both exogenous and endogenous sources of FA.
In contrast, in HIEG group in all the four dogs, there was 11C clearance resulting in correlative trend between PET Km (minute−1) and total 11C activity (Figure 3D, R 2 = 0.64, P = .2), but not with 11C-palmitate (Figure 3E). However, there was strong but not significant correlation between PET Km (minute−1) and 11CO2 (Figure 3F: R 2 = 0.83, P = .09). These data in conjunction with the observations obtained from directly measured differences in coronary sinus and arterial plasma corroborate that PET clearance of 11C activity during dobutamine-induced cardiac work in HIEG group can be attributed to myocardial 11CO2 production from oxidation of intracardiac 11C labeled TG.
Discussion
To the best of our knowledge, to date noninvasive measurements of myocardial FA metabolism using PET and radionuclide tracers have been limited to measurements of exogenous FA uptake and metabolism, including oxidation and esterification of FA. In this study, we investigated for the first time whether TG turnover including TG degradation and oxidation could be assessed noninvasively with PET and 11C-palmitate.
To do so, we used 11C-palmitate to pre-label the myocardial TG pool of dogs studied under a wide range of substrate and hormonal conditions, and using 3D PET, measured the rate of 11C washout from the myocardium at baseline and during adrenergic stimulation. To determine whether the latter in fact represented mobilization of the intracardiac TG pool, we correlated the PET rate of 11C clearance (Km (minute−1)) with directly measured arterial and coronary sinus total 11C, 11C-palmitate, and 11CO2 counts.
We found that before adrenergic stimulation, there was net uptake of total 11C activity and 11C-palmitate that exceeded 11CO2 production in all the groups (Figure 1A, C). In addition, flat PET curves were also observed in all groups indicating absence of net clearance of 11C activity from heart (Figure 2). Adrenergic stimulation with phenylephrine resulted in net myocardial uptake of total 11C activity and 11C-palmitate in IL and HIEG + IL while 11CO2 production was less than 11C-palmitate uptake. This pattern suggested exogenous FA as the main source of FA oxidation. Adrenergic stimulation with either phenylephrine or dobutamine in FAST groups resulted in negligible net 11C activity with net 11C-palmitate uptake lower than 11CO2 production, suggesting oxidation from both exogenous and endogenous sources independent of the adrenergic stimulation used. In contrast, adrenergic stimulation with dobutamine in HIEG resulted in net clearance of all 11C metabolites (total 11C activity, 11C-palmitate, and 11CO2), with 11CO2 contributing two-thirds of to total 11C washout, suggesting that in this case 11CO2 production could be attributed exclusively to oxidation of endogenous TG.
To our knowledge, this is the first attempt to label the myocardial TG pool with 11C using 11C-palmitate for subsequent imaging with PET. This approach differs significantly from the way early kinetics of PET 11C clearance have historically been used to assess myocardial oxidation of exogenous FA, in that we sought to quantify the very late kinetics of the tracer representing the metabolism of myocardial TG. This presented a challenge due to the short half-life of the tracer (20 minutes) compared to the time required to label the TG pool as well as to clear the heart of 11CO2 derived from direct oxidation of the injected 11C-palmitate. However, the 45-minute waiting period between the injection of 11C-palmitate and the beginning of the 3D PET data acquisition was sufficient, as seen from the practically flat time activity curves before adrenergic stimulation during the first 15 minutes of each scan (Figure 2A-E). This was true in all the animals regardless of the conditions under which they were studied, e.g., in the fasted state vs infused with glucose and insulin and/or Intralipid. This allowed us to determine whether adrenergic stimulation increased the rate of 11C clearance from the myocardium. Since we wanted to investigate whether an acute increase in cardiac work alone was sufficient to stimulate myocardial TG mobilization, or whether direct activation of lipolysis was required as well, cardiac work was stimulated with either phenylephrine or dobutamine. Dobutamine, as a β2-agonist, has a direct lipolytic effect42,43 while the α1-agonist phenylephrine is an inhibitor of lipolysis.44
Although both agents increased cardiac work and stimulated PET clearance of 11C from myocardium, phenylephrine infusion resulted in very low Km(PET) in FAST and IL groups (Figure 2A, B), with no significant PET clearance in HIEG + IL group (Figure 2C). In contrast, PET Km (minute−1) was 3-4 folds higher during dobutamine infusion (Figure 2D, E). At least in theory, this difference could be due to the fact that phenylephrine increased the rate pressure product by only ~40%, with this being mostly due to an increase in blood pressure, whereas dobutamine more than doubled the rate pressure product, as a result of increases in both heart rate and systolic blood pressure. These findings are expected given the higher inotropic effect of β-adrenergic agents.45 However, this differential response cannot explain the observed differences in PET clearance, because PET Km (minute−1) was still significantly higher (P < .05) in dobutamine-infused animals (0.006 ± 0.003 minute−1) than in phenylephrine-infused animals (0.002 ± 0.002 minute−1) even when the analysis was restricted to those with comparable rate-pressure products (16,526 ± 3,826 and 14,059 ± 3,915 beats/minute/mm Hg for seven dobutamine- and 13 phenylephrine-treated animals, respectively). Thus, these differences could be attributed to lipolytic effect of dobutamine that resulted in higher TG turnover.
Since the PET clearance of 11C during adrenergic stimulation of cardiac work could have resulted from utilization of either exogenous 11C-palmitate taken up from plasma or from endogenous intracardiac TG pre-labeled with 11C-palmitate, we calculated the directly measured coronary sinus-arterial difference in total 11C activity to determine whether there was a net uptake or net release of tracer. To determine the extent to which any net release of 11C could be attributed to oxidation vs egress of non-metabolized 11C-palmitate released from endogenous TG, we also calculated coronary sinus-arterial differences in 11CO2 and 11C-palmitate.
The lack of net 11C release from the myocardium following phenylephrine administration in either of the study groups (Figure 1B) did not allow for definitive identification of the source of the PET clearance under these conditions. However, analyzing the individual studies, we found that in almost one-third of the studies, there was 11C clearance from myocardium with 11CO2 production greater than 11C-palmitate uptake, suggesting that at least, in part, myocardium utilized endogenous intracardiac TG. Moreover, in two out of these seven dogs, we observed release from myocardium of not only total 11C and 11CO2 but also intracardiac TG-derived 11C-palmitate. Further attempts to determine under which metabolic conditions or level of cardiac work phenylephrine stimulated myocardial TG turnover fell short due to significant variability of metabolic and hemodynamic parameters among these experiments.
On the other hand, either negligible (FAST) or net release (HIEG) of total 11C activity from the heart was observed during dobutamine stimulation (Figure 1D), in keeping with the higher values for Km(PET) observed in these experiments (Figure 2D and E). Further analysis of individual FAST dogs showed that in two animals with the highest levels of insulin (102 and 180 μU) there was total 11C net uptake, and in the other two with significantly lower insulin levels (10.3 and 60 μU) there was net 11C release (Figure 3A).46 11CO2 production in FAST dogs was also greater than 11C-palmitate uptake, indicating that there was oxidation of both exogenous and endogenous sources of FA. In contrast, release of all 11C-metabolites in HIEG combined with correlation between Km and 11CO2 production, but not with either total 11C or 11C-palmitate, demonstrate that myocardial TG turnover could be successfully measured under conditions of enhanced cardiac work in the presence of low levels exogenous FA available for oxidation. Of note, the assumption that if there were net uptake, then there could not be net clearance of tracer is valid only for averaged net measurements. However, it does not apply to PET dynamic data presented here, where myocardial tracer uptake is mostly represented in the early kinetics of the PET 11C time-activity curves, while oxidation, as measured by the production of 11CO2, and potentially TG turnover, are mostly represented in the late kinetics of the PET curves. The fitting of a mono-exponential function to the late kinetics of PET 11C activity should then be representative of these clearances, even in the presence of net tracer uptake.
There are, however, certain limitations to this method. This approach measures only clearance of the labeled TG and does not allow for the upstream estimation of myocardial TG pool. Therefore, this method provides only an index of myocardial TG turnover. However, we showed that PET clearance curves do reflect the myocardial TG turnover, and combined with the conventional PET protocol for measurement of myocardial exogenous FA metabolism, it may provide additional valuable information regarding the contribution of the endogenous myocardial TG to overall lipid metabolism in heart. Another limitation is the fact that due to confounding effects of continued myocardial uptake of exogenous 11C-palmitate, this study method is unable to measure back-diffusion of TG-derived 11C-palmitate originating from lipolysis. As a consequence, the assessment of total TG lipolysis (as opposed to the component that undergoes oxidation) is underestimated. The third limitation is the high dose/kg of 11C-palmitate used in this study that greatly exceeds the dose allowed for humans. In our study, we had to use high dose of short half-life tracer 11C-palmitate (20 minutes) because of the rather long (105 minute = over 5 half-lives) protocol of this study. However, by the end of 45-minute waiting period, the 11C curve reached the plateau, and it is possible that a shorter period could be sufficient for pre-labeling of myocardial TG pool. We also observed that the tracer washout in response to adrenergic stimulation occurred very fast, within approximately first 15 minutes. Therefore, it is possible to shorten the current protocol time to 60 minutes (35-40 minutes of pre-labeling of the TG pool, data acquisition for 10 minutes at baseline, and 20 minutes during adrenergic stimulation), and hence, the dose sufficient for this study could be decreased to a more acceptable 20-25 mCi. Further studies are required to determine whether these measurements can be obtained using a lower dose and imaging with newer and more sensitive human 3D PET devices. Proven successful, this method can become useful as part of noninvasive basic research and human clinical studies designed to understand the role of myocardial TG turnover in the healthy and diseased heart, using metabolic interventions that result (1) in the storage and (2) in subsequent use of endogenous TG, such as HIEG + dobutamine. Thus, in order to detect alterations in myocardial TG turnover among different populations, clinical (or basic) metabolic studies, such as diabetic or obese patients vs healthy controls, young vs aging, or male vs female subjects, could be implemented after pre-labeling of the TG pool and under the same metabolic intervention (i.e., HIEG clamp and β-adrenergic stimulation of cardiac work). The approach implemented in this study is a first and critical step for the future development of more sophisticated imaging and modeling approaches. These approaches may include multi-imaging/multi-tracer approaches that would combine established imaging methods to measure the TG pool, such as 1H-MRS, and more-advanced PET kinetic approaches to assess the fate of the myocardial TG pool including back-diffusion of 11C-palmitate derived from TG degradation and TG oxidation.
Conclusion
This is the first study to demonstrate that using PET and pre-labeling of intracardiac TG pool with 11C-palmitate, noninvasive assessment of myocardial TG use is feasible under metabolic conditions that increase demand for substrate (β-adrenergic stimulation of cardiac work) but limit availability of exogenous FA (HIEG).
References
Bjorkman O. Fuel metabolism during exercise in normal and diabetic man. Diabetes Metab Rev 1986;1:319-57.
Gold M, Spitzer JJ. Metabolism of free fatty acids by myocardium and kidney. Am J Physiol 1964;206:153-8.
Lopaschuk GD, Belke DD, Gamble J, Itoi T, Schonekess BO. Regulation of fatty acid oxidation in the mammalian heart in health and disease. Biochim Biophys Acta 1994;1213:263-76.
Saddik M, Lopaschuk GD. Myocardial triglyceride turnover and contribution to energy substrate utilization in isolated working rat hearts. J Biol Chem 1991;266:8162-70.
Saddik M, Lopaschuk GD. Myocardial triglyceride turnover during reperfusion of isolated rat hearts subjected to a transient period of global ischemia. J Biol Chem 1992;267:3825-31.
Coppack SW, Fisher RM, Gibbons GF, Humphreys SM, McDonough MJ, Potts JL, et al. Postprandial substrate deposition in human forearm and adipose tissues in vivo. Clin Sci 1990;79:339-48.
Wisneski JA, Gertz EW, Neese RA, Mayr M. Myocardial metabolism of free fatty acids. Studies with 14C-labeled substrates in humans. J Clin Invest 1987;79:359-66.
Crass MFIII. Exogenous substrate effects on endogenous lipid metabolism in the working rat heart. Biochim Biophys Acta 1972;280:71-81.
Crass MFIII, Shipp JC. Metabolism of exogenous and endogenous fatty acids in heart muscle. Rec Adv Stud Cardiac Struct Metab 1972;1:115-26.
Paulson DJ, Crass MFIII. Endogenous triacylglycerol metabolism in diabetic heart. Am J Physiol Heart Circ Physiol 1982;242:H1084-94.
O’Donnell JM, Zampino M, Alpert NM, Fasano MJ, Geenen DL, Lewandowski ED. Accelerated triacylglycerol turnover kinetics in hearts of diabetic rats include evidence for compartmented lipid storage. Am J Physiol Endocrinol Metab 2006;290:E448-55.
Crass MFIII. Heart triglyceride and glycogen metabolism: Effects of catecholamines, dibutyryl cyclic AMP, theophylline, and fatty acids. Rec Adv Stud Cardiac Struct Metab 1973;33:275-90.
Crass MFIII. Regulation of triglyceride metabolism in the isotopically prelabeled perfused heart. Federation Proc 1977;36:1995-9.
Crass MFIII, Shipp JC, Pieper GM. Effects of catecholamines on myocardial endogenous substrates and contractility. Am J Physiol 1975;228:618-27.
Goodwin GW, Taegtmeyer H. Improved energy homeostasis of the heart in the metabolic state of exercise. Am J Physiol Heart Circ Physiol 2000;279:H1490-501.
Goodwin GW, Taylor CS, Taegtmeyer H. Regulation of energy metabolism of the heart during acute increase in heart work. J Biol Chem 1998;273:29530-9.
Kerner J, Zaluzec E, Gage D, Bieber LL. Characterization of the malonyl-CoA-sensitive carnitine palmitoyltransferase (CPTo) of a rat heart mitochondrial particle. Evidence that the catalytic unit is CPTi. J Biol Chem 1994;269:8209-19.
Swanton EM, Saggerson ED. Effects of adrenaline on triacylglycerol synthesis and turnover in ventricular myocytes from adult rats. Biochem J 1997;328:913-22.
O’Donnell JM, Fields AD, Sorokina N, Lewandowski ED. The absence of endogenous lipid oxidation in early stage heart failure exposes limits in lipid storage and turnover. J Mol Cell Cardiol 2008;44:315-22.
Saddik M, Lopaschuk GD. Triacylglycerol turnover in isolated working hearts of acutely diabetic rats. Can J Physiol Pharmacol 1994;72:1110-9.
van der Vusse GJ, Glatz JFC, Stam HCG, Reneman RS. Fatty acid homeostasis in the normoxic and ischemic heart. Physiol Rev 1992;72:881-940.
Zhou YT, Grayburn P, Karim A, Shimabukuro M, Higa M, Baetens D, et al. Lipotoxic heart disease in obese rats: Implications for human obesity. Proc Natl Acad Sci USA 2000;97:1784-9.
Chiu HC, Kovacs A, Ford DA, Hsu FF, Garcia R, Herrero P, et al. A novel mouse model of lipotoxic cardiomyopathy. J Clin Invest 2001;107:813-22.
Dagenais GR, Tancredi RG, Zierler KL. Free fatty acid oxidation by forearm muscle at rest, and evidence for an intramuscular lipid pool in the human forearm. J Clin Invest 1976;58:421-31.
Hurley BF, Nemeth PM, Martin WHIII, Hagberg JP, Dalsky GP, Holloszy J. Muscle triglyceride utilization during exercise: Effect of training. J Appl Physiol 1986;60:562-7.
Wicklmayr M, Rett K, Dietze G, Mehnert H. Inhibition of muscular triglyceride lipolysis by ketone bodies: A mechanism for energy-preservation in starvation. Horm Metab Res 1986;18:476-8.
Coppack SW, Jensen MD, Miles JM. In vivo regulation of lipolysis in humans. J Lipid Res 1994;35:177-93.
Reingold JS, McGavock JM, Kaka S, Tillery T, Victor RG, Szczepaniak LS. Determination of triglyceride in the human myocardium by magnetic resonance spectroscopy: Reproducibility and sensitivity of the method. Am J Physiol Endocrinol Metab 2005;289(5):E935-9.
Kankaanpää M, Lehto HR, Pärkkä JP, Komu M, Viljanen A, Ferrannini E, et al. Myocardial triglyceride content and epicardial fat mass in human obesity: Relationship to left ventricular function and serum free fatty acid levels. J Clin Endocrinol Metab 2006;91(11):4689-95.
van der Meer RW, Hammer S, Smit JW, Frölich M, Bax JJ, Diamant M, et al. Short-term caloric restriction induces accumulation of myocardial triglycerides and decreases left ventricular diastolic function in healthy subjects. Diabetes 2007;56(12):2849-53.
van der Meer RW, Doornbos J, Kozerke S, Schär M, Bax JJ, Hammer S, et al. Metabolic imaging of myocardial triglyceride content: Reproducibility of 1H MR spectroscopy with respiratory navigator gating in volunteers. Radiology 2007;245(1):251-7.
Hammer S, van der Meer RW, Lamb HJ, Schär M, de Roos A, Smit JW, et al. Progressive caloric restriction induces dose-dependent changes in myocardial triglyceride content and diastolic function in healthy men. J Clin Endocrinol Metab 2008;93(2):497-503.
Schon HR, Schelbert HR, Robinson G, et al. C-11 labeled palmitic acid for the noninvasive evaluation of regional myocardial fatty acid metabolism with positron-computed tomography I. Kinetics of C-11 palmitic acid in normal myocardium. Am Heart J 1982;103:532-47.
Lerch RA, Bergmann SR, Ambos HD, et al. Effect of flow-independent reduction of metabolism on regional myocardial clearance of 11C-palmitate. Circulation 1982;65(4):731-8.
Fox KAA, Abendschein DR, Ambos HD, Sobel BE, Bergmann SR. Eflux of metabolized and nonmetabolized fatty acids from canine myocardium: Implication for quantifying myocardial metabolism tomographically. Circ Res 1985;57:232-43.
Lerch RA, Ambos HD, Bergmann SR, et al. Localization of viable, ischemic myocardium by positron-emission tomography with 11C-palmitate. Circulation 1981;64:689-99.
Bergmann SR, Weinheimer CJ, Markham J, Herrero P. Quantitation of myocardial fatty acid metabolism using positron emission tomography. J Nucl Med 1996;37:1723-30.
Pajevic S, Daube-Withersoppon ME, Bacharach SL, Carson RE. Noise characteristics of 3-D and 2-D PET images. IEEE Transactions on Med Imaging 1998;17:9-23.
Jesmok GJ, Warltier DC, Gross GJ, et al. Transmural triglycerides in acute myocardial ischaemia. Cardiovasc Re 1978;12:659-65.
Evans JR. Importance of fatty acids in myocardial metabolism. Circ Res 1964;14&15(Suppl II):96-106.
Nellis SH, Liedtke AJ, Renstrom B. Fatty acid kinetics in aerobic myocardium: Characteristics of tracer carbon entry and washout and influence of metabolic demand. J Nucl Med 1992;33(10):1864-74.
Palmer WK, Caruso RA, Oscai LB. Possible role of lipoprotein lipase in the regulation of endogenous triacylglycerols in the rat heart. Biochem J 1981;198(1):159-66.
Kreisberg RA. Effect of epinephrine on myocardial triglyceride and free fatty acid utilization. Am J Physiol 1966;210:385-9.
Lafontan M, Dang-Tran L, Berlan M. Alpha-adrenergic antilipolytic effect of adrenaline in human fat cells of the thigh: Comparison with adrenaline responsiveness of different fat deposits. Eur J Clin Invest 1979;9(4):261-6.
Borthne K, Langslet A, Lindberg H, Skomedal T, Osnes JB. Differential recruitment of alpha 1- and beta-adrenoceptors in inotropic control of atrial child myocardium by endogenous noradrenalin. Acta Physiol Scand 2000;170(1):21-31.
Soto PF, Herrero P, Kates AM, Dence CS, Ehsani AA, Dávila-Román V, et al. Impact of aging on myocardial metabolic response to dobutamine. Am J Physiol Heart Circ Physiol 2003;285(5):H2158-64.
Acknowledgments
This study was supported by NIH grants HL-69100. We thank Margaret Morris and Paul Eisenbeis for their technical assistance, and anonymous reviewer #1 whose thorough comments resulted in more interesting article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kisrieva-Ware, Z., Coggan, A.R., Sharp, T.L. et al. Assessment of myocardial triglyceride oxidation with PET and 11C-palmitate. J. Nucl. Cardiol. 16, 411–421 (2009). https://doi.org/10.1007/s12350-009-9051-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-009-9051-7