
Abstract
Neoplastic progression in Barrett’s esophagus (BE) occurs by a multistep process associated with early molecular and morphological changes. This study evaluated cell proliferation and p53 expression and their correlation in the development and progression of esophageal adenocarcinoma. PCNA and p53 expressions were analyzed in biopsy samples by immunohistochemistry including patients with reflux esophagitis, BE, BE with concomitant esophagitis, Barrett’s dysplasia, esophageal adenocarcinoma and a control group without any histological changes. Progressive increase in cell proliferation and p53 expression was found in the sequence of malignant transformation of the esophageal mucosa. While cell proliferation was significantly lower in the control group compared with all other groups, there was no increase in p53 expression of esophageal tissues that were negative for dysplasia. Dysplastic BE tissues revealed significantly higher cell proliferation and p53 expression levels compared to BE, reflux esophagitis or BE with concomitant esophagitis. Both, cell proliferation and p53 expression were significantly higher in adenocarcinoma compared to BE or Barrett’s dysplasia. Interestingly, while just BE with concomitant esophagitis showed significantly higher p53 expression levels than BE, both, BE with concomitant esophagitis and reflux esophagitis revealed significantly higher cell proliferation levels compared to BE. Alterations of cell proliferation and p53 expression showed a strong correlation. Simultaneous activation of cell proliferation and p53 expression strongly suggest their association with esophageal epithelial tumor genesis and particularly, their specific role in the biology of esophageal adenocarcinoma. Quantification of these parameters in BE is thought to be useful to identify patients at higher risk for progression to adenocarcinoma.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Esophageal cancer is still one of the most widespread diseases. The incidence of adenocarcinoma of the esophagus has risen steadily in both the United States and in Europe over the last two to three decades, whereas the incidence of esophageal squamous cell carcinoma has remained relatively static [1, 2]. The early diagnosis of esophageal carcinoma correlates closely with improvement in prognosis. Esophageal adenocarcinoma is frequently accompanied by Barrett’s esophagus (BE) [3], recognized as metaplastic condition in which the squamous epithelium lining the lower esophagus is replaced by columnar epithelium [4], often of a specialized intestinal type, as a consequence of gastro-esophageal reflux disease (GERD) [5]. Reflux induces damage to squamous epithelial cells and causes stem cell proliferation, resulting in the replacement of squamous cells with columnar cells [6].
BE is the main precancerous condition in the development of esophageal adenocarcinoma and represents the first step in the pathway to esophageal adenocarcinoma [7]. The metaplastic esophageal mucosa subsequently progresses through dysplasia to adenocarcinoma [8].
Diagnosis of Barrett’s adenocarcinoma is usually made late, and consequently, is associated with poor prognosis [9, 10]. Earlier detection of cancer and/or characterization of dysplasia are beneficial in early identification of patients at higher risk for adenocarcinoma. Evaluation of tissue biomarkers, as cell proliferation and p53 expression has been proven useful for identifying dysplasia and estimation of malignant progression in BE [11, 12].
It has been recognized for some time that the cell cycle is dysregulated in dysplastic Barrett’s mucosa with increased cell proliferation. Moreover, there is evidence of loss of spatial organization with abnormal cell proliferation on the surface epithelium in high-grade dysplasia [13]. The proliferating cell nuclear antigen (PCNA) technique is an accepted method for measurement of cell proliferation. PCNA is the co-factor of DNA-polymerase and can be detected mostly in the late G1 and S phases, but it is also present in every phase of the cell cycle [14].
The progression of the cell cycle from G1- to S-phase, which apparently is a critical event in the cellular proliferation of Barrett’s dysplasia [15] can be downregulated by the tumor suppressor p53 [16]. One cell cycle abnormality that was observed previously in Barrett tissue was the overexpression of this tumor suppressor [17, 18]. Such overexpression usually is indicative of mutated p53, which has a longer half-life than wild-type p53 [19]. Significantly, identical p53 mutations were observed at high frequencies in Barrett high grade dysplasia and adenocarcinoma [20]. With respect to p53 overexpression, it was reported that only 5% of Barrett patients without dysplasia were positive for p53 overexpression, whereas, 15%, 45%, and 53% of patients with indefinite/low grade dysplasia, high grade dysplasia, and adenocarcinoma, respectively, were positive for p53 overexpression [17]. These results suggest that p53 mutations play a role in the progression of Barrett’s dysplasia to adenocarcinoma.
It has been proposed that the combination of p53 protein expression and disordered proliferative architecture may be used as an objective biomarker to assist in the recognition and diagnosis of dysplastic change [21, 22].
Combination of upper gastrointestinal endoscopy and light microscopic (histological) evaluation with cell/tissue biomarker identification by immunohistochemistry has been thus shown to be useful to identify patients at higher risk for progression to esophageal adenocarcinoma.
Recently, we have reported that simultaneous downregulation of gluthatione S-transferase (GST), the enzyme playing a protective role in the prevention of cancer by detoxifying potentially carcinogenic compounds, and upregulation of matrix metalloproteinase-9 (MMP-9), an aggressive factor playing a crucial role in progression of carcinogenesis, in the BE–dysplasia–adenocarcinoma sequence, strongly suggest their association with esophageal tumor development and their specific role in the stepwise sequence to carcinoma in BE [23].
To date, according to our knowledge, cell proliferation or p53 expression has not been evaluated in the whole sequence of malignant transformation of the esophagus. Therefore, here we evaluated cell proliferation (PCNA) and p53 expression by immunohistochemical techniques in the development and progression of esophageal adenocarcinoma including reflux esophagitis, BE, BE with concomitant esophagitis, dysplasia and adenocarcinoma and estimated the correlation of expression of these two markers compared to the recently described increase of MMP-9 expression in the whole sequence of malignant transformation of the esophagus.
Materials and Methods
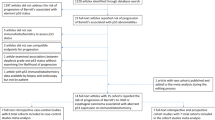
The immunohistochemical analysis of cell proliferation and p53 expression in the development and progression of reflux esophagitis–Barrett metaplasia–dysplasia–adenocarcinoma sequence in the esophagus was a retrospective study using paraffin-embedded biopsy specimens, which were taken from patients between 2000 and 2004 at the 2nd Department of Medicine, Semmelweis University Budapest.
A total of 51 formalin-fixed, paraffin-embedded esophageal tissue samples were analyzed by immunohistochemical techniques. Groups comprised 33 males and 18 females. The median age was 64 with a range from 22 to 83 years.
The selection was based on a clinical and histological evidence of the corresponding diagnosis including reflux esophagitis (n = 7; four males, three females, mean age 61 years, range 36–68 years); BE (n = 14; 9 males, five females, mean age 66 years, range 48–69 years); BE with concomitant esophagitis (n = 8; six males, two females, mean age 67 years, range 55–71 years); BE with dysplasia (n = 7; four males, three females, mean age 68 years, range 52–72 years); and esophageal adenocarcinoma (n = 8; six males, two females, mean age 71 years, range 64–83 years). Esophageal biopsies from patients with functional dyspepsia without any histological changes were used as controls (n = 7; four males, three females, mean age 49 years, range 22–56 years).
For immunohistochemistry, all biopsy specimens were fixed in buffered formalin and embedded in paraffin and four micron thick sections were cut and mounted on glass slides as previously described [24].
Immunohistochemical Staining
Proliferation—PCNA Immunohistochemistry
The 4 micron thick tissue sections were dewaxed and rehydrated. Antigen unmasking was carried out in citrate buffer pH 6.0 by microwave heat treatment (3 min 750 W and 3 min 370 W), and samples were cooled down in PBS for 20 min. Endogenous peroxidase activity was blocked by incubation for 30 min at room temperature in 3% hydrogen peroxide. After being washed thrice in PBS for 3 min, the slides were incubated with optimally diluted PCNA antibody (Clone: PC10, DAKO) for 15 min at 37°C in a dark humidified chamber. After being washed thrice in PBS, signal conversion was carried out with the LSAB2 system (DAKO: K0672) as described in the manual. Hematoxylin co-staining was done.
p53 Immunohistochemistry
The 4 micron thick tissue sections were deparaffinized in xylene and rehydrated through graded ethanol. Antigen unmasking was carried out by microwave heat treatment (samples in plastic jars containing citrate buffer pH 6.0 were put into a preheated (95–99°C) plastic water bath and were heated with 500 W for 15 min), and samples were cooled down in PBS for 20 min. Endogenous peroxidase activity was blocked by incubation for 30 min at room temperature in 3% hydrogen peroxide. After being washed thrice in PBS for 3 min, the slides were incubated with optimally diluted p53 antibody (Clone: DO-7, DAKO) at 37°C for 30 min in a humidified chamber. After being washed thrice in PBS, signal conversion was carried out with the LSAB2 system (DAKO) as described in the manual. Hematoxylin co-staining was done.
Evaluation of Immunohistochemical Staining
Immunostaining was determined semiquantitatively, as previously described [25, 26]. Known immunohistochemically-positive tissue sections were used as positive controls, and negative control sections were processed immunohistochemically after the primary antibody was replaced by PBS. None of these negative control sections exhibited immunoreactivity.
At least 600 (mainly 800) epithelial cells were counted in each sample using light microscope (40X objective). The labeling index (LI) was defined as a percentage of the positive nuclei over the total nuclei counted. The evaluation of staining intensity (i.e. number of positive cells) for both, PCNA and p53 was performed by two investigators (I.H., H.G.) independently, without the knowledge of histology and results of the other investigator. There was less than 5% variance between the results of two counts.
Statistical Analysis
Statistical analysis with one-way ANOVA, LSD test and correlation analysis were performed by the Statistica for Windows 4.3 program package. Values were expressed as mean±SD and p value <0.05 was considered statistically significant.
Results
Cell proliferation index and p53 expression scores in various types of mucosal lesions of the esophagus are shown in Tables 1 and 2.
Cell Proliferation
The cell proliferation rate has increased in the sequence of malignant transformation of the esophagus, from Barrett’s esophagus to dysplasia and adenocarcinoma (Table 1). In BE the cell proliferation (Fig. 2c) was significantly higher compared to the normal esophageal epithelium (Fig. 1a) but significantly lower compared to reflux esophagitis or BE with concomitant esophagitis (Table 1). In the epithelium of BE the proliferative compartment was mostly limited to the bottoms of the crypts (Fig. 2c). In addition, the score of cell proliferation was significantly higher in Barrett’s epithelium than in normal gastric mucosa (data not shown). Interestingly, there was no difference in proliferation index between reflux esophagitis and BE with concomitant esophagitis. Further, an upward shift of the proliferative compartment was observed from metaplasia to dysplasia and adenocarcinoma (Table 1). Finally, cell proliferation was significantly higher in adenocarcinoma (Fig. 4b) compared with dysplastic Barrett esophagus tissue (Fig. 3b), however, proliferative cells were irregularly distributed in invasive cancer areas.

Cell proliferation and p53 expression in normal esophageal epithelium, a cell proliferation (PCNA immunohistochemistry), b p53 expression. Representative histology sections are shown (×40 magnification). Cell proliferation and p53 expression is illustrated by brown staining of the nuclei

Cell proliferation and p53 expression in Barrett’s esophagus without dysplasia, a hematoxylin and eosin staining, b Alcian blue-periodic acid-Schiff staining, c cell proliferation (PCNA immunohistochemistry), d p53 expression. Representative histology sections are shown (×20/×100 immersion magnification). Cell proliferation and p53 expression is illustrated by brown staining of the nuclei

Cell proliferation and p53 expression in dysplastic Barrett’s esophagus, a hematoxylin and eosin staining, b cell proliferation (PCNA immunohistochemistry), c p53 expression. Representative histology sections are shown (×20 magnification). Cell proliferation and p53 expression is illustrated by brown staining of the nuclei
p53 Expression
We found no increase in p53 expression in Barrett esophagus tissues that were negative for dysplasia (Fig. 2d) compared to the normal esophagus epithelium (Fig. 1b) except Barrett’s esophagus with concomitant esophagitis which showed significantly higher p53 expression levels than BE and the control group (Table 2). The increased p53 accumulation in BE with concomitant esophagitis was significantly higher also compared to reflux esophagitis. There was no difference in p53 expression scores between BE and reflux esophagitis (Table 2).
Significantly higher expression levels of p53 have been observed in Barrett esophagus tissues that were positive for dysplasia (Fig. 3c) compared with BE without dysplasia (Fig. 2d) and also BE with concomitant esophagitis (Table 2).
With respect to esophageal adenocarcinoma, the p53 expression was high, as reflected by prominent nuclear immunohistochemical staining (Fig. 4c). The expression levels of p53 were significantly higher in adenocacinoma compared with dysplastic Barrett esophagus tissues and the other groups (Table 2).

Cell proliferation and p53 expression in esophageal adenocarcinoma, a hematoxylin and eosin staining, b cell proliferation (PCNA immunohistochemistry), c p53 expression. Representative histology sections are shown (×20 magnification). Cell proliferation and p53 expression is illustrated by brown staining of the nuclei
The cell proliferation and p53 expression in the development and progression of normal epithelium, reflux esophagitis, BE, dysplasia and adenocarcinoma sequence of the esophagus were linearly correlated (r = 0.91; Fig. 5) and increased with the severity of mucosal lesions.

Correlation between cell proliferation and p53 expression in the development and progression of normal epithelium, reflux esophagitis, Barrett’s esophagus, dysplasia and adenocarcinoma sequence of the esophagus. Cell proliferation is linearly correlated with p53 expression (r = 0.91; p < 0.01)
Additionally, the increase of these two markers was linearly correlated with the recently reported immunoexpression changes [23] of matrix metalloproteinase-9 (Fig. 6a–b; PCNA with MMP-9 [r = 0.84]; p53 with MMP-9 [r = 0.82]).

Correlation between cell proliferation or p53 expression and recently reported MMP-9 expression in the development and progression of normal epithelium, reflux esophagitis, Barrett’s esophagus, dysplasia and adenocarcinoma sequence of the esophagus, a cell proliferation is linearly correlated with MMP-9 expression (r = 0.84; p < 0.05), b p53 expression is linearly correlated with MMP-9 expression (r = 0.82; p < 0.05)
Discussion
Despite advances in diagnosis and therapy, esophageal adenocarcinoma remains an aggressive and usually lethal tumor. BE is the main precancerous condition in the development of esophageal adenocarcinoma, however, its pathogenesis is still poorly understood. It has been reported that BE develops as a complication of chronic gastroesophageal reflux [5] and is associated with an increased risk of esophageal adenocarcinoma [7, 27]. BE typically progresses from metaplasia with atypia to dysplasia and adenocarcinoma. This hypothesis has led to the use of endoscopic biopsy surveillance to detect dysplasia in patients before carcinoma develops [28]. It is of great clinical importance to correctly identify changes with a high risk for malignant transformation, as high-grade dysplasias and early adenocarcinomas in patients with BE to have a higher chance for cure [29].
The identification of high-risk lesions in BE by histology has also disadvantages, especially regarding sampling errors and frequent intra- and inter-observer discrepancies in the histopathologic grading/staging of these lesions. Several new biomarkers are being tested to help in better determining the risk of cancer development.
Although most of the biological markers need to be evaluated further, at present, cell proliferation, aneuploidy status, p16 and p53 gene abnormalities, or allelic losses are the most extensively documented alterations [11]. Immunostaining with a variety of antibodies provides a better understanding of the process of malignant transformation and helps to identify early markers of malignant transformation in BE [30].
We have recently reported that simultaneous downregulation of GST and upregulation of MMP-9 in the BE–dysplasia–adenocarcinoma sequence strongly suggest their association with esophageal tumor genesis and particularly their specific role in the biology of esophageal adenocarcinoma [23].
To date, according to our knowledge, cell proliferation or p53 expression has not been evaluated in the whole sequence of malignant transformation of the esophagus. Here we evaluated cell proliferation and p53 expression changes and their correlation compared with previously described increase in MMP-9 expression in the development and progression of normal epithelium, reflux esophagitis, BE, dysplasia and adenocarcinoma sequence of the esophagus.
Alterations in proliferative activity of the epithelium are related to cancer risk in most organs of the gastrointestinal tract. In the colon the occurrence of adenomas and carcinomas is associated with an increased epithelial cell proliferation [31]. Patients operated for colorectal cancer, have a higher risk for recurrent adenomas, if there is increased proliferation in random rectal biopsies [32]. In the stomach Billroth-II resections and Helicobacter pylori (H. pylori) infection, both risk factors for gastric cancer, are associated with increased cell proliferation [33], with a normalization after H. pylori eradication in the latter case. Also in BE a positive correlation has been shown between proliferative activity and risk factors for cancer, such as dysplasia, type of metaplasia and length of the Barrett segment [34]. Further, in the progression of Barrett’s metaplasia to adenocarcinoma the balance of proliferation/apoptosis is thought to play an important role [35].
In the present study, immunohistochemical analysis revealed a progressive increase in cell proliferation rate with increasing severity of esophageal lesions. We demonstrated that cell proliferation was significantly lower in normal esophageal epithelium (control group) compared with all other groups. Barrett esophagus tissues that were positive for dysplasia revealed a significantly higher cell proliferation index compared to BE, reflux esophagitis or BE with concomitant esophagitis. We observed that cell proliferation was significantly higher in adenocarcinoma compared to BE or BE tissues positive for dysplasia. Our findings are similar to the results reported by Hong et al. [13), Polkowski et al. [22] and Kim et al. [36].
Novel finding in our study is that cell proliferation in reflux esophagitis or Barrett’s esophagus with concomitant esophagitis is significantly higher compared to BE alone. It has been shown that gastric acid may stimulate cell proliferation by directly affecting the epithelium. In this respect gastric juice of low pH has mitogenic effects on isolated cells in culture, whereas pH neutral juice lacks this effect or even has some inhibitory action [37]. In a large epidemiologic study symptomatic GERD was a strong risk factor for esophageal adenocarcinoma [38]. In addition, acid reflux is increased in BE patients [39] and elimination of reflux in patients with BE and GERD, prevents from a further increase of proliferative activity at the luminal surface of Barrett epithelium in the distal esophagus [40].
These findings may support our observations, including increased p53 expression in BE with concomitant esophagitis compared to BE alone, that acid reflux in BE might induce progression from BE to dysplasia and adenocarcinoma.
Although p53 protein overexpression detected by immunohistochemistry is an indirect method of detecting a p53 gene mutation [41], it has great clinical applicability.
Several recent studies evaluating p53 accumulation using immunohistochemistry have shown increasing p53 expression in the dysplasia–adenocarcinoma progression of Barrett’s esophagus [22, 42]. However, p53 accumulation was just very rarely or was not observed in metaplastic esophageal mucosa without dysplasia [17, 22] or low-grade dysplasia with no concomitant invasive carcinoma [43]. On the other hand, it has been shown that patients with p53-immunoreactive low-grade dysplasia progress more rapidly to high-grade dysplasia and/or carcinoma [12]. Furthermore, a recent study analyzing the effect of photodynamic therapy and evaluating cell proliferation as well as p53 expression in BE reported that that BE without dysplasia shows elevated crypt proliferation but low p53 expression [44].
In our present study in correlation with previous findings of Polkowski et al. [22] and Younes et al. [45] we found a progressive increase of p53 expression in the sequence of malignant transformation of the esophagus. We demonstrated that there was no increase in p53 expression of esophageal tissues that were negative for dysplasia including Barrett’s esophagus and reflux esophagitis compared to the control group. Barrett esophagus tissues that were positive for dysplasia revealed a significantly higher p53 expression levels compared to BE, reflux esophagitis or BE with concomitant esophagitis. We observed that expression of p53 was significantly higher in adenocarcinoma compared to BE or BE tissues positive for dysplasia. Interestingly, BE with concomitant esophagitis showed significantly higher p53 expression levels than BE alone, reflux esophagitis or the control group.
This observation is consistent with our findings in cell proliferation and may support the hypothesis that increasing p53 expression is accompanied by an upward shift of the proliferative compartment and might be induced by increased acid reflux in the multistep progression model of a metaplasia–dysplasia–adenocarcinoma sequence in BE. Further, cell proliferation- and p53 expression changes in the whole BE–dysplasia–adenocarcinoma sequence of the esophagus are strongly correlated.
We have also evaluated the correlation of expression changes between cell proliferation or p53 and recently analyzed MMP-9. The analysis was performed on the same settings of samples as previously.
MMP-9 is one member of the matrix metalloproteinases family, which is capable of degrading several components of the extracellular matrix (ECM). Increased expression of MMP-9 has been found in various carcinomas. With respect to the gastrointestinal tract, increased MMP-9 expressions have been observed in gastric [46] and colorectal cancer [47]. In the specific case of esophagus, increased expression of MMP-9 has been demonstrated in esophageal squamous cell carcinoma [48] and also in the BE–dysplasia–adenocarcinoma sequence, described by our group [23].
We found a linear correlation between both, cell proliferation and MMP-9 expression or p53- and MMP-9 expression, suggesting their association with esophageal tumor development and their specific role in the stepwise sequence to carcinoma in BE.
In summary, overexpression of p53 is typical in the malignant transformation of BE and increases with histological progression; and cell proliferation of Barrett’s epithelium increases with progressive grades of dysplasia and is linearly correlated with p53 expression.
The simultaneous activation of cell proliferation and p53 expression strongly suggest their association with esophageal tumor genesis and particularly, their specific role in the biology of esophageal adenocarcinoma. Our results confirm that activation of cell proliferation and p53 protein accumulation may play a crucial role in the early phase of the multistep esophageal carcinogenesis. Together with other biological markers, quantification of these parameters in BE might be useful to identify patients at higher risk for progression to adenocarcinoma, to prevent tumor development and to improve prognosis.
References
Bosetti C, Levi F, Ferlay J et al (2008) Trends in oesophageal cancer incidence and mortality in Europe. Int J Cancer 122(5):1118–1129
Wu X, Chen VW, Andrews PA et al (2007) Incidence of esophageal and gastric cancers among Hispanics, non-Hispanic whites and non-Hispanic blacks in the United States: subsite and histology differences. Cancer Causes Control 18(6):585–593
Fléjou JF (2005) Barrett’s oesophagus: from metaplasia to dysplasia and cancer. Gut 54(Suppl 1):i6–i12
Spechler SJ, Goyal RK (1986) Barrett’s esophagus. N Engl J Med 315(6):362–371
Westhoff B, Brotze S, Weston A et al (2005) The frequency of Barrett’s esophagus in high-risk patients with chronic GERD. Gastrointest Endosc 61(2):226–231
Jankowski JA, Harrison RF, Perry I et al (2000) Barrett’s metaplasia. Lancet 356(9247):2079–2085
Shaheen NJ (2005) Advances in Barrett’s esophagus and esophageal adenocarcinoma. Gastroenterology 128(6):1554–1566
Srivastava A, Hornick JL, Li X et al (2007) Extent of low-grade dysplasia is a risk factor for the development of esophageal adenocarcinoma in Barrett’s esophagus. Am J Gastroenterol 102(3):483–493
Schlansky B, Dimarino AJ Jr, Loren D et al (2006) A survey of oesophageal cancer: pathology, stage and clinical presentation. Aliment Pharmacol Ther 23(5):587–593
Skacel M, Petras RE, Gramlich TL et al (2000) The diagnosis of low-grade dysplasia in Barrett’s esophagus and its implications for disease progression. Am J Gastroenterol 95(12):3383–3387
McManus DT, Olaru A, Meltzer SJ (2004) Biomarkers of esophageal adenocarcinoma and Barrett’s esophagus. Cancer Res 64(5):1561–1569
Younes M, Ertan A, Lechago LV et al (1997) p53 protein accumulation is a specific marker of malignant potential in Barrett’s metaplasia. Dig Dis Sci 42(4):697–701
Hong MK, Laskin WB, Herman BE et al (1995) Expansion of the Ki-67 proliferative compartment correlates with degree of dysplasia in Barrett’s esophagus. Cancer 75(2):423–429
Prelich G, Tan CK, Kostura M et al (1987) Functional identity of proliferating cell nuclear antigen and a DNA polymerase auxiliary protein. Nature 326(6112):517–520
Reid BJ, Sanchez CA, Blount PL et al (1993) Barrett’s esophagus: cell cycle abnormalities in advancing stages of neoplastic progression. Gastroenterology 105(1):119–129
el-Deiry WS, Harper JW, O’Connor PM et al (1994) WAF1/CIP1 is induced in p53-mediated G1 arrest and apoptosis. Cancer Res 54(5):1169–1174
Ramel S, Reid BJ, Sanchez CA et al (1992) Evaluation of p53 protein expression in Barrett’s esophagus by two-parameter flow cytometry. Gastroenterology 102(4 Pt 1):1220–1228
Wang DY, Xiang YY, Tanaka M et al (1994) High prevalence of p53 protein overexpression in patients with esophageal cancer in Linxian, China and its relationship to progression and prognosis. Cancer 74(12):3089–3096
Slade N, Moll UM (2003) Mutational analysis of p53 in human tumors: immunocytochemistry. Methods Mol Biol 234:231–243
Bian YS, Osterheld MC, Bosman FT et al (2001) p53 gene mutation and protein accumulation during neoplastic progression in Barrett’s esophagus. Mod Pathol 14(5):397–403
Geboes K, Van Eyken P et al (2000) The diagnosis of dysplasia and malignancy in Barrett’s oesophagus. Histopathology 37(2):99–107
Polkowski W, van Lanschot JJ, ten Kate FJ et al (1995) The value of p53 and Ki67 as markers for tumour progression in the Barrett’s dysplasia–carcinoma sequence. Surg Oncol 4(3):163–171
Herszenyi L, Hritz I, Pregun I et al (2007) Alterations of glutathione S-transferase and matrix metalloproteinase-9 expressions are early events in esophageal carcinogenesis. World J Gastroenterol 13(5):676–682
Hritz I, Kuester D, Vieth M et al (2006) Secretory leukocyte protease inhibitor expression in various types of gastritis: a specific role of Helicobacter pylori infection. Eur J Gastroenterol Hepatol 18(3):277–282
Hritz I, Herszenyi L, Molnar B et al (2005) Proton pump inhibitor co-therapy normalizes the increased cell turnover of the gastric mucosa both in NSAID and selective COX-2 users. Int J Immunpathol Pharmacol 18(1):75–84
Hritz I, Herszenyi L, Molnar B et al (2005) Long-term omeprazole and esomeprazole treatment does not significantly increase gastric epithelial cell proliferation and epithelial growth factor receptor expression and has no effect on apoptosis and p53 expression. World J Gastroenterol 11(30):4721–4726
Fitzgerald RC et al (2006) Molecular basis of Barrett’s oesophagus and oesophageal adenocarcinoma. Gut 55(12):1810–1820
Reid BJ, Weinstein WM, Lewin KJ et al (1988) Endoscopic biopsy can detect high-grade dysplasia or early adenocarcinoma in Barrett’s esophagus without grossly recognizable neoplastic lesions. Gastroenterology 94(1):81–90
Theisen J, Nigro JJ, DeMeester TR et al (2004) Chronology of the Barrett’s metaplasia–dysplasia–carcinoma sequence. Dis Esophagus 17(1):67–70
Kleeff J, Friess H, Liao Q et al (2002) Immunohistochemical presentation in non-malignant and malignant Barrett’s epithelium. Dis Esophagus 15(1):10–15
Biasco G et al (2004) Cell proliferation and differentiation in familial adenomatous polyposis (FAP). Hum Pathol 35(12):1573
Scalmati A, Roncucci L, Ghidini G et al (1990) Epithelial cell kinetics in the remaining colorectal mucosa after surgery for cancer of the large bowel. Cancer Res 50(24):7937–7941
Bechi P, Balzi M, Becciolini A et al (1996) Helicobacter pylori and cell proliferation of the gastric mucosa: possible implications for gastric carcinogenesis. Am J Gastroenterol 91(2):271–276
Peters FT, Ganesh S, Kuipers EJ et al (1998) Epithelial cell proliferative activity of Barrett’s esophagus: methodology and correlation with traditional cancer risk markers. Dig Dis Sci 43(7):1501–1506
Rioux-Leclercq N, Turlin B, Sutherland F et al (1999) Analysis of Ki-67, p53 and Bcl-2 expression in the dysplasia–carcinoma sequence of Barrett’s esophagus. Oncol Rep 6(4):877–882
Kim R, Clarke MR, Melhem MF et al (1997) Expression of p53, PCNA, and CerbB-2 in Barrett’s metaplasia and adenocarcinoma. Dig Dis Sci 42(12):2453–2462
Kataoka H, Joh T, Kasugai K et al (1997) Mitogenic properties of human gastric juice. Dig Dis Sci 42(8):1747–1754
Lagergren J, Bergstrom R, Lindgren A et al (1999) Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med 340(11):825–831
Shaheen N, Ransohoff DF et al (2002) Gastroesophageal reflux, Barrett esophagus, and esophageal cancer: scientific review. JAMA 287(15):1972–1981
Peters FT, Ganesh S, Kuipers EJ et al (2000) Effect of elimination of acid reflux on epithelial cell proliferative activity of Barrett esophagus. Scand J Gastroenterol 35(12):1238–1244
Ireland AP, Clark GW, DeMeester TR (1997) Barrett’s esophagus. The significance of p53 in clinical practice. Ann Surg 225(1):17–30
Flejou JF, Potet F, Muzeau F et al (1993) Overexpression of p53 protein in Barrett’s syndrome with malignant transformation. J Clin Pathol 46(4):330–333
Schneider PM, Casson AG, Levin B et al (1996) Mutations of p53 in Barrett’s esophagus and Barrett’s cancer: a prospective study of 98 cases. J Thorac Cardiovasc Surg 111(2):323–331
Hornick JL, Mino-Kenudson M, Lauwers GY et al (2008) Buried Barrett’s epithelium following photodynamic therapy shows reduced crypt proliferation and absence of DNA content abnormalities. Am J Gastroenterol 103(1):38–47
Younes M, Lebovitz RM, Lechago LV et al (1993) p53 protein accumulation in Barrett’s metaplasia, dysplasia, and carcinoma: a follow-up study. Gastroenterology 105(6):1637–1642
Sun WH, Sun YL, Fang RN et al (2005) Expression of cyclooxygenase-2 and matrix metalloproteinase-9 in gastric carcinoma and its correlation with angiogenesis. Jpn J Clin Oncol 35(12):707–713
Takeuchi T, Hisanaga M, Nagao M et al (2004) The membrane-anchored matrix metalloproteinase (MMP) regulator RECK in combination with MMP-9 serves as an informative prognostic indicator for colorectal cancer. Clin Cancer Res 10(16):5572–5579
Samantaray S, Sharma R, Chattopadhyaya TK et al (2004) Increased expression of MMP-2 and MMP-9 in esophageal squamous cell carcinoma. J Cancer Res Clin Oncol 130(1):37–44
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hritz, I., Gyorffy, H., Molnar, B. et al. Increased p53 Expression in the Malignant Transformation of Barrett’s Esophagus is Accompanied by an Upward Shift of the Proliferative Compartment. Pathol. Oncol. Res. 15, 183–192 (2009). https://doi.org/10.1007/s12253-008-9095-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12253-008-9095-z