
Abstract
Our aim in this study was to evaluate hyoid bone movement trajectories and the age-related changes during swallowing in healthy subjects by ultrasonography. Data were obtained from 30 healthy volunteers (15 men, 15 women) in three age groups (20–39, 40–59, 60–79 years). The subjects were examined while sitting in an upright position, with the back against a wall to control movement. The transducer was placed in a longitudinal scan above the larynx. The subjects were then given 5 mL of mineral water. The water bolus was held in their mouth until they were forced to do a rapid swallow. The imaging was repeated five times for averaging. The movement was divided into 4 phases: slowly ascending phase (A–B, Elevation); rapidly ascending phase (B–C, Anterior); temporary pause phase (position of maximum rise, Remain); and rapidly and slowly descending shifts toward the resting position phase (C–D, Return). We easily visualized the hyoid bone trajectory by using ultrasonography. In all cases, ultrasonographic analysis of the hyoid bone was confirmed to have a similar trajectory, as determined with videofluoroscopy. The average swallowing duration measurements increased with age. The measurement of the maximally elevated point of the hyoid bone decreased with age. The movement of the hyoid bone during swallowing can be visualized by US. The trajectory of the hyoid bone in sagittal section indicated the capability of swallowing, and may detect some anomalies in swallowing.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Feeding and swallowing dysfunction are of greater concern now than in the past because of the increased number of elderly people, and the potential for increased risk of pneumonia from dysphagia with frequent aspiration. X-ray videofluoroscopy is generally considered the “gold standard” method for diagnosing dysphagia [1, 2]. However, this procedure has a number of limitations, including exposure of patients to radiation and the fact that it requires use of a contrast medium. On the other hand, transabdominal ultrasonography (US) is applied widely in clinical practice because of its low cost, safety of the technique, speed, and absence of radiation exposure. If US would make it possible safely and conveniently to carry out the evaluation of the swallowing function, it would become a useful method for diagnosing dysphagia. To our knowledge, in two groups the hyoid bone movement was measured during swallowing [3, 4]. However, not much has been done to clarify the analyses of hyoid bone movement by US. Our aim in this study was to use US to evaluate hyoid bone movement trajectories and the age-related changes during swallowing in healthy subjects.
Methods
Subjects
A total of 30 healthy adult volunteers underwent sonographic examination of swallowing. The subjects were divided into three age groups: 20–39 years (n = 10 with 5 men and 5 women; mean age, 29.6 ± 6.4), 40–59 years (n = 10 with 5 men and 5 women; mean age, 47.7 ± 4.4), and 60–79 years (n = 10 with 5 men and 5 women; mean age, 65.1 ± 5.3). The subjects had no complaints or history of swallowing difficulties, or any medical conditions that might affect deglutition. The study was approved by the ethics committee of Katsuragi hospital, and informed consent was obtained from all subjects.
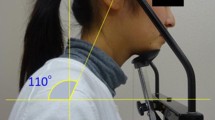
Instrumentation (Fig. 1)
The subjects were examined sitting in the upright position, with their back resting against a wall to control movement. With the transducer placed in a longitudinal scan above the larynx, the hyoid bone was located in the middle of the screen. The measuring point to be located was the tip of the cranial hyoid bone, and the monitor displayed the cranial part on the left side and the caudal part on the right side. The hyoid bone was identified on the scan as a high echoic area with a posterior acoustic shadow. The subjects were then given 5 mL of mineral water. The water bolus was held in their mouth, and they were forced to do a rapid swallow. The imaging was repeated five times for averaging. A swallow was judged complete when the transducer was correctly placed and the hyoid bone returned to its resting position. The moving images were preserved on a hard disk by use of US equipment. Ultrasound diagnostic equipment (Xario, Toshiba Medical Systems, Tokyo, Japan) was used with curved-array (3.5–7.0 MHz) transducers (PVT-674BT, Toshiba) which allowed for replay and observation in slow motion or frame by frame mode.

a The submental position of the transducer and setting of the curved-array transducers during scanning of the hyoid bone in the sagittal plane. b Sonograms show the measurement point of the hyoid bone
Data analysis
Image J software was used for image analysis and processing, and digital-sonographic recordings were viewed at 30 frames/s for 3 s. Frozen frames of the moving image were analyzed, and the range of movement of the hyoid bone from the resting point was measured (X axis, horizontal migration length; Y axis, perpendicular migration length). We measured the time intervals between A and B, B and C, and C and D (Fig. 2). A corresponds to the initiation of hyoid motion, B indicates full elevation and beginning of anterior motion, C corresponds to maximum anterior displacement and beginning of return motion, and D indicates completion of the return to the original resting position. The total swallowing duration was calculated by determination of the interval from A to D. The maximal elevated point of the hyoid bone was measured from A to C in all subjects.

a Diagram shows hyoid bone trajectory by videofluoroscopy. b Sonograms show the range of hyoid bone movement from the resting point on coordinate axes
One-way analysis of variance was used for comparison of the mean swallowing duration times among the groups. Statistical analyses were performed with SPSS 10.0 software (SPSS Inc, Chicago, IL), and P < 0.05 was considered to indicate significance.
Result
Analysis of hyoid bone movement
In all cases, the normal hyoid bone trajectory was easily visualized by US. Figure 3 shows the trajectories of 5 swallows of one normal subject. This figure demonstrates that a normal swallow generally consists of four phases. First, the hyoid bone rises from its resting position (A–B, labeled Elevation) after swallowing is initiated. Second, the hyoid bone move anteriorly to reach its maximum displacement (B–C, Anterior). Third, the hyoid bone remains in a temporary phase (position of maximum rise, Remain). Finally, the hyoid bone returns to its resting position (C–D, Return).

The normal hyoid bone trajectory of 5 consecutive swallows (5-mL water boluses) in a 24-year-old female
Swallowing duration times in the three groups
Table 1 shows the measurements of the average duration (Elevation, Anterior, Remain, and Return) of the 3 groups for 5 control swallows of 5 mL of water each. Regarding the duration of measurements of the 30 normal subjects, the total time for the Elevation, Anterior and Return average swallowing duration measurements increased with age. There was a significant difference in swallowing duration (total time) between the 20–39 group and the 40–59 group and between the 20–39 group and 60–79 group (P < 0.05). However, the Remain average swallowing duration decreased from age 60–79 years during that interval. The measurement of the maximally elevated point of the hyoid bone decreased with age (Fig. 4). Significant differences were found between the 20–39 group and 60–79 group (P < 0.05) in the maximally elevated point of the hyoid bone.

Representative maximally elevated points of hyoid bone by age group. The maximal hyoid elevation was reduced in old persons
Discussion
A swallowing test is a simple, easy-to-use method of bedside dysphagia screening; many dysphagia patients are bedridden. Videofluoroscopic assessment of swallowing is widely used in clinical settings, it has a number of limitations, practicability, and the exposure of patients to radiation. Similarly, fiberoptic endoscopic evaluation of swallowing for identifying patients with in stressful situation [5], and is not just a screening procedure [6].
Clinical tests can be performed at the bedside; however, these are not quantitative tests [7]. US has the advantage of being a quick screening tool which can be used safely and easily at the bedside. In this study, the trajectory of the hyoid bone identified by US analysis was confirmed to be similar to that seen by videofluoroscopy [3, 8–10]. Sonies et al. [3] reported that they used US for an analysis of hyoid bone movement for only six normal volunteers, and they obtained similar result. However, it is not a simple technique, because the machine must be correctly selected. In addition, the ultrasound Doppler beam will be missed due to reflection of the movement of the muscles surrounding the hyoid bone. Kuhl et al. [4] showed that laryngeal elevation could be measured by identification of the thyroid cartilage and the hyoid bone, but they did not track the hyoid bone motion. In this study, US accurately determined the swallowing duration and the trajectory of hyoid bone movement. In addition, US can be a useful tool for monitoring of swallowing movement, which allows for repeated swallowing tests.
On imaging 5 times the hyoid bone trajectories were depicted similarly, displaying accuracy of movement in the same subject. Some studies have reported that the position of the head influences pharyngeal swallowing [11, 12]. Investigators should realize several important issues, including control of transducer placement and control of head movement [13]. In this study, another probable reason for the difficulty in natural swallowing is due to the transducer over pressing the hyoid bone. Therefore, future studies would need to use better quality ultrasound equipment to ensure more effective image evaluation. Based on the ultrasonographic observation, swallowing affected the jaw and cartilago thyroidea; a convex type or sector type probe should be used.
The total average swallowing duration measured increased with age. Review of three phases, the average duration of hyoid bone Elevation (A–B), Anterior (B–C), and Return (C–D) movement increased with age; however, the hyoid bone remains in a temporary phase decreased rapidly in conformed with aged 60–79 years. Also, the maximal elevation point of the hyoid bone movement trajectories decreased with age. Kendall et al. [14] reported that the hyoid elevation was slow, and the duration of maximal hyoid elevation was reduced, in elderly persons. Ekberg et al. [5] found that elderly persons had a much higher frequency of swallowing dysfunction. The reason might be that reduced hyoid bone elevation due to atrophy of the surrounding muscles (digastric muscle, mylohyoid muscle, stylohyoid muscle, geniohyoid muscle) results in less tension and in loosening of ligaments during swallowing. The number of functioning muscle motor units declines with age [15]. In this study, we used drinking water as convenient samples; however, any test food or drink can be chosen. Thus, we will plan to examine the effect of food on hyoid bone motion.
This study had some limitations. First, we did not include subjects more than 80 years old, nor did we include subjects who had swallowing disorders. Moreover, the number of subjects was small. Second, the sonography-displayed hyoid bone movement during swallowing could not be compared with that on an X-ray videofluoroscopy, for the obvious reason that invasive examination, such as the use of a contrast medium or radiation exposure, is not possible in healthy subjects. We plan to study hyoid bone movement in older subjects and in those with dysphagia in the future.
Conclusion
The results showed that dynamic phase images of the every hyoid bone movement can be obtained by means of ultrasonographic visualization. US can be a quantitative method for clinical evaluation of hyoid bone movement during swallowing. Our findings may indicate that the position of the hyoid bone can be “detected” by US for analysis of abnormal movements of the hyoid bone.
References
Logemann JA, Pauloski BR, Rademaker AW, Colangelo LA, Kahrilas PJ, Smith CH. Temporal and biomechanical characteristics of oropharyngeal swallow in younger and older men. J Speech Lang Hear Res. 2000;43:264–74.
Logemann JA, Pauloski BR, Rademaker AW, Kahrilas PJ. Oropharyngeal swallow in younger and older women: videofluoroscopic analysis. J Speech Lang Hear Res. 2002;45:434–45.
Sonies BC, Wang C, Sapper DJ. Evaluation of normal and abnormal hyoid bone movement during swallowing by use of ultrasound duplex-Doppler imaging. Ultrasound Med Biol. 1996;22:1169–75.
Kuhl V, Eicke BM, Dieterich M, Urban PP. Sonographic analysis of laryngeal elevation during swallowing. J Neurol. 2003;250:333–7.
Ekberg O, Feinberg MJ. Altered swallowing function in elderly patients without dysphagia: radiologic findings in 56 cases. Am J Roentgenol. 1991;156:1181–4.
Hafner G, Neuhuber A, Hirtenfelder S, Schmedler B, Eckel HE. Fiberoptic endoscopic evaluation of swallowing in intensive care unit patients. Eur Arch Otorhinolaryngol. 2008;265:441–6.
Martino R, Pron G, Diamant N. Screening for oropharyngeal dysphagia in stroke: insufficient evidence for guidelines. Dysphagia. 2000;15:19–30.
Saunders JB, Davis C, Miller ER. The mechanism of deglutition (second stage) as revealed by cine-radiography. Ann Otol Rhinol Laryngol. 1951;60:897–916.
Ramsey GH, Watson JS, Gramiak R, Weinberg SA. Cinefluorographic analysis of the mechanism of swallowing. Radiology. 1955;64:498–518.
Perlman AL, VanDaele DJ, Otterbacher MS. Quantitative assessment of hyoid bone displacement from video images during swallowing. J Speech Hear Res. 1995;38:579–85.
Logemann JA, Kahrilas PJ, Kobara M, Vakil NB. The benefit of head rotation on pharyngoesophageal dysphagia. Arch Phys Med Rehabil. 1989;70:767–71.
Ekberg O. Posture of the head and pharyngeal swallowing. Acta Radiol Diagn. 1986;27:691–6.
Chi-Fishman G. Quantitative lingual, pharyngeal and laryngeal ultrasonography in swallowing research: a technical review. Clin Linguist Phon. 2005;19:589–604.
Kendall KA, Leonard RJ. Hyoid movement during swallowing in older patients with dysphagia. Arch Otolaryngol Head Neck Surg. 2001;127:1224–9.
Campbell MJ, McComas AJ, Petito F. Physiological changes in ageing muscles. J Neurol Neurosurg Psychiatry. 1973;36:174–82.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Yabunaka, K., Sanada, H., Sanada, S. et al. Sonographic assessment of hyoid bone movement during swallowing: a study of normal adults with advancing age. Radiol Phys Technol 4, 73–77 (2011). https://doi.org/10.1007/s12194-010-0107-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12194-010-0107-9