
Abstract
To err is human. Human errors and flaws in the system and quality of health care persist despite patient safety initiatives and identification of new strategies of improvement. A significant focus in surgery is to identify strategies and improve patient safety, prevent postoperative complications and any adverse events. The World Health Organization (WHO) surgical safety checklist has been shown to decrease mortality and complications and has been adopted worldwide. A retrospective pre-intervention study was done from September 2014 to August 2015, data analysed, necessary training, changes and awareness was implemented over 1 month and then, a prospective study was done post-intervention using WHO safety check list from October 2015 to September 2016 both at Rajarajeswari Medical College and Hospital, Bangalore, India by implementing the safety check list and by corrections of errors present during the pre-intervention phase. A total of 216 patients were recorded during the pre-intervention phase, and a total of 248 patients were included in the post-intervention analysis after implementing the WHO safety check list. Our study showed a reduction of intraoperative surgical complications from 5.1 to 2.41% and from 6.48 to 4.44% in postoperative surgical complications after the implementation of safety check list. There were significant reductions in anaesthesia complications, during and after surgery post implementation (intraoperative from 2.78 to 1.61%, postoperative from 1.4 to 0.8%). We also observed a significant change in the death rates post-implementation. Intraoperative death reduced from 1.4 to 0.4% and postoperative deaths reduced from 12.04 to 8%. Surgical safety check list improves the quality of patient care and improves perceptions on patient safety. It significantly reduces the morbidity and mortality by reducing the complications and improving the quality of treatment and health care. It is easy to understand and implement the surgical safety check list after training, proper guidance, and education. It is a must to implement the surgical safety check list in all institutions to improve the patient safety and to reduce the errors in patient care.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Health care is a team effort. When human limitations are combined with organizational complexity, human error becomes inevitable. Average error rates of 10% are seen in hospital admissions [1].
Numerous changes have since been advocated to improve patient safety like mandating minimum nurse to patient ratios, reducing working hours of trainee/resident doctors, introduction of ‘care bundles’ that improve patient outcomes, introduction of safety checklists and advances in the science of simulation and teamwork training.
The WHO launched Global Patient Safety Challenge: Safe Surgery Saves Lives (SSSL) in 2006 in response to the global need to improve outcomes in surgery.
A checklist is more than a technical solution; if used properly, it ensures that few things will be reviewed at certain times.
For these reasons, incident reporting appears to be a surrogate marker of safety culture.
In our hospital, implementation of surgical safety checklist was started from September 2015.
Aims and Objectives
The main aim of this study is to assess the effectiveness of surgical safety checklist in our Institution. We also study and analyse the errors in our operation theatre, compare with international standards, train and educate the theatre personnel and implement the necessary corrections to avoid errors and ensure maximum safety for the patients.
Methods
Study Design
This study was conducted in the Department of General Surgery at Rajarajeswari Medical College and Hospital, Bangalore, India. All the elective surgical cases were included and all the emergency cases were excluded in our study.
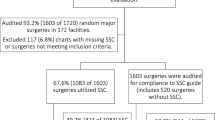
A retrospective study of pre-intervention from September 2014 to August 2015 was done to analyse the errors in surgical safety and then, a prospective study of post-intervention from October 2015 to September 2016 was done by implementing the safety check list and by corrections of errors present during the pre-intervention phase (Fig. 1).

Flow chart of the study about the use of surgical safety check list
A local investigator was chosen and was trained in the identification and reporting of process, measures, errors and complications. This person worked on the study full-time and did not have clinical responsibilities at the study site. Data analysis and implementation of the check list was done by the principal investigator, in this case the author and his assistant, the co-author (Fig. 2).

WHO surgical safety check list
Ten essential objectives for safe surgery were identified:
(i) Correct site of surgery
(ii) Provision of safe anaesthesia
(iii) Panagement of airway problems
(iv) Mmanagement of haemorrhage
(v) Avoiding known allergies
(vi) Minimizing the risk of surgical site infection
(vii) Preventing the retention of swabs and instruments
(viii) Accurate identification of specimens
(ix) Effective communication within the surgical team
(x) Routine surveillance of surgical outcomes.
Intervention
After collecting baseline data retrospectively, the local investigator was given information to identify errors and deficiencies and was then asked to implement the 19-item WHO safe-surgery checklist. The checklist consists of an oral confirmation by surgical teams at the time of sign in, time out and sign out.
The Departments of Surgery and Anaesthesiology, the operation theatre personnel and the design team created an education program focused on the checklist. The education program consisted of oral, online education module and an educational video showing the checklist process, elements involved, theatre and perioperative service area. A weekly frequently asked question communications to surgical team members and theatre. The local investigator introduced the checklist to operating-room staff, using lectures, written materials or direct guidance. The checklist was introduced over a period of 1 month. Personnel training regarding the benefits of the checklist and the checklist process was conducted for a period of 1 month.
Data Collection
Standardized data sheets completed by the local investigators and the clinical teams involved in surgical care were analysed. Perioperative data included the demographic characteristics of patients, procedural data and the type of anaesthesia used as per the WHO surgical safety check list.
Patients were followed prospectively until discharge or for 30 days, whichever came first, for death and complications. Outcomes were identified through chart monitoring and communication with clinical staff. Completed data forms were directed to primary investigator.
Who Surgical Safety Check List
Knowledge of the safety checklist was analysed based on a questionnaire used before and after implementation for the surgeons, anaesthesiologists and the theatre personnel. The scoring was done on a scale of ten and the following results were drawn as per Table 1.
The questionnaire as shown in Table 2 was based on a Likert type scale and a yes/no question. Post-implementation also included the above questionnaire along with open-ended questions like the overall satisfaction of using the check list, ease and benefits of using the check list and if it would be beneficial in implementing the check list for patient’s safety.
Results
A total of 216 patients were included in the pre-intervention study and a total of 248 patients were included in the post-intervention study. The intraoperative and the postoperative complications both due to surgery and the anaesthesia were assessed and recorded (Table 3).
The effectiveness of the safety check list was studied and analysed by comparing the intraoperative and postoperative complications before and after its implementation.
Our study showed a reduction of intraoperative surgical complications from 5.1 to 2.41% and from 6.48 to 4.44% in postoperative surgical complications after the implementation of safety check list (Table 4).
There was a significant reduction in anaesthesia complications, both during and after surgery post-implementation (intraoperative from 2.78 to 1.61%, postoperative from 1.4 to 0.8%) as shown in Table 4.
We also observed a significant change in the death rates post-implementation. Intraoperative death reduced from 1.4 to 0.4% and postoperative deaths reduced from 12.04 to 8% (Table 5).
The data we analysed before and implementation of the safety check list was comparable with the studies done by B Haynes [2] et al. and Haugen et al. [3]. Complications before implementation in our study were 15.76% as compared to Haynes et al. [2] which was 21 and 2.93% in Haugen et al. [3] study. Post-implementation, our study showed 9.26% in the complication rate while their studies showed 12 and 2.77%, respectively (Fig. 3).

Comparison of our study with other studies before and after implementation of safety check list
Death rate in our study was 13.44 and 1.20% before and after implementation, while the study done by B Haynes et al. [2] had a comparison of 1.10 and 0.30% before and after implementation. Study done by Haugen et al. [3] had no mortality rate (Fig. 3).
Discussion
The implementation of WHO surgical safety checklist showed significant and positive changes, with overall improvement in the awareness of patient safety, communication and quality of care. Improvements were noted in the perception of value and participation in the time-out process, surgical team communication and the establishment and clarity of patient care needs.
Use of this check list will help to bring about effective modifications in the process of execution as an ongoing quality improvement in our institution.
The checklist has garnered significant worldwide enthusiasm, with programs implemented in 26 countries and more than 3000 hospitals worldwide within 3 years of its introduction. [4].
It has been suggested that the simplicity of the checklist facilitates a rapid and effective implementation process [5]. The surgical safety checklist has been shown to improve postoperative morbidity and mortality [6]. Poor communication between surgeons and surgical team members has been previously reported, and team training may be required for effective checklist use [7].
Humans are fallible, and this checklist enhances consistency in surgical team performance at critical times, fostering good communication, teamwork and a culture of patient safety [8].
There was improvement in patient safety following implementation of surgical safety checklist in our study suggested by a reduction in percentage of complications by 5.3% and percentage of deaths by 4.03%.
Conclusion
By this study, it is eminently evident that surgical safety checklist can be implemented in all the institutions.
Implementation of surgical safety checklist is a prerequisite in surgical health care team to reduce the errors associated and for improved patient safety.
Knowledge about surgical safety checklist in surgical team has scope for improvement.
References
Sevdalis N, Hull L, Birnbach DJ (2012) Improving patient safety in the operating theatre and perioperative care: obstacles, interventions, and priorities for accelerating progress. Br J Anaesth 109:3–16
Haynes B, Weiser G, Berry R et al (2009) A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med 360(3):491–499
Haugen AS, Softeland E, Eide GE et al (2013) Impact of WHO’s surgical safety checklist on a safety culture in the operating theatre. British J Anaesth 110(5):807–815
World Health Organization. Safe Surgery Saves Lives. 2013 http://www.who.int/patientsafety/safesurgery/en/index.html. Accessed December 20, 2012.
Haynes AB, Weiser TG, Berry WR et al (2009 Jan 29) A safe surgery saves lives study group. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med 360(5):491–499 Epub 2009 Jan 14
Bliss LA, Ross-Richardson CB, Sanzari LJ et al (2012 Dec) Thirty-day outcomes support implementation of a surgical safety checklist. J Am Coll Surg 215(6):766–776 Epub 2012 Aug 28
Fourcade A, Blache JL, Grenier C, Bourgain JL, Minvielle E (2012 Mar) Barriers to staff adoption of a surgical safety checklist. BMJ Qual Saf 21(3):191–197 Epub 2011 Nov 7
Haynes AB, Weiser TG, Berry WR, Lipsitz SR, Breizat AH, Dellinger EP, Dziekan G, Herbosa T, Kibatala PL, Lapitan MC, Merry AF, Reznick RK, Taylor B, Vats A, Gawande AA, Safe Surgery Saves Lives Study Group (2011) Changes in safety attitude and relationship to decreased postoperative morbidity and mortality following implementation of a checklist-based surgical safety intervention. BMJ Qual Saf 20(1):102–107
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Haridarshan, S.J., Girish, C.S. & Rajagopalan, S. Effects of Implementation of W.H.O Surgical Safety Check List: Our Institutional Analysis. Indian J Surg 80, 465–469 (2018). https://doi.org/10.1007/s12262-017-1635-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-017-1635-x