
Abstract
The treatment for displaced mid-shaft clavicle fracture is highly controversial. In the last years, several biomechanical studies showed better functional results after surgical treatment. The purpose of this study is to evaluate the use of pre-contoured angular stability plate in this type of fracture. From June 2005 to July 2009, we have surgically treated 89 patients with displaced clavicle fracture. We have reevaluated 68 patients for a total of 70 interventions. Outcomes were assessed with Constant score, Dash questionnaire and X-rays. The mean follow-up period was 2 years. Excellent and good results were achieved for all the patients revaluated. The mean Constant score was 94.1 pt, and DASH score was 4.1. We had two cases of nonunion (2.9 %), while there was no case of infection and vascular or nervous lesions. A review of the international literature indicates that there is not a largely accepted gold standard for the treatment for displaced mid-shaft clavicle fractures. In the last 10 years, biomechanical and clinical studies have shown that nonoperative treatment for this type of fractures, with marked shortening or diastasis of the clavicle superior to 2 cm, may result in lower functional outcomes or higher percentage of nonunion. Nowadays, a lot of surgical options are available for the treatment for displaced mid-shaft clavicle fractures. Our experience with pre-contoured angular stability plates has shown excellent clinical outcome. On the basis of our study, we support the use of pre-contoured angular stability plate.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Clavicle fractures have an incidence rate of 5 % of all fractures and account for up to 45 % of fractures of the shoulder girdle with significant involvement of young population [1–3]. For many years, on the basis of historical studies performed in the 1960s by Neer and Rowe [4, 5], it was believed that nonoperative treatment was the gold standard. But in the last 10 years, an increasing number of biomechanical and clinical studies [2, 6–8] have placed this practice up for discussion. Today, displaced fractures of the clavicle are more and more frequently treated surgically, to restore the shoulder girdle full functionality, especially for fractures with severe comminution and shortening or diastasis greater than 2 cm [9–12]. There are many surgical methods available, although treatment with angular stability plates appears to offer greater success guarantees [13, 14]. We present our surgical experience in treating these fractures with the pre-contoured angular stability plate system (Acumed®). The purpose of this study is to evaluate the characteristics of this system of osteosynthesis, highlighting pros and cons based on the clinical data obtained.
Materials and methods
At the Orthopedics Department of the University Hospital in Modena, Italy, from June 2005 to July 2009, we surgically treated 89 patients with displaced clavicle fracture with pre-contoured angular stability plate. We reviewed 68 patients in a total of 70 clavicles. Twenty-one patients were untraceable at follow-up.
The fractures were classified according to Robinson’s classification [1] (Fig. 1), which is more accurate, complete and descriptive than the old Allman’s classification [15].

Robinson’s classification
We have had 25 type 2b1, 3 type 3b1, 39 type 2b2 and 3 type 3b2 fractures. One fracture was exposed, 16 patients have had associated injuries to the same arm (Table 1), and no neurovascular injury was noted. A total of 52 fractures concerned the left side and 18 the right side. A total of 58 patients were men (82.9 %) and 12 women (17.1 %), with an average age of 35.8 years (range 14–75 years) at the trauma.
All 68 patients were surgically treated with a pre-contoured angular stability plate system.
We took into consideration the following characteristics to decide for the surgical treatment: the severe comminution and the distance between the major two fragments greater than 2 cm of clavicle, shortening or diastasis. In particular, in order to evaluate the distance, it is very useful to perform a 15° up-tilted anteroposterior panorama radiograph of the shoulder girdle showing both clavicles on a single X-ray standing up. The shortening was measured with the following formula: PDL [%] = US-FS\US × 100 (PDL, proportional length difference; US, unfractured side; FS, fracture side) [16]. The starting point of measurement was the intersection point between a line centered in the lateral axis of the clavicle and the AC joint. The endpoint was defined as intersection point between a line centered in the medial axis of the clavicle and the SC joint. The unfractured side was used as reference with a relative length of 100 % [16] (Fig. 2). In two cases, there was a simultaneous bilateral fracture; therefore for those four fractures, comparison was not possible.

Anteroposterior Rx, the unfractured side is used as reference
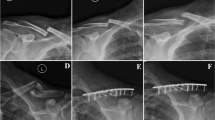
The plates are pre-shaped and divided into left and right, with a large modular system that allows treatment for fractures of all clavicle areas. Plates are made of titanium and have small thickness with holes where it is possible to insert standard or angular stability screws of 2.7 or 3.5 mm diameter. We used eleven 6-hole plates, fifty-one 7-hole plates, five 9-hole plates and three 10-hole plates. In each fixation, we used a minimum of 3 screws on each side of the fracture. We used 50 left plates plus 2 right plates for 52 left clavicle fractures and 17 right plates plus 1 left plate for 18 right clavicle fractures. In all cases, the plate was implanted according to the practice described above. We did not report any screw head rupture during plate application. All patients were subjected to general anesthesia in beach chair position. Anterosuperior surgical cutaneous incision was applied. Once fracture anatomic reduction was performed, we proceeded with osteosynthesis using suitable pre-contoured plate with compression and angular stability screws according to fracture type and location (Figs. 3 and 4). When a third fragment was noted, we fixated it by applying one or more interfragmentary screws. During the postoperative period, patients wore a sling for 15 days; afterward, sutures were removed and patients started passive and active arm mobilization. We removed the plate after fracture consolidation in ten patients (14.3 %). The causes were intolerance in three cases and patient’s request for esthetic reason for the remaining seven cases. None of those patients had a refracture after 12 months from the removal.

Fracture reduction

Osteosynthesis using suitable pre-contoured plate
Results
All 68 patients for a total of 70 fractures have been clinically reevaluated according to the Constant score and the Dash score. X-rays have been taken at 1, 2, 3, 6 and 12 months after surgery (Figs. 5, 6). The average follow-up period was 24.1 months (range 7–51). We obtained excellent clinical results with a mean Constant score of 94.1 ± 8.2 pt (range 53–100) and Dash score of 4.8 ± 7 (range 31.7–0). The average period of radiographic fracture consolidation was 2 months. The mean time to return to active life was 2.3 months.

Postoperative Rx

Twelve months after surgery Rx
We registered the following complications: 2 cases of nonunion (2.9 %) and 1 plate system mobilization due to a new trauma; moreover, we registered 2 superficial dehiscences of the surgical wound. There was no case of deep infection or vascular nervous lesion.
While performing a statistical analysis of the collected data (SPSS® Inc., USA—version 18.0), a statistically relevant difference (p = 0.00) between men and women arose regarding the mean Constant score, in favor of the male gender (95.5 ± 6.4 vs. 87.3 ± 12.2 pt). No significant difference appeared in Dash scores (p = 0.33) (Table 2). Considering the fracture type according to the Robinson’s classification, there was no evidence of significant differences (p > 0.05 at Constant and Dash scores); in addition, no further statistically significant differences in results appeared between mean Constant and mean Dash scores of patients with greater and minor shortening.
Discussion
On the basis of the results by Neer and Rowe [4, 5] in the 1960s, for many years it was considered that, barring a limited number of exceptions, a nonoperative treatment for mid-shaft-displaced clavicle fractures always produced good results, although these two studies are subjected to relevant criticism: firstly, a high number of teenagers—whose treatment is usually nonoperative—were included in their case records and secondly, evaluation tests for upper limb functioning, such as Dash and Constant scores, were not available.
Hill [2] was the first to carry out an extensive review of patients treated with figure-of-eight bandages for displaced middle-third clavicle fractures, discovering up to 31 % of patients reporting unsatisfactory results of the outcome. From a biomechanical point of view, it should be noted that during elevation, the clavicle performs a triple movement—rotation on its own axis, posterior inclination and upward inclination [16, 17]—contributing to scapulo-thoracic articulation movement and consequently to the shoulder girdle movement. Moreover, the clavicle is tasked of the transmission of the force from the trunk to the upper arms, giving stability to overhead movements. In their biomechanical studies, Lazarides [11] and Ledger [10] showed how clavicle nonunion with shortening over 2 cm can determine a significant reduction in leverage and subacromial space. A radiological study, carried out by Andhemar [9], showed for these cases the sternoclavicular angle increase, which can lead to a malpositioning of the scapula on the chest wall.
All these alterations can cause pain and strength reduction in overhead movements in clavicle fractures malunions, as shown by the study of McKee [6].
The surgical treatment for such lesions can be performed with several surgical techniques; the most widely employed are the intramedullary nail and the plate with screws. Several biomechanical studies have shown the superiority of the plate over the nail [17, 18]. In fact, laboratory loading tests have demonstrated how the plate and screws system has much more compression and torsional resistance, standing solicitations to the cyclic loading tests up to 20 % more than nail system. Robertson and Celestre’s [13, 14] studies successively demonstrated the superiority of angular stability systems over nonstability ones in the treatment for such fractures, because of a higher capacitance to resist to compression loads.
Moreover, the same biomechanical tests underlined the best performance when the locked plate is positioned at the top rather than anteriorly, above all for the torsional force.
In the field of angular stability plates for the treatment for displaced clavicle fractures, we have employed a new system of pre-contoured plates proposed by ACUMED®.
They are low-profile stability plates of titanium and exhibit peculiarities with respect to other plates on the market. They are pre-contoured and separate in right and left, with a wide modularity of the system allowing the treatment for all clavicle areas; they exhibit alternate holes where it is possible to apply standard or angular stability screws of 2.7 or 3.5 mm diameter.
From a biomechanical point of view, this plate presents the same characteristics of the LCDC plate at the laboratory tests in terms of resistance to the axial compression and torsional force [19].
This osteosynthesis system has many substantial advantages. The low profile of the plate reduces intolerance risk, as demonstrated by the small number of removals. The pre-contoured feature permits to obtain a more accurate and quick anatomic reduction. The large modularity allows to face all types of fractures in order to achieve a steady osteosynthesis. Clinically, these characteristics support the possibility of a faster mobilization and shorter recovery period compared with other surgical techniques.
Disadvantages are the implant cost (mean cost for a six-hole plate with six screws is 1,500 EUR) and the possibility of cold fusion phenomena of titanium screws that make the removal difficult (two cases of hard removal were noted).
In two cases, we have applied a right plate on left arm and in one case a left plate on right arm, in order to obtain a better adaptability to the clavicle-restored anatomic profile.
During these 4 years, we have treated 89 patients for displaced clavicle fracture using ACUMED® plate. Sixty-eight patients have been reevaluated for a total of 70 fractures, with a mean follow-up period of 2 years. Analysis of results has shown excellent mean Constant scores (94.1 pt) and Dash score (4.8). In addition, the mean consolidation period (2 months) and the return to active life period (2.3 months) appeared as optimal.
The percentage of complications is similar to the results of the major international case records available [8, 20–22]: in particular, for nonunion, we have had a percentage of 2.9 %, while no cases of infection or iatrogenic vascular nervous lesion have been recorded.
From a statistical point of view, our data point out that men achieve better outcome than women (p < 0.05), as reported in other studies [23, 24]. At the moment, there is not any explanation for this in literature; a hypothesis could be a little anatomic differences leading to a better adaptability of the pre-contoured plate for male gender, as the Huang’s study shows [24].
Moreover, we underline that in the literature there are not any clinical data regarding the application of pre-contoured plates in the treatment for mid-shaft clavicle fractures.
Conclusion
We deem that displaced mid-shaft clavicle fractures should be treated operatively using angular stability plates, in case surgical treatment is indicated by criteria explained above. We have reported our experience with pre-contoured angular stability plates. The clinical data reported in the study underline the efficacy of this fixation device.
When compared with other systems with the same biomechanical features, the pre-contoured plates present the advantage to achieve a more anatomic, firm and quick osteosynthesis. In addition, plate’s low profile seems to reduce intolerance and removal request.
These characteristics assure a better recovery time, compared with other osteosynthesis devices.
Nevertheless, some doubtful points still remain: high implant costs, imperfect plate adaptability in a limited number of cases and the possibility of cold fusion phenomena of titanium screws during a possible removal.
References
Robinson CM (1998) Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg [Br] 80-B:476–484
Hill JM, McGuire MH, Crosby LA (1997) Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg [Br] 79-B:537–539
Postacchini F, Gumina S, De Santis P et al (2002) Epidemiology of clavicle fractures. J Shoulder Elbow Surg 11:452–456
Neer CS (1960) Nonunion of the clavicle. JAMA 172(10):1006–1011
Rowe CR (1968) An atlas of anatomy and treatment of mid-clavicular fractures. Clin Orthop Related Res 58:29–42
McKee MD, Wild LM, Schemitsch EH (2003) Midshaft malunions of the clavicle. J Bone Joint Surg [Am] 85-A:790–797
Postacchini R, Gumina S, Farsetti P, Postacchini F (2010) Long-term results of conservative management of midshaft clavicle fracture. Int Orthop 34(5):731–736
Canadian Orthopaedic Trauma Society (2007) Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. J Bone Joint Surg [Am] 89-A:1–10
Andermahr J, Jubel A, Elsner A (2006) Malunion of the clavicle causes significant; 28 glenoid malposition: a quantitative anatomic investigation. Surg Radiol Anat 28:447–456
Ledger M, Leeks N, Ackland T et al (2005) Short malunions of the clavicle: an anatomic and functional study. J Shoulder Elbow Surg 14:349–354
Lazarides S, Zafiropoulos G (2006) Conservative treatment of fractures at the middle third of the clavicle: the relevance of shortening and clinical outcome. J Shoulder Elbow Surg 15(2):191–194
Wick M, Müller EJ, Kollig E et al (2001) Midshaft fractures of the clavicle with a shortening of more than 2 cm predispose to non-union. Arch Orthop Trauma Surg 121:207–211
Robertson C, Celestre P, Mahar A et al (2009) Reconstruction plates for stabilization of midshaft clavicle fractures: differences between nonlocked and locked plates in two different positions. J Shoulder Elbow Surg 18:204–209
Celestre P, Robertson C, Mahar A et al (2008) Biomechanical evaluation of clavicle fracture plating techniques: does a locking plate provide improved stability? J Orthop Trauma 22:241–247
Allman FL Jr (1967) Fractures and ligamentous injuries of the clavicle and its articulation. J Bone Joint Surg [Am] 49(4):774–784
Smekal V, Deml C, Iremberger A et al (2008) Length determination in midshaft clavicle fractures: validation of measurement. J Orthop Trauma 22:458–462
Kapandji IA (1988) The physiology of the joints, vol 1: Upper limb
Golish SR, Oliviero JA, Francke EI et al (2008) A biomechanical study of plate versus intramedullary devices for midshaft clavicle fixation. J Orthop Surg Res 3(28):1–5
Goswami T, Markert RJ, Anderson CG et al (2008) Biomechanical evaluation of a pre-contoured clavicle plate. J Shoulder Elbow Surg 17:815–818
Preston CF, Egol KA (2009) Midshaft clavicle fractures in adults. Bull NYU Hosp Joint Dis 67(1):52–57
Lee Y-S, Huang H-L, Lo T-Y et al (2008) Surgical treatment of midclavicular fractures: a prospective comparison of Knowles pinning and plate fixation. Int Orthop (SICOT) 32:541–545
Chen C-H, Chen J-C, Wang C et al (2008) Semitubular plates for acutely midclavicular fractures: a retrospective study of 111 patients followed for 2.5 to 6 years. J Orthop Trauma 22:463–466
Jeray KJ (2007) Acute midshaft clavicular fracture. J Am Acad Orthop Surg 15:239–248
Huang JI, Toogood P, Chen MR et al (2007) Clavicular anatomy and the applicability of precontoured plates. J Bone Joint Surg Am 89:2260–2265
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Campochiaro, G., Tsatsis, C., Gazzotti, G. et al. Displaced mid-shaft clavicular fractures: surgical treatment with a pre-contoured angular stability plate. Musculoskelet Surg 96 (Suppl 1), 21–26 (2012). https://doi.org/10.1007/s12306-012-0196-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12306-012-0196-1