
Abstract
Schools can play a significant role in promoting timely access to mental health services by utilizing proactive approaches to identifying and supporting students’ social, emotional, and behavioral needs. However, recent data suggest that few schools in the USA are taking such proactive approaches. Given that implementation of school-based programs is determined by a complex interplay of influences at multiple levels (i.e., individual, innovation, environment), more research is needed to understand the perceptions of stakeholders representing each of these unique levels. The purpose of this study was therefore to compare stakeholders’ knowledge, beliefs, and opinions regarding school-based approaches to identifying and supporting students at risk of SEB challenges. Survey responses were obtained from district administrators, school building administrators, school support staff, teachers, and parents within 1330 school districts across the USA. Although some differences across groups were noted, patterns generally supported that stakeholders (a) reported being knowledgeable about social, emotional, and behavioral problems and the school-based approaches to identifying and assessing them, (b) believed that student social, emotional, and behavioral problems should be a prioritized concern and identified using screening procedures, and (c) perceived moderate amounts of pressure to change social, emotional, and behavioral screening practices from different sources in their communities. In addition, respondents across stakeholder groups reported consistently strong agreement that screening should be used to proactively identify not only which students are exhibiting internalizing/externalizing problems, but also which students possess various risk and resilience factors.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Estimates indicate that as many as 20% of children and adolescents struggle with mental health disorders and that nearly half of these disorders begin in early adolescence (World Health Organization, 2011). Although research has unfortunately documented a large percentage of youth with unmet mental health needs in the USA (e.g., Simon, Pastor, Reuben, Huang, & Goldstrom, 2015), it has been argued that schools can play a significant role in reducing these disparities by utilizing proactive approaches to identifying and supporting students’ social, emotional, and behavioral (SEB) needs (Levitt, Saka, Romanelli, & Hoagwood, 2007). Given that over 90% of children attend public schools in the USA, school-based mental health professionals come into contact with the majority of the youth population on a daily basis (Romer & McIntosh, 2005). If those students who are at risk of significant SEB problems can be identified early on—before problems are allowed to compound and crystallize—there exists a much greater likelihood of preventing negative life outcomes (Bradley, Doolittle, & Bartolotta, 2008).
One approach to the proactive identification of students with SEB needs that have gained increased attention over the past decade is the use of universal SEB screening. In contrast to relying on teachers to refer students after significant problems have already arisen, universal screening involves assessing all students on a regular basis to proactively identify any SEB concerns. The use of universal screening has been advocated at the federal level, both by experts (e.g., New Freedom Commission on Mental Health, 2003; US Public Health Service, 2000) and within legislation (e.g., Individuals with Disabilities Education Act, 2004). In addition, as of 2015, roughly half of state departments of education provided local education agencies with guidance surrounding the implementation of universal screening to identify students with some level of SEB risk (Briesch, Chafouleas, & Chaffee, 2017). However, despite multiple calls to implement SEB screening in school-based settings as part of a full continuum of prevention efforts, actual implementation remains discouragingly low (i.e., 9–13%; Dineen et al., 2019; Bruhn, Woods-Groves, & Huddle, 2014), supporting the need to explore potential explanations for why it is not being conducted.
Over the years, various theoretical models have been put forth to understand which factors help to predict sustained use of evidence-based innovations (i.e., interventions, assessments); however, many acknowledge that usage may best be understood by simultaneously considering variables at the levels of the individual, innovation, and environment (Sanetti & Kratochwill, 2009). Individual-level variables are those that are internal to the potential implementer and include factors such as how acceptable an individual finds an innovation to be or how willing the individual is to try something new. Variables specific to the innovation, on the other hand, include how complicated an innovation appears, how much time it will take to implement, or how effective it is perceived to be. Finally, environmental influences include whether there is sufficient support (e.g., logistical, philosophical) for usage and whether the innovation fits within the existing context. Although individual factors may exert more or less influence in a given situation, it has been argued that consideration should be given to each in examining the research to practice gap (Briesch, Chafouleas, Neugebauer, & Riley-Tillman, 2013).
Individual-Level Influences on Implementation
At the most proximal level, usage of a program or tool may be influenced by the degree to which the individuals charged with implementation understand and are accepting of the technology (Briesch et al., 2013). Critical school-based implementers of SEB screening include classroom teachers as well as student support staff (e.g., school psychologists, school social workers). To date, no studies have specifically explored the perspectives of teachers or student support staff regarding SEB screening; however, there does exist research to suggest that comfort and confidence in the SEB domain are far from achieved.
Over the years, several studies have examined teachers’ beliefs and attitudes related to SEB concerns and addressing these concerns in schools. Teachers in some surveys have reported believing that schools should work to address student mental health needs (Reinke et al., 2011), and that addressing mental health needs was a critical part of their jobs (Roeser & Midgley, 1997; Rothi et al., 2008). At the same time, however, other studies have highlighted that some teachers perceive that addressing mental health issues detracts from the learning that should be happening in the classroom and do not see this as part of their role responsibility (Graham et al., 2011). Researchers have also identified a lack of perceived knowledge to address SEB concerns as an implementation barrier. Roughly two-thirds of elementary teachers in one study reported that they felt overwhelmed by students’ mental health needs (Roeser & Midgley, 1997), and teachers have consistently noted a lack of training to address mental health concerns in the classroom to be a problem (Reinke et al., 2011; Walter, Gouze, & Lim, 2006). Similar findings have been noted in studies of school support staff including school psychologists (Power, Bower, Webber, & Martinson, 2010) and school nurses (Pryjmachuk, Graham, Haddad, & Tylee, 2011), with both groups reporting concerns about their ability to adequately serve students with SEB needs. Taken together, the research conducted to date seems to suggest that much work is needed to improve the confidence of teachers and student support staff in addressing student SEB problems. Further exploration must be conducted, however, to understand whether these hesitancies similarly extend to the realm of SEB assessment.
Innovation-Level Influences on Implementation
Although knowledge and beliefs are important in influencing usage, theoretical models also emphasize practical considerations related to a program or tool, including how feasible the procedures are believed to be (Briesch et al., 2013). Several hypotheses have been put forth to explain the underutilization of SEB screening procedures, including both logistical (e.g., resources needed) and philosophical (e.g., concerns about misidentification) concerns (National Research Council and Institute of Medicine; NRCIM, 2009). To date, however, the only study to directly assess perceived barriers was a survey study of 454 school personnel conducted by Bruhn and colleagues (2014). These authors found that nearly 90% of school districts reported that they did not conduct SEB screening. When asked to specify the reasons why screening was not being conducted, respondents most frequently endorsed that (a) they were unaware that this type of screening was conducted, (b) the financial costs were prohibitive, and (c) they did not have access to appropriate screening measures. Although some degree of overlap was identified with those barriers previously hypothesized, one particularly notable finding was the lack of knowledge regarding SEB screening reported by over one-third of respondents in Bruhn et al.’s (2014) study, suggesting that education and access may be a primary—and potentially overlooked—barrier to implementation.
Environmental Influences on Implementation
Although individual- and innovation-level variables may have the most direct influence on implementation, school-based programs are not carried out in the vacuum of a classroom. Rather, staffs are nested within schools, districts, and communities, and are therefore subject to broader contextual factors (Greenberg et al., 2005). Administrators often serve as the gatekeepers in determining whether a program is introduced into a school building (Han & Weiss, 2005). If a practice or program is believed to be aligned with the district priorities, district administrators are more likely to allocate resources toward it to enhance the likelihood of success (Greenberg et al., 2005). School building administrators, on the other hand, are typically the ones who provide training to teachers and allocate time in the schedule for implementing programs or practices (Han & Weiss, 2005). Additionally, research has shown that administrators’ attitudes toward (Gottfredson & Gottfredson, 2002), and support for (Kam, Greenberg, & Walls, 2003), a program may significantly influence both program implementation and effectiveness. Stakeholders have therefore stressed the importance of having strong administrator buy-in at both the school and district levels in order for new mental health initiatives to be successful (Mendenhall, Iachini, & Anderson-Butcher, 2013).
Although far less is known about administrators’ attitudes and knowledge than those of teachers, some recent research has begun to explore the perspectives of school principals regarding youth and adolescent mental health needs. Preliminary findings have been consistent with surveys of teachers, indicating that across grade levels (i.e., elementary, middle, and high school), principals identified student behavioral and mental health as the greatest area of student need (Iachini, Pitner, Morgan, & Rhodes, 2015). Further, school leaders believed that unaddressed student mental health needs impact both individual students’ ability to be successful in school and overall school functioning (Blackman et al., 2016). However, although elementary principals have articulated a strong need for professional development related to student mental health (Frabutt & Speach, 2012), little is known about where this need specifically lies. Additional research is therefore needed in order to explore administrators’ perceptions of how best to identify and support students’ SEB needs.
Finally, in addition to within-school influences, it is also important to consider community-level influences on implementation. Sociopolitical priorities help to determine what policies and priorities exist at the district and school levels (Han & Weiss, 2005), and support from legislators and community agencies may be needed in order to implement a program (Greenberg et al., 2005). However, one critical stakeholder group when considering the implementation of school-based SEB supports is families. Although some studies have found that parents are supportive of school mental health promotion and intervention efforts (e.g., Wegmann, Powers, & Blackman, 2013), fear concerning stigma has been identified as one of the central barriers to families seeking help for mental health concerns (Murry, Heflinger, Suite, & Brody, 2011). Additionally, research involving adult populations has found both the positive attitudes (Greenley, Mechanic & Cleary, 1987) and negative responses (Leaf, Bruce, & Tischler, 1987) of family members to be predictive of mental health treatment use.
Purpose of Study
Although SEB screening has been advocated as a way to identify and support struggling students before problems escalate, recent survey studies suggest that very few schools are implementing these practices (Dineen et al., 2019; Bruhn et al., 2014). Given that the success of school-based efforts to address student SEB needs depends on the buy-in and commitment of multiple stakeholders (Greenberg et al., 2005) and is determined by a complex interplay of influences at multiple levels (i.e., individual, innovation, environment), more research is needed to understand the perceptions of stakeholders representing each of these unique levels. The purpose of this study was therefore to compare stakeholders’ knowledge and beliefs regarding school-based approaches to identifying and supporting students at risk of SEB challenges. Specifically, we sought to answer the following research questions:
- 1.
How knowledgeable do stakeholders report feeling regarding SEB problems and the school-based approaches to identifying and assessing them? Does reported knowledge differ across stakeholder groups?
- 2.
To what extent do stakeholders believe that SEB problems are a concern that should be addressed in schools? Do reported beliefs differ across stakeholder groups?
- 3.
To what extent do stakeholders perceive that there is pressure to change school-based screening from different sources in their communities? Do perceptions differ across stakeholder groups?
- 4.
Which particular behaviors or risk factors do stakeholders believe schools should screen for the presence of in school settings?
- 5.
What approaches do stakeholders believe schools should take to identifying and supporting the SEB needs of students?
It was hypothesized that differences would exist with regard to reported knowledge and beliefs, given the varied levels of preparation across stakeholder groups for addressing student SEB concerns. For example, it was anticipated that school support staff would report higher levels of knowledge and stronger beliefs regarding the importance of addressing SEB problems than teachers or parents. Additionally, it was hypothesized that school-based stakeholders would be more likely to endorse the use of screening procedures to identify a range of SEB concerns than parents/guardians given concerns raised by families regarding potential stigmatization.
Methods
Data for this study were collected as part of a larger survey project designed to explore the current status of school-based SEB assessment and intervention practices. School districts were identified for participation using the 2013–14 Common Core of Data Local Education Agency Universe Survey (National Center for Education Statistics, 2013–14), a federally maintained database of all public elementary and secondary schools in the USA. An invitation to participate in the overall project was sent to all eligible district superintendents (n = 12,132). Eligible districts included both regular local school districts and those that were part of a supervisory union in which more than 100 students were enrolled (thus excluding special districts such as those affiliated with a special population, charter schools, virtual schools, etc.). Once district approval was obtained, the first survey was sent to a district-level administrator who was most familiar with the SEB assessment and intervention practices in the district (e.g., Superintendent, Director of Special Education). Completion of the district-level survey subsequently prompted the random selection of one elementary (i.e., lowest grade = PK-4, highest grade = PK-8) and one secondary (lowest grade = 5–12, highest grade = 5–12) level school within the district. School building administrators (e.g., Principal, Assistant Principal) were then asked to (a) complete a building-level survey, (b) provide contact information for a student support personnel (e.g., school psychologist, school social worker) who would complete their own survey, and (c) distribute a survey link to all teachers and parents/guardians in the building. Any respondents who completed the surveys were eligible to participate in a raffle to win an Amazon gift card. Complete information regarding the project methodology appears in Marcy et al., (2018).
All survey responses were collected between December 2015 and December 2016. Although 1330 district administrators responded to the initial survey, participation from the other four stakeholder groups was highly variable across districts. That is, although substantial numbers responded within each stakeholder group (i.e., 495 school building administrators, 320 school support staff, 1652 teachers, 3243 parents), not every district had respondents from all groups. The sample of 1330 school districts comes from the Northeast (34%), Midwest (35%), South (19%), and West (12%). Two-thirds of participating districts served between 1001 and 5000 students (46%) or 5001–15,000 students (25%), with lesser representation of districts serving 100–500 (13%), 501–1000 (11%), and 15,001 or more (5%) students.
Materials
The research team developed five survey measures within the larger project to understand both the current status of SEB practices in schools, as well as the knowledge and beliefs of key stakeholders related to student SEB concerns and the options for addressing them. These surveys were developed through a multistage process. First, item content was generated based upon a review of the literature as well as input from experts in the fields of school mental health. Draft measures were next shared with an Advisory Board comprised of individuals with expertise in school-based assessment, educational policy, implementation science, and youth mental health. The Advisory Board members were asked to provide feedback with regard to both the item content and wording, which was used to drive revisions to the measures. Next, the survey measures underwent cognitive testing to identify any potentially unclear questions, response options, or language within the surveys. Members of the research team conducted cognitive interviews with a total of three district administrators, four school building administrators, six student support staff, six teachers, and six parents across both elementary and secondary levels. Feedback from the cognitive interviews was used to inform any final edits to the measures.
As previously noted, all respondents completed online surveys specifically tailored to their role within the school district (i.e., district administrator, school building administrator, student support staff, teacher, and parent). As such, the content and length of each survey varied across stakeholder groups. For example, although both administrators and student support staff reported on current assessment practices employed within the district or school, parent and teacher surveys did not include these questions (for complete surveys, see Authors, 2018). As the goal of the current paper was to compare reported knowledge and beliefs across stakeholder groups, only those survey items included across all five stakeholder surveys are described here.
All stakeholder groups completed three sections of the survey. The first section (19 items) addressed stakeholders’ knowledge and beliefs regarding SEB problems, in general, and SEB screening, in particular (see Table 1 for example items). Within the second section of the survey, all respondents were asked one question about what approach they personally believed that schools should take to identifying and supporting the SEB needs of students. Five different SEB identification approaches were offered (see Table 2 for descriptions), which were randomized in the online survey by participant to minimize presumed desirability of any given approach. If respondents favored an alternative approach or were not sure of what approach schools should take, they could indicate this as well. The final section of the survey explained that some schools are now screening for SEB problems in a similar way to how schools have traditionally screened for physical health issues like scoliosis (i.e., assessing all students to identify those at risk). Across 17 items, respondents were then asked to indicate the degree to which they believed schools should screen for either problems or resilience factors.
Data Analysis
In order to draw meaningful and dependable comparisons across stakeholder groups, we conducted exploratory factor analyses using SPSS 25.0 in order to reduce the items within Sections 1 and 3 of the survey into a smaller number of dimensions. Factor analyses were conducted using the full survey sample (i.e., 7040 respondents). Subsequent to ensuring that the matrix was factorable (i.e., Kaiser–Meyer–Olkin measure of sampling adequacy = 0.90; Bartlett’s test of sphericity χ2(171) = 65,086.22, p < 0.001), the correlation matrix was examined for evidence of multicollinearity (i.e., inter-item correlations above 0.80) and the table of communalities was reviewed to identify any values below 0.30 (which would indicate minimal relatedness with other items). This step resulted in two items being identified as problematic and therefore deleted. The remaining 17 items were subjected to principal axis factoring with an oblimin rotation given that the factors were expected to correlate. Both (a) review of the eigenvalues and scree plot and (b) results of parallel analysis suggested the presence of three primary factors. All 17 items were found to load strongly (i.e., pattern coefficient above 0.45) on one primary factor, and descriptions of these subscales are presented in Table 1.
A similar factor analytic process was followed in order to reduce the item content within the third section of the survey after determining that the item matrix was factorable (Kaiser–Meyer–Olkin measure of sampling adequacy = 0.92; Bartlett’s test of sphericity χ2(136) = 87,014.24, p < 0.001. The 17 items were screened for evidence of multicollinearity or low communalities; however, no items were identified to be problematic. Again, the eigenvalues, scree plot, and results of parallel analysis suggested the presence of three primary factors and all items were found to load strongly (see Table 1 for descriptions of these factors).
With the six factors described in Table 1 (i.e., Knowledge, Beliefs, Pressure, Psychopathology, Competence, and Abuse), we sought to determine whether statistically significant differences existed in mean scores on these factors across stakeholder groups for the full survey sample of 7040 respondents in 1330 districts. The respondents included 1330 district administrators (19%), 495 building administrators (7%), 3243 parents (46%), 320 school support staff (5%), and 1652 (23%) teachers.
To determine whether statistically significant differences existed on the latent factors across stakeholder groups, we employed a Multiple Indicators Multiple Causes (MIMIC) model (Hauser & Goldberger, 1971; Jöreskog & Goldberger, 1975). The MIMIC model, a special type of structural equation model (Bollen, 1989), evaluates mean group differences between the stakeholder groups. The MIMIC model used in this study is essentially a multivariate analysis of covariance (MANCOVA) design because we are testing the mean differences across five groups on six dependent variables simultaneously controlling for district size, district census region, and the percent of nonwhite students in the district. The MIMIC model approach with the factors regressed on the covariate causes, including the group membership dummy variables with district administrator as the reference group, allows for testing group differences on the six factors which is analogous to simultaneous dummy variable regressions (Kaplan, 2001).
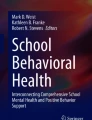
The MIMIC model includes two pieces: a measurement model and a structural model. The measurement model describes the relationships between each of the six factors and their indicators. The structural model specifies a set of regressions for each of the covariates in the model which are assumed to influence the latent factors. The covariates in the MIMIC model include stakeholder group (with district administrators as the reference group), district census region (with Midwest as the reference group), district size, and the percentage of nonwhite students in the district. A depiction of the MIMIC model can be seen in Fig. 1.

Multiple indicators multiple causes model for this study. e1–e24 are the measurement errors in the model. Press. pressure, Comp. competence, Psych. psychopathology, Know. knowledge
Given the MANCOVA design, and the interest in comparing mean differences across each of the stakeholder groups on each of the six factors in Table 1, a series of omnibus tests are employed to control the familywise error rate (Maxwell & Delaney, 2004). First, a MANCOVA omnibus test using the Wald chi-squared test is performed in Mplus (Muthén & Muthén, 2017). This multivariate omnibus test evaluates whether all the stakeholder means are equal across all six factors. This multivariate omnibus is followed by six univariate (one for each of the latent factors) analysis of variance (ANOVA) omnibus tests using the Wald chi-squared test in Mplus (Muthén & Muthén, 2017). If each of these tests is statistically significant, it provides protection against inflation of the familywise Type I error rate, and post hoc multiple comparisons across each of the stakeholder groups on the six factors can be evaluated (Maxwell & Delaney, 2004).
Prior to fitting the MIMIC model, the measurement model for this study was evaluated using confirmatory factor analysis (CFA; Brown, 2006). The CFA for the measurement model and the MIMIC model were conducted in Mplus Version 8 using weighted least square mean variance (WLSMV) estimator (Muthén & Muthén, 2017). The WLMSV estimator is used due to the ordinal Likert scale of the indicators in the measurement model. Measures of goodness of fit that was used in this study were the root mean square error of approximation (RMSE), and the comparative fit index (CFI), the Tucker–Lewis Index (TLI).Footnote 1 The three indices, for which there is considerable disagreement, are considered as demonstrating adequate fit when the RMSEA ≤ 0.05 and the CFI and TLI are greater than ≥ 0.95 (Hu & Bentler, 1999). The chi-square tests of model fit are reported. The chi-square tests are known to be influenced by sample size and model fit (Cheung & Rensvold, 2002).
Although a maximum of two school building administrators and two student support staff could participate within each district (i.e., one elementary, one secondary), the number of teacher and parent respondents varied widely across included districts. The mean number of participating teachers within each district was 9.23 (SD = 7.96), whereas the mean number of participating parents was 29.75 (SD = 32.00). To ensure that comparisons across stakeholder groups and districts were meaningful (i.e., not overly influenced by the sample size of one particular group/district), we used the Mplus TYPE = Complex option to obtain correct standard errors and a chi-square test of model fit taking into account clustering within district (Muthén & Muthén, 2017).
There was approximately 1% of missing data in this study. There were only 10 cases with missing on the covariates and 61 cases with missing on the indicators. The WLMSV approach handles missing data with a pairwise present approach (Asparouhov & Muthén, 2010). The pairwise present approach allows all observations to be used when estimating correlations.
Results
The measurement model had 34 indicators or observed variables for the six factors. The measurement model also included nine observed variables for the covariates that correlate freely with the six latent variables: percent nonwhite, district size, three dummy variables for district census region, and four dummy variables for building administrator, school support staff, teachers, and parents. The goodness of fit indices for the measurement model are reported in Table 3. The goodness of fit indices provide evidence of adequate model fit according to the CFI/TLI (0.977/0.974) and RMSEA (0.035). The chi-square was statistically significant, χ2 (800) = 7886.707, p < 0.01. The results of the measurement model are not depicted here; however, we do note that standardized loadings ranged from 0.77 to 0.84 for Knowledge, 0.65–0.84 for Beliefs, 0.77–0.867 for Pressure, 0.78–0.84 for Psychopathology, 0.72–0.84 for Competence, and 0.81–0.97 for Abuse.
The goodness of fit indices for the MIMIC model in Fig. 1 are also in Table 3. The fit indices provide evidence of adequate model fit according to the CFI/TLI (0.977/0.973) and RMSEA (0.036). The chi square was statistically significant, χ2(764) = 7780.78, p < 0.01. The results of the MIMIC model are reported in Table 4. The multivariate Wald test was statistically significant (χ2 = 561.832, df = 18, p < 0.01). The six univariate Wald test for the knowledge (χ2 = 140.907, df = 3, p < 0.01), Beliefs (χ2 = 14.864, df = 3, p < 0.01), Pressure χ2 = 235.023, df = 3, p < 0.01), Psychopathology χ2 = 12.101, df = 3, p < 0.01), Competence (χ2 = 24.081, df = 3, p < 0.01), and Abuse (χ2 = 30.716, df = 3, p < 0.01) dependent variables were each statistically significant (Wald test results in parenthesis). Given that the MIMIC model used district administrators as the reference group for the dummy variables, post hoc multiple comparison contrasts between all the other pairs of stakeholder groups were computed and these are reported in Table 5. The group differences for the six factors are also shown in Fig. 2 with error bars. The correlations among the latent factors are reported in Table 6. For the results reported below, only standardized coefficients for statistically significant effects are reported in text. The R-squared for the latent factors were Knowledge (R2 = 0.04), Beliefs (R2 = 0.02), Pressure (R2 = 0.09), Psychopathology (R2 = 0.02), Competence (R2 = 0.01), and Abuse (R2 = 0.02) and are reported in Table 4.

Group differences on the six latent factors reported with standard error bars. The mean of the group on the right-hand side of the dash is subtracted from the mean of the group on the left-hand side of the dash. BLD building administrators, DST district administrators, PAR parents, SSS school support staff, TCH teachers. Standardized differences are reported
Stakeholder Knowledge of SEB Problems
From the MIMIC model, a number of differences across the stakeholder groups become apparent. In standardized coefficients, from Tables 4 and 5, we can see that school support staff reported greater knowledge of SEB problems than district administrators (β = 0.49), building administrators (β = − 0.60),Footnote 2 parents (β = − 0.87), and teachers (β = 0.81). Additionally, both teachers and parents reported less knowledge than district administrators (Teachers: β = − 0.31; Parents: β = − 0.36) or school building administrators (Teachers: β = − 0.21; Parents: β = − 0.27).
Mean item responses on the items associated with the knowledge factor are shown in Table 7. Although most mean responses indicated strong levels of reported knowledge, reported agreement was in the moderate to strong range concerning the options for treating SEB problems (range 3.18–4.08), options for preventing SEB problems (range 3.15–3.89), and the approaches to SEB assessment (range 3.06–3.86), but in the strong to complete range for knowledge of the effects of SEB problems on student success (range 4.13–4.54).
Stakeholder Beliefs Regarding SEB Problems
From the MIMIC model, we see there are several statistically significant differences between the stakeholder groups in terms of beliefs regarding SEB problems. Again, in terms of standardized coefficients from Tables 4 and 5, we see school support staff reporting stronger beliefs regarding SEB problems than district administrators (β = 0.33), school building administrators (β = − 0.37), parents (β = − 0.27), and teachers (β = 0.21). Teachers also reported having stronger beliefs regarding SEB problems than district administrators (β = 0.12) and school building administrators (β = − 0.15). There were no other statistically significant differences between the remaining stakeholder groups.
Mean responses for each belief item are presented across stakeholder groups in Table 8. Stakeholders reported consistently strong agreement that student SEB problems are a concern (range 4.45–4.63), addressing them should be a priority (range 4.47–4.75), and that including SEB screening procedures is an important step toward addressing SEB problems at school (range 4.08–4.33).
Stakeholder Pressure to Change
From the MIMIC model, in terms of standardized coefficients from Tables 4 and 5, we can see that parents reported greater perceived pressure to change than district administrators (β = 0.52), building administrators (β = − 0.61), school support staff (β = 0.75), and teachers (β = 0.58). Besides parents, the only other statistically significant group differences were found with respect to school support staff, who reported less perceived pressure to change than both district administrators (β = − 0.20) and teachers (β = − 0.17). There were no other statistically significant differences between the remaining stakeholder groups.
The mean responses for each pressure to change item are presented across stakeholder groups in Table 9. Although pressure was perceived to be fairly modest across most stakeholders and sources (i.e., roughly a mean score of 3 on a 1–5 scale), the four school-based stakeholder groups perceived there to be notably less pressure from local political leaders (range 1.84–2.18) than from school personnel (range 3.04–3.68) or community members (range 2.43–3.42).
Appropriate Screening Targets
Finally, respondents were asked to indicate whether they believed that schools should screen for the presence of particular behaviors or risk factors. As indicated earlier, the items in this section assessed three underlying constructs: internalizing/externalizing problems, competence/resilience factors, and abuse/neglect. The MIMIC model provided several insights into stakeholder beliefs regarding appropriate screening targets (see Tables 4, 5). Although the two administrator groups (i.e., district, school building) reported consistent beliefs concerning what schools should screen for, notable differences were identified across the other three stakeholder groups. First, school support staff, teachers, and parents were all more likely to report that schools should screen for internalizing/externalizing behaviors than building administrators (Support staff: β = − 0.23; Teachers: β = − 0.23; Parents: β = − 0.23) or district administrators (Support staff: β = 0.32; Teachers: β = 0.31; Parents: β = 0.32). Second, teachers were less likely to report that schools should screen for indicators of competence than student support staff (β = − 0.30) or parents (β = − 0.16), and district administrators were similarly less likely to endorse screening for competence than school support staff (β = 0.28) or parents (β = 0.14). Finally, parents were more likely to report that schools should screen for abuse than district administrators (β = 0.33), school building administrators (β = − 0.32), and student support staff (β = 0.33). Teachers were similarly more likely to report that abuse should be screened for than district administrators (β = 0.27), building administrators (β = − 0.26), and student support staff (β = − 0.27).
Table 10 provides further insight into these data. The values in the table represent the proportion of respondents that indicated schools definitely should screen for a particular problem/construct. As can be seen, there was some variability within each overall category. The majority of respondents—regardless of stakeholder group—indicated that schools should definitely screen for the presence of internalizing behaviors (range 63–78%), the presence of aggressive or violent behavior (range 59–76%), and whether a student has experienced emotional, physical, or sexual abuse (range 69–80%). Endorsements were more mixed with regard to the appropriateness of screening for inattentive/hyperactive behavior and defiance, with administrators endorsing these behaviors less commonly (range 48–54%) than student support staff, teachers, and parents (range 58–66%). Finally, strong endorsement was least common when respondents were asked to consider screening for indicators of student competence or resilience. For example, less than half of respondents across all five stakeholder groups indicated that schools should definitely screen for whether students have a belief that somehow life will work out well.
Contextual Factors
Controlling for district size, census region, and percent nonwhite students allowed for the exploration of contextual factors influence on the six factors in this study. The results indicated that there were a few differences by district region. For instance, the results indicate that respondents from the Southern US had lower beliefs regarding SEB problems (β = − 0.18) and perceived there as being less pressure to change SEB screening practices (β = − 0.16) than respondents from the Midwest. Those in the West were also more likely to report lower pressure to change than the Midwest (β = − 0.08). The percent of nonwhite students in the district was only found to influence pressure to change (β = 0.19), with those districts with greater percentages of nonwhite students reporting greater perceived pressure to change. District size was modestly positively related to knowledge of SEB problems (β = 0.05), beliefs regarding SEB (β = 0.09), and screening for competence (β = 0.04), with larger districts reporting greater levels of knowledge, stronger beliefs, and stronger beliefs that schools should screen for competence and resilience factors.
Relationships Among Six Factors
From the table of correlations among the six factors in this study in Table 6, we can see that in general those respondents with higher reported levels of knowledge also reported higher levels of beliefs (ρ = 0.37). Those with stronger beliefs about SEB problems were also more likely to believe that schools should screen for psychopathology (ρ = 0.46), competence (ρ = 0.41), and abuse (ρ = 0.33). Perceived pressure to change was not found to be strongly correlated with any of the other factors. There were also strong correlations between respondents’ endorsements of different screening targets. That is, those who endorsed screening for indicators of psychopathology were also likely to endorse screening for competence (ρ = 0.70) and abuse (ρ = 0.57), and those who endorsed screening for competence were more likely to endorse screening for abuse (ρ = 0.40).
Ideal Approach to Identifying Students with SEB Risk
Lastly, respondents were asked to indicate which of the five primary approaches to identifying and supporting the SEB needs of students they believed that schools should take (see Table 11). The two most popular endorsements across all five stakeholder groups were for the use of universal screening (range 32–42%) or for referral of at-risk students to an internal support team (range 25–41%). Modest support was provided for the use of targeted screening (range 9–12%) and for encouraging teachers to independently develop interventions (range 6–10%). The proportions of respondents endorsing the use of external referral were found to be very low (range 2–7%).
Discussion
Population studies have consistently demonstrated that a large percentage of youth with mental health needs do not receive appropriate services (e.g., Simon et al., 2015). Given that over 90% of children under the age of 10 attend school, there is great potential for schools to play a role in identifying struggling students early through universal screening and providing them with the supports necessary to alter negative trajectories (Romer & McIntosh, 2005). However, the success of school-based efforts to address student SEB needs is largely dependent on the buy-in and commitment of multiple stakeholders (Greenberg et al., 2005). Although prior surveys have sought to understand teachers’ perceptions of SEB problems (e.g., Reinke et al., 2011; Rothi et al., 2008), decidedly less is known regarding the viewpoints of other critical stakeholders. The current study therefore sought to compare stakeholders’ knowledge and beliefs regarding SEB problems and school-based approaches to identifying them. Although some statistically significant differences were identified across stakeholder groups, patterns generally supported that stakeholders (a) reported being knowledgeable about social, emotional, and behavioral problems and the school-based approaches to identifying and assessing them, (b) believed that student social, emotional, and behavioral problems should be a prioritized concern and identified using screening procedures, and (c) perceived moderate amounts of pressure to change social, emotional, and behavioral screening practices from different sources in their communities.
Prior research has found that both teachers (e.g., Reinke et al., 2011) and administrators (e.g., Iachini et al., 2015) are greatly concerned about student SEB problems, and results of the current study echoed these concerns across stakeholder groups. Although student support staff and teachers’ reported beliefs were significantly stronger than both groups of administrators, it is notable that all mean scores fell at or above a 4.00, suggesting widespread agreement than SEB problems are a concern that should be prioritized and addressed using proactive methods of identification. Also of interest was the fact that larger districts reported stronger beliefs than smaller districts. Although there is not a perfect correspondence, urban schools tend to be larger in size than suburban or rural schools, and also to have higher percentages of students living in poverty as well as exhibiting behavior problems (Lippman, Burns, & McArthur, 1996). These factors may help to explain why larger schools are more likely to view student SEB problems as a concern that needs to be addressed.
Another notable finding was that all stakeholder groups reported fairly high levels of knowledge about SEB problems, including their causes, impacts, and approaches to identifying and addressing them. Student support personnel reported higher levels of knowledge than any other group, which was not necessarily surprising given their specialized training. What was both unexpected and encouraging, however, were the higher levels of knowledge reported by other school personnel in the current study. Previous survey studies have found that both teachers (e.g., Reinke et al., 2011; Walter et al., 2006) and principals (e.g., Frabutt & Speach, 2012) feel that they need additional training to effectively address SEB problems in the schools. Although respondents were not asked about their self-efficacy for addressing SEB problems in the current study, responses from district administrators, building administrators, and teachers did indicate knowledge of not only the causes, signs, and prevalence of SEB problems, but of the options for identifying and treating these problems as well. Although knowledge does not inherently lead to appropriate action, educators’ understanding of the nature of SEB problems is a critical cornerstone of an effective school mental health program (US Public Health Service, 2000). In contrast, parents reported significantly lower levels of knowledge than any of the other stakeholder groups, suggesting that parental education in this realm may be important.
When stakeholders were asked what approach they believed schools should take to identifying and addressing SEB problems, the overwhelming majority of respondents indicated the responsibility fell with the school as opposed to something that should be referred externally. The use of universal screening was most strongly endorsed by student support staff and parents, whereas both groups of administrators and teachers more strongly endorsed referring students to an internal support team. Given that multidisciplinary consultation teams have been in place in schools for several decades and have demonstrated effectiveness in improving both academic and behavioral outcomes, it is not surprising that these groups endorsed the use of internal referral (Chalfant, Pysh, & Moultrie, 1979). Potential reasons why administrators and teachers may be somewhat less interested in implementing universal screening have been suggested in prior literature. For example, district administrators have highlighted resource constraints involved in screening (e.g., financial costs, availability of materials) (Bruhn et al., 2014) and concerns regarding reduced input on the part of teachers have also been raised (NRCIM, 2009).
In light of the low rates of SEB screening implementation identified in prior work (i.e., 9–13% of schools; Dineen et al., 2019; Bruhn et al., 2014), we were curious to know the extent to which stakeholders perceived pressure to change the practices used to identify and support students with SEB needs within their local communities. Interestingly, parents perceived there to be stronger levels of pressure to change practices than any of the other stakeholder groups. Although statistical comparisons could not be made based on individual items, examination of the item descriptives seems to suggest that whereas parents perceive pressure as coming from both the school and local communities, school staff feel that pressure is exerted more strongly from within. This raises the question of whether schools are regularly soliciting input from families and communities regarding what supports they believe are necessary for students. An additional finding of interest was the fact that there were higher levels of perceived pressure to change practices within those school communities that were more racially and ethnically diverse. Although further exploration is needed, this perceived pressure may be linked to the problems noted with disproportionality in the use of exclusionary discipline practices between students from majority and minority backgrounds (US Department of Education Office for Civil Rights, 2016).
More than one interesting finding emerged when stakeholders were asked what behaviors and risk factors they believed that schools should include in screening. First, endorsements were consistently high across both broad constructs and individual items. In most cases, over half of respondents indicated that schools definitely should screen for a particular concern, and in some cases, percentages were upwards of 70% (e.g., anxiety/depression, physical abuse or neglect). When school districts have indicated use of SEB screening (Bruhn et al., 2014), they have been most likely to report using tools designed to identify the presence of internalizing and/or externalizing problems, such as the Behavior Assessment System for Children-3 Behavioral and Emotional Screening System (Kamphaus & Reynolds, 2015) or the Student Risk Screening Scale (Drummond, 1994). Current data suggest, however, that there is also interest in screening for both student strengths and risk factors, thereby potentially warranting the need to educate stakeholders on the broader range of screening tools available for use in schools (e.g., Moore et al., 2015).
Second, although levels of endorsement for screening were found to be fairly high across behavioral targets, there were a couple of differences across stakeholder groups worth noting. For one, district administrators were less likely to endorse screening across constructs (i.e., internalizing/externalizing, competence/resilience, abuse). Although the reasons for this were unfortunately not explored, barriers to screening identified by administrators in a prior study included the availability of materials and costs involved (Bruhn et al., 2014). Such findings do raise some concern, given that administrators’ philosophical and logistical support for a program may determine whether it is ultimately implemented (e.g., Gottfredson & Gottfredson, 2002; Kam, Greenberg, & Walls, 2003). Additionally, it was notable that levels of support for screening among parents were higher than anticipated, whereas it has been hypothesized that fears related to stigmatization identified in prior research (e.g., Murry et al., 2011) would make parents more reticent to endorse school-based screening, this was not evidenced in the data. In fact, parents were significantly more likely to endorse screening for competence/resilience factors than teachers and for indicators of abuse than administrators or student support staff.
Limitations and Directions for Future Research
Results of the current study help to advance our understanding of what stakeholders know and believe about school-based efforts to identify and support student SEB needs; however, limitations of this study should be noted.
First, because there was a great deal of variation in terms of the number of respondents within each stakeholder group, we chose to adjust the standard errors in the MIMIC model using the TYPE = COMPLEX procedure in Mplus. The procedure allowed us to account for differences in cluster sizes and obtain clustered standard errors. Although this allowed us to make more balanced comparisons across districts and stakeholder groups, clustered standard errors are not without limitation. An assumption of clustered standard errors is that the number of clusters goes to infinity (Ibragimov & Müller, 2016). With fewer clusters, the standard errors will not be estimated as precisely. The number of clusters in this study is quite large (1330) and may reduce this concern.
Second, the R-squared values in this study were quite low (less than 10% and a few near 1–2%). Even though the predictors of interest were found to be statistically significant, the low R-squared indicates that the predictors do not explain a substantial amount of the variability in the latent factors. These low R-squared values indicate that any predictions based on a respondent’s level of a latent factor would be less precise.
Lastly, stakeholders self-reported on their knowledge, beliefs, and opinions regarding student SEB problems via an online survey. Limitations of self-report include the fact that respondents may have been more likely to respond in a socially desirable way or to believe that they know more than they may actually do. For example, respondents may believe that they can identify the signs of SEB problems when, in fact, they may not comprehend the full range of signs. It is important to note that although statistically significant differences were identified across stakeholder groups, the overall mean levels of knowledge and beliefs reported were fairly high. For example, mean scores across those items assessing both knowledge and beliefs concerning SEB problems largely fell between 3.50 and 4.00 on a 5-point scale. Higher levels of reported knowledge and beliefs may have contributed to ceiling effects in some cases. In addition, having respondents complete a survey meant that we were unable to ask clarification questions. For example, as noted previously, respondents seemed to be less likely to strongly endorse screening for externalizing than internalizing concerns; however, the specific reasons for this remain unknown.
Implications
Results of the current study suggest that a role for schools in the identification and treatment of SEB problems is a shared priority within local communities (e.g., among parents, teachers, administrators). That is, key stakeholders not only acknowledged that student SEB problems are significant and need to be addressed, but also endorsed the use of proactive school-based approaches to risk identification and treatment. The percentages of respondents who endorsed the use of universal SEB screening in the current sample (range 32–42%) were much larger than would be anticipated given actual implementation estimates (i.e., 9%; Dineen et al., 2019), suggesting that additional factors beyond acceptability may need to be considered when trying to understand why calls from researchers and policymakers have not translated into practice. Much attention, for example, has been paid in recent years to the development and psychometric validation of school-based SEB screening instruments; however, the feasibility and ongoing practicality of these assessment procedures has received decidedly less emphasis. Feasibility concerns including financial costs, the availability of trained staff, and the extra work involved in carrying out assessment procedures have all been identified as potential barriers to universal screening implementation (NRCIM, 2009). Schools may also be hesitant to implement universal SEB screening procedures if they do not have the appropriate resources in place to offer follow-up services (NRCIM, 2009). Additionally, although the results of the current study indicate that there is strong support for school-based screening across a broad range of SEB constructs, schools may not be familiar with, or have access to, instruments that align with the constructs of most interest. Thus, future work to provide districts with more detailed guidance about how screening can be used to identify a range of relevant issues might further help to reduce the barriers to actual implementation.
Notes
The weighted root mean square residual (WRMR) is available. However, this statistic is not reported as it is still considered experimental and not recommend with large sample sizes (cf, DiStefano, Liu, Jiang & Shi, 2018).
Recall that the negative here is simply due to the contrast. The negative in this case indicates that school support staff have greater knowledge as the contrast was coded as building administrator minus school support staff.
References
Asparouhov, T., & Muthén, B. (2010). Weighted least squares estimation with missing data. Mplus Technical Appendix,2010, 1–10.
Blackman, K. F., Powers, J. D., Edwards, J. D., Wegmann, K. M., Lechner, E., & Swick, D. C. (2016). Closing the gap: Principal perspectives on an innovative school-based mental health intervention. Urban Review,48, 245–263.
Bollen, K. A. (1989). Structural equations with latent variables. New York, NY: Wiley.
Bradley, R., Doolittle, J., & Bartolotta, R. (2008). Building on the data and adding to the discussion: The experiences and outcomes of students with emotional disturbance. Journal of Behavioral Education,17, 4–23.
Briesch, A. M., Chafouleas, S. M., & Chaffee, R. K. (2017). Analysis of state-level guidance regarding school-based universal screening for social, emotional, and behavioral risk. School Mental Health,10, 147–162. https://doi.org/10.1007/s12310-017-9232-5.
Briesch, A. M., Chafouleas, S. M., Neugebauer, S. R., & Riley-Tillman, T. C. (2013). Assessing influences on intervention implementation: Revision of the usage rating profile-intervention. Journal of School Psychology,51, 81–96.
Brown, T. A. (2006). Confirmatory factor analysis for applied research. New York, NY: Guilford Press.
Bruhn, A. L., Woods-Groves, S., & Huddle, S. (2014). A preliminary investigation of emotional and behavioral screening practices in K − 12 schools. Education and Treatment of Children,37, 611–634.
Chalfant, J., Pysh, M., & Moultrie, R. (1979). Teacher assistance teams: A model for within-building problem solving. Learning Disabilities Quarterly,2, 85–89.
Cheung, G. W., & Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling,9, 233–255.
DiStefano, C., Liu, J., Jiang, N., & Shi, D. (2018). Examination of the weighted root mean square residual: Evidence for trustworthiness? Structural Equation Modeling: A Multidisciplinary Journal,25, 453–466.
Dineen, J. N., Chafouleas, S. M., Newton, S. D., Briesch, A. M., McCoach, D. B., & Cintron, D. W. (2019). Exploring social, emotional, and behavioral screening practices in U.S. public school district. Manuscript in submission.
Drummond, T. (1994). The student risk screening scale (SRSS). Grants Pass, OR: Josephine County Mental Health Program.
Frabutt, J. M., & Speach, G. (2012). Principals’ perspectives on school mental health and wellness in US Catholic Elementary Schools. School Mental Health,4, 155–169.
Gottfredson, D. C., & Gottfredson, G. D. (2002). Quality of school-based prevention programs: Results from a national survey. Journal of Research in Crime and Delinquency,39, 3–35.
Graham, A., Phelps, R., Maddison, C., & Fitzgerald, R. (2011). Supporting children’s mental health in schools: Teacher views. Teachers and Teaching: Theory and Practice,17, 479–496.
Greenberg, M. T., Domitrovich, C. E., Graczyk, P. A., & Zins, J. E. (2005). The study of implementation in school-based preventive interventions: Theory, research, and practice (Vol. 3). DHHS Pub. No. (SMA). Rockville, MD: Center for Mental Health Services, Substance Abuse and Mental Health Services Administration.
Greenley, J. R., Mechanic, D., & Cleary, P. (1987). Seeking help for psychological problems: A replication and extension. Medical Care,25, 1113–1128.
Han, S. S., & Weiss, B. (2005). Sustainability of teacher implementation of school-based mental health programs. Journal of Abnormal Child Psychology,33, 665–679.
Hauser, R. M., & Goldberger, A. S. (1971). The treatment of unobservable variables in path analysis. Sociological Methodology,3, 81–117.
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling,6, 1–55.
Iachini, A. L., Pitner, R. O., Morgan, F., & Rhodes, K. (2015). Exploring the principal perspective: Implications for expanded school improvement and school mental health. Children and Schools,38, 40–48.
Ibragimov, R., & Müller, U. K. (2016). Inference with few heterogeneous clusters. Review of Economics and Statistics,98, 83–96.
Individuals with Disabilities Act. (2004). 20 U.S.C. § 1400.
Jöreskog, K. G., & Goldberger, A. S. (1975). Estimation of a model with multiple indicators and multiple causes of a single latent variable. Journal of the American Statistical Association,70, 631–639.
Kam, C., Greenberg, M. T., & Walls, C. T. (2003). Examining the role of implementation quality in school-based prevention using the PATHS curriculum. Prevention Science,4, 55–63.
Kamphaus, R. W., & Reynolds, C. R. (2015). Behavior assessment system for children—3rd ed. (BASC-3): Behavioral and emotional screening system (BESS). Bloomington, MN: Pearson.
Kaplan, D. (2001). Structural equation modeling: Foundations and extensions. Thousand Oaks, CA: Sage.
Leaf, P. J., Bruce, M. L., Tischler, G. L., & Holzer, C. E. (1987). The relationship between demographic factors and attitudes toward mental health services. Journal of Community Psychology,15, 275–284.
Levitt, J. M., Saka, N., Romanelli, L. H., & Hoagwood, K. (2007). Early identification of mental health problems in schools: The status of instrumentation. Journal of School Psychology,45, 163–191. https://doi.org/10.1016/j.jsp.2006.11.005.
Lippman, L., Burns, S., & McArthur, E. (1996). Urban schools: The challenge of location and poverty. Washington, DC: National Center for Education Statistics.
Marcy, H. M., Dineen, J. N., McCoach, D. B., Chafouleas, S. M., & Briesch, A. M. (2018, December). The NEEDs2 Project: Project Methodology. Available at https://needs2.education.uconn.edu/methods/.
Maxwell, S. E., & Delaney, H. D. (2004). Designing experiments and analyzing data (2nd ed.). Mahwah, NJ: Lawrence Erlbaum.
Mendenhall, A. N., Iachini, A., & Anderson-Butcher, D. (2013). Exploring stakeholder perceptions of facilitators and barriers to implementation of an expanded school improvement model. Children and Schools,35, 225–234.
Moore, S. A., Widales-Benitez, O., Carnazzo, K. W., Kim, E. K., Moffa, K., & Dowdy, E. (2015). Conducting universal complete mental health screening via student self-report. Contemporary School Psychology,19, 253–267.
Murry, V. M., Heflinger, C. A., Suiter, S. V., & Brody, G. H. (2011). Examining perceptions about mental health care and help-seeking among rural African American families of adolescents. Journal of Youth Adolescence,40, 1118–1131.
Muthén, L. K., & Muthén, B. O. (2017). Mplus user’s guide (8th ed.). Los Angeles: Muthén & Muthén.
National Research Council and Institute of Medicine. (2009). Preventing mental, emotional, and behavioral disorders among young people: Progress and possibilities. Washington, DC: The National Academies Press.
New Freedom Commission on Mental Health. (2003). Achieving the promise: Transforming mental health care in America. Final report. DHHS pub. no. SMA-03-3832. Rockville, MD.
Powers, J. D., Bower, H. A., Webber, K. C., & Martinson, N. (2010). Promoting school based mental health: Perspectives from school practitioners. Social Work in Mental Health,9, 22–36. https://doi.org/10.1080/15332985.2010.522929.
Pryjmachuk, S., Graham, T., Haddad, M., & Tylee, A. (2011). School nurses’ perspectives on managing mental health problems in children and young people. Journal of Clinical Nursing,21, 850–859.
Reinke, W. M., Stormont, M., Herman, K. C., Puri, R., & Goel, N. (2011). Supporting children’s mental health in schools: Teacher perceptions of needs, roles, and barriers. School Psychology Quarterly,26, 1–13.
Roeser, R. W., & Midgley, C. (1997). Teachers’ views of issues involving students’ mental health. The Elementary School Journal,98, 115–133.
Romer, D., & McIntosh, M. (2005). The roles and perspectives of school mental health professionals in promoting adolescent mental health. In D. Evans, E. Foa, R. Gur, H. Hendin, C. O’Brien, M. Seligman, & B. Walsh (Eds.), Treating and preventing adolescent mental health disorders: What we know and what we don’t know (pp. 598–615). New York: Oxford University Press Inc.
Rothi, D. M., Leavey, G., & Best, R. (2008). On the front-line: Teachers as active observers of pupils’ mental health. Teaching and Teacher Education,24, 1217–1231.
Sanetti, L. M. H., & Kratochwill, T. R. (2009). Toward developing a science of treatment integrity: Introduction to the special series. School Psychology Review,38, 445–459.
Simon, A. E., Pastor, P. N., Reuben, C. A., Huang, L. N., & Goldstrom, I. D. (2015). Use of mental health services by children ages six to 11 with emotional or behavioral difficulties. Psychiatric Services,66, 930–937.
US Department of Education Office for Civil Rights. (2016). 2015–2016 Civil rights data collection: School climate and safety. Retrieved from https://www2.ed.gov/about/offices/list/ocr/docs/school-climate-and-safety.pdf.
US Public Health Service. (2000). Report of the surgeon general’s conference on children’s mental health: A national action Agenda. Washington, DC: US Department of Health and Human Services. http://www.surgeongeneral.gov/topics/cmh/childreport.htm.
Walter, H. J., Gouze, K., & Lim, K. G. (2006). Teachers’ beliefs about mental health needs in inner city elementary schools. Journal of the American Academy of Child and Adolescent Psychiatry,45, 61–68.
Wegmann, K. M., Powers, J. D., & Blackman, K. (2013). Supporting vulnerable families through school-based mental health services: Results of caregiver and teacher focus groups. Journal of Family Social Work,16, 297–313.
World Health Organization. (2011). Mental health: A state of well-being. Geneva: World Health Organization. http://www.who.int/features/factfiles/mental_health/en/index.html.
Acknowledgements
Special thanks are provided to all survey participants for their time, and appreciation is extended to research team members for their assistance on the project.
Funding
Preparation of this article was supported by funding provided by the Institute of Education Sciences, US Department of Education (R305A140543: PI Chafouleas). Opinions expressed herein do not necessarily reflect the position of the US Department of Education, and as such, endorsements should not be inferred.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Standards
All procedures performed were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was deemed exempt from obtaining signed written consent from participants in accordance with HHS regulations at 45 CFR 46.117(c). This article does not contain any studies with animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Briesch, A.M., Cintron, D.W., Dineen, J.N. et al. Comparing Stakeholders’ Knowledge and Beliefs About Supporting Students’ Social, Emotional, and Behavioral Health in Schools. School Mental Health 12, 222–238 (2020). https://doi.org/10.1007/s12310-019-09355-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12310-019-09355-9